
Abstract
Background:
Orthotic and prosthetic residency preceptors have little guidance transitioning residents between observing and performing patient care. Understanding current entrustment trends and factors can help guide resident progression during residency.
Objectives:
To identify entrustment trends and factors within an orthotics and prosthetics residency affecting a supervisor’s decision to entrust residents with independent patient care.
Study design:
Cross-sectional study
Methods:
In this cross-sectional study, 831 National Commission of Orthotic and Prosthetic Education preceptors were invited to complete a 26-question, online questionnaire that examined possible entrustment factors.
Results:
A total of 77 preceptors completed the questionnaire. The top-reported behavioral qualities impacting entrustment were recognition of limitations and willingness to ask for help (n = 45) and competence (n = 37). Preceptors ranked evaluation (n = 27) as the professional skill which most affected entrustability; technical skill least affected entrustability (n = 4). Preceptors of 12-month residencies entrust residents to indirect supervision when they have completed approximately 75% (i.e. 9 months) of the program. Preceptors of 18-month residencies reported that they entrust their residents by the time they reach 50% (i.e. 9 months) of their training. A small number of preceptors (n = 19) never allow a resident to independently perform practice management.
Conclusion:
Residency supervisors value interpersonal and evaluation skills when making entrustment decisions. Residency mentors can use these findings to inform their entrustment decisions and support a resident’s progression toward independent practice.
Clinical relevance
This study presents information which can inform clinical preceptors and residents on what factors contribute to the decision to progress a resident from observation to independent patient care. These findings may influence clinical education standards which aim to promote both resident training and patient access to quality care.
Background
Orthotic and prosthetic (O&P) residents need practice providing independent patient care prior to becoming certified and licensed practitioners. 1 Residency preceptors, here used to also reflect the terms mentors and supervisors, help students progress from observing patient care to independently providing patient care by entrusting residents with responsibilities at varying levels of supervision.2–8 As part of the healthcare team, practitioners are expected to provide quality and appropriate patient care. 9 Poor or inadequate care from a resident practitioner could negatively impact a patient’s general trust in his or her healthcare providers. It is challenging for residency preceptors to balance providing educational clinical experience for residents while still ensuring quality patient care. 10
Like other healthcare supervisors, O&P residency preceptors progress residents from observing to independently providing patient care using a competency-based training approach. 1 The National Commission on Orthotic and Prosthetic Education (NCOPE) 1 publishes a list of competencies that O&P residencies must incorporate to ensure proficient resident education. These competencies reflect the responsibilities of current practicing orthotists and prosthetists that the American Board of Certification for Orthotics, Prosthetics, and Pedorthics (ABC) compiled in their 2015 Practice Analysis of Certified Practitioners. 11 Consistency between NCOPE and ABC standards ensures that students and residents are learning what is deemed necessary for the provision of quality patient care.
Of the two possible O&P NCOPE-approved residency formats, the most common is the 12-month residency in one discipline (i.e. orthotics or prosthetics) followed by another 12-month residency in the other discipline within the same or with a different organization. An alternative to the sequential 12-month residency is the 18-month residency which combines both O&P disciplines and is typically within one organization. In some clinical organizations, residents rotate with different practitioners during the 12- or 18-month residency time frame. These rotations can vary greatly in duration, with some lasting a week and others lasting for months.
Within the residency, residents are trained in a number of distinct areas related to professional practice, patient care, and delivery of an O&P device. As a part of developing competency, residents must be entrusted to progress from observation to assistance to direct supervision and, finally, indirect supervision. 1 NCOPE defines direct supervision as real-time in-person oversight; indirect supervision does not require the supervising practitioner to be physically present. Although there are well-outlined residency requirements, there are currently no established standards or behaviors residency preceptors can use to identify an opportunity to increase a resident’s independence. To optimize learning and resident engagement, entrustment guidelines could help preceptors determine when to advance residents through different responsibilities as well as help residents identify areas of improvement.3–5 Before developing these guidelines, it is critical to first understand the entrustment decision-making process and the factors preceptors consider when entrusting a resident.
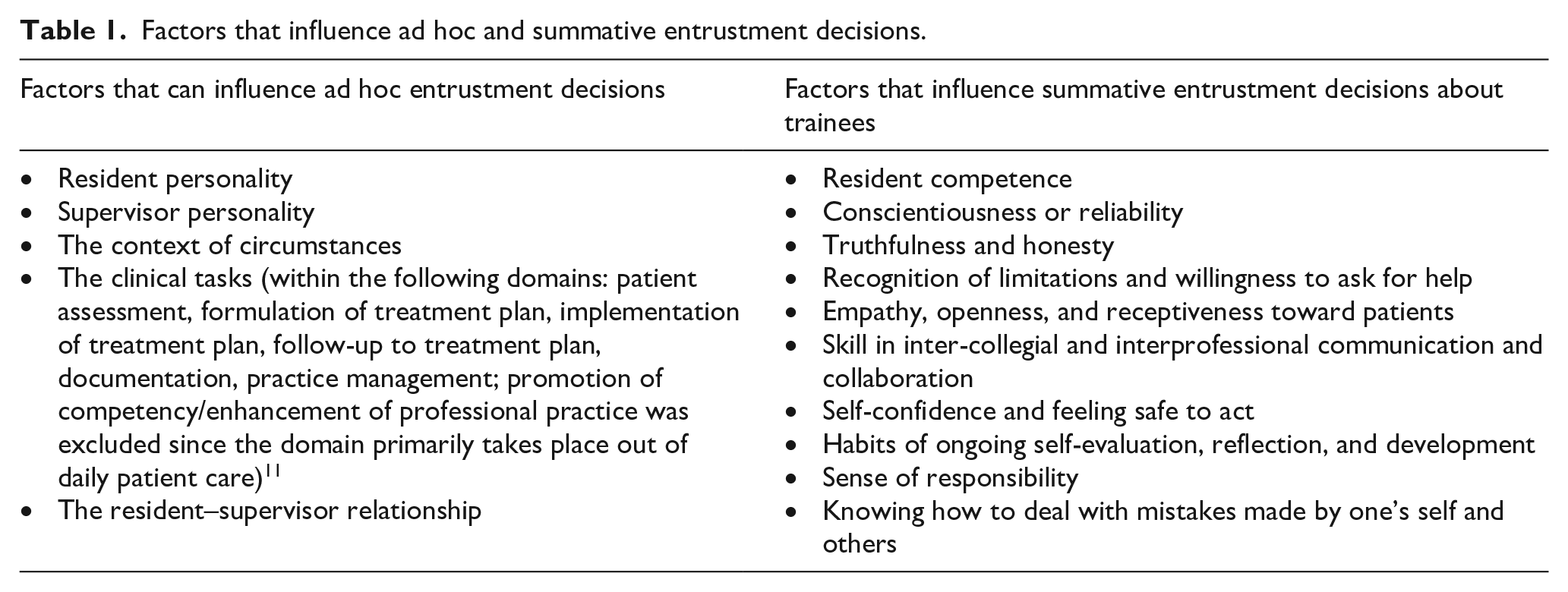
Preceptors can entrust the resident with a certain responsibility at various levels: be present and observe, act with direct supervision, act with indirect supervision, act without supervision, and provide supervision to other residents or trainees. 2 However, determining when to transition between different levels of supervision can be challenging. Preceptors make two types of entrustment decisions: ad hoc and summative decisions.3–5 Ad hoc decisions are based on the risk and urgency of the situation, the appropriateness of the task for the resident, and the amount of trust in the resident. These decisions do not necessarily apply to other situations. Conversely, summative decisions are based on qualifications established by school program directors or clinical competency committees and have finality. Different factors may determine whether an ad hoc or summative decision is made (Table 1). 3 Understanding how these factors influence preceptors’ choice to reduce their level of supervision can provide insight into what might promote or restrict entrustment decisions. This study examined entrustment trends across different types of O&P residencies in order to inform the development of entrustment guidelines.
Factors that influence ad hoc and summative entrustment decisions.
Methods
Survey development and dissemination
A custom O&P entrustment survey (online supplement) was developed from concepts outlined on previous entrustment surveys used in other healthcare professions, 2 the ABC Practice Analysis, 11 and other residency characteristics defined by NCOPE. 1 Questions about the preceptor’s personality type, clinical education, and residency training were also included to provide context to their survey responses. The survey questions were designed to gather insight into various decision-making factors, including those contributing to ad hoc and summative decisions. The survey was designed to be completed in 20 min.
This protocol was approved by the institutional review board at Baylor College of Medicine (H-39530). The survey link was provided to staff at NCOPE, who disseminated the link to all 831 NCOPE-qualified preceptors, which included both residency directors and residency preceptors. The survey was open from February to July 2017, and a reminder email was sent 2 weeks prior to the closing date.
Inclusion criteria
Potential participants included NCOPE-certified, O&P residency directors and preceptors. These certified and/or licensed orthotists and/or prosthetists were presumed to be familiar with the residency requirements established by NCOPE since they had completed required preceptor training.
Preceptor demographics and residency characteristics
For educational priorities, preceptors were asked which of the following ABC Practice Analysis domains was most important in regard to successful resident entrustment: patient assessment, formulation of treatment plan, implementation of treatment plan, follow-up to treatment plan, documentation, practice management, and promotion of competency/enhancement of professional practice. Documentation was isolated from practice management to create an additional domain due to the authors’ experience of documentation being a unique entrustable professional activity. Preceptors were asked to report whether they supervised a 12-month residency, 18-month residency, or a rotation within a residency. Preceptors also reported if their residents focused on orthotics, prosthetics, or both disciplines simultaneously.
Resident qualities
For resident characteristics, respondents were asked to rank-order, from most to least influential, their general clinical skills and behavioral traits that promote entrustment decisions. These prompts reflected both ad hoc and summative entrustment factors (Table 1).
Overall entrustment versus length of residency versus discipline
Preceptors reported at what time during residency they start entrusting residents with clinical tasks within the ABC Practice Analysis domains (patient assessment, formulation of treatment plan, implementation of treatment plan, follow-up to treatment plan, documentation, and practice management; promotion of competency/enhancement of professional practice was excluded since the domain primarily takes place out of daily patient care) with direct and indirect supervision. In order to clearly delineate the time frames for entrustment, we divided residencies into milestones, loosely based upon the NCOPE 1 requirement for quarterly evaluations. Additional division was added to the beginning of the residency in order to capture the period in which supervisors assess a resident’s baseline knowledge and skills. The 12-month residencies were divided into seven milestones (first day, first week, first month, second quarter, third quarter, fourth quarter, and never), 18-month residencies into nine milestones (first day, first week, first month, months 4–6, months 7–9, months 10–12, months 13–15, months 16–18, and never), and rotational residencies into five milestones (first day, first week, midway through rotation, within the last few weeks of rotation, and never).
Data analysis
Data were analyzed with SPSS Statistics Version 24 (IBM Corp, Armonk, NY, USA). Descriptive statistics were generated, and the following factors were analyzed: preceptor age, gender, discipline of overseen residency, resident behavior qualities, resident developmental qualities, progression of percent of overall entrustment based on discipline, and direct or indirect supervision versus progression of residency based on length (12-month, 18-month, or rotation—typically less than 12 months).
Results
Preceptor demographics and residency characteristics
Of 831, 77 (9%) of NCOPE-certified preceptors completed the survey. There were 15 respondents who reported they supervised only orthotic residents, 15 respondents who supervised only prosthetic residents, and 47 respondents overseeing both O&P residents (Figure 1(a)). Most preceptors identified as male (80.5%), with the remainder identifying as female, and the majority of both genders overseeing both O&P residents (Figure 1(b)). Most respondents were between 30 and 69 years old (Figure 2), with the age range of 60–69 years being the most frequently selected. About 71% of preceptors indicated they oversaw 12-month residencies, 20% indicated they oversaw 18-month residencies, and 26% reported they oversaw rotational residencies (Figure 1(a)). Of the preceptors overseeing rotations, seven reported they oversaw residents in 2- to 3-month periods, one reported a weekly rotation, three reported between 6 and 12 months, and two reported 2 years (two 12-month, single-discipline residencies). There were 12 preceptors who oversaw more than one length of residency, but none oversaw all three lengths of residency. Rotational programs included rotations between different companies and preceptors, or rotations within the same organization at different locations and/or with different preceptors.
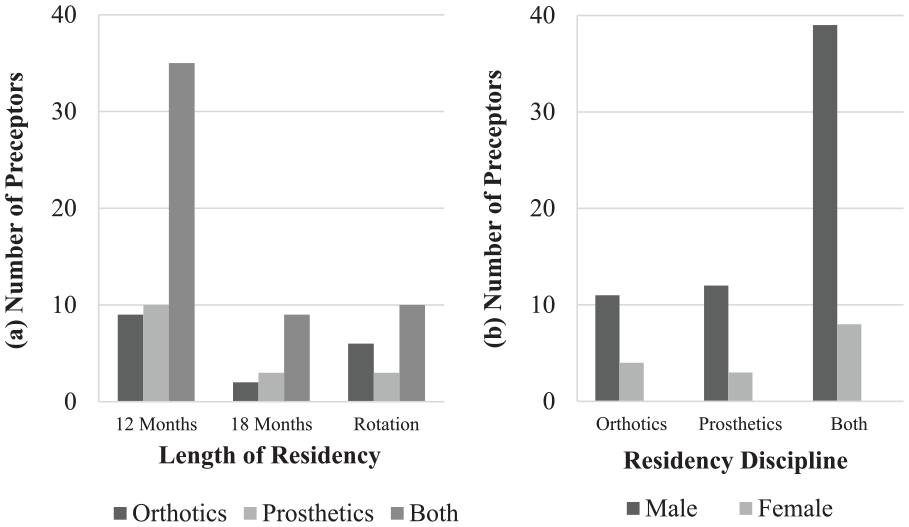
Types of residencies overseen by preceptor respondents, based on (a) duration of the residency and (b) residency discipline.
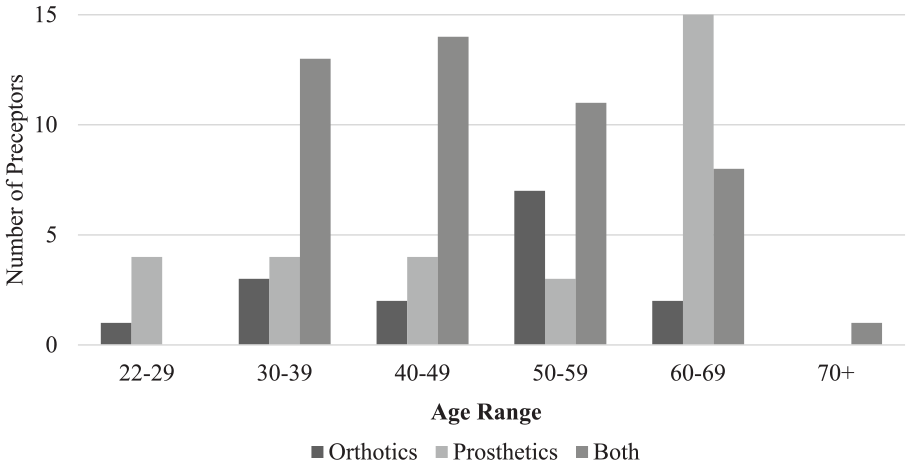
Age of preceptor respondents by residency discipline.
ABC practice analysis domains
Preceptors were asked to rank the ABC Practice Analysis 11 domains from most important to least important to resident success (Figure 3). Most respondents chose patient assessment as the most critical domain (82.0% chose it as the most important), followed by formulation of treatment plan (63.3% chose it as the second most important), and implementation of treatment plan as the third most critical domain (53.2% chose it as the third most important). The promotion of the competency/enhancement of professional practice domain was ranked as being the least critical to resident success (64.6% chose it as the least important).
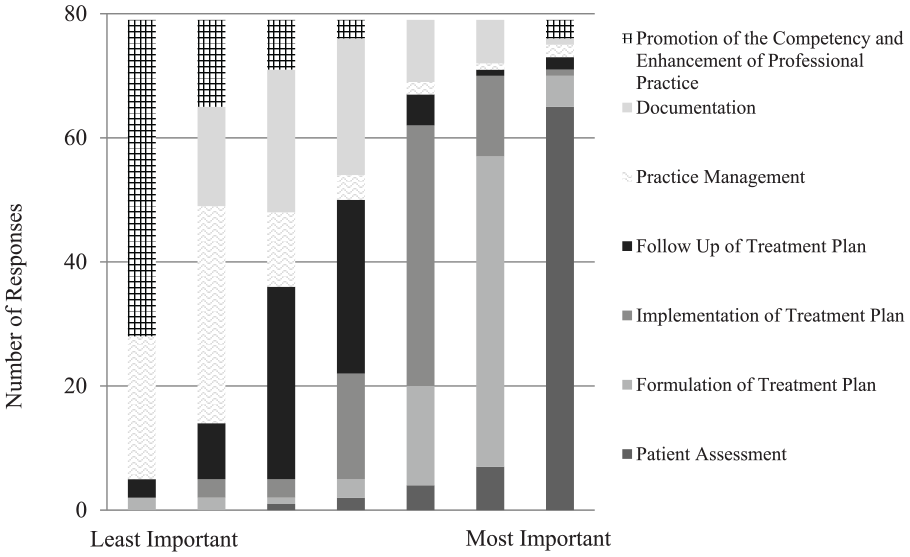
Preceptor respondent rankings of which practice domains contributed most to resident success, from least important (left) to most important (right).
Resident qualities
Most preceptors (56.3%) selected ‘recognition of limitations and willingness to ask for help’ as the resident behavioral quality that indicates progression toward independence followed by ‘residence competence’ (46.3%) (Figure 4). These were closely followed by ‘self-evaluation, reflection, and development’ (33.8%), ‘sense of responsibility’ (32.5%), and ‘ability to effectively address mistakes’ (32.5%). For resident developmental skills, 27 preceptors selected ‘evaluation skills’ as the most critical skill for residents (32.5% ranked it as most important), followed by ‘interpersonal skills’ (38.8% ranked it as second most important), and ‘knowledge and plan formulation skills’ (25.0% ranked it as third most important) (Figure 5). Technical skills were ranked as the least important skill (56.3% ranked it as fifth most important out of five).
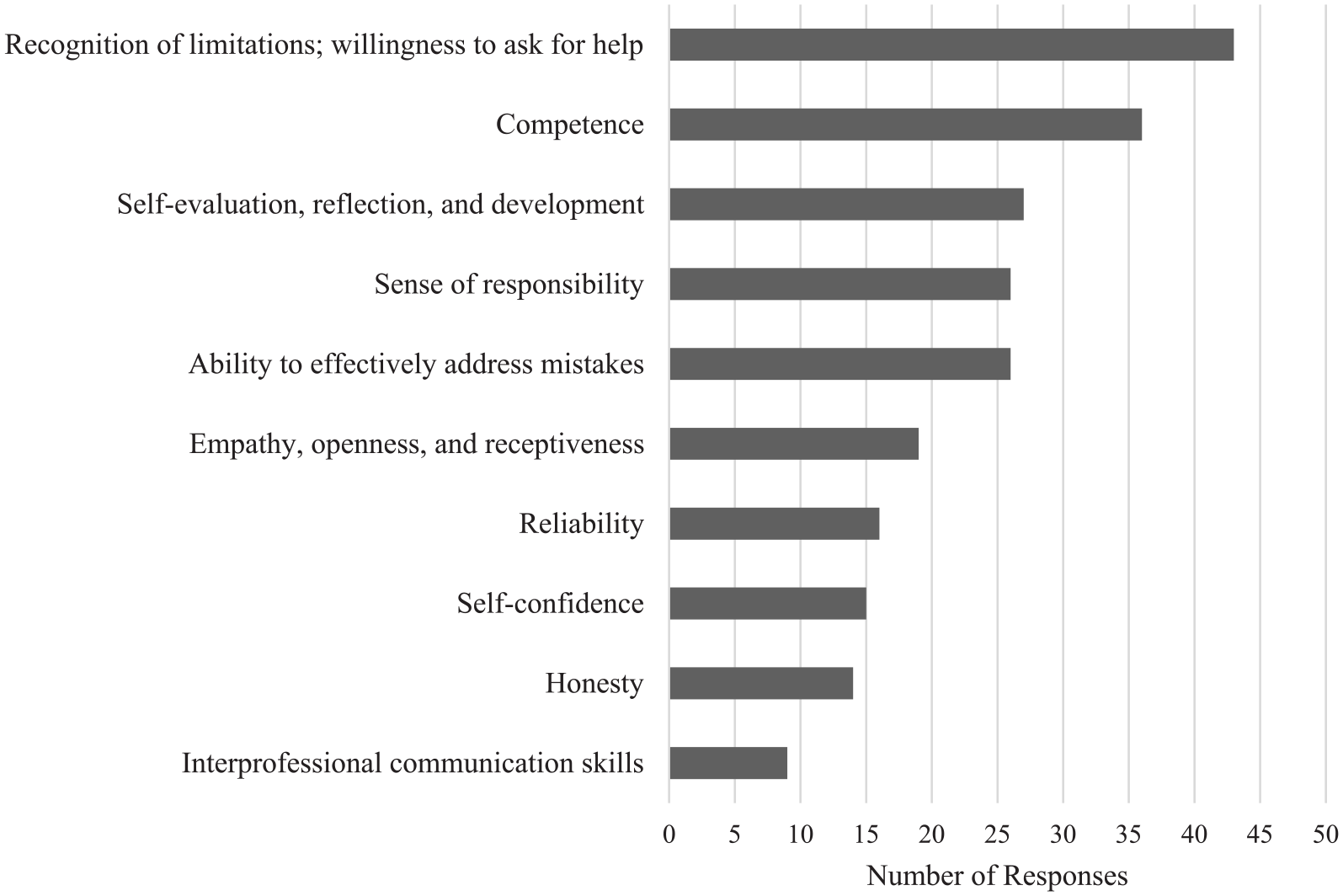
Behavior qualities deemed to be most critical in determining entrustment. Preceptors were asked to select their top 3 choices.
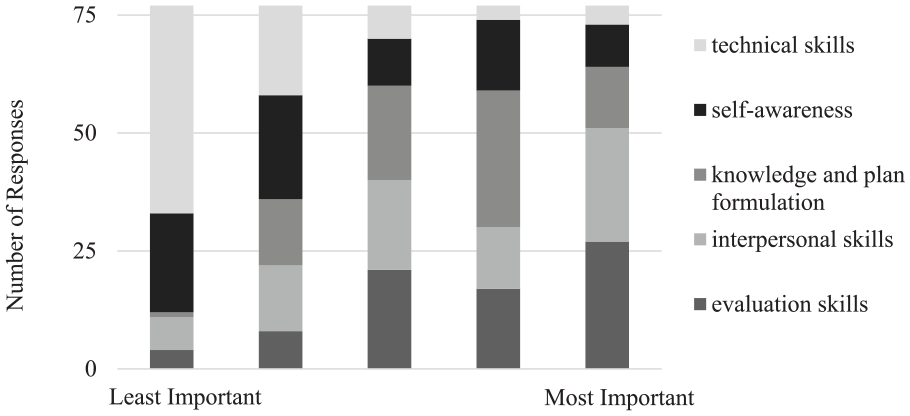
Preceptor respondent rankings of which skills determine resident entrustment.
Overall entrustment versus length of residency
Rates of entrustment to indirect supervision increased similarly across 12- and 18-month residencies (Figure 6). In both lengths of residency, documentation was the domain of patient care most frequently entrusted at the earliest time point in the residency. In all, 75% of preceptors in 12-month residencies and 99.9% of preceptors in 18-month residencies reported allowing residents to document with indirect supervision by halfway through the residency. By the fourth quarter of a 12-month residency, all but one respondent indicated they provided indirect supervision for patient assessment, plan formulation, implementation, follow-up, and documentation. In all, 14% of preceptors in 12-month residencies never allowed residents to conduct practice management with indirect supervision. By 15 months into the 18-month residency, 99.9% of respondents reported providing indirect supervision to residents in patient assessment, plan formulation, implementation, follow-up, and documentation. In all, 21.2% of preceptors in 18-month residencies never allowed residents to perform practice management with indirect supervision.
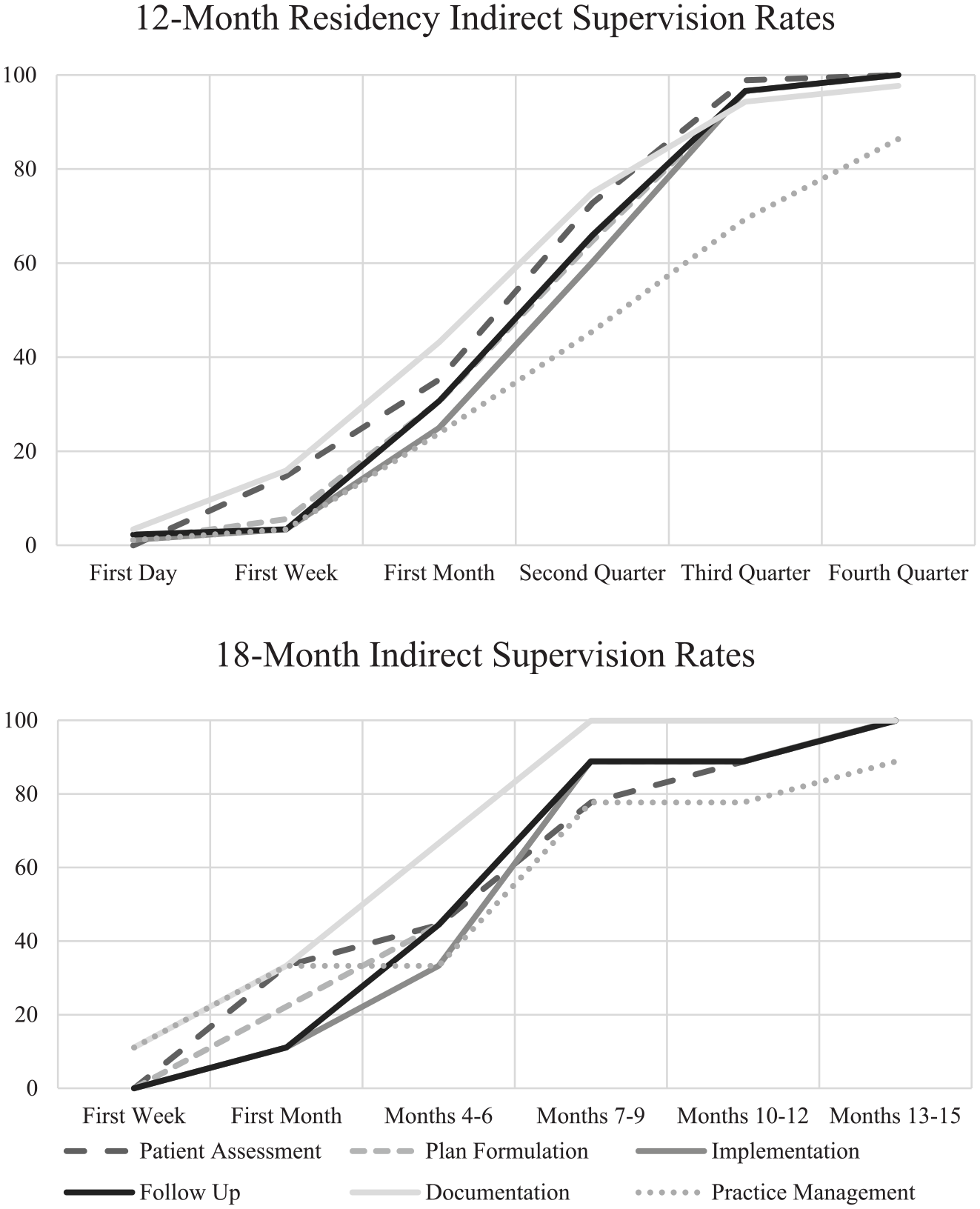
Cumulative percentage of preceptors who reported entrusting residents with indirect supervision in each domain of patient care.
Discussion
This study determined multiple entrustment factors that residency directors and mentors use when transitioning a resident from observation to direct supervision, and from direct supervision to indirect supervision. We found that residency preceptors indicated intrapersonal skills and patient evaluation skills highly affected their decision to progress a resident, whereas interprofessional communication and technical skills affected entrustment the least. Preceptors generally entrust residents with the majority of tasks by a point midway through the residency.
Most preceptors prioritized educating residents about patient assessment above all other domains. Arguably, if a resident cannot assess a patient correctly, it will be more challenging to provide optimal care to the patient. Preceptors also prioritized formulation, implementation, and follow-up of the treatment plan, which reflects the importance of making sure the patient’s needs are met. Our findings align with the ABC Practice Analysis, which reported that orthotists spend the most time on patient assessment and prosthetists spend the most time on implementation of the treatment plan. 11
For resident behavioral qualities, ‘recognition of limitations and willingness to ask for help’ was ranked as the most valued quality that influences the amount of entrustment awarded to a resident. Preceptors likely have increased confidence in clinical residents with strong intra- and interpersonal skills. Other healthcare providers have noted the importance of ability, humility, integrity, and reliability in making entrustment decisions.12,13 Reciprocally, clinical students in other health professions have noted increased satisfaction with clinical educators who demonstrate superior interpersonal skills, model professional behavior, and execute effective teaching strategies.14,15 For developmental competencies, clinical skills such as ‘patient evaluation skills’ and ‘interpersonal skills,’ as opposed to ‘technical skills,’ predicted resident progress toward independence, reflecting the profession’s focus on patient care. 16 Spaulding et al.’s 17 conceptual framework for O&P education supports our findings that, despite historical precedence, technical skills are only a portion of skills required to provide patient-centered care. In this context, results of our study suggest that it is important for residents not only to exhibit technical skills, but also to possess strong evaluation and interpersonal skills when making clinical decisions.
Overall entrustment of clinical responsibilities was similar between 12- and 18-month residencies. This finding shows that, over the longer residencies, the amount of entrustment over the same relative percentage of the supervision period increases at similar rates. By three-quarters of the way through a residency, most preceptors reported allowing residents to perform all domains of patient care with indirect supervision. Documentation, a domain of patient care that does not necessarily involve direct patient contact, was the earliest skill to be entrusted, followed closely by follow-up, implementation, patient assessment, and plan formulation. Variation in entrustment practices could be due to a lack of clarity on activities related to each domain and individual differences between residents and clinical preceptors. 13 Future research is needed to determine normative standards in resident experiences, milestones, and time periods by which a preceptor should expect to be able to provide indirect supervision to a resident.
Notably, 15% of preceptors indicated not allowing residents to perform practice management with only indirect supervision. ABC defines practice management as ‘adherence to policies and procedures regarding human resources, physical environment, business and financial practices, reimbursement requirements and organizational management.’ 11 The tasks within this domain represent the responsibilities of a clinic manager or business owner. The description of this domain specifically notes adherence to policies, rather than determination of, policies; the variability of interpretation of this description likely accounts for preceptors indicating a lack of complete entrustment.
As noted above, one important limitation to this study was the response rate. The goal sample size was over 200 with expected 30% response rate for a sample size of 831. Less than half of the desired responses were collected. 18 Therefore, external validity is limited, and a larger sample size is needed to determine whether these findings accurately reflect the general views of residency supervisors. Furthermore, comparisons between types of residency (i.e. 12-month, 18-month, and rotational) were challenged by the varying number of time-point milestones we used for the same question in the survey (i.e. 7, 9, and 5, respectively). This inconsistency made it difficult to directly compare responses from preceptors from different types of residencies. We did not explicitly define rotational residency, which may have required respondents to interpret that classification, confounding the data. Other factors not addressed in this study may impact entrustment decisions.
Conclusion
This study examined factors preceptors consider when determining entrustment, as well as typical entrustment trends based on discipline, length of residency, and the amount of supervision provided. These entrustment factors may help preceptors provide actionable feedback to residents, serve as a reference for preceptors and residents to reflect on the residency milestones, and offer insight into how residents most effectively transition from observing to performing with supervision and to performing with indirect supervision. Future studies could continue to explore circumstances in which transitional guidance may help create a more efficient education for the resident while continuing to provide quality patient care. Both the preceptor and resident can use queues and other signs to measure, evaluate, and encourage resident progress at appropriate times.
Supplemental Material
OPEntrustment_Survey_Edited – Supplemental material for Entrustment trends in orthotic and prosthetic residencies
Supplemental material, OPEntrustment_Survey_Edited for Entrustment trends in orthotic and prosthetic residencies by Maria Lourdes Carmela Cruz, Joshua B Utay and Ashley H Mullen in Prosthetics and Orthotics International
Footnotes
Acknowledgements
We would like to thank the staff at the National Commission on Orthotics and Prosthetics Education for supporting this study. In addition, special thanks goes to Dominique Mungo who disseminated the survey to all NCOPE residency mentors and directors.
Author contributions
M.L.C.C. was responsible for data acquisition, analysis, interpretation, and manuscript generation. J.B.U. contributed to development of the survey instrument, interpretation, and manuscript preparation. A.H.M. proposed the design of the work and contributed to data analysis, interpretation, and manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics statement
This study was approved by the Baylor College of Medicine Institutional Review Board (protocol H-39530).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.