
Abstract
Background:
Variables that influence orthotic and prosthetic patient outcomes beyond direct care are poorly conceptualized for orthotic and prosthetic students. Restructuring educational curricula around important clinical reasoning variables (i.e. factors that may influence outcomes) could improve teaching, learning, and clinical practice.
Objectives:
To propose an orthotic and prosthetic education framework to enhance the development of orthotic and prosthetic students’ clinical reasoning skills.
Study Design:
Scoping review.
Methods:
We conducted a scoping review, identified variables of orthotic and prosthetic usability, and performed a qualitative thematic analysis through the lens of orthotic and prosthetic clinical educators to develop a conceptual framework for orthotic and prosthetic education.
Results:
Sorting of variables identified from the literature resulted in three thematic areas: (1) the state of functioning, disability, and health (International Classification of Functioning, Disability and Health); (2) orthotic and prosthetic technical properties, procedures, and appropriateness; and (3) professional service as part of orthotic and prosthetic interventions. The proposed orthotic and prosthetic education framework includes these three areas situated within the context of patient-centered care.
Conclusions:
A conceptual framework was developed from variables identified in peer-reviewed literature. This orthotic and prosthetic education framework provides a structure to explore orthotic and prosthetic clinical reasoning and advance our teaching and assessment of students’ clinical reasoning skills.
Clinical Relevance
The proposed orthotic and prosthetic (O&P) education framework is intended to promote conversation about variables (e.g. health condition, procedures, services, and O&P principles) that influence O&P clinical practice outcomes and further advance our teaching and assessment of students’ clinical reasoning skills.
Background
The success of orthotic and prosthetic (O&P) interventions depends on the clinical reasoning practitioners use to integrate their technical expertise with knowledge of the patient-specific context.1–4 Clinical reasoning is defined as a “complex cognitive process leading to meaningful interpretation of patients’ problems and formulation of an effective management plan.” 5 Across health care, problems with clinical reasoning occur due to lack of knowledge and flaws in data gathering, data processing, and metacognition.5,6 One difference between expert and novice clinical reasoning skills is the ability to mentally categorize information in a logical manner. 7 A conceptual framework that illustrates decision-making variables may broaden perspectives, 8 thereby serving to facilitate information gathering, processing, and synthesis.
Health care models and frameworks, such as evidence-based approaches9,10 and social determinants of health,11,12 provide a structure for advancing O&P clinical practice and expanding the complexity of clinical reasoning. To help students integrate and apply principles from potentially useful health care frameworks, educators must be explicit about the variables that influence clinical reasoning (e.g. health condition, culture, available technology, clinician’s experience) and their potential impact on patient outcomes. One such framework, the International Classification of Functioning, Disability and Health (ICF), provides a conceptual basis for health and disability and illustrates interactions of patient-specific characteristics across several domains. 13 The ICF categorizes assistive products and technology as static devices within the environmental domain. Researchers have used the ICF to evaluate the impact of O&P interventions on patient outcomes14,15 and organize O&P outcome measures.16,17 For orthotists and prosthetists, the ICF provides the patient-specific context for formulation of a treatment plan; however, the current ICF perspective that the environmental factors encapsulate O&P interventions, fails to acknowledge the clinical reasoning variables that are important for designing, implementing, and evaluating O&P interventions that meet patient-specific needs.
Research efforts have identified important O&P clinical reasoning variables;3,18–22 however, no O&P-specific framework exists to organize these variables and their interactions into a coherent education paradigm for students. Schaffalitzky et al. 3 recommend using a checklist to formulate and evaluate prosthetic prescriptions. Organizational tools such as checklists can be useful to guide O&P students in gathering patient evaluation information. However, checklists do not illustrate the complex interactions between the patient, the O&P intervention, and associated services that affect health care outcomes and are thus useful but insufficient. Instead, these interactions require clinical reasoning skills such as critical thinking, interpretation, and reflection about evaluation findings. 23 A conceptual, education framework would provide a structure to illustrate the complex interactions and relationships that clinicians consider when developing O&P treatment plans.
Conceptual frameworks combine theoretical assumptions, rules, and principles to organize ideas and illustrate complex issues. For example, frameworks may be used to evaluate problems through a specific perspective or lens. 24 The use of conceptual frameworks in clinical education is well-established8,25,26 and particularly valuable for novices to (a) explicitly define variables that may influence outcomes; (b) prioritize variables that directly or indirectly influence outcomes; (c) illustrate interactions between variables, interventions, and outcomes; and (d) examine how changes in practice may affect outcomes.24,27,28 An O&P education conceptual framework would structure and guide clinical reasoning by helping students identify clinical variables and explore their interactions.
Because little is known about clinical reasoning skill development in O&P education, a scoping review is particularly useful to provide evidence to support a conceptual framework. Scoping reviews have been used to develop frameworks in speech language pathology, 29 post-acute care rehabilitation, 30 and occupational therapy. 31 Scoping reviews target the breadth (rather than depth) of knowledge in a particular area or discipline and synthesize findings from different types of studies. The purpose of this project was to propose an O&P education framework to enhance the development of O&P students’ clinical reasoning skills. Such a framework can promote conversations about O&P clinical reasoning, advance our teaching of students’ clinical reasoning skills, and help evaluate O&P educational curricula. The proposed O&P education framework is intended to serve as a tool for O&P students and educators to organize and analyze variables that may affect the use of O&P interventions.
Methods
To develop our conceptual framework for enhancing clinical reasoning skills within O&P education, we conducted a scoping review to identify and collate variables that influence outcomes in O&P. We did not attempt to evaluate the methods or quality of available research, but rather used an iterative and narrative approach to extract variables of interest. As outlined below, our scoping review closely follows the five-stage method developed by Arksey and O’Malley 32 and enhanced by Levac et al. 33
Stage 1: the research question
The specific aim of the scoping review was to identify and collate common variables (e.g. health condition, procedures, services) that may influence O&P clinical outcomes. For this project, we defined “clinical outcomes” as the “usability of interventions.” The International Organization for Standardization (ISO) 9241-11 defines usability as: “the extent to which a product can be used by specified users to achieve specified goals with effectiveness, efficiency and satisfaction in a specified context of use” 34 Therefore, we considered O&P device use (i.e. the extent to which a patient can use O&P interventions) as a broad concept related to optimal clinical outcomes. Our scoping review addressed the following research question: What variables determine O&P device use?
Stage 2: identify relevant studies
An initial literature search was conducted between February–May 2015. We searched all English-language articles using the following keywords and medical subject heading terms: “usability,” “abandonment,” “benchmark,” “orthosis,” “orthotic,” “prosthesis,” “prosthetic,” and “artificial limb.” Additional articles were identified by hand searching reference lists. A second follow-up search of all English-language articles from July 2015 to June 2018 helped ensure inclusion of additional literature by using the search phrase: (((usability OR abandonment OR benchmark OR satisfaction) AND (orthosis OR orthotic OR (limb prosthesis) OR prosthetic OR (artificial limb)) NOT (dental OR orthopedic OR denture OR operation OR case OR breast OR surg*)).
Stage 3: article selection
We only reviewed articles that evaluated O&P usability. These evaluations used various methods, including patient surveys, Delphi studies, randomized control trials, and case reports. To be included in the review, studies had to (1) be related to O&P services and (2) report the effectiveness, efficiency, or satisfaction of O&P services. Studies were not excluded or evaluated based on methodological quality or study design.
Stage 4: charting the data
Two authors reviewed the selected articles and identified variables investigated in association with O&P device use. The data charting form used to record information from our article review included the following details: author(s), year of publication, purpose of study, study populations, methods of data collection, study design, outcomes of interest and outcome measures employed, specific usability variables, and the source from which the data were collected (i.e. patient, provider, or both). We compiled a list of variables that were used to investigate usability, but we did not draw any conclusions regarding the magnitude of association or causality between each variable and device use.
Stage 5: collating, summarizing, and reporting the results
After charting the data, the identified variables were collated into general themes using qualitative thematic analysis. Using this approach, two experienced O&P educators at the same O&P institution independently sorted the related variables into general themes. Independent grouping of variables were then merged, and any discrepancies about the sorting were discussed among the research team to achieve consensus. Frameworks (e.g. ICF) and outcome measures (e.g. Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0), Orthotic and Prosthetic User Survey (OPUS)) from the articles under review helped guide the initial categorization of identified variables. The themes were further refined by frameworks and clinical philosophies that inform our own clinical and education reasoning (e.g. patient-centered care, 35 interdisciplinary care 12 and contextual fit 36 ). Ultimately, we organized the identified variables that determine O&P device use into broad themes.
Next, through an iterative process, we identified and charted all variables and further defined the framework areas. We independently reviewed articles and then collectively discussed if and where the variables fit into each broad framework area. Through an iterative process, we further organized the variables by (1) subdividing professional service and (2) differentiating between the patient and provider perspectives based on whether the source of the data was patient, clinician, or both. The variables were grouped into categories within each area; each category was operationally defined and assigned a code. The final two steps of Stage 5 included summarizing and reporting the results to address our overall purpose of developing an O&P education conceptual framework. These final two steps are described in the Results section.
Results
The initial search yielded 106 articles. We excluded 78 articles that did not include a description of usability of O&P services. Eleven additional articles were identified through a subsequent review of reference lists, for a final pool of 39 articles published from 1993 to 2015 for review. The second follow-up search in June 2018 yielded 129 new articles; 93 titles that did not include a description of usability of O&P services were excluded, resulting in an additional 36 articles. Thus, a total of 75 articles were reviewed to identify variables that may influence use of O&P interventions (Table 1). Figure 1 combines the results from the initial and follow-up literature searches. The articles described patients,’ clinicians’, and researchers’ perspectives related to O&P device use with the following populations: lower limb orthoses (n = 20), lower limb prostheses (n = 18), shoes (n = 3), upper limb orthoses (n = 7), upper limb prostheses (n = 20), spinal orthoses (n = 2), and studies with a combination of populations (n = 5) (Table 2). Study participants included clinicians, researchers, and O&P patients. Authors most commonly surveyed patient perceptions about the technical variable of patient–device interaction (71% of reviewed articles). Although study methods varied, less than half of the studies (43%) were cross-sectional, collecting descriptive responses at a single time point.
Codes for the themes and variables identified in studies.
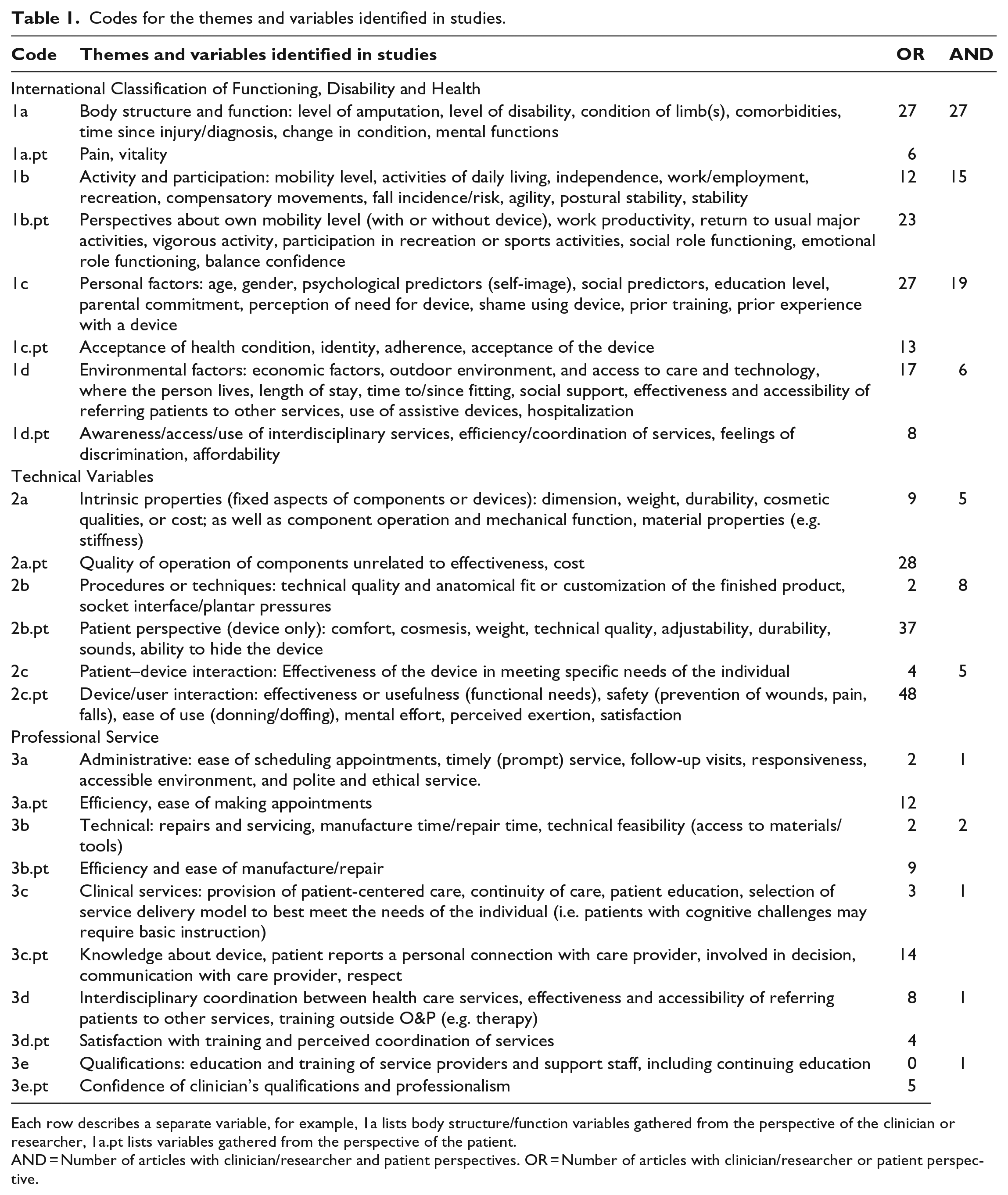
Each row describes a separate variable, for example, 1a lists body structure/function variables gathered from the perspective of the clinician or researcher, 1a.pt lists variables gathered from the perspective of the patient.
AND = Number of articles with clinician/researcher and patient perspectives. OR = Number of articles with clinician/researcher or patient perspective.
Variables identified in scoping review, organized by date within each population of study.
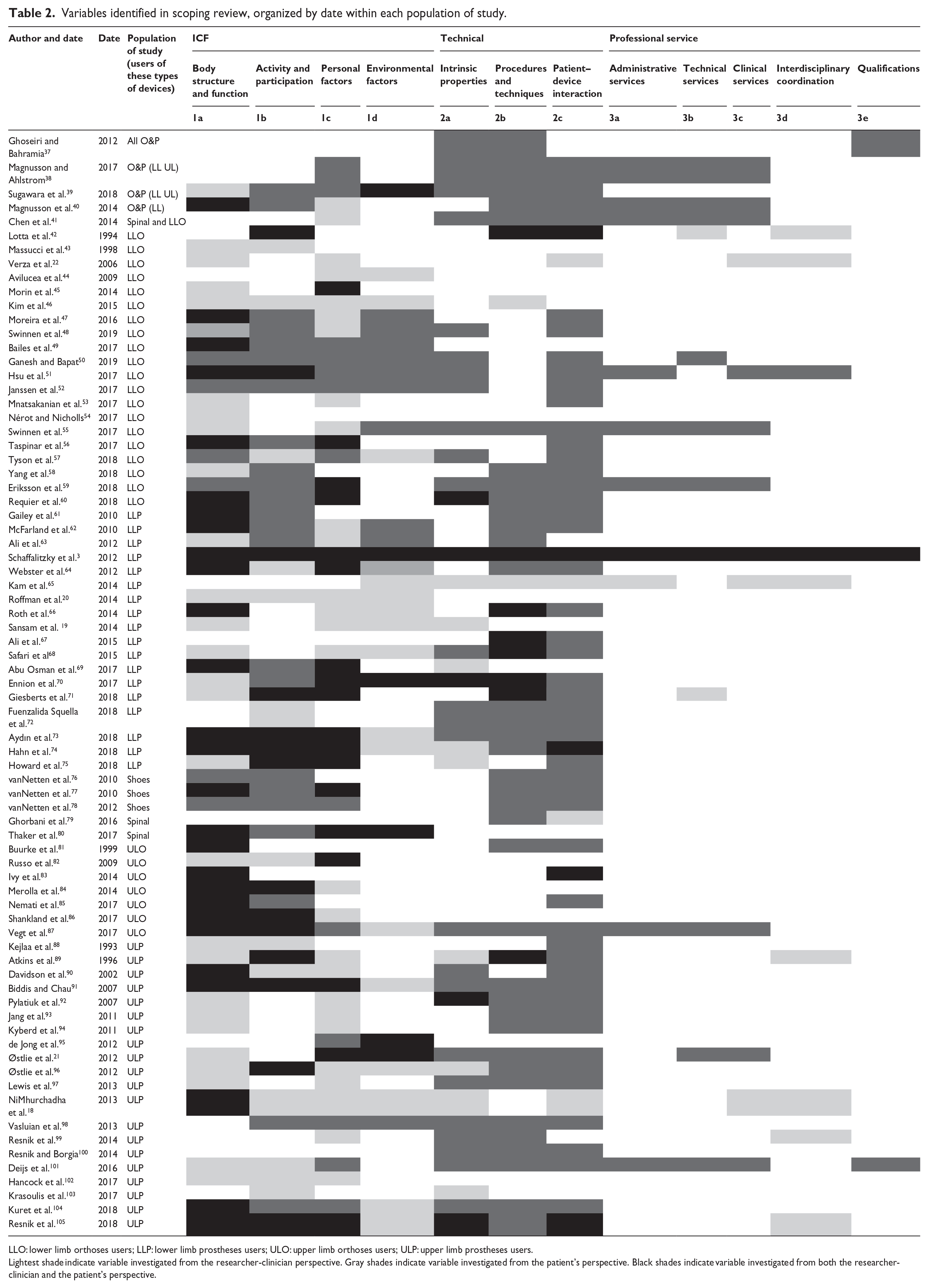
LLO: lower limb orthoses users; LLP: lower limb prostheses users; ULO: upper limb orthoses users; ULP: upper limb prostheses users.
Lightest shade indicate variable investigated from the researcher-clinician perspective. Gray shades indicate variable investigated from the patient’s perspective. Black shades indicate variable investigated from both the researcher-clinician and the patient’s perspective.
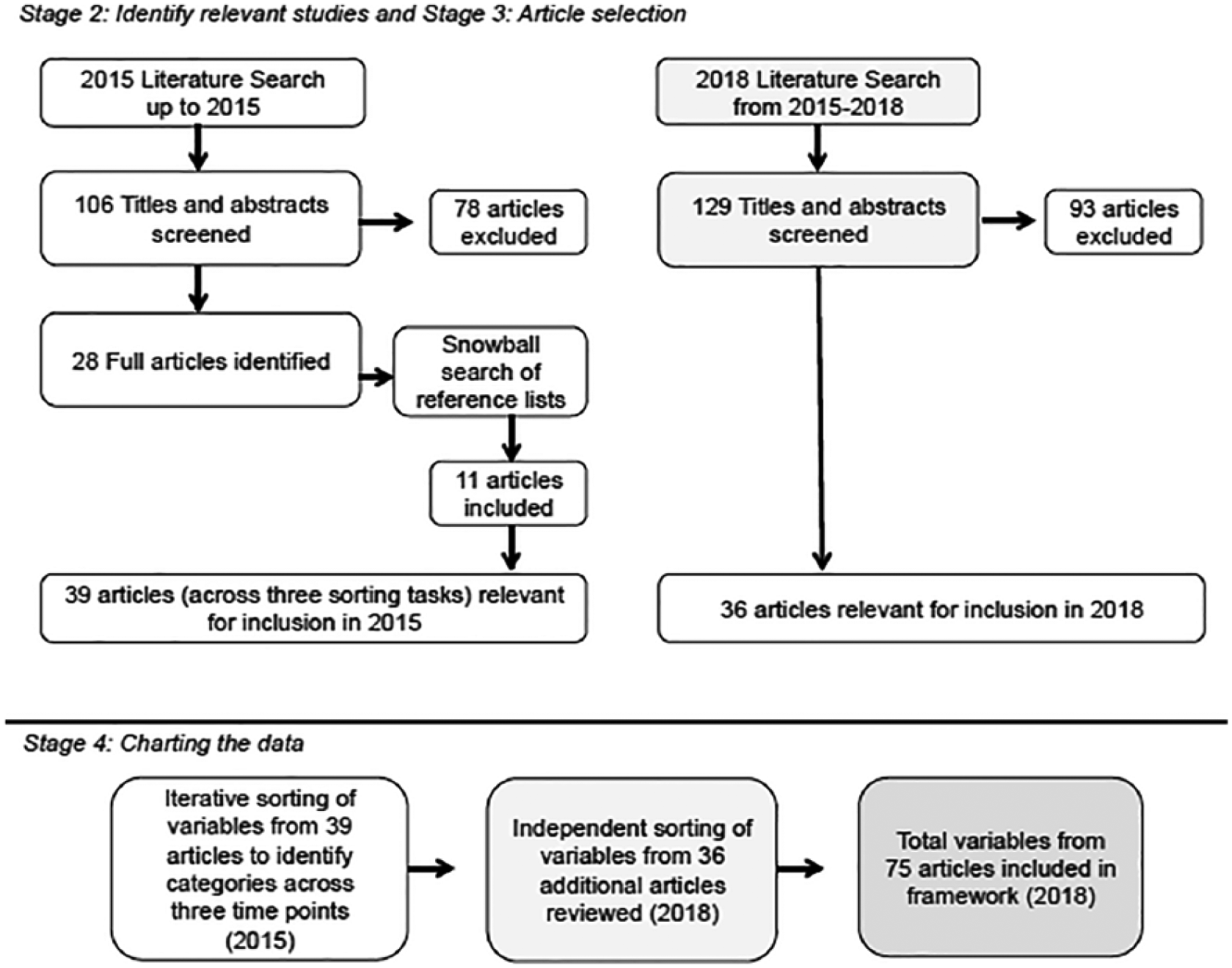
Diagram of the literature review process and charting of variables.
O&P Education Framework Areas
The identified variables related to O&P device use investigated by researchers and reported by participants were sorted into three thematic areas described below.
1. The ICF comprised the first area for our framework. Developed by the World Health Organization, the ICF provides a conceptual basis for health and disability 13 and includes six categories (body structure, body function, activity, participation, personal and environmental factors). The ICF describes the patient-specific health condition and the state of functioning, disability, and health and is the context for determining clinical services and interventions. Orthoses and prostheses are designed to match the context of each individual patient.
Four studies mentioned using the ICF to guide and organize their methods and/or findings.19,49,65,98 Many studies explored how level of injury/amputation, health comorbidities, and change in health condition may affect an individual’s decision to use a prosthesis/orthosis (Table 2). Some investigators examined personal variables, such as psychological predictors (e.g. self-image) and social predictors (e.g. access to care and social support). Pain often was identified as a potential deterrent to use (44% of reviewed articles).
2. The second framework area encompassed technical variables. This included intrinsic properties of the components or devices, quality of the procedures, and patient–device interaction. Intrinsic properties are fixed specifications of components or devices, such as dimensions, weight, durability, component operation, and component cost. The variables within the quality of procedures category varied based on perspective. Practitioners’ perspectives about quality of procedures included the technical quality and anatomical fit or customization of finished products, whereas patients’ perspectives of quality of procedures include comfort, cosmesis, weight, technical quality, adjustability, and durability. Finally, the patient–device interaction is the extent to which the device matches the context of the patient. In other words, it is the effectiveness or appropriateness of the device in meeting the specific needs of the patient from the clinicians,’ researchers’ and the patients’ perspectives.
Most of the identified technical variables included patient report relating to quality of technical procedures, ease of use, and whether the device was meeting patient needs (Table 2). Articles investigating the development of prosthetic components focused on the characteristics of the device/components. Specifically, researchers were interested in learning about patients’ perspectives of the intrinsic properties of components, such as weight, durability, and mechanical operation.99,100,106
3. The third framework area included professional service variables. The thematic variables in this area involved provision of professional, quality service throughout (before, during, and after) the plan of care. Professional service includes administrative services, technical services, clinical services, interdisciplinary coordination and care, and qualifications of providers and support staff. Professional service ensures that the individual needs of the patient are addressed. Although most studies (59%) did not examine professional service, this variable appeared primarily in more recent articles (i.e. after 2006) (Table 2). Ten studies37,38,40,41,55,59,60,70,87,101 used the Orthotic & Prosthetic User Survey (OPUS) or Quebec User Evaluation of Satisfaction with Assistive Technology (Quest 2.0). Both measures evaluate patient perspectives about professional service.
We recorded whether the source of data investigated by authors was from the patient, clinician, or both. Most of the selected articles surveyed patient perception about perceived usefulness of the device. This finding highlighted patient input as a critical variable of usability. Therefore, the proposed O&P education framework (Figure 2) illustrates patient-centeredness (patient perspectives) surrounding all aspects of care. Bettoni et al. 107 found patient perspective to be a crucial aspect of patient satisfaction.
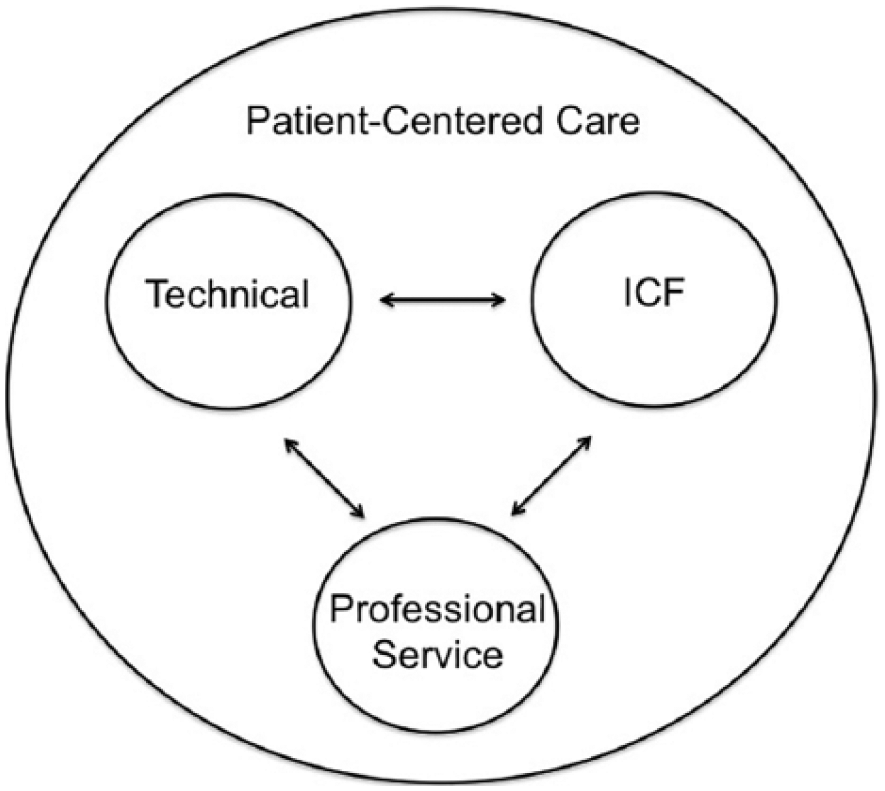
The orthotic and prosthetic education framework recognizes the interrelationships between the (1) International Classification of Functioning, Disability and Health (ICF), (2) Technical Variables, and (3) Professional Services and integrates Patient-Centered Care throughout the clinical reasoning process.
Because all of the variables identified in the studies were relevant for clinical reasoning, they were included in the O&P education framework (Table 1). The resulting framework depicts interaction among the variables. For example, the patient–device interaction is a dynamic relationship between the ICF, technical and professional service variables and represents the balance of all three areas from both the practitioner and patient perspectives. Although our framework illustrates an interaction between the areas and the importance of this aspect of O&P clinical care, our review did not attempt to define magnitude or implications of these interactions.
Implications for O&P Education
The development of this O&P education conceptual framework took an outcome-based approach, focusing on variables identified in the existing literature that may influence the use of O&P interventions to help students develop clinical reasoning skills. Many studies we reviewed highlighted variables and outcomes that influence O&P device use. Roffman et al. 20 stated that successful use of a prosthesis can be predicted by evaluating variables related to the amputation, demographic variables, and current levels of mobility, whereas Webster et al. 64 found higher social support to be associated with greater prosthetic ambulation and suggested further evaluation of the effects of treatment for depression and social support to enhance outcomes. Others highlighted the importance of evaluating personal, social, and environmental variables in addition to health care variables.3,18 Finally, Sugawara et al. 39 suggested focusing more on user assessment, prescription, training, and follow-up, emphasizing the need for a user-centered approach. Only one of the reviewed studies identified all of the categories depicted in our framework. 3
A particular strength of this proposed O&P framework is the potential to help students think critically about the organization and interaction of important variables within a clearly defined structure.24,27,28 Developed through the lens of O&P clinical educators, our education framework includes three areas situated within the context of patient-centered care: (1) the state of functioning, disability, and health (ICF); (2) O&P technical properties, procedures, and appropriateness; and (3) professional service as part of O&P interventions. Most of the reviewed studies included variables from the ICF and the technical areas, but only more recent studies included variables from the professional service area. Quality professional service, such as administrative services 108 and interdisciplinary care, 12 is necessary for optimal patient outcomes. Although only four studies19,49,65,98 used the ICF to organize their methods and/or findings, most studies used at least one ICF category to examine the usefulness of O&P services. This is not surprising. The ICF has been promoted for use in O&P to encourage a holistic and patient-centered approach 109 and has been proposed as a framework to guide clinical reasoning. 110
While individuals’ use of prostheses and orthoses is classified within the environmental factors category of the ICF, the ICF does not provide the level of detail nor the quality characteristics necessary for clinical interpretation and reasoning. In addition to the health care variables (i.e. body structure, function, activities, participation, personal and environmental factors), prosthetists–orthotists evaluate specific technical criteria (e.g. material properties) and develop technical goals (e.g. alignment and anatomical fit) when formulating their treatment plans. Furthermore, clinicians analyze and predict how technical details of their interventions influence other technical variables and the functional goals of the patient. For example, a knee–ankle–foot orthosis may be prescribed to correct genu recurvatum in order to provide knee stability during gait. The orthotist must analyze the patient’s health condition (e.g. muscle strength, range of motion, gait) as well as the advantages and disadvantages of the various technical options. With this information, the clinician determines the technical details: the knee joint alignment, material properties, and corrective forces for appropriate anatomical fit. Because the ICF does not allow for this level of detail, the O&P education framework includes technical variables as a separate area to encourage deeper critical thinking about the variables that affect O&P technical and functional outcomes.
During their training, O&P students might use this education framework as a structure to identify and systematically categorize variables, explore relationships between variables, and recognize how variables may affect the quality of device and the quality of professional service in producing the desired outcomes. This scaffolding has the potential to facilitate the development of students’ clinical reasoning skills from novice toward expert level. For example, students often focus on the anatomical fit and socket comfort during their prosthetic clinical outcome evaluations. However, focusing only on the technical adequacy may lead to a clinical bias, where the clinician only views the patient in terms of providing a device rather than recognizing (and thus evaluating) the patient within the context of their activities. 111 A relationship exists between technical goals, professional service, and functional goals; specifically, the socket comfort (technical), anatomical fit (technical), and quality of initial education and training (professional service) will likely impact the clinical outcome of meeting a patient’s functional goals (ICF).
The articles included in the scoping review reported usefulness of a device from the clinician/researcher’s perspective and from the patient’s perspective (Table 2). Although stakeholder perspectives are important, they make it difficult to distinguish between areas within our proposed O&P education framework. For example, within the technical area, intrinsic characteristics (i.e. fixed or semi-fixed properties of components or materials) are easily recognizable to prosthetists/orthotists; however, patients or other health care providers may be unable to differentiate between technical operation of the component and functional operation of the completed device. Although both criteria influence the overall appropriateness and perceived usefulness of the device, they represent two independent variables of usability.
A scoping review was a useful method to identify variables that have been used to measure the effectiveness, efficiency, or satisfaction of O&P services. However, we recognize the limitations of this scoping review and O&P education framework development. First, the number and variety of identified variables may be limited because only English-language articles were reviewed. Since research published in other languages was not included, different cultural perspectives may have been omitted. Medline was the only electronic database searched, potentially restricting the number and types of study designs. Although the search terms were intentionally broad, our inclusion criteria limited the addition of research evaluating criteria other than usability variables. Second, the studies were not examined for methodological rigor; therefore, the weight or relative value of identified variables is unknown. Third, the proposed O&P education framework was developed by a small group of O&P educators from one university in the United States. As such, the O&P education framework only represents our perspectives and should be vetted further with relevant stakeholders (i.e. orthotists–prosthetists, people who use O&P devices, students, therapists, physicians, and other educators). Finally, determinant frameworks 27 are inherently limited by variables identified in the research literature, whether the influence of these variables is hypothetical or real; thus, a linear relationship between variables and outcomes cannot be assumed, as individual variables may interact in various ways.
This proposed O&P education framework is intended to promote conversations that advance our teaching and assessment of students’ clinical reasoning skills. Future directions for this work may include review by stakeholder groups to provide qualitative feedback and further refinement or application of the Delphi method to achieve consensus on clinical reasoning variables, their interactions, and their relative importance. Considering the “contextual fit” 36 of patient–device interaction would broaden our understanding about how/why variables might affect both the quality of intervention implementation and whether the intervention actually produces the desired outcomes. Because conceptual frameworks identify gaps in learning or evaluation, 112 integration of a framework, such as the one proposed, may lead to a deeper discussion about how to teach and learn O&P clinical reasoning skills. Conceptual frameworks require ongoing discussion and iterative review. They are dynamic and should be challenged and altered to meet the needs of the profession. 24
Conclusion
Our proposed conceptual framework, developed with input from a scoping review, organizes variables that may influence O&P device use and is intended to enhance O&P students’ clinical reasoning skills. The O&P education framework, developed through the lens of O&P clinical educators, includes three distinct areas situated within the context of patient-centered care: (1) the state of functioning, disability, and health (ICF); (2) O&P technical properties, procedures, and appropriateness; and (3) professional service as part of O&P interventions. This framework provides a structure to broaden perspectives and to systematically categorize clinical reasoning variables. Thus, students may use this framework to critically think about how/why variables might affect the quality of the device, the quality of professional service, and whether the intervention actually produces the desired outcomes.
Footnotes
Acknowledgements
The authors wish to thank Brian Hafner, PhD, Sara Morgan, CPO, PhD, Ramona Okumura, CP and Geoffrey Balkman, CPO, for their helpful review and suggested revisions to this article.
Author contributions
Initial concept: Scott A Spaulding and Susan E Spaulding. Acquisition of articles: Susan E Spaulding. Analysis and design of education framework: Ann Yamane, Cody L McDonald, and Susan E Spaulding. Drafting the work: Susan E Spaulding. Revising it critically for important intellectual content: Ann Yamane and Cody L McDonald. Final approval of the version to be published: Susan E Spaulding, Ann Yamane, Cody L McDonald, and Scott A Spaulding.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.