
Abstract
There is a long history of prosthetic and orthotic services helping to mitigate the impact of physical impairment by restoring function, and enabling and equipping the user. The training of health professionals who design, fit, and maintain prosthetic and orthotic devices has evolved over the centuries, reflecting an increase in knowledge, technology, understanding, and social attitudes in each era. Improvements in pedagogical thinking and biomechanical understanding, as well as the advent of new integrated technologies, have driven the profession over the past 50 years to modernize, evolve training and service delivery models in line with new attitudes toward clients, and search for new ways to improve users’ quality of life. In this narrative review, the authors examined the evolution of prosthetic and orthotic education, the impact of changing educational techniques and technologies, and the impact of the International Society for Prosthetics and Orthotics in that process. Through conversations with experts and review of peer-reviewed literature, accreditation documents, and the International Society for Prosthetics and Orthotics records and databases, the authors identified three areas of change in prosthetics and orthotics education over the past 50 years: (1) prosthetic/orthotic curriculum content, (2) pedagogy and course delivery, and (3) internships/residencies. This narrative review is a snapshot of a growing profession and we can only speculate where the next 50 years will lead us as we strive to serve patients, ever placing their needs and aspirations at the center of this professional service.
History of prosthetic and orthotic education
Since the initial interregional seminar on standards for the training of prosthetists in 1968, efforts continue to improve the implementation and outcomes of prosthetic and orthotic (P&O) education to serve patient-specific needs. P&O leadership has engaged stakeholders in workshops throughout the world to continually reassess the status of P&O education and further develop the profession (Table 1). This article describes changes in P&O education worldwide, focusing primarily on efforts by the International Society for Prosthetics and Orthotics (ISPO) over the past 50 years and considerations as we progress forward in the next 50 years. Specifically, this article explores changes within these three major areas: (1) program and academic requirements from ISPO, (2) pedagogy and course delivery, and (3) requirements of internships/residencies.
Timeline of P&O education workshops.
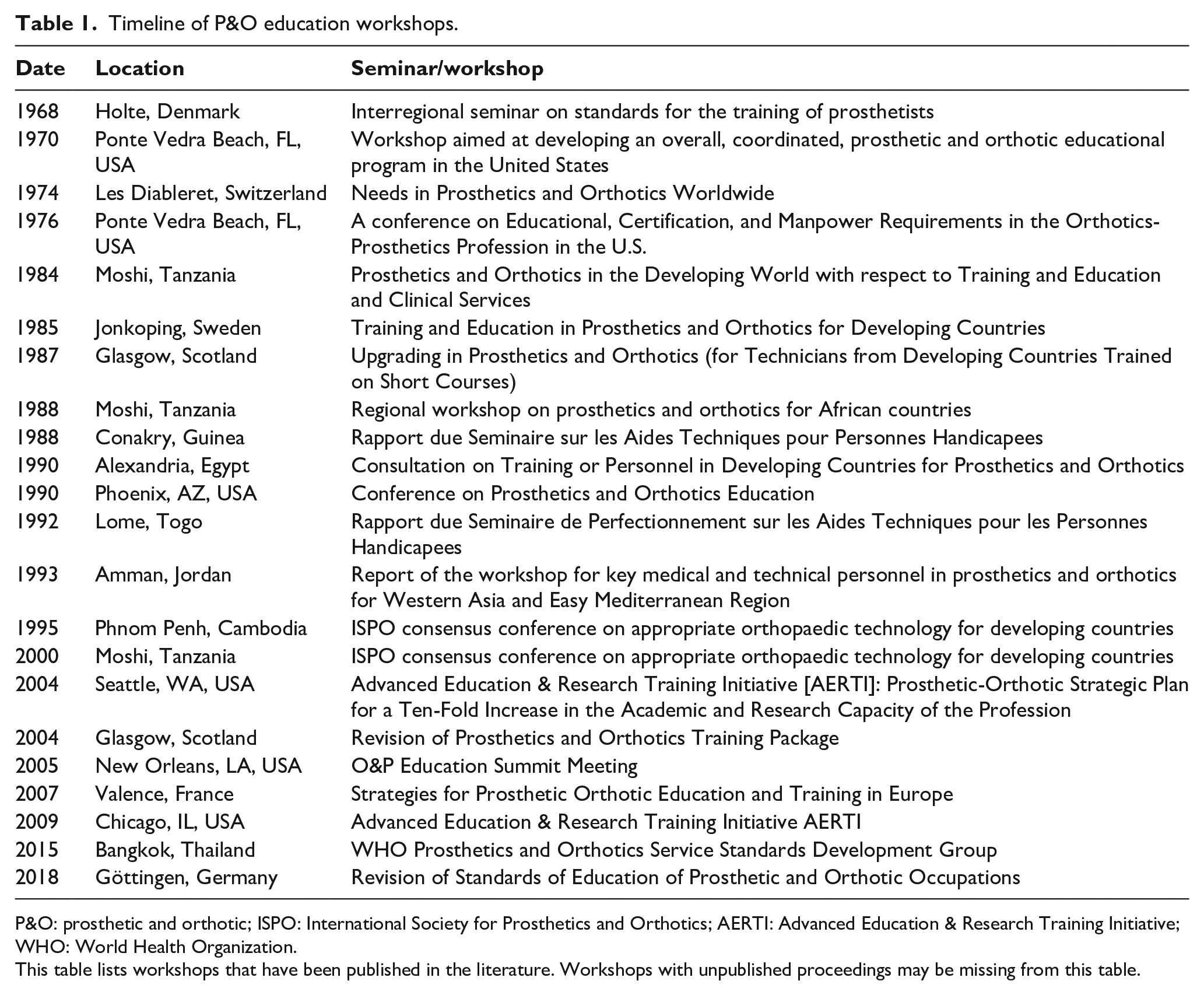
P&O: prosthetic and orthotic; ISPO: International Society for Prosthetics and Orthotics; AERTI: Advanced Education & Research Training Initiative; WHO: World Health Organization.
This table lists workshops that have been published in the literature. Workshops with unpublished proceedings may be missing from this table.
During the 1968 seminar in Holte Denmark, international researchers, clinicians and educators developed an outline to formalize P&O professional education.
1
The authors of the Holte report recognized that the professional contributions of prosthetists–orthotists were not generally understood, thus they made a concerted effort to define the roles of P&O professionals and to demarcate the distinct professional responsibilities between the prosthetist–orthotist and the P&O technician. They also emphasized the importance of research, and interprofessional collaborations with other healthcare professionals and engineers:
For the prosthetist, it is no longer sufficient just to know his trade since by virtue of his greater knowledge of medical aspects, he must cooperate with doctors and therapists. He must also be able to understand the engineer first of all to utilize the special knowledge of the engineer, secondly to be able to contribute to prosthetic/orthotic research. (Lynquist E.)
1
The prosthetist/orthotist who is educated in a college will not have the tasks of carrying out professional skills in a workshop, which will be done by a technician. But he will concentrate on the more complex duties of fitting and alignment on patients. (George S.)
1
In 1990, in Alexandria, Egypt, a World Health Organization (WHO) Consultation group advanced the Guidelines for training personnel in developing countries to provide P&O services. The Alexandria report defines the scope of practice and the education Guidelines for four levels of P&O professionals: the engineer (i.e. researcher), the prosthetist–orthotist, the assistant, and the technician. Role overlap was introduced between the prosthetist-orthotist and the PO assistant in order to address clinical needs in absence of trained prosthetists–orthotists in low and middle income countries (LMIC).2,3
Founded in 1970 as a multidisciplinary society, ISPO developed the most recent 2018 Education Standards 4 in parallel with the World Health Organization (WHO) Standards for P&O service delivery. The standards, which parallel the format of standards for other health professionals, define the core competencies for P&O professionals across the globe: prosthetist–orthotist (formerly Category I), associate P&O (formerly Category II) and P&O technician (formerly Category III). ISPO recognizes P&O programs internationally, some of which are in countries where national accreditation agencies do not exist. With the publication of the 2018 Standards, 4 ISPO acts as a program auditor and offers “accreditation” both in high income countries (HICs) and LMICs. Prior to 2018, education programs were only “recognized.”
The scope of practice defined by the three levels of P&O professionals has remained consistent over time (Table 2), but P&O education has changed over the years. Through conversations with experts and review of the peer-reviewed literature, accreditation documents, and ISPO records and databases, the authors identified three major areas of change in P&O education worldwide over the past 50 years: (1) prosthetic and orthotic curriculum content, (2) pedagogy and course delivery, and (3) internships/residencies.
Changes in descriptions of P&O professionals over time.
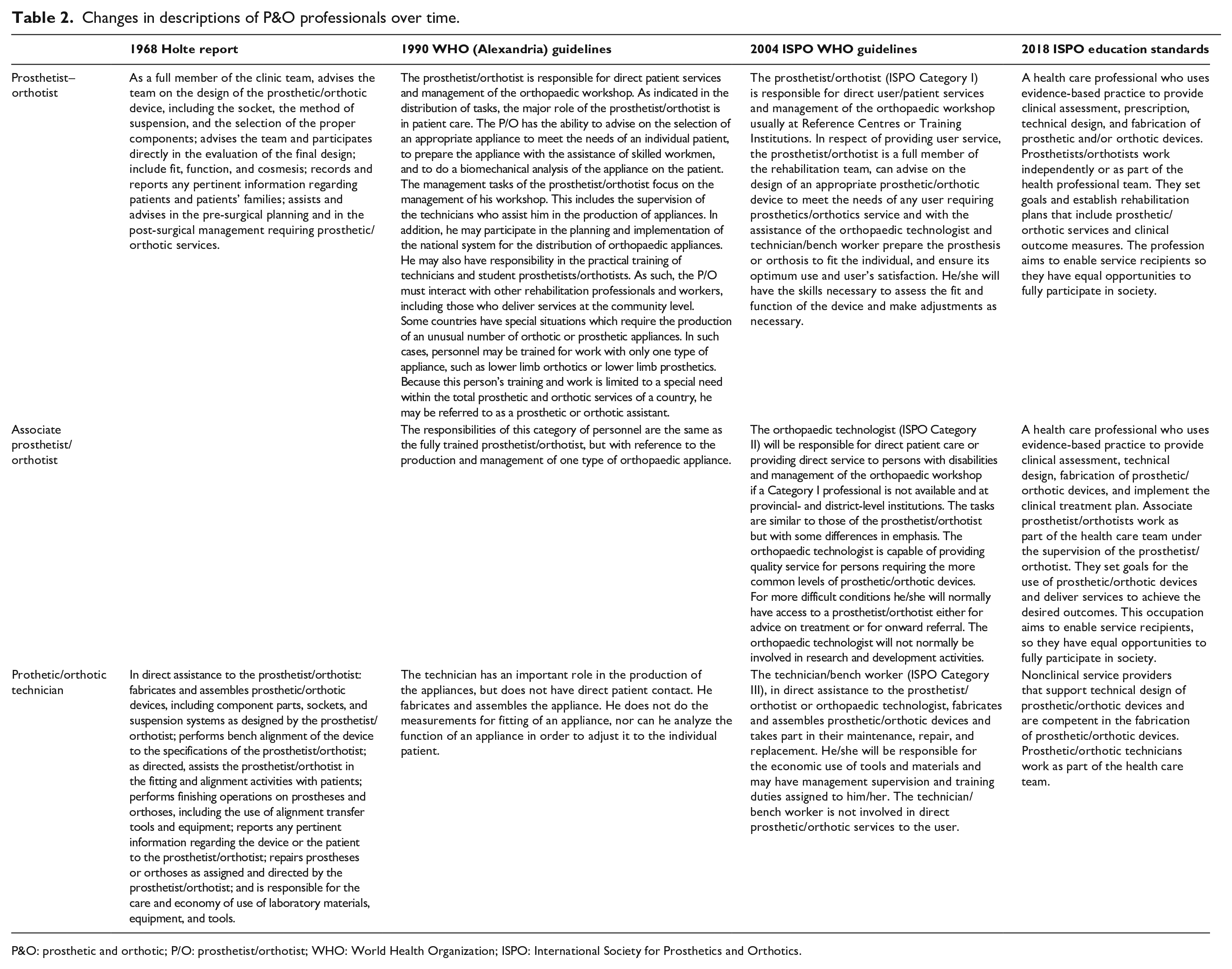
P&O: prosthetic and orthotic; P/O: prosthetist/orthotist; WHO: World Health Organization; ISPO: International Society for Prosthetics and Orthotics.
Prosthetic and orthotic curriculum content
Accreditation of P&O education has followed a path similar to that of other health professions, moving from a focus on structure and content to process and outcomes. With this movement toward competency-based professional standards, academic programs design curriculum to achieve required competencies rather than specific courses. Competencies are defined as
the cluster of related knowledge, skills, and abilities that affects a major part of one’s job (a role or responsibility), that correlates with performance on the job, that can be measured against well-accepted standards, and that can be improved via training and development.
5
Early P&O education Guidelines listed the specific courses, and laboratory and clinical practice experiences necessary to prepare P&O graduates to perform job-related responsibilities. The description of specific courses expanded with each revision until the establishment of the 2018 ISPO Education Standards
6
and the WHO Standards
4
in P&O Services. This change did not signify a reduction in educational content. Rather, compared with the earlier Guidelines, the 2018 Standards more closely align with other health professionals in format, and with the P&O professionals’ scopes of practice, leaving the specific pathway of how to prepare students for clinical practice to each program’s discretion. The Standards include professional competencies that align with societal health goals, including equity, quality, and efficiency. Furthermore, they define global standards as listed in the International Qualifications Framework
7
to facilitate the assessment of the national and international comparability of qualifications. The movement toward international standards aligns with the suggestion from the Lancet Commission Report:
the importance of global principles with context specificity is ever more relevant for professional education in our mobile and interdependent world. Global principles would bring consistency, transparency, and open accountability to the accreditation process, while easing the emergence of communities of knowledge and practice. Achievement of some global–local balance is a priority, indeed a necessity, as institutional interdependence grows.
8
Competency-based accreditation standards also enable programs to adapt to regional variations.5,8 While P&O programs from a range of regions have substantial consensus regarding the importance of program objectives dealing with student abilities, professional skills, and contemporary understanding, several regions highlight distinctive objectives, such as management and supervision in the Middle East and Southern Asia, internationalization in Europe and Southern Asia, and information and communication technology in Oceania P&O programs. 9 The ISPO Standards are adaptable to local educational needs.
Pedagogy and course delivery
Curriculum provided through multiple strategies and technologies foster students who are engaged, and can subsequently retain and demonstrate knowledge. Health education is often viewed as being static and providing fragmented, suboptimal education to students. 10 However, P&O programs across the globe use varying teaching strategies. HICs tend to put the responsibility of learning on the student, whereas the faculty in LMICs guide students more carefully under supervision. 11 The internet also offers a plethora of resources for educators and students. As faculty embrace these resources and use them, in addition to more traditional textbooks and laboratory manuals, students learn to be resourceful and creative in their approach to learning and to patient care. 10 The most notable change in recent times is the ability to reach different audiences through communication technology, specifically video conferencing software such as Zoom (Zoom Video Communications, San Jose, CA, USA) or GoToMeeting (LogMeIn, Inc., Boston, MA, USA) and e-learning platforms such as Canvas (Instructure, Salt Lake City, UT, USA) or Blackboard (Blackboard, Inc., Washington, DC, USA). To provide meaningful learning, faculty who design curriculum are encouraged to select strategies that match the learning objectives as well as the students’ learning styles, experiences, and interests.10,12
Many teaching strategies exist, some long-standing and some more current and innovative, each with levels of success commensurate with the amount of preparation by faculty and the amount of enthusiasm with which they are delivered. One example, problem-based learning (PBL) puts the obligation of learning on the student, while the faculty role becomes that of a facilitator. Principles of PBL are collaboration, self-directed learning, and student-centered learning; it uses small group discussion and debate, generally to problem solve and answer a clinical question.12,13 It is most ideal when case based, guiding students through the clinical decision-making process, and when they show mastery of the material. This clinical focus has been shown to result in improved retention and clinical skills, as case scenarios simulate what the students will encounter once they begin practicing. 13
Clinical and technical training prior to internship or residency is a component of all P&O programs and varies in length, location, and intensity. 12 This training may occur by using volunteer patient models and/or in clinics under the mentorship of practicing clinicians providing for an even more valuable learning experience.14,15 Hands-on laboratory work occurs in both locales to complement didactic and clinical work.
Internship (or residency)
Internships are the real-world learning experiences required prior to graduation and/or prior to becoming certified/licensed as a prosthetist–orthotist, associate P&O, and P&O technician, depending on the education pathway and national requirements. Although clinical internships have always been an important component of P&O education,1 –4,6 a noticeable shift is the recognized need for structure and a common set of requirements.6,16 Internships provide opportunities for students to respond to frontline service, work in various clinical/laboratory settings, and understand business operations and different models of P&O service provision and funding. 17 In the past, time in the clinic without clear expectations was the norm and led to varied experiences for students. P&O internships are in the process of changing to include clear expectations and oversight. Following a competency-based education model, clinical and technician students demonstrate their ability to perform common learning outcomes and professional competencies, as set forth by the program and/or accreditation agency. Students receive formative feedback about their level of competence and independence.
Clinical internships have been shown to be essential when the academic program is delivered online. 18 As a single discipline (i.e., prosthetics or orthotics) or dual discipline (i.e., prosthetics and orthotics) internship, they provide opportunities for collaboration between the interns and programs with host institutions to facilitate development of both soft and hard skills. 19 Aligning the prosthetist–orthotist and associated P&O clinical skills within the health professions is important as rehabilitation interventions shift with the growing global need of assistive and rehabilitation technology.6,20 Development of professional integrity and ethical practice with equity, diversity, and inclusion principles have all been identified as highly valuable qualities in P&O practice 4
Current state of prosthetic and orthotic education
Approximately 140 clinician (prosthetist–orthotist and associate P&O) programs and 17 P&O technician programs currently exist worldwide. Of these, 35 P&O programs, 16 associate P&O programs, and 1 P&O technician program have been accredited/recognized by ISPO. The current ratio of accredited or unaccredited clinician (prosthetist–orthotist and associate P&O) programs to technician programs is 8:1. If we assume the number of students graduating from these programs is somewhat equivalent, this ratio is opposite to that suggested by the 1990 report, 2 2004 3 guidelines and the 2018 standards, 4 which range between 1:1 and 1:5. Although the number of P&O technicians is underrepresented as many are trained “on the job,” there remains a need for trained technicians to reduce the inefficiency of prosthetists–orthotists and associate P&Os tasked with technical work.4,17,21 Further inefficiencies to P&O clinical care occur when associate P&O in LMIC take responsibility for roles in physical rehabilitation interventions, out of necessity, when other rehabilitation members such as, P&O technician, occupational therapist, physical therapist, rehabilitation doctor, shoemaker, or podiatrist, are unavailable.
The ratio of ISPO accredited prosthetist–orthotist programs to associate P&O programs is 2:1, with a ratio of 27:1 in HICs and 8:15 in LMICs. Only China and Germany have both levels of ISPO-accredited clinician programs within their countries. More P&O users could be treated per team with associate P&Os working under the direction and supervision of the prosthetist–orthotist.4,21 In addition, the capacity of some graduates is underutilized due to lack of resources or poor organizational capacity. 21 Although this is a service delivery issue, it is recommended that P&O education systems respond to the lack of resources by providing more associate P&O graduates to support prosthetists–orthotists.16,17 In addition, training of prosthetists–orthotists might include leadership skills to communicate effectively and manage P&O associates and technicians.
Graduate and employer surveys provide useful information to assess professional preparedness.21 –23 Recent P&O graduates report difficulties in biomechanics24,25 and clinical management of specific pathological conditions. 26 Some report feeling unprepared for rural working conditions 25 and many request continuing professional development.22,24,26 Graduates suggest that the teaching faculty need teaching qualifications and greater instruction on the use of technology,27,28 not unlike early recommendations for P&O instructors. 1 Graduates in HIC feel strongly that their technical skills are essential to their role; 22 while graduates in LMIC report difficulties when working in clinics with lack of infrastructure17,29 and when there is low awareness and prioritization of P&O services.26,29
Consideration for the coming 50 years
P&O professionals have a unique combination of knowledge and skills that require substantial clinical and technical judgment. Early and ongoing challenges of P&O education include the need for additional clinical and education research;1,2,30 –32 a stronger foundation of scientific knowledge; 31 a more evidence-based approach to applying new technology and materials: more explicit competencies and self-assessment of education standards; 33 increased level of education; 34 enhanced sustainability and cost-effectiveness of P&O education programs;1,33 improved coordination and communication between P&O providers and education institutions;34,35 improved legislation affecting persons needing P&O services; 34 and more P&O professionals.33,36
The ISPO accreditation 2018 Education Standards 6 established a new level of professionalism that encourages common attitudes, values, and behaviors as the foundation in clinical service. They also promote common P&O knowledge, skills, and evidence-based practices. The following statements are considerations for the coming 50 years to prepare students for the realities of clinical service, teamwork, leadership, and lifelong learning (Box 1). 8
Areas of consideration for the coming 50 years.
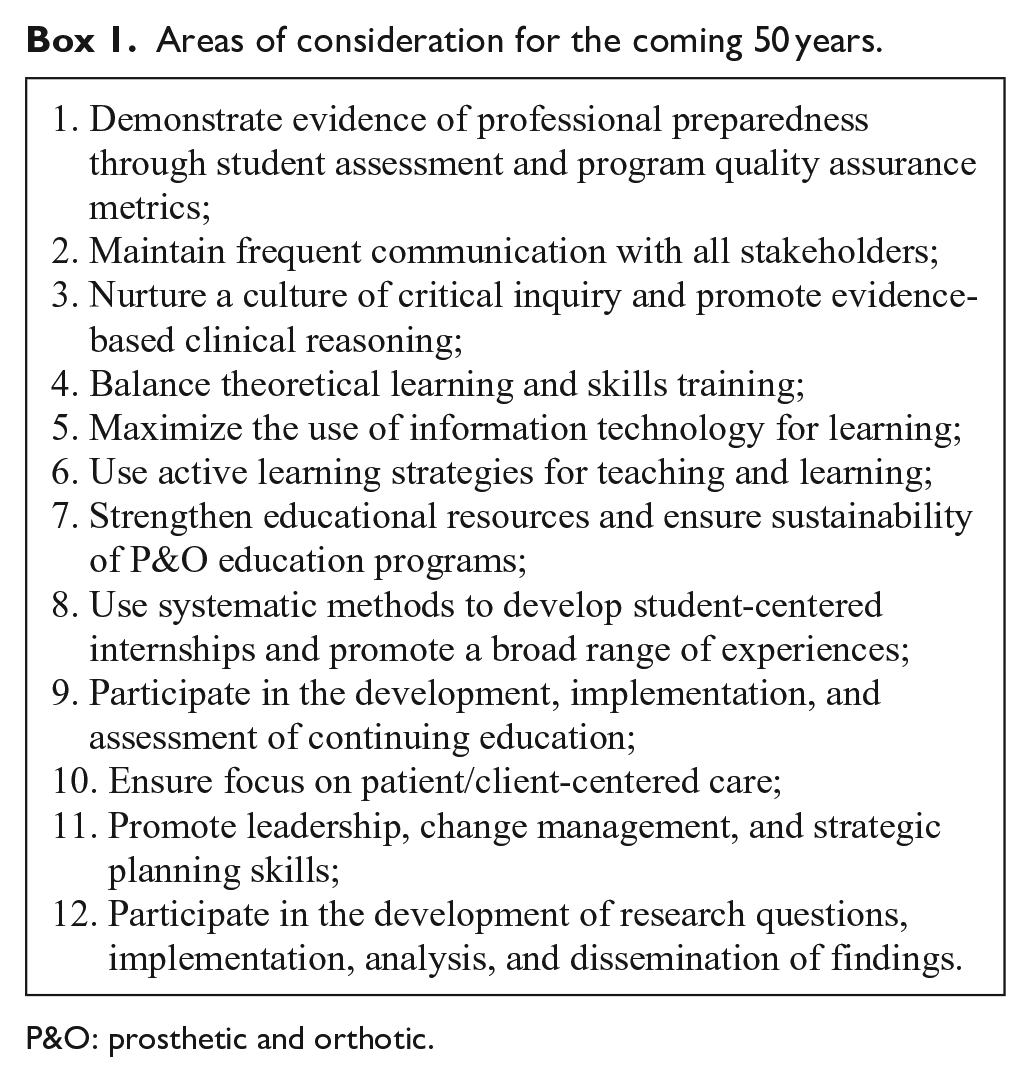
P&O: prosthetic and orthotic.
Demonstrate evidence of professional preparedness through student assessment and program quality assurance metrics
P&O education accreditors are beginning to require evidence of professional preparedness and program outcomes with reliable evaluation methodologies. 6 P&O education needs effective educational assessment tools to evaluate and demonstrate program outcomes, as well as student learning outcomes in each competency area. 37 Once the program selects appropriate tools, it can systematically gather and monitor outcomes at five levels of quality assurance: student learning within courses, student learning across courses, individual courses, programs, and the institution. 38 The WHO suggests that institutional-level quality assurance metrics address the teaching staff needs; equipment and teaching methodologies; learning environments; curricula to match the realities of local environments; and the promotion of a culture of social accountability. 39 Program, course, and student-level outcomes may improve as more P&O instructors become involved in accreditation procedures, critical assessment of program outcomes, and self-assessment of teaching methods. Additional resources on assessment methods are available.7,38,40 –42
Maintain frequent communication with all stakeholders
Frequent and transparent communication among stakeholders such as health employers, credentialing agencies, interprofessional colleagues, and educators will continue to be essential. Communication between educational institutions and health employers is necessary to align program goals with population healthcare needs.8,39 Systematic implementation and analysis of graduate and employer surveys provide valuable feedback about professional preparedness,21 –23 and can be used to adapt program competencies for local needs. 43 Educator–employer communication may be further enhanced through advisory meetings with stakeholders, continuing education efforts, collaborative research projects, and development of clinical cases for student learning. In addition, communication with credentialing agencies may inform educators about challenging content for graduates.
A notable benefit of the small scale of the P&O community is the potential to connect with educational institutions worldwide. ISPO Global Educators Meetings 44 provide opportunities for educators to share academic materials, strategies and challenges, (e.g., curriculum resources, didactic materials, student and program assessment tools, technology transfers, models of care concepts, standards of operation, and quality assurance approaches). They also serve as a means to connect students and faculty internationally through placement holding, exchange programs, or online instruction.
Health care is increasingly multidisciplinary and collaborative. P&O health care professionals recognize the need to further strengthen relationships with other health disciplines to improve communication for clinical services, and to reduce delays and service gaps.1,6,17 While in school, interdisciplinary education could focus on learning general competencies, such as communication, leadership, and evidence-based practice skills 8 together, so as to better reflect the situations students are likely to encounter after graduation.
Nurture a culture of critical inquiry and promote evidence-based clinical reasoning
“Critical inquiry is crucial to mobilise scientific knowledge, ethical deliberation, and public reasoning and debate.” 8 Educators should promote critical inquiry through activities that involve synthesis of information from multiple sources that then lead to new ideas and deeper questions (inquiries) about a topic. This educational approach requires that students know how to use information technology to search, identify, and critically appraise literature; activities that enable a culture of lifelong learning. Consequently, this approach may enable development of students’ evidence-based practice skills and address graduates’ desire to critically analyze and be more discerning with prescription choices.25,45,46 In addition, this approach could mobilize P&O scientific knowledge as there remains a need for more scientific, 31 clinical,30,47,48 and educational 32 evidence in P&O.
In the future, P&O clinicians will need to make judgments based on expanding amounts of information and data. P&O students’ critical thinking skills have been shown to improve with P&O education. 49 To develop students’ clinical reasoning skills in a systematic way, students could use frameworks to map and compare variables that affect desired technical and functional outcomes.50,51 Once students identify a pathway to make clinical decisions about a case, they can explore how various contexts might alter the outcomes and, thus, the clinical decision. Finally, to further develop critical inquiry, educators could use prosthetic threshold concepts (i.e. content that is difficult to learn and changes the way one thinks about a concept) such as “how we walk,” “learning to talk,” and “considering the person” to enhance student understanding of difficult concepts. 52
Balance theoretical learning and skills training
In addition to the minimum competencies required by students in any health profession, P&O students must practice to be skilled in evaluation, fitting, alignment, aesthetics, and outcome assessment; and P&O technicians must be skilled with materials and fabrication. 4 With the addition of new technologies and techniques, there is never enough time in the academic schedule to cover everything. P&O clinician graduates report the importance of technical skills 22 and some employers complain that P&O clinician graduates have poor practical hand skills. Fabrication knowledge and skills (i.e. mechanical reasoning, material science, and psychomotor skills) will continue to be important foundations in P&O. Educators may explore educational theory from other professions to improve the efficiency of student learning and consider different academic pathways to create the right balance of theoretical and skills training.
Maximize the use of information technology for learning
Accreditation agencies do not dictate how curriculum is delivered, but instead focus on learning outcomes. 15 With the abundance of electronic information, schools now play a larger role than ever before in helping students access and use data to improve their own learning. Programs of the future will require information technology departments to manage connectivity and instructional technology experts to design virtual experiences, quality distance learning programs, and implement instructional strategies that align with future technologies. 8 The authors envision software applications, available to all P&O schools, that will allow for clinical simulations such as dynamic alignment including changing socket pressures and force couples throughout gait, orthotic corrective forces, prescription formulation, interprofessional communication, critical inquiry, and interpretation of outcome data.
E-learning, which takes multiple formats, not only enhances the learning experience but also affords learning opportunities to many across the globe. Open or distance learning was introduced in 1969 by the Open University in the United Kingdom. With advancements in technology, distance learning has morphed from hardcopy learning packets to synchronous and asynchronous delivery methods. E-learning can be used to support on-campus seated students through a learning management system for content management, or it can be used to communicate with and deliver curriculum to students at a distance. One P&O program recorded synchronous lectures to seated students for transmission to the distance learning cohort. 15 The 24/7 availability gives students the freedom to work from anywhere, anytime allowing for employment and cost-savings by not having to relocate.14,53 A blended model of electronic and face-to-face delivery can promote quality learning. 18 Even with face-to-face interaction, which can be live or via a conferencing system, e-learning benefits students by allowing access to demonstrations and lectures multiple times in preparation for exams without additional faculty resources. 53
Use active learning strategies for teaching and learning
Educators have limited time to provide increasing amounts of content and learning experiences to students. Thus, focusing on the selection of teaching strategies that match learning goals could maximize the learning outcomes. One engaging learning strategy that has a growing body of evidence is the use of simulations prior to actual patient contact.54,10 For example, by allowing students time to practice their psychomotor skills on models of hands or residual limbs, they are able to take their time and think through the task in a less stressful environment and are better able to transfer those skills to a live patient care session. 54 Game-based education simulation can complement other strategies while keeping students engaged. 10 Finally, providing immediate and authentic feedback is a teaching strategy to employ as often as possible.
Portfolios help students organize their thoughts, remain accountable, and structure their own learning environment. Students use portfolios to reflect and understand what and how they learned. 55 The problem-based learning approach has shown promise at improving students’ critical thinking about their own clinical and technical decisions after completing a research-informed clinical practice module. 56 Small group learning, where students are given the opportunity to share and contribute, can be more effective than traditional lectures. 12 Active learning includes discussion, role-playing, case studies, group projects, clinic and lab experiences, peer teaching, and debates to name a few. These strategies help students to build knowledge as faculty support their learning by adding on more difficult concepts. This helps students to become more competent and confident. When initially introducing theoretical material, better outcomes may be achieved by balancing a teacher-centered with a student-centered approach. 12
Strengthen educational resources and ensure sustainability of P&O education programs
Academic program resources will continue to be necessary instruments to achieve professional competencies. 8 For example, prosthetist–orthotist and associate P&O students must demonstrate basic skills in conducting research. However, graduates report challenges participating in research due to limited infrastructure. 28 Resources include personnel and human resources, physical facilities, budget allocation, student-support services, didactic and laboratory teaching tools and materials, communication technologies, and open access to journals. Furthermore, P&O graduate feedback has suggested that faculty need teaching qualifications.27,28 Programs could consider using a systematic process to track resources, for example, to ensure that faculty responsible for P&O-specific courses possess relevant teaching and clinical experience and have opportunities for professional development, 6 including the support of advanced degrees (i.e. MEd and PhD). Universities in the future will likely require teaching faculty with Master’s and PhD-level degrees.
Funding of P&O academic programs continues to be a challenge. The development of rich teaching resources, international partnerships, development of digital footprints of the program, preparedness for the market demand, and multiple sources of funding contribute to the sustainability of programs. The majority of P&O programs around the world have found accreditation useful. Other branding and positive images of programs may include international exchanges (educators and students, either South–South or North–South) with a focus on inclusion, diversity, and equitable opportunity, where programs could impact social changes and elevate the professional credential both locally and globally. The inclusion of different aspects of physical rehabilitation interventions and technologies equip students to respond to the needs of case management in real-world practice. 4 Furthermore, programs might consider participating in policy development, policy changes, and professional standards to set a professional footprint for national, regional, and global awareness.
Use systematic methods to develop student-centered internships and promote a broad range of experiences
Practical experiences in clinics or technical laboratories will continue to be an important aspect of P&O student learning. Universally, the learning outcomes of an internship (or residency) program are developed within the core competencies rubric evaluation. 6 Because each student enters their internship with differing strengths and areas for improvement, the balance of exposure to technologies, clinical experiences, and technical skills, as well as preparedness for employment, needs to be organized once a placement is set. To mitigate potential risks for an unsuccessful internship, the program can review its internship protocols with stakeholders (i.e. graduates, employers, supervisors, mentors, placement hosts, and users of P&O services) to assure common expectations. Repository resources to support the students could be helpful for interns, supervisors, and hosts to monitor and evaluate students’ progress.
The affective domain will continue to be important for healthcare professionals. When determining the level of oversight, clinical internship mentors (supervisors) report the value of interpersonal skills (e.g. recognition of personal limitations, self-evaluation, and reflection skills) and patient evaluation skills more than technical skills. 19 Reflective writing 57 and effective communication have been endorsed to enhance emotional intelligence, particularly over the placement period, where caseload management in real life could be made with qualitative analysis, on-time feedback, and debriefing techniques. Internship portfolios can be useful tools for in-depth analyses of learning with the use of reflective writing to enhance clinical decision-making skills and academic performance. 58
P&O internships of the future will include case conferences, case reflections, skill advancement appraisal, interprofessional communication, and systematic assessment of practice skills with regular constructive feedback from clinical supervisors and clinical mentors. This could contribute to 360-degree performance reviews and lifelong learning skills. In addition, advancements in technologies, e-learning, and e-health are seen to have a potential impact on how students conduct their internships. Thus, the inclusion and early introduction of these educational strategies in the academic programs would be helpful for students. Finally, systematic, documented internship outcomes and actual placement outcomes have been shown to be essential for the program to review its trend of internships, impacts, and effectiveness of clinical placement guidelines. As with academic program outcomes, internship outcomes needs to demonstrate how much students learn, and not how much instructors or mentors have taught (Outcome Based Education and Professional Competencies Performance). 6
Participate in the development, implementation, and assessment of continuing education
P&O professionals will need to continue to stay up-to-date with new technologies and techniques in order to maintain their skills and understanding of P&O after graduation. 21 In graduate surveys, P&O graduates often request continuing professional development (CPD).22,24,26 In low resource settings or where the national regulations on CPD are absent, educational programs and professional associations often take the lead and contribute to the development, implementation, and delivery of CPD. However, in many countries, the assessment and accreditation of CPD does not exist. Participation in the development, implementation, and assessment of CPD experiences could create potential national and international collaborations, and develop partnerships between education programs and employers. The projected increase in the number of people with disabilities 59 encourages both innovative models for training more students and advancing skills of current practitioners. E-learning, blended education, and distance programs have potential for the future upscaling of the number of practitioners and CPD activities in flexible learning environments at a reduced cost (capital and administrative). However, accreditation, quality assurance, and structured monitoring systems will continue to be essential for programs to safeguard the quality of education and to ensure patient safety.
Ensure focus on patient/client-centered care
The patient-specific context will continue to be paramount to the success of P&O interventions. So it is surprising that schools in only one region (N. Europe) reported it in their program objectives. 9 Patient/client-centered care is an overarching principle of clinical care 60 that needs to be integrated through all aspects of the P&O treatment plan. The patient-specific focus is an important focus of clinical care now and in the future; P&O educators should make this consistently explicit throughout the P&O curriculum.
Promote leadership, change management, and strategic planning skills
Leadership skills are vital for P&O professionals at all levels. Leadership skills promote integrity, stewardship, and accountability. 60 They are the foundation of interdisciplinary teamwork 5 and are necessary to advocate for the profession. 21 Thus, P&O programs can promote student leadership skills by threading teaching strategies that promote leadership behaviors throughout the curriculum. Furthermore, CPD training can provide graduates who are service managers with leadership, change management, and strategic planning skills. 21 These skill sets could provide opportunities for graduates to assume leadership positions, advance service delivery models, and participate in research. 4
Participate in the development of research questions, implementation, analysis, and dissemination of findings
The need for evidence in P&O has been repeatedly noted since the 1968 Holte report. A recent systematic review of education research found that 21 of the 25 identified articles were published in the past decade when searching back to 1966. The identified topics of research included (1) teaching/learning methods such as web-based and e-learning approaches, study abroad experiences, critical thinking development, and education strategies; (2) aspects of curriculum like interprofessional education and general curriculum development; (3) program-level topics such as competency standards, theoretical concepts, and graduate competency; and (4) country/region-level topics such as a description of current clinical practice and education and country-level outcomes. 32 The authors of that review reported a need for high-quality evidence to improve P&O education and to promote global advancement of the P&O profession. P&O educators at academic institutions and clinical/technical sites of the future will have more opportunities to take part in research at any stage. The advancement of P&O education and the profession requires professionals who are qualified and competent to conduct and lead research efforts.
Conclusion
Continued advancements in P&O education need to anticipate and reflect shifts in healthcare, 10 pedagogical thinking, technology, and student expectations. Accrediting agencies encourage innovation in education with a focus on competency-based standards and student learning outcomes. P&O programs of the future will implement systematic quality assurance metrics that demonstrate student learning of evidence-based practice skills, emotional intelligence, and discipline-specific cognitive (knowledge); psychomotor (skills); and affective (behavior) learning domains that contribute to quality patient care, clear communication with interdisciplinary colleagues, and advancement of practice standards. P&O education and the profession will advance through professionals who are qualified and competent to conduct and lead research efforts. Finally, consistent communication with all stakeholders will continue to be essential. Communication is important between educators, recent graduates, and clinical sites to ensure that learning outcomes remain relevant to changing technology and outcome-oriented healthcare environments; and communication with fellow educators is important to further develop innovative programs, research collaborations, and international partnerships for more equitable and inclusive efforts. Continued efforts toward cooperation and collaboration remain a challenge and a goal. 35
Footnotes
Acknowledgements
The authors thank Helen Cochrane, CPO(c), Dan Blocka, CO(c), FCBC, Nerrolyn Ramstrand, PhD, BP&O(Hons), and Sarah Anderson, PhD, MPH, BPO, for their helpful information for this manuscript.
Author Contributions
Conceptualization: SES, SK, SK, CH.
Acquisition of articles: SES.
Writing-original draft: SES, SK, SK.
Writing-review and editing: SES, SK, SK, CH.
Final approval of the version to be published: SES, SK, SK, CH
Declaration of Conflicting Interests
The author(s) disclosed no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed that they received no financial support for the research, authorship, and/or publication of this article.