
Abstract
Background:
Education and training in prosthetics and orthotics typically comply with International Society for Prosthetics and Orthotics standards based on three categories of prosthetic and orthotic professionals.
Objective:
This scoping study sought to describe the evidence base available to answer the question, How are prosthetic and orthotic services influenced by the training of staff providing them?
Study design:
Scoping review.
Methods:
A structured search of the peer-reviewed literature catalogued in major electronic databases yielded 3039 papers. Following review of title and abstract, 93 articles were considered relevant. Full-text review reduced this number to 25.
Results:
Only two articles were identified as providing direct evidence of the effects of training and education on service provision. While both suggested that there was an impact, it is difficult to see how the more specific conclusions of either could be generalised. The other 23 articles provide a useful background to a range of issues including the specification of competencies that training programmes should deliver (3 articles), descriptions of a range of training programmes and the effects of training and education on student knowledge and skills.
Conclusion:
Although it is considered axiomatic, the service quality is dependent on practitioner education and training. There is insufficient evidence to establish whether levels of training and education in prosthetics and orthotics have an effect on the quality of prosthetic and orthotic services.
Clinical relevance
There is very little evidence about the effects of training and education of prosthetists and orthotists on service quality. While this is a somewhat negative finding, we feel that it is important to bring this to the attention of the prosthetics and orthotics community.
Background
Formal education in prosthetics started in the United States in the 1950s with programmes at the University of California (Los Angeles) in 1952, New York University in 1956 and Northwestern University in 1958. 1 The first national scheme for the accreditation of prosthetic and orthotic (P&O) training programmes was also developed in the United States when the American Board for Certification in Orthotics, Prosthetics & Pedorthics (ABC) created the Educational Accreditation Commission (which has now evolved into the National Commission on Orthotic and Prosthetic Education) in 1972. 2 In other countries, responsibilities for developing benchmark statements and accreditation have been developed by quasi-governmental organisations as in the National Health Service 3 and Quality Assurance Agency for Higher Education 4 in the United Kingdom.
International efforts to standardise training and service delivery in P&O, under the auspices of the United Nations (UN), can be traced to the Inter-regional Seminar in Standards for Training of Prosthetists in Holte, Denmark in 1968. 5 This was followed by three meetings in 1984 and 1985 organised by the International Society for Prosthetics and Orthotics (ISPO) 6 and a further World Health Organization (WHO) meeting in Egypt in 1990 which resulted in the publication of Guidelines for training personnel in developing countries for prosthetics and orthotics services. 7 The most recent version of these guidelines 8 was prepared by a joint WHO/ISPO meeting in Scotland in 2003. This laid the foundation for the Evaluation and Recognition scheme operated by ISPO which has so far recognised 42 training programmes in 26 countries. 9
The WHO/ISPO Guidelines 8 propose three categories of P&O professional. Category I prosthetist/orthotist is the level of professional who should ideally provide all P&O services within a rehabilitation team. ISPO Category I professionals are competent in all aspects of service delivery including referral and appointment, assessment, prescription, funding and ordering, product preparation, fitting, user training, follow-up, maintenance and repairs. ISPO Category I professionals are also expected to participate in research and service development activities. In countries where resources and finances are not available to train all clinical staff to this level, training to ISPO Category II level is believed to represent a compromise that will still provide a quality service, preferably with supervision from ISPO Category I professionals for difficult cases. ISPO Category II professionals will not usually be trained in all areas of clinical practice but rather in specific areas such as lower limb prosthetics or lower limb orthotics only. ISPO Category III professionals have a technical role and support ISPO Category I or II staff in fabricating, assembling, maintaining and repairing devices. They will not, generally, have direct contact with the service user. The broad guidelines on minimum entry requirements and training were tabulated in the original WHO/ISPO Guidelines and have been reproduced as Table 1. To supplement the WHO/ISPO Guidelines, a further three Information Packages have been published giving detailed guidance on the level of training required for each category of professional.10–12
Type of personnel as specified in the original Guidelines for training personnel in developing countries for prosthetics and orthotics services. 8
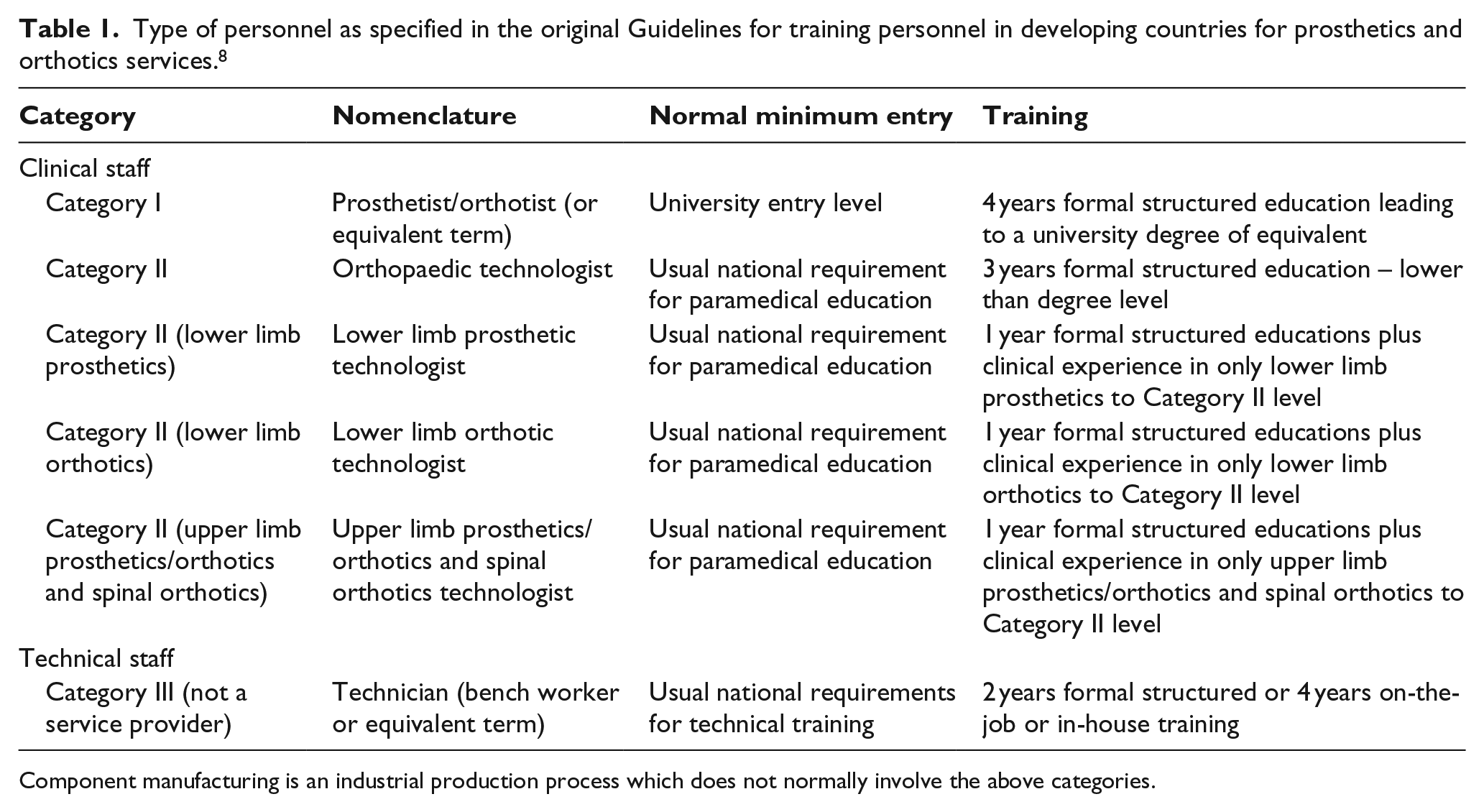
Component manufacturing is an industrial production process which does not normally involve the above categories.
Inherent in these developments is a recognition that although in an ideal world P&O services would be led by an ISPO Category I professional, compromises might have made to be in resource-limited environments. The extent to which these compromises are required will clearly be determined by the balance between the clinical need and the resources available to address them. The recent WHO World Report on Disability 13 has raised the estimated percentage of the population who live with disability from 10% to 15%, equivalent to over a billion people. This is largely as a result of the ageing population and the global increase in chronic health conditions associated with disability. Furthermore, the report concludes that disability disproportionately affects vulnerable populations with a higher prevalence in lower income countries than in higher income countries.
A more recent report, Transforming and scaling up health professionals’ education and training, 14 acknowledges a severe and global healthcare crisis. Millions of people do not have access to healthcare services, in part, because of the uneven geographical distribution of health professionals and the limited skill-mix of healthcare teams. The report calls on governments in affected countries to increase capacity for training of healthcare professionals but also for new approaches to education that foster community engagement and more local service delivery.
Given the number of healthcare professionals required to meet the projected demand, questions about the level of training required to provide high-quality care are appropriate. In environments where resources are relatively plentiful, the assumption that more highly trained professionals will deliver higher quality services seems to be well accepted. However, where resources are limited, it is important that we understand how increased training affects the volume and quality of service delivery to make well-informed decisions about how healthcare and education resources can be best utilised.
In a clinical world increasingly dominated by evidence-based practice, such an analysis should be based on objective evidence published within the peer-reviewed literature. Based on a preliminary search of the literature, the authors were unaware of studies describing the effect of staff training on service-level outcomes (e.g. quality, volume), and it was thus decided that a scoping review would be appropriate to answer the question: How are P&O services influenced by the training of staff providing them?
Methods
This review followed the recommendations for scoping reviews provided by Armstrong et al. 15 on behalf of the Cochrane Collaboration. Ethical approval (IR.MUI.REC.1394.211) was obtained from the Isfahan University of Medical Sciences Ethics Committee (Isfahan, Iran) prior to the study. Three databases – Medline (through OVID), Web of Science and Scopus – were searched using a combination of search terms and acronyms related to prosthetics and orthotics, service provision and education and training (Table 2). Most searches were conducted on the basis of title, keyword and abstract. However, searches related to education and training did not include an abstract search to avoid studies of patient education, as opposed to the education of healthcare professionals. The search term prosthetic is very widely used across healthcare (e.g. hip implants), and as such, a number of exclusions were specified to improve the precision of the yield (Table 2). Given that the major developments in education and training in prosthetics and orthotics have occurred over the last 20 years, the search was limited to the years 1995–2015, inclusive. The final results were exported into a single EndNote® (Thomson Reuters, Philadelphia, PA, USA) database and duplicates were removed.
Search terms and yield.
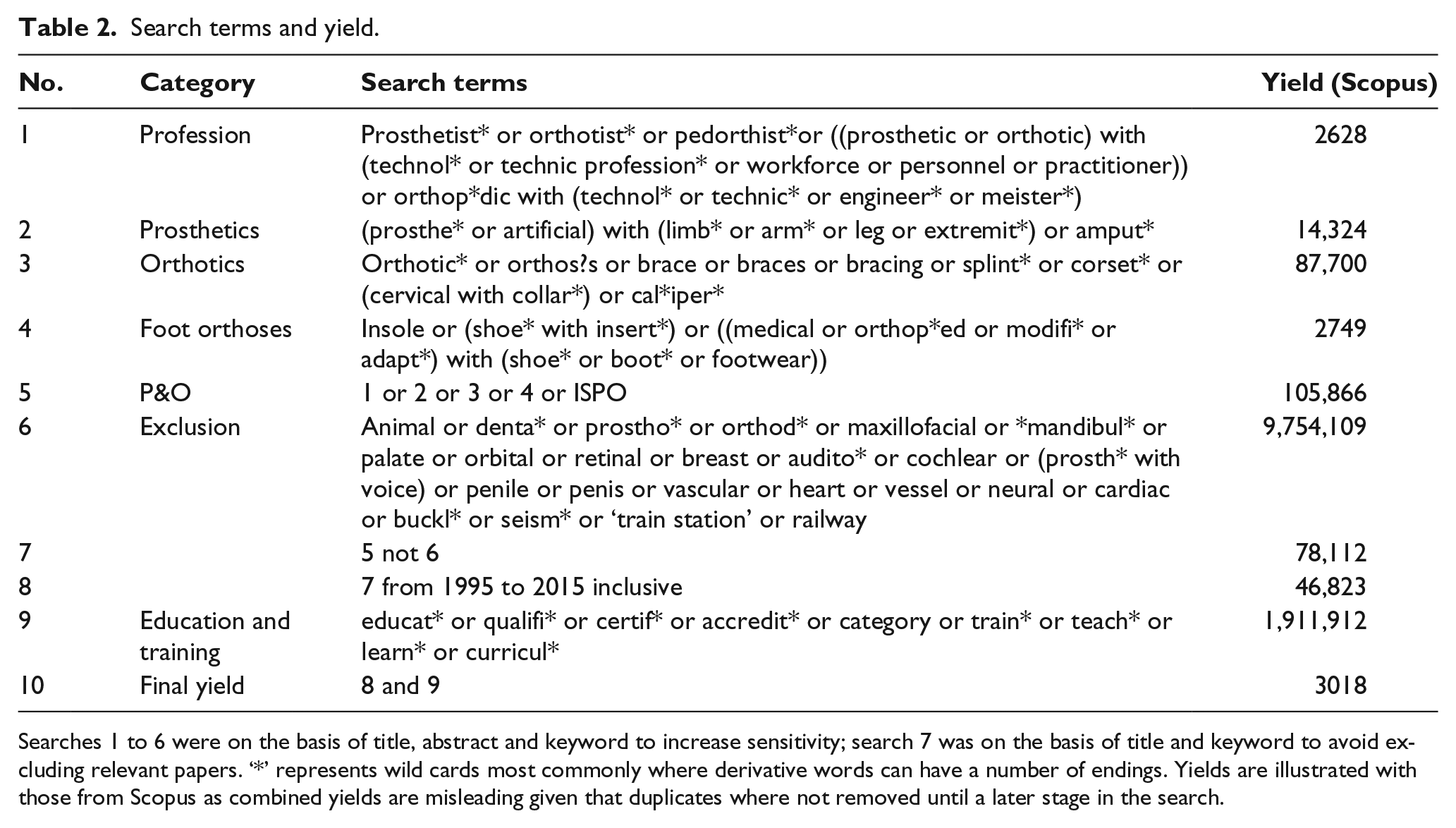
Searches 1 to 6 were on the basis of title, abstract and keyword to increase sensitivity; search 7 was on the basis of title and keyword to avoid excluding relevant papers. ‘*’ represents wild cards most commonly where derivative words can have a number of endings. Yields are illustrated with those from Scopus as combined yields are misleading given that duplicates where not removed until a later stage in the search.
Broad selection criteria appropriate to a scoping review were used. 15 Articles were included if they provided evidence or opinion of the impact of staff training on service provision. In order to ensure that all relevant papers were included, more specific limitations (e.g. study design or outcome measures) were not used. Two of the co-authors (E.S.-D. and S.F.) independently vetted studies based on title and abstract. Articles deemed irrelevant by both investigators were excluded. Three of the co-authors (E.S.-D., S.F., and R.B.) then assessed full-text articles to identify studies for inclusion. Any disagreements were resolved through discussion leading to consensus.
The purpose of the review was to provide an overview of the existing literature, 15 and this was achieved by identifying a number of themes that were addressed by the included papers. A narrative was then constructed for each theme describing the type of information contained in relevant articles. Given that this was a scoping review, no formal analysis of quality or meta-analysis of data 15 was performed.
Results
The search yielded a total of 3039 articles, of which 93 remained after vetting based on title and abstract (see Table 2). Review of the full-text article resulted in 25 papers, among which four predominant themes were identified: specifications of competencies that training programmes should deliver (3 articles), descriptions of training programmes, 13 effects of training on students, 8 and effects of training on service delivery. 2 All except one paper 16 addressed a single theme.
Specifications of competencies that training programmes should deliver
Three articles made recommendations about the competencies that undergraduate programmes in P&O should deliver.16–18 Such recommendations arose out of research with other primary objectives and are generally quite specific to the location in which the study was performed. For example, Magnusson and Ahlstrom 18 conducted a survey of the experiences of 15 P&O technicians working in Sierra Leone and concluded that there was a need for ‘further education and development specifically with regard to rehabilitation practice, prosthetic and orthotic design, modern technologies and rehabilitation, and prosthetic and orthotic theory’.
Descriptions of training programmes
In all, 13 articles describe either existing19–26 or planned27–31 P&O programmes including descriptions of entire programmes,21,24,25,27,28 research residencies29–31 and problem-based, 23 open 26 and distance 22 learning. Although published in peer-reviewed journals, these studies are mostly descriptive presenting little qualitative or quantitative analysis of the effectiveness of the activities they describe. Thus, for example, Simpson 26 outlines the development of new post-graduate open-learning opportunities but only reports the number of students registered and not whether there has been any effect on service provision as a consequence.
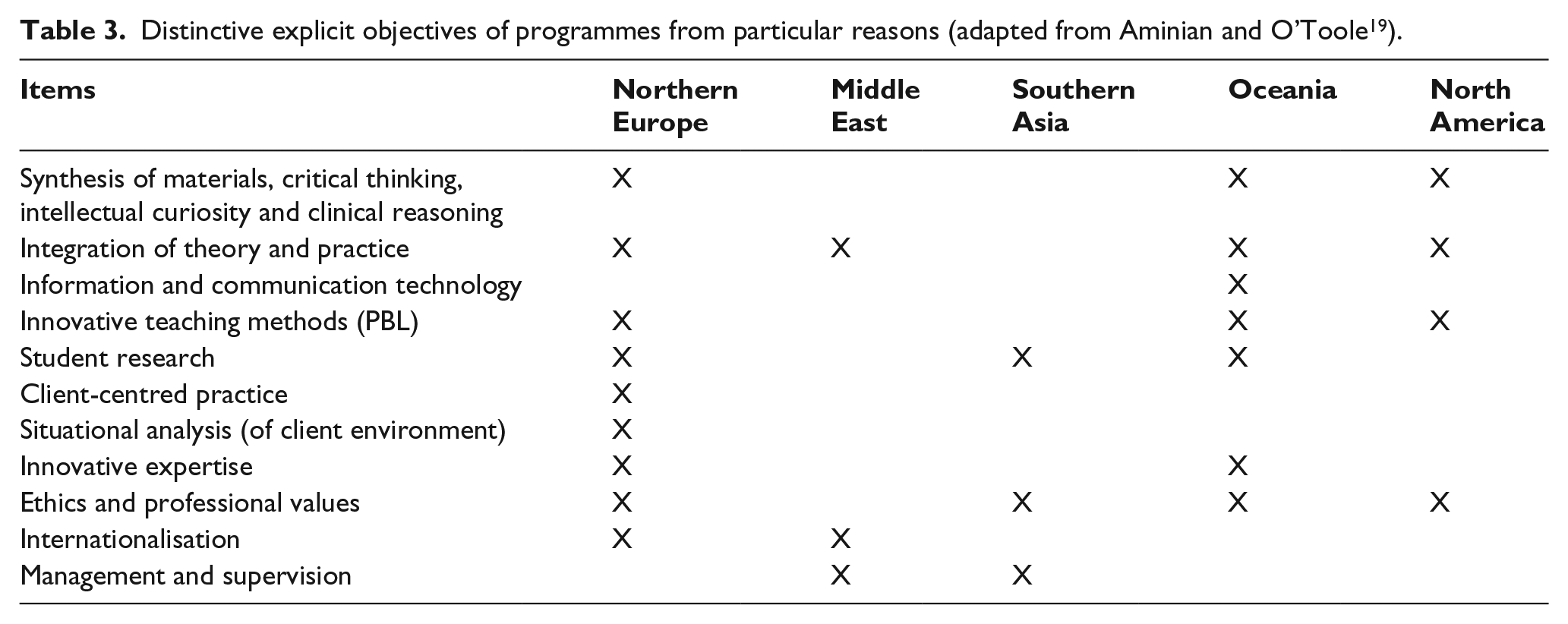
Two papers within this category (and from the same group) present comparisons of the curricula offered internationally19,20 by a range of programmes that have been recognised by ISPO. The first of these 19 concluded that while many of the core competencies required for P&O practice were similar across programmes, there was considerable variability in a range of more general learning outcomes as described in Table 3. Through a Delphi study, it also ‘revealed disagreement amongst the expert panel regarding the effectiveness of different approaches to teaching undergraduate P&O students’. The later study 20 conducted a more detailed analysis of attitudes to different approaches to education. Institutions in developed countries saw students as responsible for their own learning and tended to focus on developing critical thinking skills. By contrast, institutions in developing countries focussed more on skill development under close supervision from instructors. It commented that while student-focussed approaches are now broadly accepted, they are still more common in developed countries but less common, regardless of location, than ‘might have been expected from the general health sciences literature’.
Distinctive explicit objectives of programmes from particular reasons (adapted from Aminian and O’Toole 19 ).
Effects of training on students
Seven papers32–39 assessed various aspects of education and training on students either by surveying student opinion32–35,38,39 or evaluating differences in the attainment of learning outcomes.36,37 Most focussed on specific aspects of curriculum development such as integrating research, 32 continuing professional development, 33 interprofessional education, 36 training in critical thinking 37 and distance or e-learning.38,39 The other two reported on more general aspects of undergraduate education.34,35 These studies generally suggest that developing particular aspects of the curriculum results in improvements in learning outcomes and/or the perceived student experience. The disparate nature of the studies, however, prevents any more specific conclusions. The quality of the evidence is generally quite poor with most being relatively small numbers of students in specific geographical contexts that limits generalisability.
Effects of training on service delivery
Two articles provide evidence relating patient outcomes to the characteristics of professional training. The first 40 highlighted differences in outcomes when health professionals from three different disciplines provided foot orthoses. Given that the primary differences between these groups were how they were trained, differences in outcomes suggest an effect of that training; 10 Dutch podiatrists, 10 pedorthist (specialists in footwear adaptations) and 11 orthotists made a pair of foot orthoses for each of three patients with foot complaints. Between disciplines, there was an extensive variation in construction of the orthoses, particularly between those constructed by the podiatrist and other groups. Foot orthoses provided by podiatrists reduced maximal peak pressures by smaller amounts than those from the other two professional groups (p < 0.001), and a subjective patient reported ‘walking convenience’ score and also suggested lower levels of satisfaction with orthoses produced by podiatrists. There were a number of limitations to this study including a very small number of patients, lack of generalisability beyond the geographic region in which the research was conducted and the confounding effects of a difference in design principles and years of professional experience between the professional groups. In spite of these limitations, the work provides some, albeit limited evidence that the education provided to different health professionals may lead to different outcomes.
The second of these studies reported on the impact of P&O service delivery of the graduates (ISPO Category I or II) from the Tanzania Training Centre for Orthopaedic Technologies (TATCOT) on P&O service delivered in Tanzania, Kenya and Uganda. 16 The report was based on a field visit and included interviews with Ministries, Heads of Hospital Services, P&O Service Mangers, graduates and their clients. While the report is essentially narrative, it presents a considerable body of qualitative, and limited quantitative, evidence of the positive contribution that graduates are now making to P&O service delivery and that their competencies generally match those stated in the relevant ISPO guidelines.11,12 It was notable that a small number of ISPO Category I professionals were leading and developing services (although it was acknowledged that some ISPO Category II professionals were also showing potential in these areas). While the report implies that improved training leads to better service provision, there is too little detail to support any more specific or generalisable conclusion.
Discussion
There are a number of reasons why research into the effect of education on health outcomes may not have been performed. It is considered axiomatic across healthcare that service quality is dependent on practitioner education and training. This is reflected in the recent WHO Guidelines for Transforming and scaling up health professionals’ education and training 14 which provides no evidence that the quantity, quality and relevance of health education impact health service outcomes but rather assumes that this is self-evident. It is also assumed that pre-service education is the only factor driving outcomes of the service despite many other influences such as the availability of resources, opportunities for continuing professional development and mentoring of junior staff as well as the culture within organisations that can promote opportunities for further education and training in the workplace.
Given the complexity of modern healthcare services, considerable ingenuity will be required to isolate the effects of pre-service education on the quality and quantity of service delivery. True clinical trials would require comparison between services differing only in the level of staff training. It seems unlikely that these will occur naturally or could be created artificially for research purposes. It might, however, be possible to audit outcomes of a range of different services and use the outcomes to construct regression models to determine the extent to which these are affected by factors such as education. Including other factors in the regression models, such as general level of resources, years of experience or models of service delivery would control for the confounding influence of these and help isolate the unique effect of education. Clearly, the first stage of such an analysis would be to identify appropriate general outcome measures and start recording these as a routine component of service delivery.
The review also yielded a number of articles which appear to provide a broader perspective on a range of issues affecting education and training in prosthetics and orthotics such as the curriculum delivered,16–20 modes of delivery22,23,26,29–31 and their effectiveness in educating students32–39 (as opposed to effects on service delivery). Individual studies, however, tend to be of low quality, and generalisability is limited by specific local factors and multiple potential confounders. Heterogeneity between studies also prevents any useful synthesis.
This study is a scoping review and as such is subject to the general limitation of this form of research 15 including the provisional nature of the literature search and the absence of any formal quality assessment or meta-analysis. A potential limitation of this particular scoping review may be the decision not to attempt a comprehensive search of the grey literature. It is also possible that despite any formal restriction on language, the search strategy was likely to bias results towards publications in English. The virtual absence of directly relevant papers yielded by the search of relevant electronic databases which was conducted and was specifically designed to be sensitive makes it extremely unlikely, however, that information contained in the grey or foreign language literature would lead to any more definitive conclusions.
The main reason for performing a scoping review is to map what information is available within the literature as a basis for assessing the usefulness and potential scope for a systematic review. It is clear from the results of this particular scoping review that there is insufficient literature available to warrant such a review in this area.
Conclusion
The primary finding of this review is that there are no studies specifically designed to establish whether levels of training and education in prosthetics and orthotics have an effect on the quality of P&O services or the health outcomes of those using the service. As such, it is not known whether tailoring pre-service education to the three ISPO categories of health professional has any specific effect on the quality of service delivery.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study has been made possible by the generous support of the American People through the United States Agency for International Development (USAID) grant to the International Society of Prosthetics and Orthotics (ISPO) for the project Rehabilitation of physically disabled people in developing countries (DFD-A-00-08-00309-00). Additional funding was provided by the Isfahan University of Medical Sciences, Iran (MUI-194211).