
Abstract
There is a lack of published literature investigating the impact of anaesthesia-specific automated medication dispensing systems on theatre staff. This study aimed to investigate the perspectives of theatre staff from multiple disciplines on their experience using anaesthesia stations three years after implementation at our Western Australian quaternary hospital institution. A web-based survey was distributed to 440 theatre staff, which included consultant anaesthetists, anaesthetic trainees, nurses, anaesthetic technicians and pharmacists, and 118 responses were received (response rate 26.8%). Eighty-one percent of the anaesthetic medical staff responders reported that the anaesthesia stations were fit for purpose and 66.67% of the anaesthetic medical staff reported that they were user friendly. Sixty-seven percent of anaesthetic medical staff agreed that controlled medication (e.g. schedule 8 and schedule 4 recordable) transactions were more efficient with the anaesthesia stations, and 66.67% agreed that the anaesthesia stations improved accountability for these transactions. Sixty-seven percent of anaesthetic medical staff preferred to use anaesthesia stations and 21.2% of all the responders preferred a manual medication trolley (P ≤ 0.001). This survey of user experience with anaesthesia stations was found to be predominantly positive with the majority of theatre staff and anaesthetic medical staff preferring anaesthesia stations.
Keywords
Introduction
Medication errors cause significant morbidity and occasional mortality to patients worldwide, and increase healthcare costs and hospital lengths of stay.1–3 In Australian hospitals, medication errors have been reported to occur in 71%–85% of inpatients. 4 In operating theatres, multiple studies have investigated anaesthetic medication errors and ‘near miss events’ (where an error was detected before it caused harm). The incidence of such events is described as occurring in one in every 133–450 medication administrations.5–7 Technology that improves medication safety can assist by reducing medication errors and patient harm.
One way medication errors can be reduced is by the use of anaesthesia-specific automated medication dispensing systems (anaesthesia stations; A-stations). These can reduce the risk factors for medication error, particularly by improving documentation. 8 These systems incorporate a computer with medication storage. Access requires a password or bio-identification to remove individual medications, with all transactions recorded against the user, improving accountability. This can potentially satisfy relevant legislative requirements for managing controlled medications (e.g. schedule 4 recordable and schedule 8) avoiding the need for paper-based systems. A-stations allow easier access to these medications during surgical procedures by placing the device at the patient’s side. Medication safety is strengthened by standard medication layouts and colour codes for medication class and compartments to separate medications; however, this is not unique to A-stations and can be achieved through non-automated systems. High-risk medications can be stored in A-stations in sealed compartments that open only when the relevant medication is selected on the computer interface.
Our institution is a 783-bed metropolitan quaternary hospital in Western Australia providing elective, emergency, cardiothoracic, burns and transplant surgery. Thirty-eight anaesthesia-specific automated medication dispensing systems (A-stations, Figure 1), (BD Pyxis™ Anesthesia Station ES, Becton Dickinson, Franklin Lakes, NJ, USA), were deployed to all theatres and procedural areas across the hospital in 2016. The primary reason for implementation was to improve medication safety and governance within these areas. Each A-station contained all critical medications required for anaesthesia, including controlled medications requiring additional documentation as per state legislation and were located within the procedural area itself. This system replaced the use of manual anaesthetic medication trolleys inside procedural areas for the storage of non-controlled medications only. Centralised locked cupboards were used for storage of controlled medications and stock procurement for the procedural areas prior to implementation of A-stations.

A-stations. BD Pyxis™ Anesthesia Station ES (Becton Dickinson, Franklin Lakes, NJ, USA).
Following an initial user registration and identification process, the system is accessed using bio-identification combined with their hospital identification number, negating the need to remember and change written passwords. Anaesthetic medical staff (consultant anaesthetists, senior registrars/fellows and registrars) are the primary users of A-stations to remove medications, record transactions and administer medications to patients in theatres and procedural areas at our institution. Nurses may also remove and administer medications to patients from A-stations at our institution, although less frequently than anaesthetic medical staff. Nurses and anaesthetic technicians are responsible for the restocking of the A-stations, including controlled medications. The number of medication units (ampoules/vials) withdrawn from the A-station is recorded, including the ability to ‘waste’ any part not used, along with a designated witness to the process when required under Western Australia state law.
There is limited published literature regarding the experiences of theatre and procedural area staff with automated A-stations in useability, timely access to medications, perceived impact of medication errors and preference for manual or automated A-stations. We conducted a survey of these staff from multiple disciplines within the theatre setting regarding their experience of A-stations three years after implementation at our institution. The aims were to determine whether they preferred A-stations versus manual trolleys, to identify which features of A-stations were perceived as favourable or unfavourable and, when possible, to identify areas of potential improvement for the A-stations.
Materials and methods
A cross-sectional anonymous online survey using a combination of categorical questions, Likert scales (strongly agree through to strongly disagree) and open-ended questions was emailed to all theatre staff (SurveyMonkey, San Mateo, CA, USA). These survey questions are available as Supplementary material. Theatre staff were categorised as either ‘anaesthetic medical staff’, or ‘all other theatre staff (nurses, anaesthetic technicians and pharmacists)’. Anaesthetic medical staff predominantly utilised the A-station for direct patient care, and non-medical staff predominantly utilised the A-station for inventory management. Responses were collected over a period of four weeks, with reminder emails sent out by study investigators, during 2019.
Responses were analysed using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) and Stata Statistical Software: release 17 (StataCorp LLC, College Station, TX, USA). Categorical responses were analysed with a chi-squared test to assess if there were differences in responses based on the responder’s occupation or years of experience in anaesthetics. Statistical significance was designated a priori as P ≤ 0.05.
This study was approved by the institution’s safety and quality committee as a quality improvement project (GEKO 33530).
Results
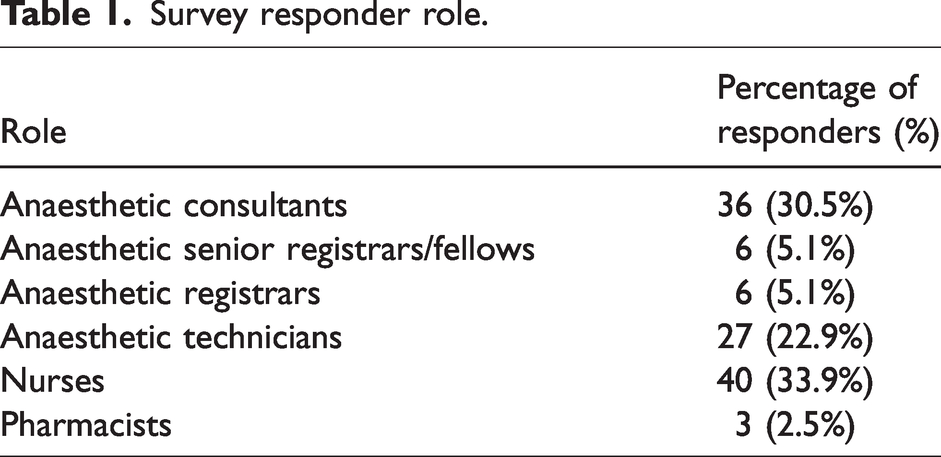
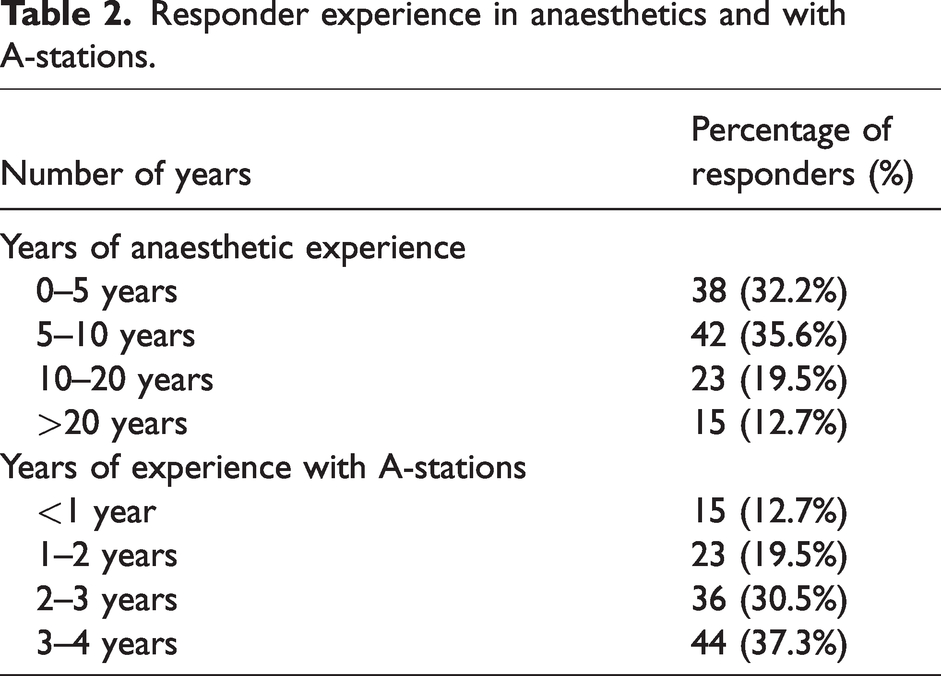
There was a 26.8% (118/440) overall response rate from theatre staff for the survey. Demographics of respondents are detailed in Table 1. Responses from anaesthetic medical staff represented 40.7% of the overall theatre staff responses. The remaining 59.3% of the responders were theatre nurses, anaesthetic technicians or theatre pharmacists. Thirty-two percent of the responders had less than five years of experience in anaesthetics, 35.6% had five to ten years, 19.5% had between ten and 20 years and 12.7% had more than 20 years. Table 2 details the responder’s experience in anaesthesia and with A-stations. The majority of the responders (67.8%) had more than two years of experience using the A-stations.
Survey responder role.
Responder experience in anaesthetics and with A-stations.
The overall grouped responses for each Likert scale statement are presented in Table 3. Questions 1 to 10 were directed at all the responders and questions 11 and 12 were directed at non-medical theatre staff (nurses, anaesthetic technicians and pharmacists) only. The majority of anaesthetic medical staff responders (81.25%) and all other theatre staff responders (85.71%) considered the A-stations to be fit for purpose. Sixty-seven percent of anaesthetic medical staff responders and 72.86% of all other staff responders found the A-stations to be user friendly. A similar percentage of anaesthetic medical staff responders (58.33%) and 60% of all other theatre staff responders agreed that A-stations allowed timely access to medications.
Responses to statements about A-stations in theatre.
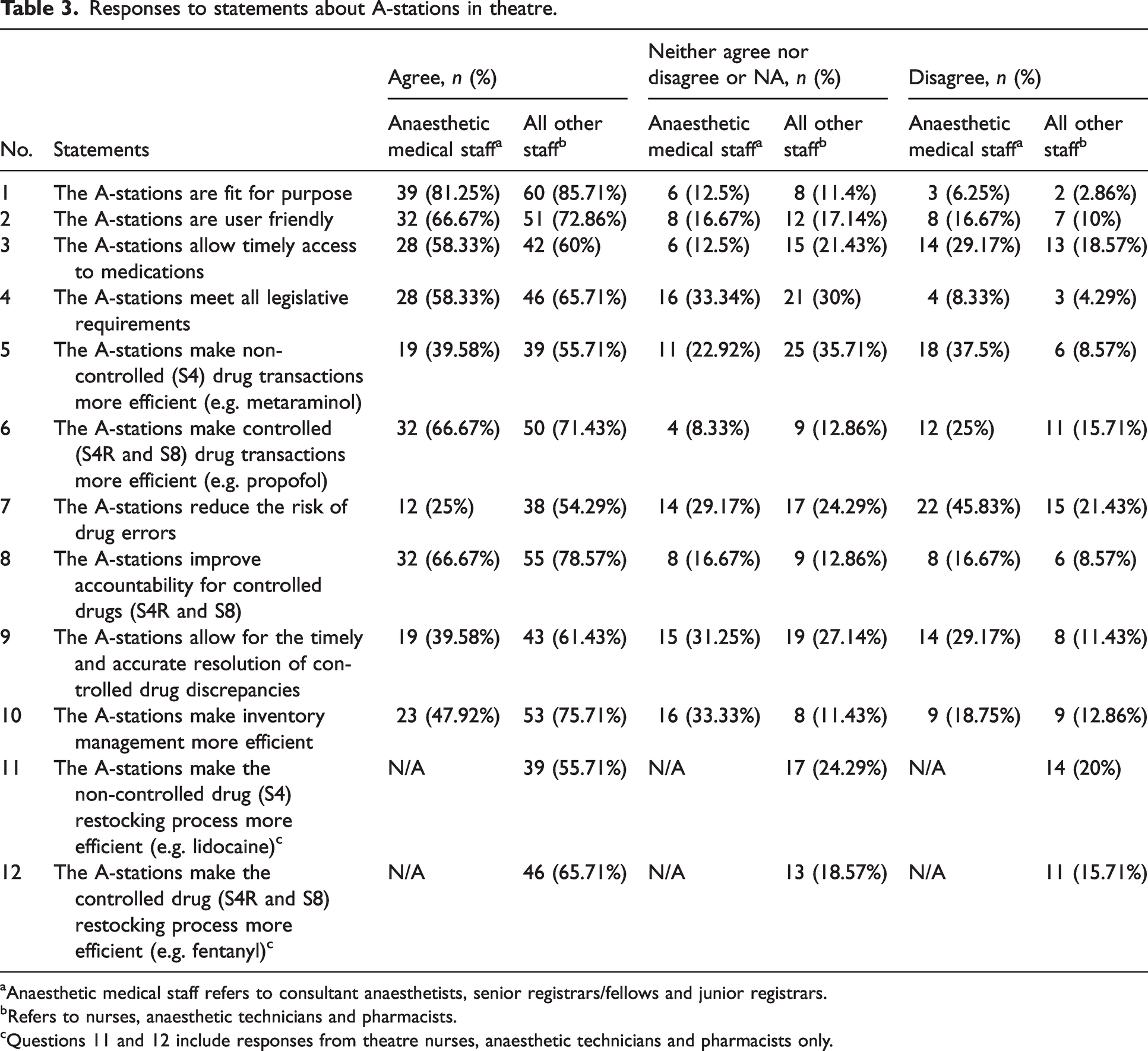
aAnaesthetic medical staff refers to consultant anaesthetists, senior registrars/fellows and junior registrars.
bRefers to nurses, anaesthetic technicians and pharmacists.
cQuestions 11 and 12 include responses from theatre nurses, anaesthetic technicians and pharmacists only.
Forty percent of anaesthetic medical staff responders and 55.71% of all other theatre staff responders agreed that the A-stations made non-controlled medication transactions more efficient (Table 3). Significant differences were observed based on the responder’s occupation and role (P = 0.047) and experience in anaesthetics (P = 0.014).
Anaesthetic medical staff responders were less likely to report that A-stations reduced the risk of medication errors (25%) compared to all other theatre staff responders (54.3%). Responses to the statement ‘The A-stations reduce the risk of drug errors’ varied significantly according to the responder’s occupation and role (P = 0.025), with more negative responses from anaesthetic medical staff (45.8% disagreed), compared to all other theatre staff of whom 21.4% disagreed (Table 3).
The statement ‘The A-stations allow for the timely and accurate resolution of controlled drug discrepancies’ had significant differences based on the responder’s experience in anaesthetics (P = 0.002); 68.4% of all the responders with less than five years of experience in anaesthetics agreed. The statement ‘The A-stations make inventory management more efficient’ had significant differences based on the responder’s occupation and role (P = 0.002) and experience in anaesthetics (P = 0.01) in which 47.9% of anaesthetic medical staff responders agreed and 75.7% of all other responders agreed. Seventy-nine percent of responses from those with less than five years of experience agreed. No statistically significant differences in the responder’s occupation and role or experience were observed in other survey questions.
Overall, 74.6% of all the responders preferred the A-station and 21.2% preferred a manual medication trolley (P ≤ 0.001). The variation of responses was not significantly different when comparing anaesthetic medical staff responders to all other theatre staff responders, in which 66.67% preferred the A-station compared with 80%. Table 4 displays the preference by the responder’s role.
Responders’ preference for A-stations.

The respondents made a total of 33 written comments, 24% were positive feedback regarding A-stations and 36% were negative. The remaining comments (39%) were not relevant to A-stations or were neutral. Most respondents who preferred the A-station commented that the A-station allowed safe, timely access to medications with greater accountability over controlled medications. Respondents who preferred a manual medication trolley mostly commented that their preference was due to the A-station negatively impacting timely access to critical medications in emergency situations (four out of eight responders).
The BD Pyxis Anesthesia Station ES at our institution was the first experience with automated A-stations in theatres for the majority of all staff surveyed (90.7%). Of the ten consultant anaesthetists who had prior experience with pharmacy automation in theatres, seven (70%) reported that the Pyxis Anesthesia Station ES at our institution was better, and the remaining three (30%) said it was about the same.
Discussion
This survey of user experience with A-stations was positive overall, with 81.3% of anaesthetic medical staff responders assessing A-stations as fit for purpose, while 67% found them to be user friendly. Eighty-six percent of all other theatre staff responders found the A-stations fit for purpose and 72.86% reported that they were user friendly. The majority of all the responders (74%) preferred the A-stations to manual anaesthetic medication trolleys. Our survey was conducted three years after implementation of the A-stations, allowing theatre staff adequate time to become familiar with using the devices.
A-stations have previously been demonstrated to reduce discrepancies in the management of controlled medications.9,10 Although more than half of anaesthetic medical staff and other respondents agreed that the A-stations met legislative requirements, fewer than 40% of anaesthetic medical staff agreed that A-stations allowed for the timely and accurate resolution of controlled drug discrepancies. This was in contrast to over 60% of other theatre staff. This difference probably reflects the fact that discrepancies at our institution involving anaesthetic medical staff tend to be more complex, and often rely on a paper anaesthetic record to document medication administration.
Published literature describing theatre staff experience with automated A-stations is scarce. Wang et al. 8 collected feedback from anaesthetists in China on their satisfaction of using an automated A-station compared with a manual medication trolley at the completion of each theatre case. Anaesthetists preferred to use the A-station, but the reasons why were not reported. 8 Merry et al. demonstrated that a multimodal approach to medication safety in the operating theatre, including customised medication trays, medication barcode scanning and an electronic anaesthetic record, was preferred by anaesthetists compared to the conventional approach. 11
A-stations are considered a strong medication safety approach and are therefore more likely to reduce medication errors compared to weaker approaches such as warnings and labels. 12 Wang et al. 8 also reported that using A-stations compared to manual medication trolleys demonstrated a significant reduction in medication errors (11.9% versus 7.3%, P < 0.01). However, errors of selection or omission remained similar in both groups. 8 At our institution, some medications (e.g. controlled medication, high-risk and high cost medication) are located in secure sections of the A-station that will open only when the user selects the specific medication. This contrasted with the transparent cover described in the study by Wang et al. 8 There is still the risk of selection error from the open sections in the A-stations at our institution, which may have contributed to anaesthetic medical staff responders being less likely to believe that the A-station reduces the risk of medication errors (25%) compared with all other theatre staff responders (54.29%). Multimodal approaches have demonstrated medication error reduction, including omission and look-alike medication errors in New Zealand and the USA.5,11,13,14
Potential safety issues with mixing different medications within the same drawer of anaesthetic medication trolleys have been described, such as the co-location of different vasopressors with similar ampoule size and shape. 15 Look-alike medication ampoules or medications with read-alike names have been linked to multiple errors, including nearly 40% of medication errors in a South African study in anaesthetics.6,7 A-stations have reduced these risks, with a dedicated section for each medication type/strength, and a colour-coded section for each medication as per the International Organization for Standardization standard for colours for medications used during anaesthesia. 16
Guidelines on the medication contents of anaesthetic medication trolleys are limited, with varied contents depending on the hospital and the type of procedural area or theatre. 17 Having a primarily standardised list and consistent layout of medications within the A-station at our institution may have resulted in more staff responding that A-stations improved medication safety and efficiency.
Our study has several limitations, including the low response rate of 26.8%, which may not reflect the majority of all theatre staff and may have been subject to participation bias, as well as low numbers of pharmacists in the theatre setting. Despite the low response rate, the proportion of the responders per user-role was similar to the proportion of transactions by user role recorded on A-stations during the survey period; anaesthetic medical staff comprised 34.76% of A-station transactions compared with 40.5% survey response rate, anaesthetic technicians 22.5% versus 22.9%, nurses 42% versus 33.9% and pharmacists 0.74% versus 2.5%. A-stations were also not integrated with an electronic medical record leading to barriers to managing medication discrepancies. The A-stations can also perform barcode scanning of medications. However, this feature was not implemented at our institution, reducing the opportunity to improve medication safety further. The majority of users only had experience of A-stations at the one institution and were unable to compare other systems. As a single-centre study, our results may not be generalisable to other settings.
This survey of user experience with A-stations was predominantly positive. Eighty-one percent of anaesthetic medical staff responders found the A-stations are fit for purpose and 67% reported that they were user friendly. Eighty-six percent of all other staff responders found the A-stations fit for purpose and 72.9% reported that they were user friendly. Three-quarters of all the responders preferred the A-stations to manual anaesthetic medication trolleys. Further investigation should explore these variations, including the role of A-stations in preventing medication errors, the addition of medication barcode scanning and the impact of integrating A-stations with the electronic medical record.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X221109614 - Supplemental material for A survey of operating theatre staff on the impact of automated medication dispensing systems in operating theatres in an Australian hospital
Supplemental material, sj-pdf-1-aic-10.1177_0310057X221109614 for A survey of operating theatre staff on the impact of automated medication dispensing systems in operating theatres in an Australian hospital by Emma C Fox, Jeanie Misko, Matthew DM Rawlins, Angela Cheaib, Yan Ghee Peng, Glenn R Boardman, Kenneth K Tam, Noelle M Freir in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.