
Abstract
This study aimed to investigate whether there was an association between an unanticipated prolonged post-anaesthesia care unit (PACU) length of stay and early postoperative deterioration, as defined as the need for a rapid response team activation, within the first seven days of surgery. We conducted a single-centre retrospective cohort study of adult surgical patients, who stayed at least one night in hospital, and were not admitted to critical care immediately postoperatively, between 1 July 2017 and 30 June 2019. A total of 11,885 cases were analysed. PACU length of stay was significantly associated with rapid response team activation on both univariate (odds ratio (OR) per increment 1.57, 95% confidence intervals (CI) 1.45 to 1.69, P < 0.001) and multivariate analysis (OR per increment 1.41, 95% CI 1.28 to 1.55, P < 0.001). Patients who stayed less than one hour were at low risk of deterioration (absolute risk 3.7%). In patients staying longer than one hour, the absolute increase in risk was small but observable within six hours of PACU discharge. Compar\ed to a one-hour length of stay, a five-hour stay had a relative risk of 4.9 (95% CI 3.7 to 6.1). Other factors associated with rapid response team activation included non-elective surgery (OR 1.78, P < 0.001) and theatre length of stay (OR per increment 1.61, P < 0.001). PACU length of stay was also independently associated with predefined complications and unplanned intensive care unit admission postoperatively. In our cohort, an unanticipated prolonged PACU length of stay of over one hour was associated with an increased incidence of rapid response team activation in the first seven days postoperatively.
Keywords
Introduction
Surgical patients are at risk of complications in the immediate postoperative period.1,2 Admission to a post-anaesthesia care unit (PACU), or post-anaesthesia recovery room, is the accepted standard of care after surgery and anaesthesia. These units allow patients to be monitored in a high nurse-to-patient ratio environment until sufficient physiological recovery occurs to allow discharge to the ward. This, in combination with their close proximity to anaesthesia and operating rooms, facilitates timely intervention in the event of early deterioration.
The most common problems faced by patients in the immediate postoperative period are cardiovascular (24%–42%) and respiratory (22%–23%),1,2 and patients who develop such issues may experience a longer PACU admission than those who do not.2,3 However, despite the PACU being a routine part of the patient’s perioperative journey, the importance of an unanticipated prolonged PACU stay on early postoperative deterioration is unclear.
Hospitalised patients with physiological derangements are at risk of significant deterioration, 4 and rapid response systems have been developed in many health systems to identify such patients. 5 A rapid response team (RRT) activation in the postoperative period is an indicator that early deterioration has occurred.6,7 Identifying variables that are associated with a patient’s risk of subsequent RRT activation is a topic of interest 8 as early detection and intervention may prevent progression to deterioration. 9
This study aimed to examine the hypothesis that an unanticipated prolonged PACU length of stay is associated with early postoperative deterioration among adult surgical patients, as defined by at least one RRT activation within seven days of surgery, as well as other adverse postoperative outcomes.
Methods
Study design and setting
We performed a single-centre retrospective cohort study in a tertiary university hospital based in Melbourne, Australia. This study was approved, and a waiver of consent was obtained from the Austin Health Human Research Ethics Committee (Audit/19/Austin/78) on 31 July 2019. Our hospital utilises an electronic medical record platform (Cerner, North Kansas City, MO, USA) to capture comprehensive patient health data in the perioperative setting. We have an established and extensively studied rapid response system for recognising and responding to deteriorating hospitalised patients.10,11 Data were obtained from the electronic health record platform with the assistance of the Austin Health Data Analytics Research and Evaluation (DARE) Centre.
Patient selection
All patients undergoing surgery between and including 1 July 2017 and 30 June 2019 were screened for analysis. Patients were included if they were aged 18 years or older and were admitted for one or more nights postoperatively. To explore only unanticipated prolonged PACU stays, cases were excluded from the analysis if the patient was planned for an extended admission to PACU or was anticipated to require high dependency unit (HDU) or intensive care unit (ICU) admission immediately postoperatively, as identified in our electronic medical record. Cases were also excluded if they were performed by a non-surgical specialty (cardiology, respiratory, gastroenterology and psychiatry), very low volume of practice specialties (gynaecology) or involved a diagnostic procedure under anaesthesia.
Data collected
For each surgical case, patient characteristics, Charlson comorbidity index scores, surgical and perioperative details, preoperative pathology, RRT activations, complications on discharge, re-admissions, return to theatre and mortality data were extracted from the electronic medical records. Preoperative haemoglobin, creatinine and albumin levels were taken as the last recorded measurement prior to the commencement of surgery. Postoperative critical care requirements and anticipated extended admission to the PACU were identified from bed request bookings, anaesthesia consult notes and perioperative tracking flags within the electronic medical record. PACU length of stay was recorded as the difference between the time of arrival in the PACU and the time of being medically suitable for discharge from the PACU to the hospital ward. Our discharge criteria include sufficient emergence from anaesthesia, adequate symptom control and cardiovascular and respiratory stability (see Appendix: Table 1).
Case characteristics.
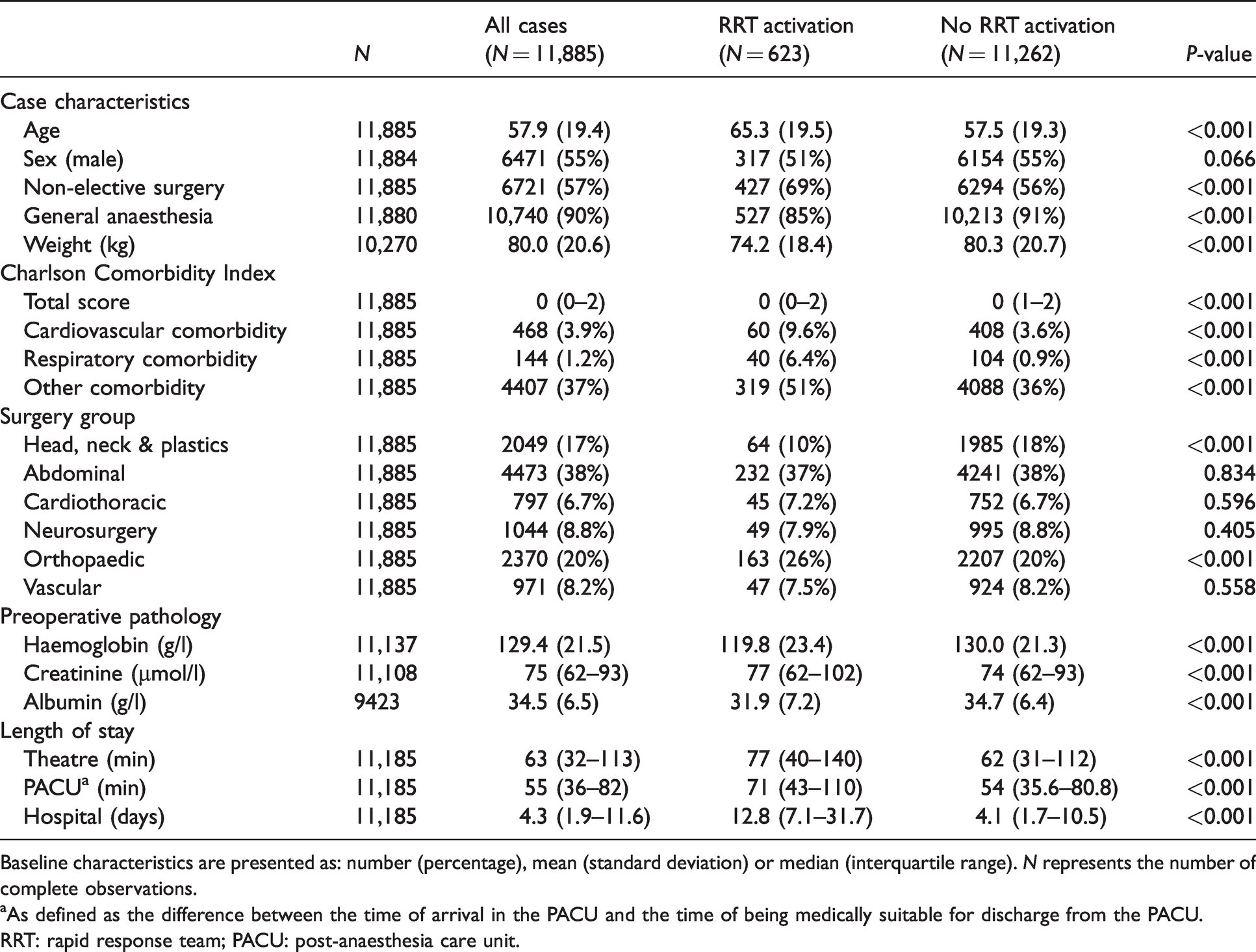
Baseline characteristics are presented as: number (percentage), mean (standard deviation) or median (interquartile range). N represents the number of complete observations.
aAs defined as the difference between the time of arrival in the PACU and the time of being medically suitable for discharge from the PACU.
RRT: rapid response team; PACU: post-anaesthesia care unit.
RRT activations were prompted in response to breaches in predefined criteria (see Appendix: Table 2), unless otherwise altered by the treating team, and resulted in urgent clinical review by senior intensive care and other medical staff. Only the first postoperative RRT activation occurring after discharge from the PACU and within seven days of surgery was included for analysis. RRT activations were divided into three subtypes by the primary reason for the response: cardiovascular, pertaining to changes in heart rate or blood pressure; respiratory, pertaining to oxygen saturation or respiratory rate; and others, pertaining to any other reason (see Appendix: Table 3). If an RRT activation was in response to multiple reasons, the most deranged physiological parameter was selected.
Postoperative RRT activation versus PACU length of stay.
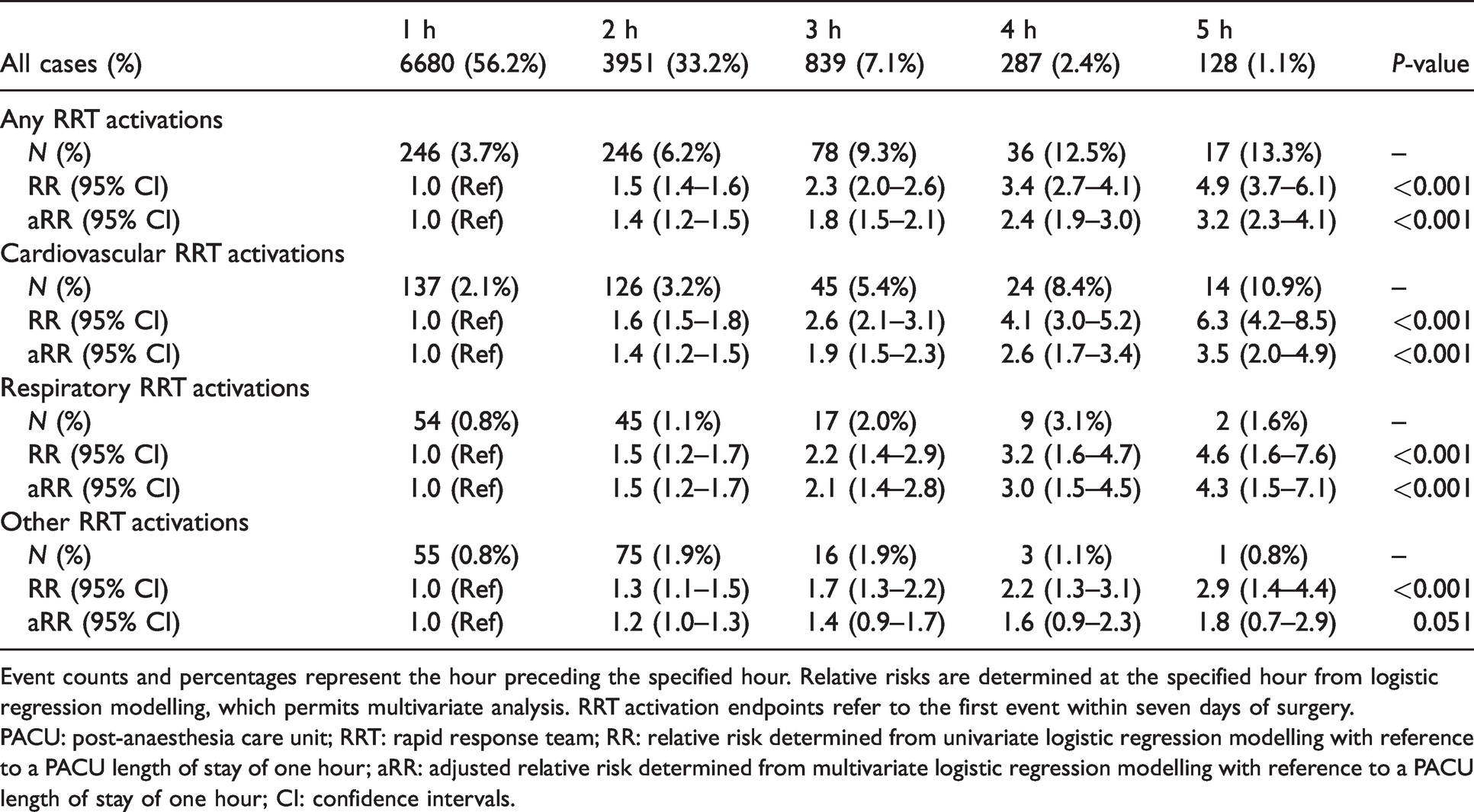
Event counts and percentages represent the hour preceding the specified hour. Relative risks are determined at the specified hour from logistic regression modelling, which permits multivariate analysis. RRT activation endpoints refer to the first event within seven days of surgery.
PACU: post-anaesthesia care unit; RRT: rapid response team; RR: relative risk determined from univariate logistic regression modelling with reference to a PACU length of stay of one hour; aRR: adjusted relative risk determined from multivariate logistic regression modelling with reference to a PACU length of stay of one hour; CI: confidence intervals.
Multivariate logistic regression model for any postoperative RRT activation.
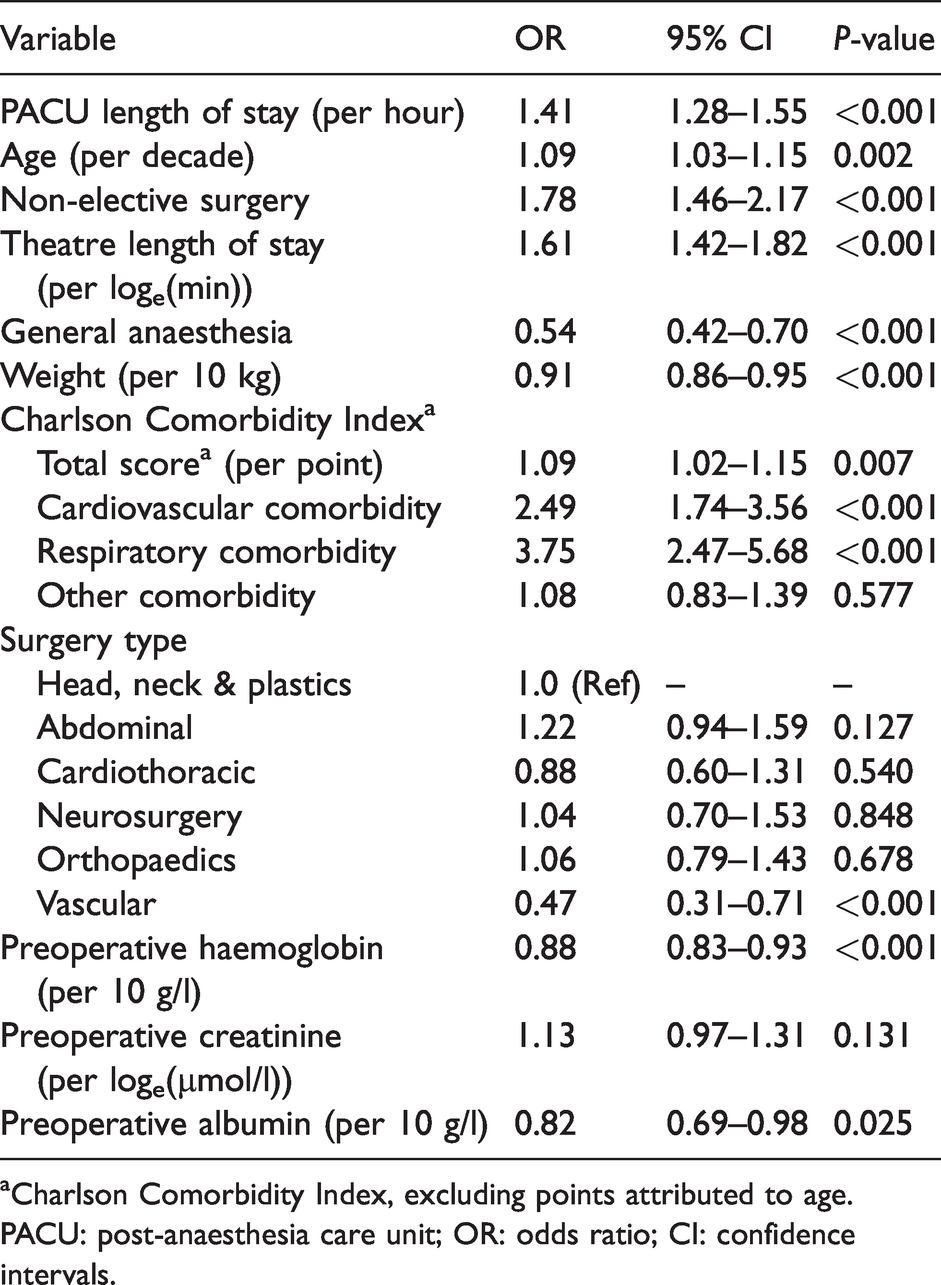
aCharlson Comorbidity Index, excluding points attributed to age.
PACU: post-anaesthesia care unit; OR: odds ratio; CI: confidence intervals.
Charlson Comorbidity Index scores were calculated from International Classification of Disease version 10 (ICD-10) codes on admission. Complications were identified using predefined ICD-10 codes (see Appendix: Table 4) assigned on discharge and were grouped into: cardiovascular, including cardiac arrest, myocardial ischaemia/infarction and arrhythmia; respiratory, including respiratory failure, pneumonia, pulmonary oedema, venous thromboembolism; and other, including renal impairment, cerebrovascular incident, delirium, fall, pressure injury, wound infection, sepsis, anaemia and bleeding.
Patient outcomes versus PACU length of stay.
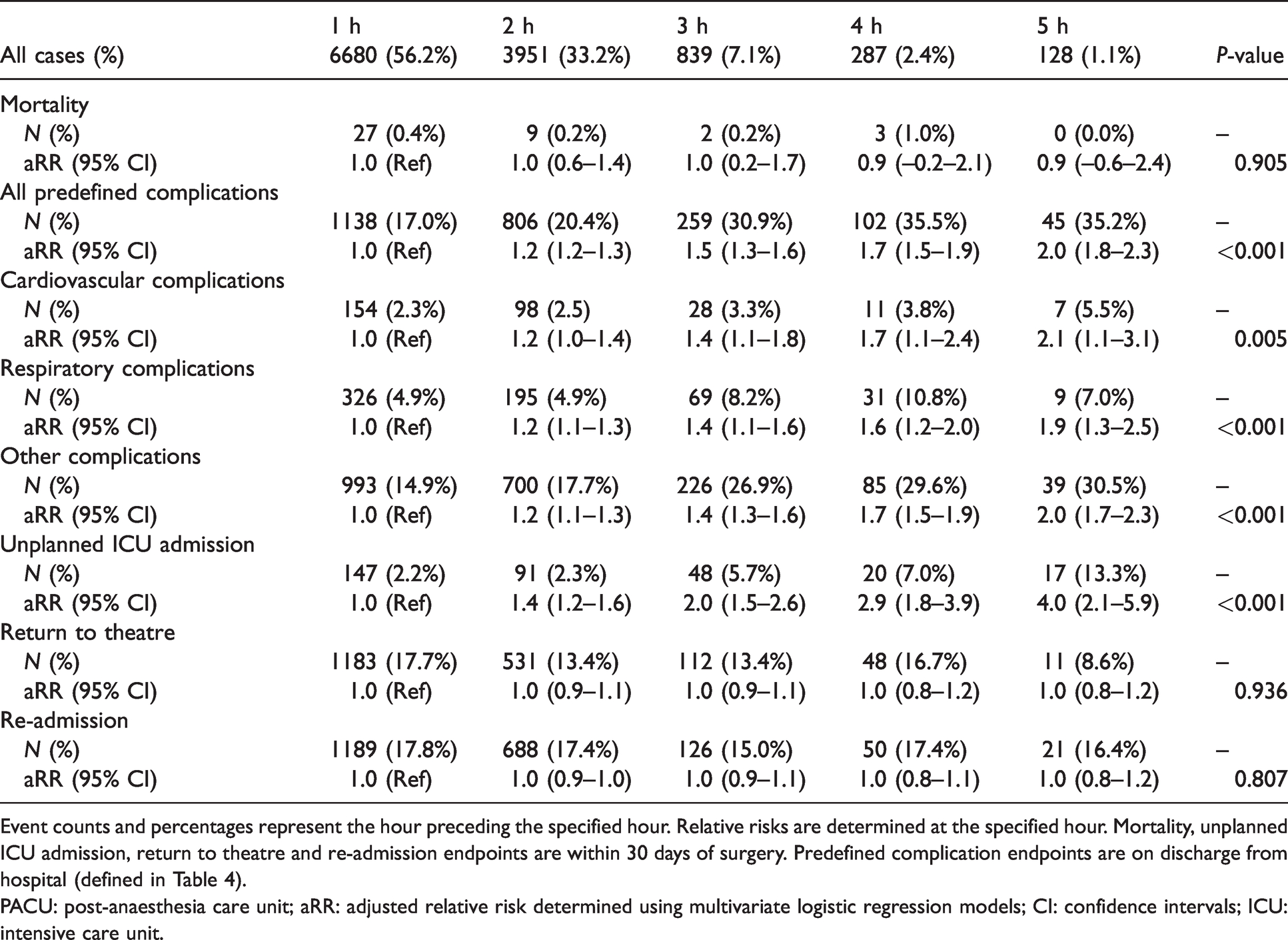
Event counts and percentages represent the hour preceding the specified hour. Relative risks are determined at the specified hour. Mortality, unplanned ICU admission, return to theatre and re-admission endpoints are within 30 days of surgery. Predefined complication endpoints are on discharge from hospital (defined in Table 4).
PACU: post-anaesthesia care unit; aRR: adjusted relative risk determined using multivariate logistic regression models; CI: confidence intervals; ICU: intensive care unit.
Unplanned ICU admission was defined as any admission to the HDU or ICU within 30 days of surgery, in cases in which the patient was not admitted to these locations electively. Return to theatre was defined as any planned or unplanned operations within 30 days of surgery, as the two could not be reliably distinguished in our dataset. Re-admission was defined as any rehospitalisation at our hospital within 30 days of surgery. Mortality was defined as death within 30 days of surgery.
Outcomes
The primary outcome of the study was the occurrence of at least one RRT activation within seven days of surgery. Secondary outcomes included 30-day mortality, predefined complications on discharge, unplanned ICU admission within 30 days, return to theatre within 30 days or re-admission within 30 days.
Statistical analysis
The statistical analysis plan was determined prior to data collection. Data were analysed for coding errors and were excluded if: the operation duration was unknown or was less than one minute or greater than 24 hours; PACU length of stay was unknown or was less than one minute or greater than five hours; or hospital coding data were incomplete. Patients with a PACU length of stay of longer than five hours were considered extreme outliers and were thought to represent coding errors. Extreme outliers, and non-binary values for binary variables, were removed and treated as missing data.
After assessing baseline characteristics, data were assessed for missing values. When missing data occurred in less than 1% of cases, values were confirmed from hospital records. Subsequently, when missing data occurred in less than 3% of cases, values were assumed to be the mode value. When missing data occurred in greater than 3% of cases, data were assumed to be missing at random, and were accounted for using multiple imputation. Based on a truncated regression model and using the multiple imputation chained equations (MICE) technique, 20 imputed datasets were constructed. The model included the primary outcome and all covariates. Outcome analysis was performed on each imputed dataset and the results were combined to provide mean estimates and standard errors that account for the imputation process. Imputed variables included weight (13.6% missing), preoperative haemoglobin (6.3% missing), preoperative creatinine (6.5% missing) and preoperative albumin (20.7% missing).
Two-sample t-test and chi-squared tests were performed on the non-imputed dataset to assess baseline characteristics of all cases, those that had a postoperative RRT activation and those that did not. The number of events and percentages of all events are reported for binary variables. The mean and standard deviation are reported for normally distributed variables. The median and interquartile range are reported for non-normally distributed variables. Data were grouped by PACU length of stay intervals of one hour. A two-tail P-value less than 0.05 was considered statistically significant.
Logistic regression modelling was used to describe the associations between PACU length of stay and the primary and secondary outcomes. PACU length of stay was analysed as a continuous variable. The odds ratios (ORs) and 95% confidence intervals (CIs) are reported for all primary and secondary outcomes, per hour stay in the PACU. Univariate logistic regression models were constructed using the imputed dataset. Multivariate logistic regression models were constructed from statistically significant univariate preoperative and intraoperative covariates using the imputed dataset. Multivariate model collinearity was assessed using the variance inflation factor. Calibration plots were generated to assess model performance. Receiver operating curve analysis was used to assess model discrimination. Sensitivity analyses were performed to determine whether the results remained significant after eliminating imputed variables.
Predictive margins were also used to estimate the relative risk (RR) for our primary and secondary outcomes at increasing PACU lengths of stays. This is to assist in interpreting the clinical significance of our findings, and to describe better the modelled difference in risk between two different PACU lengths of stays than can otherwise be achieved using ORs. The RRs are provided with reference to a PACU length of stay approximating the median value. This was decided a priori, and the median value was subsequently identified to be one hour on post hoc analysis. Kaplan–Meier analysis was performed for the primary outcome, stratified by PACU length of stay.
Statistical analyses were performed using Stata/SE version 15.1 (StataCorp, College Station, TX, USA). Graphs were produced using Prism version 8.2.1 (GraphPad, San Diego, CA, USA). This study is compliant with STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines.
Results
During the study period, 14,315 patients and 20,901 cases met the inclusion criteria. Of these, 4051 cases were excluded because they were either anticipated to require (670 cases) or did require (2900 cases) HDU or ICU admission immediately postoperatively or were anticipated to have a prolonged PACU stay (481 cases). A further 4544 cases were excluded on the basis of their procedure type (cardiology: 308; respiratory: 132; gastroenterology: 2691; psychiatry: 733; gynaecology: 38; diagnostic: 642). On review of the data, a further 421 cases were excluded due to coding errors. A total of 11,885 cases in 9555 patients were identified for analysis, and of these patients, 8183 underwent one surgery, 919 underwent two surgeries and 453 underwent three or more surgeries (Figure 1).
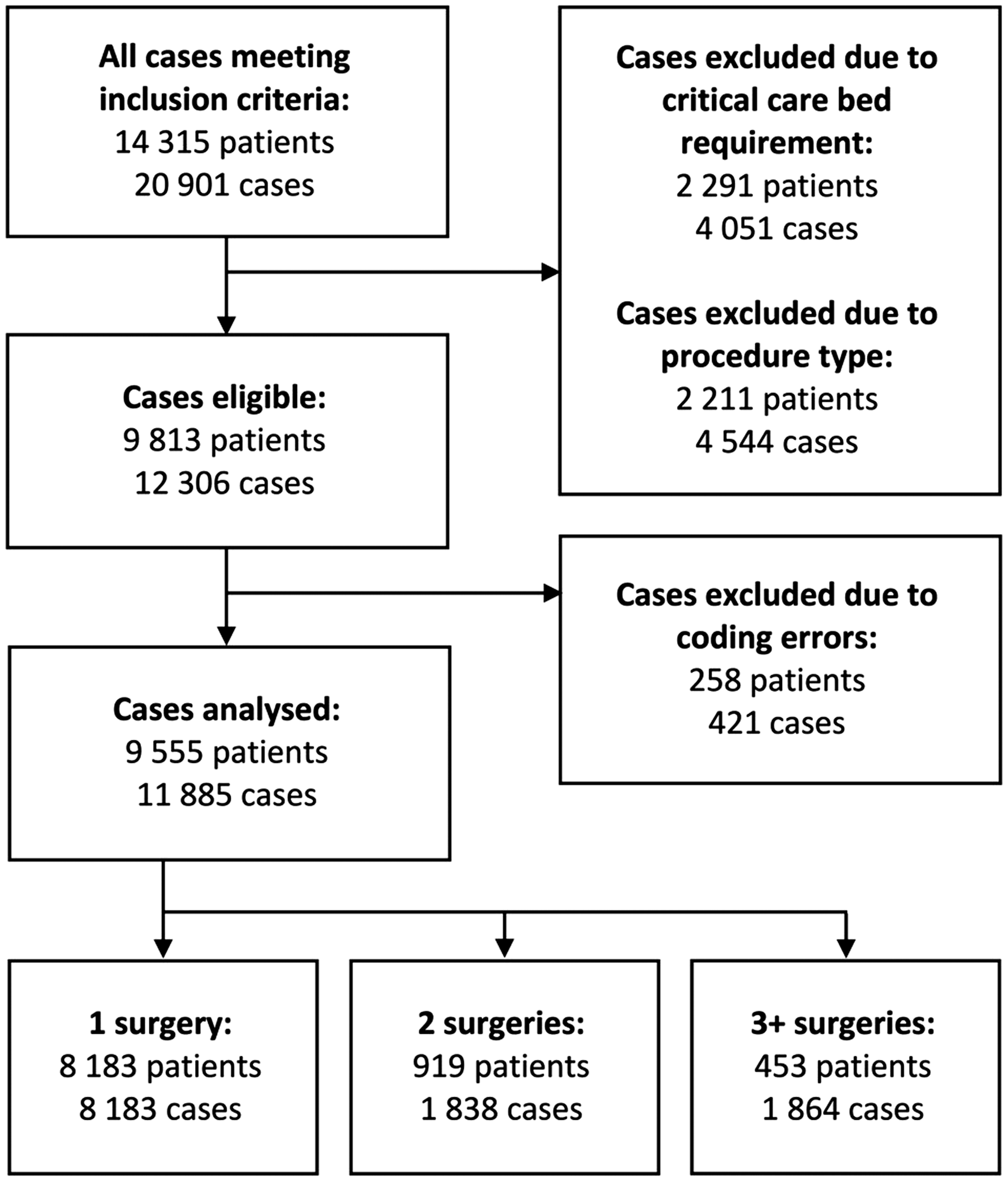
Inclusions and exclusions.
Baseline characteristics
The baseline characteristics for all cases, including those that had an RRT activation and those that did not, are presented in Table 1. Overall, 623 cases (5.2%) resulted in a postoperative RRT activation within seven days of surgery. Patients in this cohort were older (mean difference (MD) 7.8 years, P < 0.001), had more comorbidities (Charlson Comorbidity Index score MD 0.8, P < 0.001), weighed less (MD –6.1 kg, P < 0.001), underwent more non-elective surgery (MD 12.7%, P < 0.001) and a lower general anaesthetic rate (MD –6.1%, P < 0.001). They had a higher rate of orthopaedic surgery (MD 6.6%, P < 0.001) and a lower rate of head, neck and plastic surgery (MD –7.4%, P < 0.001). These patients had longer median surgery durations (77 versus 62 minutes, P < 0.001), had a longer median PACU length of stay (71 versus 54 minutes, P < 0.001) and had a longer median hospital admissions length (12.8 versus 4.1 days, P < 0.001).
Primary outcome
Association between PACU length of stay and any postoperative RRT activation
The association between PACU length of stay and postoperative RRT activation is described in Table 2. Across all cases, 6680 cases (56.2%) had a PACU length of stay of less than one hour, of which 246 cases (3.7%) went on to have a postoperative RRT activation. The remaining 5205 cases (43.8%) had a PACU length of stay exceeding one hour, of which 377 cases (7.2%) went on to have a postoperative RRT activation.
On univariate analysis, there was a significant association between PACU length of stay and postoperative RRT activation, with an OR per increment of 1.57 (95% CI 1.45 to 1.69, P < 0.001). Compared to a PACU length of stay of one hour, the RR of having a postoperative RRT activation is 1.5 at two hours (95% CI 1.4 to 1.6), 2.3 at three hours (95% CI 2.0 to 2.6), 3.4 at four hours (95% CI 2.7 to 4.1) and 4.9 at five hours (95% CI 3.7 to 6.1).
On univariate analysis, PACU length of stay demonstrates low discriminative accuracy for detecting postoperative RRT activation (area under the receiver operator curve (AUROC) 0.61). Using a threshold of one hour, PACU length of stay has a sensitivity of 60.5%, a specificity of 57.1%, a positive predictive value of 7.2% and a negative predictive value of 96.3%.
Results of the multivariate analysis are shown in Table 3. There was no significant collinearity in the multivariate model. After adjusting for confounders, the PACU length of stay remained significantly associated with postoperative RRT activation, with an OR per increment of 1.41 (95% CI 1.28 to 1.55, P < 0.001). On sensitivity analysis, this remained similarly significant on elimination of multiply imputed variables. The RR for each additional hour in PACU is presented in Table 2 and Figure 2.
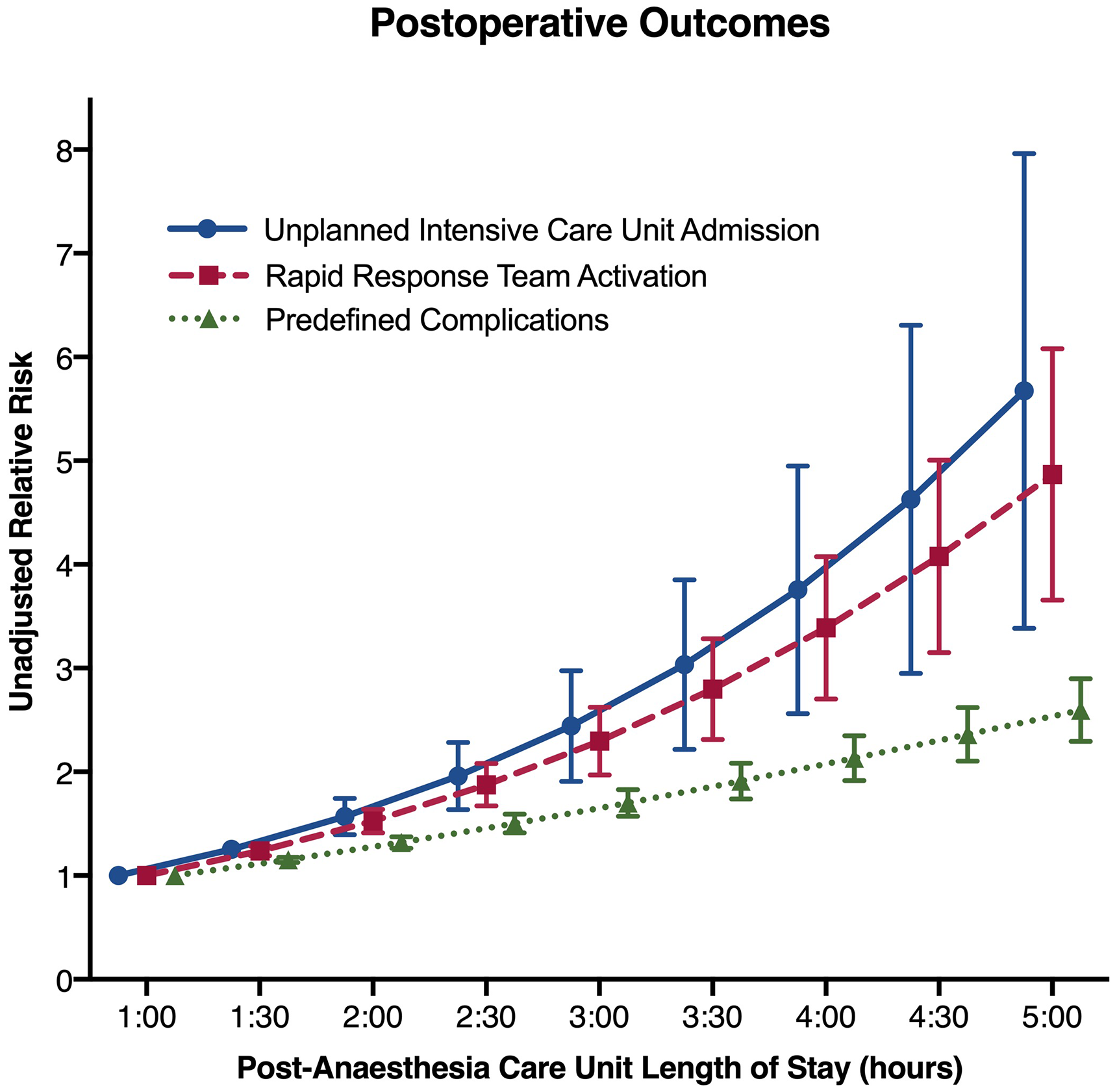
Postoperative outcomes.
Univariate and multivariate analyses were performed for cardiovascular, respiratory and other RRT activation subtypes. PACU length of stay was associated with a significant increase in cardiovascular and respiratory RRT activations on both univariate and multivariate analysis. While the PACU length of stay was associated with a significantly increased risk of other RRT activations on univariate analysis (OR per increment 1.31, 95% CI 1.15 to 1.51, P < 0.001), this association was not significant on multivariate analysis (OR per increment 1.17, 95% CI 1.00 to 1.37, P = 0.051) (Table 2, Figure 3).
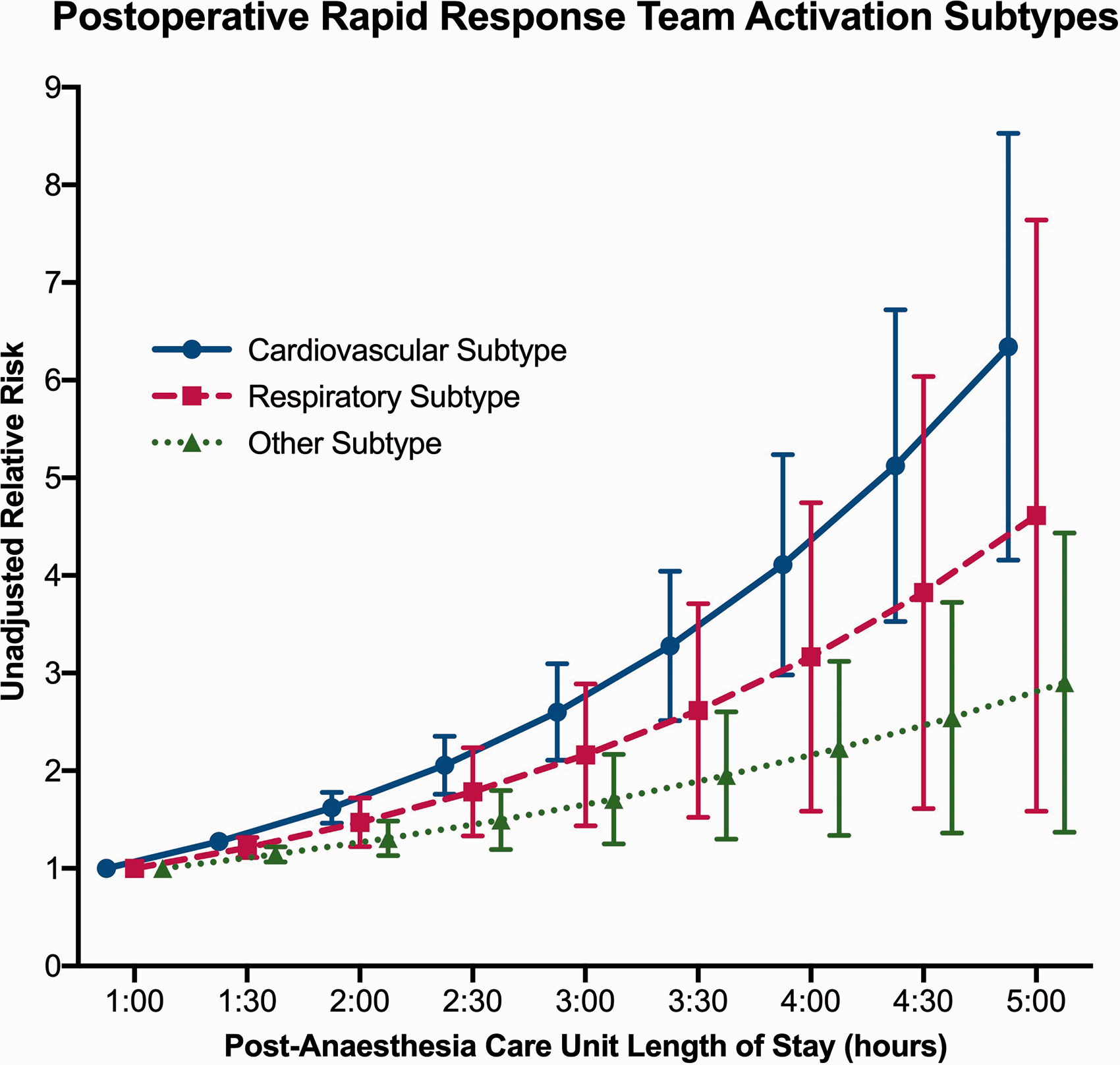
Postoperative rapid response team (RRT) activation types.
Kaplan–Meier analysis demonstrates the early separation of patients who had a postoperative RRT activation when stratified by PACU length of stay. Compared to a PACU length of stay of up to one hour, statistically significant separation is first seen at: six hours, 30 minutes after PACU discharge in patients staying one to two hours; and four hours 18 minutes after PACU discharge in patients staying two to five hours (Figure 4).
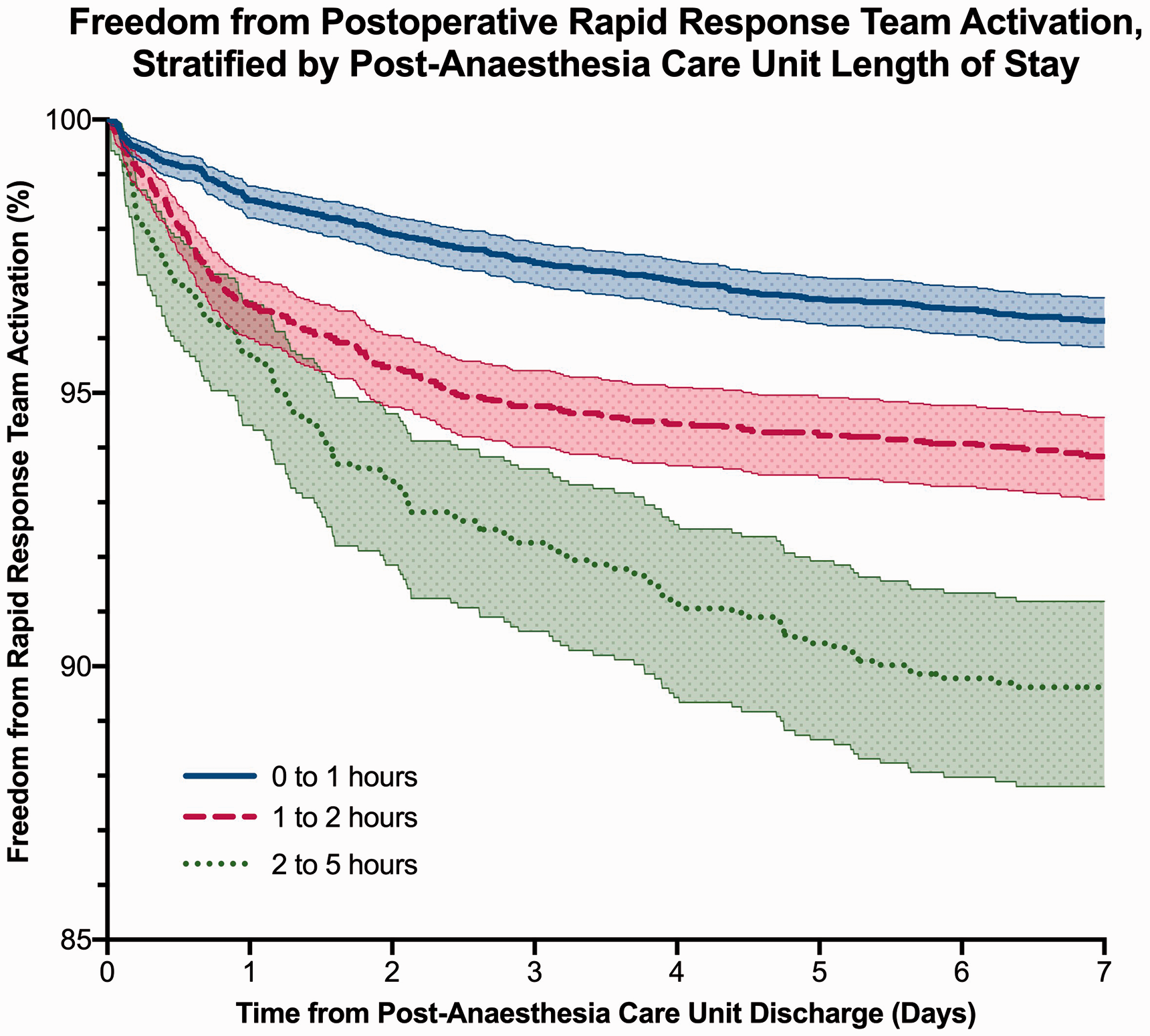
Freedom from postoperative rapid response team (RRT) activation, stratified by post-anaesthesia care unit length of stay.
Secondary outcomes
Predefined complications
On univariate analysis, there was a significant association between PACU length of stay and developing at least one predefined complication on discharge, with an OR per increment of 1.42 (95% CI 1.35 to 1.50, P < 0.001). There was no length of stay that demonstrated discriminative accuracy with regard to predefined complications. On multivariate analysis, after adjusting for confounders, this association remained significant, with an OR per increment of 1.37 (95% CI 1.28 to 1.47, P < 0.001) (Table 4, Figure 2).
Univariate and multivariate analyses were performed for cardiovascular, respiratory and other predefined complication subtypes. On both analyses, the PACU length of stay was associated with a significant increase in all predefined complication subtypes (Table 4).
Unplanned ICU admission
On univariate analysis, there was a significant association between PACU length of stay and unplanned ICU admission within 30 days, with an OR per increment of 1.59 (95% CI 1.42 to 1.79, P < 0.001). There was no length of stay that demonstrated discriminative accuracy with regard to unplanned ICU admission. On multivariate analysis, after adjusting for confounders, this association remained significant, with an OR per increment of 1.47 (95% CI 1.28 to 1.70, P < 0.001) (Table 4, Figure 2).
Other patient outcomes
There was no statistically significant univariate or multivariate association between the PACU length of stay and 30-day mortality, or 30-day re-admission to hospital (Table 4). While a negative association between PACU length of stay and return to theatre within 30 days was observed on univariate analysis (OR per increment 0.82, 95% CI 0.76 to 0.88, P < 0.001), this was not significant on multivariate analysis after adjusting for confounders (Table 4).
Discussion
Main findings
Our study shows that, in our cohort, an unanticipated prolonged PACU length of stay was strongly associated with at least one postoperative RRT activation within seven days of surgery. Although the discrimination of PACU length of stay of one hour was relatively poor, the association with RRT activation remained significant after multivariate analysis. Furthermore, other markers of deterioration, including complications and unplanned ICU admission within 30 days, were also associated with longer PACU stays.
Implications of findings
While the PACU length of stay was strongly associated with postoperative deterioration, it appears unlikely that the cumulative duration of exposure to the PACU environment is responsible for this elevated risk, or that early discharge from the PACU may improve patient outcomes. Instead, it is likely that longer PACU stays represent a broad spectrum of potential clinical comorbidity and events that significantly affect the patient’s risk of subsequent deterioration in the early postoperative period.
Our findings suggest that PACU length of stay, an easily measured metric, could be used to aid in risk stratification for early deterioration after surgery in our hospital. To our knowledge this is the first time a study has assessed this as a potential marker for RRT activation. Almost 50% of patients admitted to the PACU stayed longer than one hour. In these patients, the risk of RRT activation increased to nearly five-fold after a five-hour stay in the PACU, and this difference is observed within hours of discharge. Most of these patients do not deteriorate in the postoperative period, and intervention aimed at preventing this deterioration would have to be very widely applied with potentially significant resource usage. However, it is possible that a hospital-specific threshold for PACU length of stay could be chosen based on the balance between resource use and the aim to pre-empt RRT activation. Alternatively, PACU length of stay could be investigated for use in a multivariable predictive model, using a prospectively collected database, which would be likely to provide more granularity for variables such as procedure type and comorbidity. A more accurate prediction may enable the better allocation of postoperative resources. These approaches require further study.
Kaplan–Meier analysis demonstrated that the first RRT activation occurred most frequently within the first few days of surgery but continued to occur at a sustained rate up to seven days postoperatively. An increasing PACU length of stay was associated with both a steeper initial and sustained rate of RRT activation. Early separation of groups implies that the path to deterioration may be established prior to discharge from the PACU. Our secondary outcome analysis shows that PACU length of stay is independently associated with predefined complications and unplanned ICU admission within 30 days. Identifying these at-risk patients prior to deterioration may be important.12,13
However, our modelling is only meant to be explanatory and further studies are required to assess the diagnostic accuracy of PACU length of stay as a predictor of postoperative deterioration and adverse outcomes.
Comparison with previous literature
To our knowledge, this is the first study published that explores the association between PACU length of stay and adverse postoperative outcomes. The previously literature in this field describes patterns of deterioration in the PACU,1,2 and factors associated with PACU length of stay.3,12–14
The baseline characteristics of those who had a postoperative RRT activation are similar to those described in the literature, representing an older and more comorbid patient cohort.7,15 The observed incidence and causes of postoperative RRT activation—primarily cardiovascular and respiratory—are also similar.7,15
Interestingly, our multivariate model found that patients who did not receive a general anaesthetic were more likely to have a postoperative RRT activation than those who did. Previous studies have demonstrated that neuraxial anaesthesia may reduce postoperative complications and ICU admission. 16 In our cohort, we speculate that the use of neuraxial or regional anaesthesia techniques may indicate a group of patients in which general anaesthesia was intentionally avoided due to high perioperative risk, although we are unable to confirm this.
Furthermore, our model also identified that vascular surgery patients—a traditionally high-risk group—were less likely to have a postoperative RRT activation compared to the reference group. In our cohort, the majority of these patients were undergoing minor peripheral surgery and were lower risk patients as critical care support immediately postoperatively was neither anticipated nor required. The increasing use of endovascular techniques may also have contributed to this finding.
Strengths and limitations
Our study featured a large cohort of patients over a recent two-year period, allowing for more detailed outcome analysis and improved recognition of clinically relevant differences in the data. In addition, the cohort is a heterogeneous group of surgical patients, which improves the generalisability, and allows the conclusions to be applied to most patients in the immediate postoperative period.
We performed multivariate logistic regression analyses to account for the effect of measured confounders. RRs were derived from logistic regression models, rather than from the ratios of observed incidences, to permit comparison of univariate and multivariate analyses. We used multiple imputation to account for variables that were mostly, but not completely, recorded, allowing us to maximise the use of the available data. Multiple imputation generates a distribution of possible values for those that are missing, allowing the uncertainty of the true value to be reflected in our modelling.
Our study was conducted in a hospital with a well-established and extensively studied rapid response system,10,11 which increases the reliability of our conclusions. Furthermore, as perioperative time tracking is an integrated part of the recovery workflow, the timestamp data collected are very accurate and further strengthen our findings. As organisational and logistical factors can arbitrarily lengthen the PACU length of stay, 12 we chose to exclude time spent in the PACU after a patient was medically suitable for discharge to the ward.
Our study has some limitations. First, it should be noted that other, well-established predictors of postoperative deterioration were also strongly associated with postoperative RRT activation, including non-elective surgery, theatre length of stay, cardiovascular comorbidity and respiratory comorbidity. The additional diagnostic utility of PACU length of stay as a predictor of postoperative deterioration may be small. Furthermore, it is acknowledged that PACU length of stay as a univariate predictor of postoperative RRT activation has relatively poor sensitivity, specificity and positive predictive value (7.2%) when a one hour cut-off is used, due to the relatively infrequent occurrence of postoperative deterioration, and the relatively common occurrence of staying longer than one hour in the PACU. Any intervention based on PACU length of stay would therefore require a low resource implementation—such as an automated monitoring and alert system—or would need to be based on additional risk factors to improve the predictive value.
Second, it is a retrospective, single-centre study which may reduce the generalisability of the findings, but is partially offset by the large and heterogeneous patient cohort. Furthermore, as data from this study were collected over a two-year period, some patients are featured more than once in this dataset, which could introduce bias into our modelling. Our findings may not be generalisable to patients undergoing gynaecological surgery as these were very few and were excluded. Third, we selected RRT activation as our marker of clinical deterioration, which formed our primary outcome. While we acknowledge that deterioration occurs heterogeneously, our study primarily focused on deterioration associated with RRT activation. Fourth, the data were obtained from a clinical and administrative database, which may be prone to data collection, measurement or coding error. Importantly, complications were derived from ICD-10 codes and may not capture all events. In addition, our analysis is limited to the data available in our database, which did not include such variables as the American Society of Anesthesiologists (ASA) physical status score. This prevented us from reporting other acute health evaluation scores and perioperative risk indices, including the Surgical Outcome Risk Tool (SORT) score 17 and the Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity (POSSUM), 18 which may outperform PACU length of stay as a predictor for postoperative deterioration. Unmeasured confounders may better explain our observations and reduce the significance of our findings. Missing data and the assumptions made to address them may introduce bias into the model. Furthermore, to assess the effects of an unanticipated prolonged stay in the PACU, patients were excluded if they were anticipated to have a prolonged PACU length of stay or were anticipated to require postoperative HDU or ICU support, even if they did not eventually receive it. These patients are likely to be at elevated risk of postoperative deterioration but are not the focus of this study. Finally, we also chose to focus our analysis on patients who stayed less than five hours in the PACU by excluding those who infrequently stayed longer (N = 110). Initial analyses of this cohort were underpowered, and on further review, many were found to be coding errors. Furthermore, most of our patients stayed less than 3 hours in the PACU, and relatively few stayed longer (N = 415). Our results should be interpreted with caution in these patients.
Our findings may only apply to our patient cohort and may not be generalisable to patients in other hospitals and settings. Large, multicentre, prospective studies are needed to validate the associations described in this study.
Conclusions
In our hospital, an unanticipated prolonged PACU length of stay is strongly associated with early postoperative RRT activation (univariate OR per increment 1.57, multivariate OR per increment 1.41) and other markers of deterioration. Other identified predictors include non-elective surgery (OR 1.78), theatre length of stay (OR per increment 1.61) and Charlson Comorbidity Index score (OR per increment 1.09). It is possible that PACU length of stay, in conjunction with other risk factors, could be used as a measure to help in risk stratification and early intervention to prevent deterioration. Further research is needed to examine the identified associations in other hospitals, integrate PACU length of stay into predictive models for postoperative deterioration for patients who stay in the PACU for longer than one hour, and assess the potential benefits of proactive intervention.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X211059191 - Supplemental material for The association between unanticipated prolonged post-anaesthesia care unit length of stay and early postoperative deterioration: A retrospective cohort study
Supplemental material, sj-pdf-1-aic-10.1177_0310057X211059191 for The association between unanticipated prolonged post-anaesthesia care unit length of stay and early postoperative deterioration: A retrospective cohort study by Luke R Fletcher Conceptualization Data curation Formal analysis Investigation Methodology Project administration Resources Software Validation Visualization Writing original draft Writing review editing Timothy G Coulson Conceptualization Formal analysis Methodology Project administration Resources Supervision Visualization Writing original draft Writing review editing David A Story Formal analysis Project administration Resources Supervision Writing review editing Richard J Hiscock Data curation Formal analysis Investigation Project administration Supervision Visualization >Writing review editing Nada Marhoon Data curation Resources Software Writing review editing Justin M Nazareth Conceptualization Formal analysis Investigation Methodology Project administration Resources Supervision Visualization Writing original draft Writing review editing in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) declare that there are no additional acknowledgements.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.