
Abstract
Background:
Little is known about the patterns of prosthesis use and satisfaction of those who cease use or begin to use upper limb prostheses.
Objectives:
Among a longitudinal sample of Veterans with upper limb amputation, (1) describe changes in prosthesis use over 1 year, (2) examine rates of receipt of new prostheses, and (3) compare prosthesis satisfaction in respondents who received a new prosthesis to those who did not.
Study Design:
Longitudinal survey.
Methods:
808 Veterans who had participated in a baseline interview 1 year earlier were invited to participate in structured telephone interviews.
Results:
A total of 562 persons with unilateral and 23 with bilateral amputation participated in the interviews (Response rate = 72.4% and 85.2%, respectively). Prosthesis use, frequency and intensity of use, and types of prostheses used were stable over 1 year. About 24% reported using a different primary terminal device type at follow-up than baseline. Prosthesis use was less frequent/intense at baseline among those who discontinued use compared with those who did not (P < 0.05), and less frequent/intense for those who started compared with those who continued using a prosthesis (P < 0.0001). Rates of prosthetic training were higher among those who received a different prosthesis type compared with those using the same type (P = 0.06). Satisfaction scores were higher (P < 0.01) for new prosthesis recipients, and lower at baseline for prosthesis abandoners compared with continued users (P = 0.03).
Conclusion:
Prosthesis abandonment appears to be predicated on dissatisfaction with the device, as well as less frequent/intense prosthesis use. These findings can be used to identify those at risk for prosthesis abandonment and improve their prosthesis experience.
Background
Many cross-sectional studies have examined use and abandonment of upper limb prostheses,1–6 reporting prevalent dissatisfaction, and abandonment in about 26% of the population. 7 A 2018 survey of Veterans with upper limb amputation found that 60% with unilateral upper limb amputation were using prostheses, a rate of use below that reported in prior systematic reviews and studies of Vietnam and recent combat Veterans. 8 While prevalence rates of rejection for myoelectric and body-powered prostheses have been reported as roughly equivalent, 7 rates of terminal device rejection may vary. Rejection rates for myoelectric hands, body-powered hooks, and passive hands have been reported to be 39%, 50%, and 53%, respectively. 9
Our survey of Veterans found 50% with unilateral amputation had discontinued using a prosthesis in the past, with 36% of Veterans abandoning body-powered and 18% abandoning myoelectric prostheses. 8 However, to date, there have been no data to determine how often Veterans change prosthesis types. Cross-sectional studies provide a snapshot of prosthesis use, but do not provide information about use over time. It is likely that in any given year, some will start using a prosthesis, some will stop using prostheses, some will resume using a device after a period of disuse, and some will switch to a new prosthesis type.
Prior research reported that between 2000 and 2010, Veterans received a new upper limb prosthesis every 3.5 years. 10 However, this research did not evaluate whether new prostheses received were of the same type. The relationship between prosthesis satisfaction and switching to or obtaining a new prosthesis has also not been previously examined. In addition, little is known about the patterns of prosthesis use among those who stop using prostheses or those who begin using new ones. Finally, no studies to date have examined the 1-year incidence rates of prosthesis abandonment or uptake, or the factors associated with these events.
Prevalent dissatisfaction with upper limb prostheses among Veterans has been previously recognized. An Office of the Inspector General (OIG) report called for additional research to evaluate the needs of Veterans with upper limb amputations. 11 To meet this need, we conducted the aforementioned survey of Veterans with upper limb amputation. 8 We followed this cohort over 1 year to examine stability and change in prosthesis use and satisfaction over time. This article presents summary findings from this longitudinal study. The purposes were to (1) describe 1 year changes in prosthesis use; (2) examine the rate of receipt of new prostheses and terminal devices; and (3) compare prosthesis satisfaction among prosthesis users who received a new prosthesis to those who did not.
Methods
The structured baseline interview included a representative sample of Veterans with major upper limb amputation who received care in the Veterans Administration (VA) between 2010 and 2015. The VA is a comprehensive, integrated health care system that serves more than 8.9 million U.S. Veterans annually. VA providers prescribe prostheses and amputation rehabilitation services based upon a Veteran’s clinical needs. The VA furnishes authorized items to eligible Veterans through internal VA resources or through an authorized VA vendor or contractor based in the community.
The sampling frame, described in a prior publication, was identified using amputation diagnosis and procedure codes from VA Corporate Data Warehouse (CDW) sources. 8 Those with valid addresses and telephone numbers were contacted by letter and provided an opportunity to opt-out of study participation. Those who did not opt-out were contacted by telephone. Participants provided oral informed consent by telephone prior to participating in the interview. A waiver of documentation of informed consent was obtained from the VA Central IRB. Forty-five-minute structured telephone interviews were conducted at baseline and follow-up by professional interviewers from an academic survey center who were trained by the study PI. Respondents who agreed to participate in future activities were re-contacted 1 year after the baseline interview. Response (RR) and cooperation (CR) rates were calculated using American Association of Public Opinion Research guidelines (AAPOR RR4 and CR4). 12 To assess for potential nonresponse bias, we compared baseline and follow-up respondents to Veterans with upper limb amputation diagnoses identified in the original full sampling frame on data available in CDW (age, sex, and year of most recent encounter at the VA).
Data collection
The content of the interview has been described in detail elsewhere. 8 Items relevant to the analyses presented in this article are described below and provided as supplemental material. The baseline and longitudinal interview contained a demographics section that asked about characteristics including age, sex, marital status, number of children, race/ethnicity, and employment; and a section on amputation that included items on side of limb loss, and amputation level, date, and etiology. For our analyses, we collapsed amputation levels into three groups: (1) TR, which included those with transradial and wrist disarticulation amputation, (2) TH, which included those with transhumeral and elbow disarticulation, and (3) SH, which included those with shoulder disarticulation and forequarter amputation.
The interview also contained questions specific to prosthesis users. Specifically, those who used a prosthesis were asked to identify type of prosthesis and terminal devices that they used, as well as the suspension method. In addition, those who indicated that they used more than one type of prosthesis were asked to identify the primary prosthesis and the prosthesis that they considered their secondary prosthesis. They were then asked how these prostheses were suspended on their body.
Respondents who were current prosthesis users were asked if they had received prosthetic training (yes or no). They were also asked to report frequency of prosthesis use (daily, weekly, monthly, every few months, 1 to 2 times per year), and average hours per day of use. Prosthesis satisfaction was assessed using two measures: the Trinity Amputation and Prosthetic Experience Scale (TAPES) satisfaction scale, and the modified 8-item Orthotics and Prosthetics Users Survey (OPUS) Client Satisfaction with Device (CSD) scale.13–15
Statistical analyses
We conducted descriptive analyses to characterize prosthesis use and changes in use between baseline and follow-up and identified respondents who had ceased using, started using, or continued using a prosthesis. Chi-square analyses were used to compare the proportion of unilateral vs bilateral prothesis users who used two or more prostheses or two or more terminal devices. We examined differences between these groups in terms of days and hours of use with Wilcoxon Mann–Whitney tests. For those who reported using a prosthesis at both baseline and follow-up, we compared days and hours of use at each time point with Wilcoxon signed-ranks tests. For prothesis users with bilateral amputation, prosthesis use of the dominant side was used for analysis. We calculated the proportion of respondents who reported using a different type of primary prosthesis or terminal device in the follow-up and baseline interviews. In these analyses, we utilized the prosthesis and terminal device type of the dominant side for bilateral prosthesis users.
We examined the rates of receipt of a new prosthesis in the year prior to the baseline and follow-up. We also identified respondents who reported a type of prosthesis at follow-up that was not reported at baseline. For those who received a new prosthesis between baseline and follow-up, we used a chi-square test to compare rates of receipt of any prosthetic training between those who received a different prothesis type and those who received a similar prosthesis type. To determine whether there were differences in rates of switching prosthesis types for persons who used body-powered and myoelectric prostheses (the two largest groups), we performed a McNemar’s comparison.
We compared CSD and TAPES satisfaction scores at baseline and follow-up for respondents who were using the same primary prosthesis type and for those who received a new device. Because normality tests of the satisfaction measures all rejected the assumption of normality in this sample, Wilcoxon signed-rank tests were used. We used nonparametric Wilcoxon Mann–Whitney tests to determine whether poorer baseline prosthesis satisfaction predicted prosthesis abandonment 1 year later. We also compared baseline satisfaction scores between respondents who had stopped using a prosthesis in the subsequent year to those who continued prosthesis use. A critical alpha of 0.05 was used for all analyses.
Results
Sampling frame and response rate
Eight-hundred eight persons were interviewed at baseline and 585 at follow-up. Figure 1 shows the reasons for loss to follow-up. The response rate and cooperation rate at follow-up among those who completed the baseline survey was 72.4% and 85.2%, respectively. Table 1 shows the characteristics of follow-up respondents, baseline completers, and those identified as eligible or of unknown eligibility in the initial sampling frame.
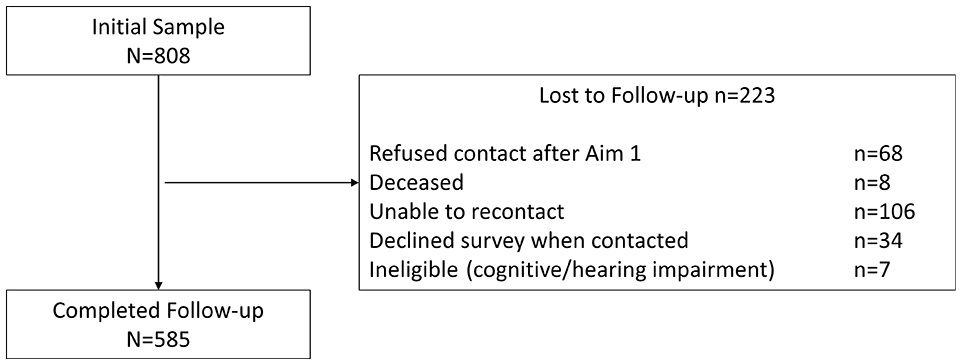
Flow diagram of study participation.
Characteristics of Veterans assumed eligible and those who completed baseline and follow-up interviews.
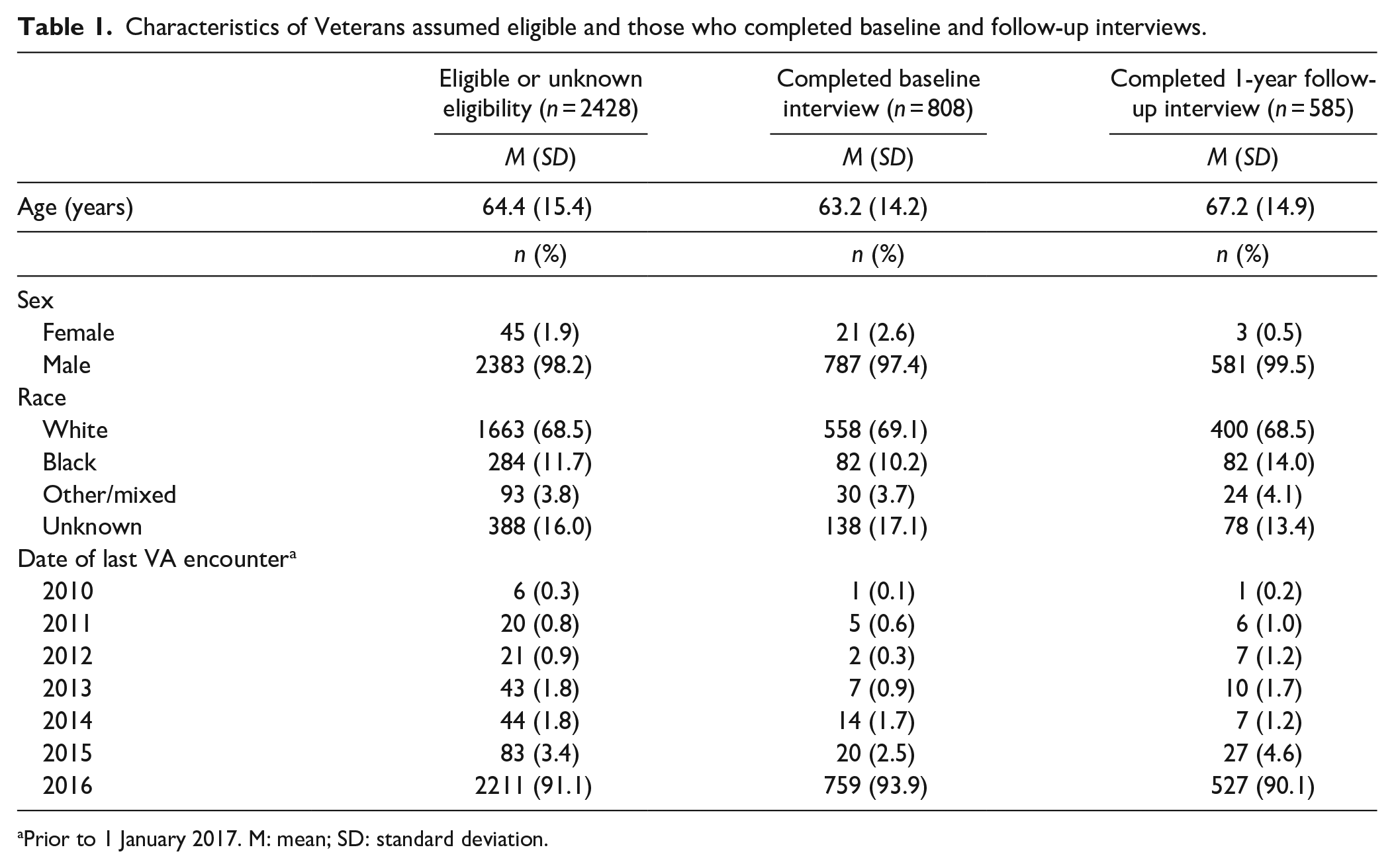
Prior to 1 January 2017. M: mean; SD: standard deviation.
Sample characteristics and prosthesis use
Table 2 compares characteristics of those with unilateral (n = 562) and bilateral (n = 23) amputation in the longitudinal sample. Fifty-two percent (n = 293) of persons with unilateral amputation were classified in the TR group, 37% in the TH group (n = 206) and 11% in the SH group (n = 11). In the group with bilateral amputation, 65% (n = 15) had TR amputation on both sides, 13% (n = 13) had TH amputation on both sides, 9% (n = 2) had TR on one side and TH on the other side, 9% (n = 2) had TR amputation on one side and shoulder level amputation on the other, while 4% (n = 1) had shoulder amputation on one side and TH on the other.
Longitudinal sample: demographic characteristics.
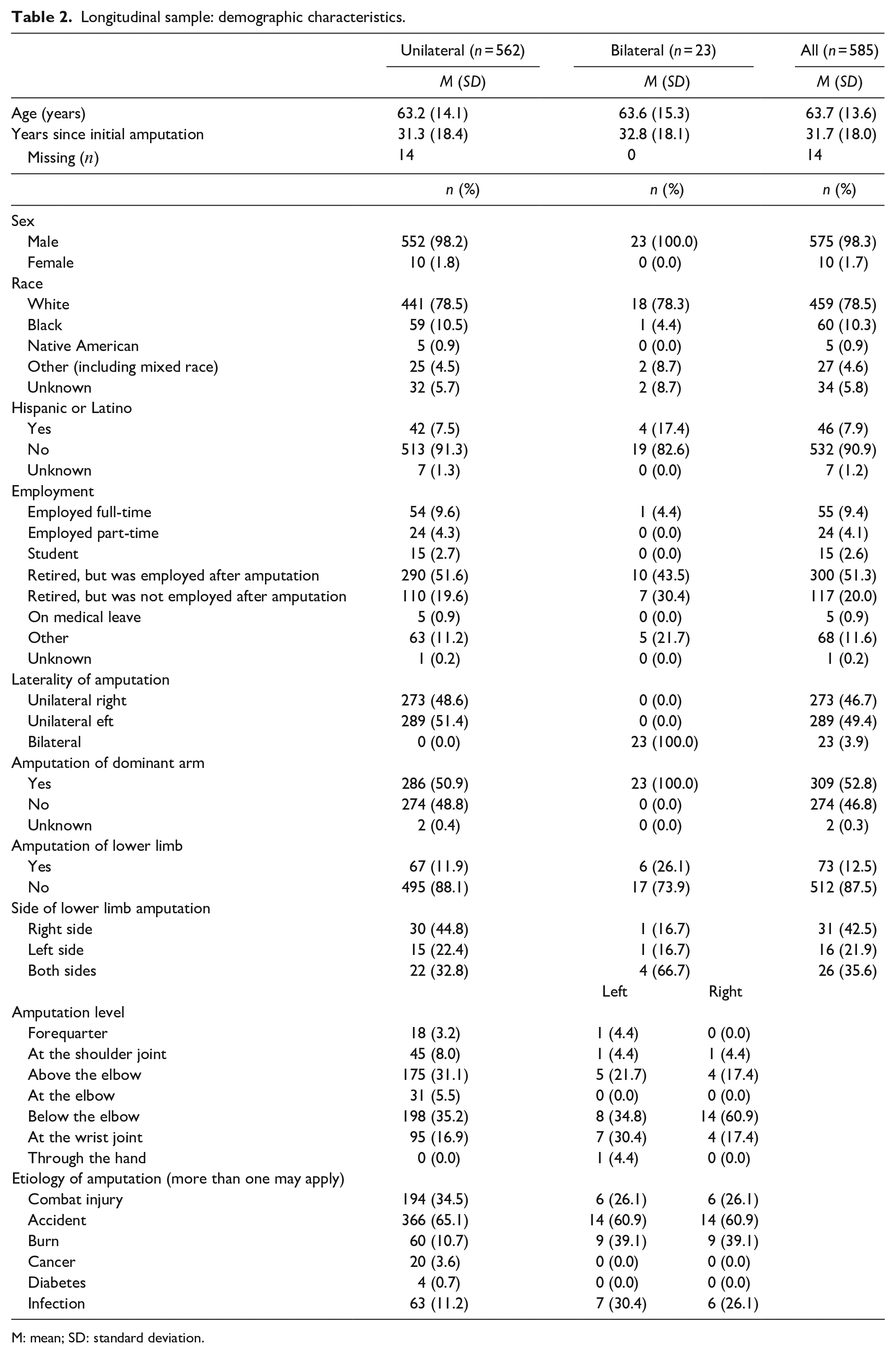
M: mean; SD: standard deviation.
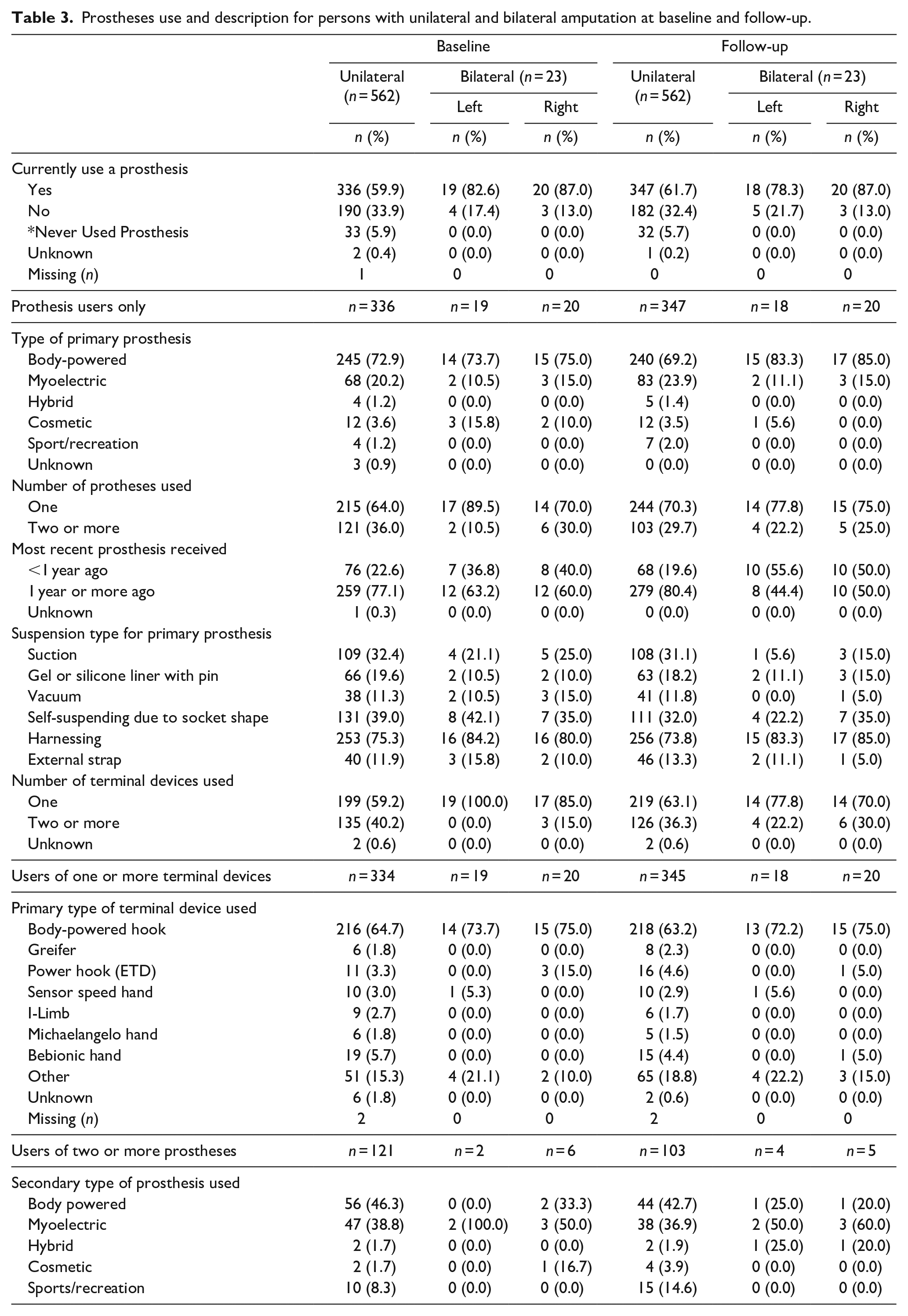
There were no changes in amputation level from baseline to follow-up. Prosthesis use was stable over the 1-year period. Among individuals with unilateral amputation, 59.9% and 61.7% used a prosthesis at baseline and follow-up, respectively (Table 3). 95% of individuals with bilateral amputation used a prosthesis (on at least one side) at baseline and at follow-up. 6% of those with unilateral amputation had never used a prosthesis at either baseline or follow-up. Prevalence of prosthesis types at baseline and follow-up are shown in Table 3. Body-powered devices were used by 73% of persons with unilateral amputation and 75% of persons with bilateral amputation (on at least one side) at baseline and 69% of persons with unilateral amputation and 85% of persons with bilateral amputation at follow-up. Figure 2 shows data for persons with bilateral amputation, showing levels of amputation and the prostheses combinations used. 60% of persons with bilateral transradial amputation used a body-powered device on both sides.
Prostheses use and description for persons with unilateral and bilateral amputation at baseline and follow-up.
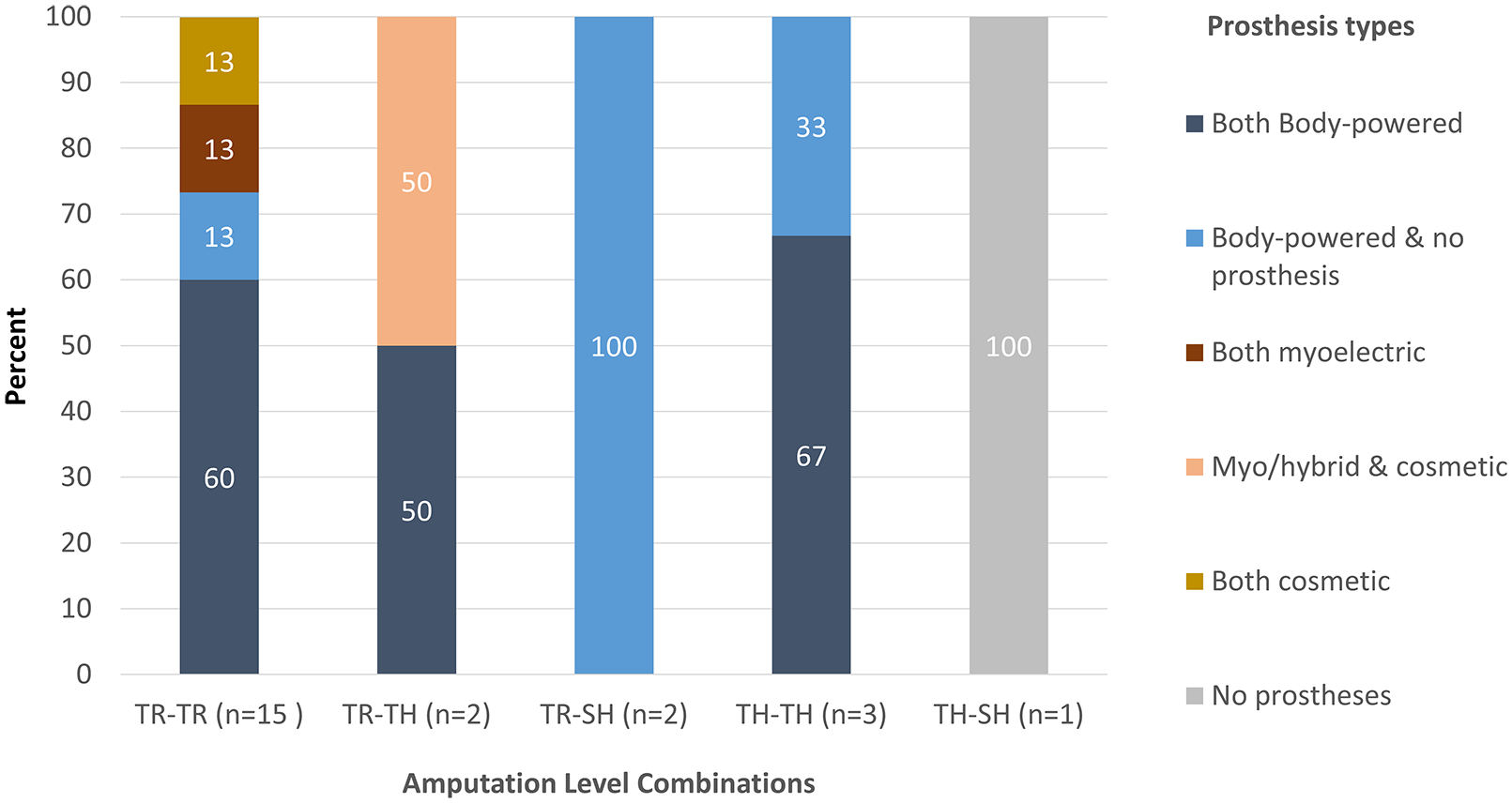
Amputation level and primary prostheses types used for persons with bilateral amputation (n = 23).
The proportion reporting use of multiple prostheses was stable over the 1-year period. 30% of prosthesis users with unilateral amputation used two or more prostheses at follow-up (as compared with 36.0% at baseline), and 22.7% of prosthesis users with bilateral amputation used two or more prostheses on at least one side at follow-up (compared with 27.3% at baseline). Rate of receipt of new prostheses within the past year was stable from baseline to follow-up for those with unilateral (23% and 20%) and bilateral (50% and 50%) amputation. There were no significant differences in the proportion of respondents with unilateral vs bilateral amputation who used two or more prostheses at either baseline (χ2 = 0.48, P = 0.49) or at follow-up (χ2 = 0.77, P = 0.38).
About the same proportion of respondents used multiple terminal devices across the 1-year period. 36% of prosthesis users with unilateral amputation used two or more types of terminal devices at follow-up (40% at baseline). In contrast, 27% of prosthesis users with bilateral amputation used two or more terminal devices on at least one side at follow-up (14% at baseline). The proportions of those using two or more terminal devices was significantly different between those with unilateral vs bilateral amputation only at baseline (χ2 = 6.23, P = 0.01).
Terminal device type and suspension method at follow-up were similar to those at baseline. At follow-up, the most common types of primary terminal devices were body-powered hooks (unilateral: 63%, bilateral: 72% left, 75% right). Multi-degree of freedom terminal devices (including the I-limb, 13 Michaelangelo Hand, 14 and Bebionic) 15 were used by 8% and 4.5% of those with unilateral and bilateral amputation, respectively.
Changes in prosthesis use in prior year
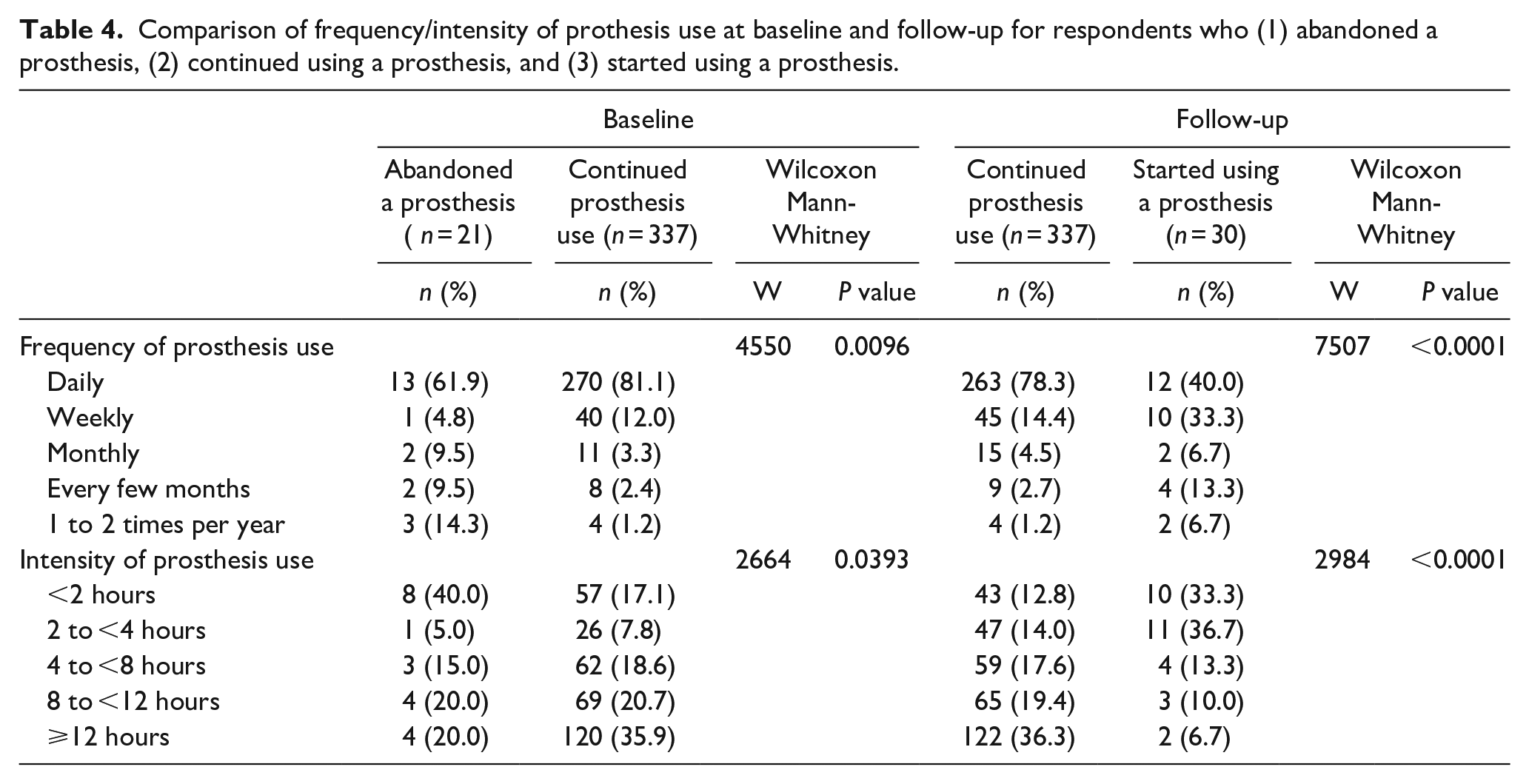
Table 4 shows comparisons of prosthesis use frequency and intensity for the separate sub-groups who (1) ceased using a prosthesis; (2) continued using a prosthesis; and (3) started using a prosthesis between baseline and follow-up. Prosthesis use as reported at baseline was less frequent and less intense among the 6% of prosthesis users who abandoned a prosthesis during the subsequent year as compared with those who did not (P = 0.01). At follow-up, respondents who started using a prosthesis reported significantly less frequent prosthesis use, and fewer hours of prosthesis use compared with those who reported prosthesis use at both time points (P < 0.0001).
Comparison of frequency/intensity of prothesis use at baseline and follow-up for respondents who (1) abandoned a prosthesis, (2) continued using a prosthesis, and (3) started using a prosthesis.
Transition to new type of prosthesis in prior year
The majority of participants with unilateral or bilateral amputation used the same type of primary prosthesis at baseline and follow-up (Figure 3). 12% of myoelectric/hybrid users and 13% of body-powered users reported changing primary prosthesis type between baseline and follow-up. In addition, half of the 14 cosmetic users switched to using either a body-powered (36%) or myoelectric (14%) prosthesis as their primary prosthesis type between baseline and follow-up.
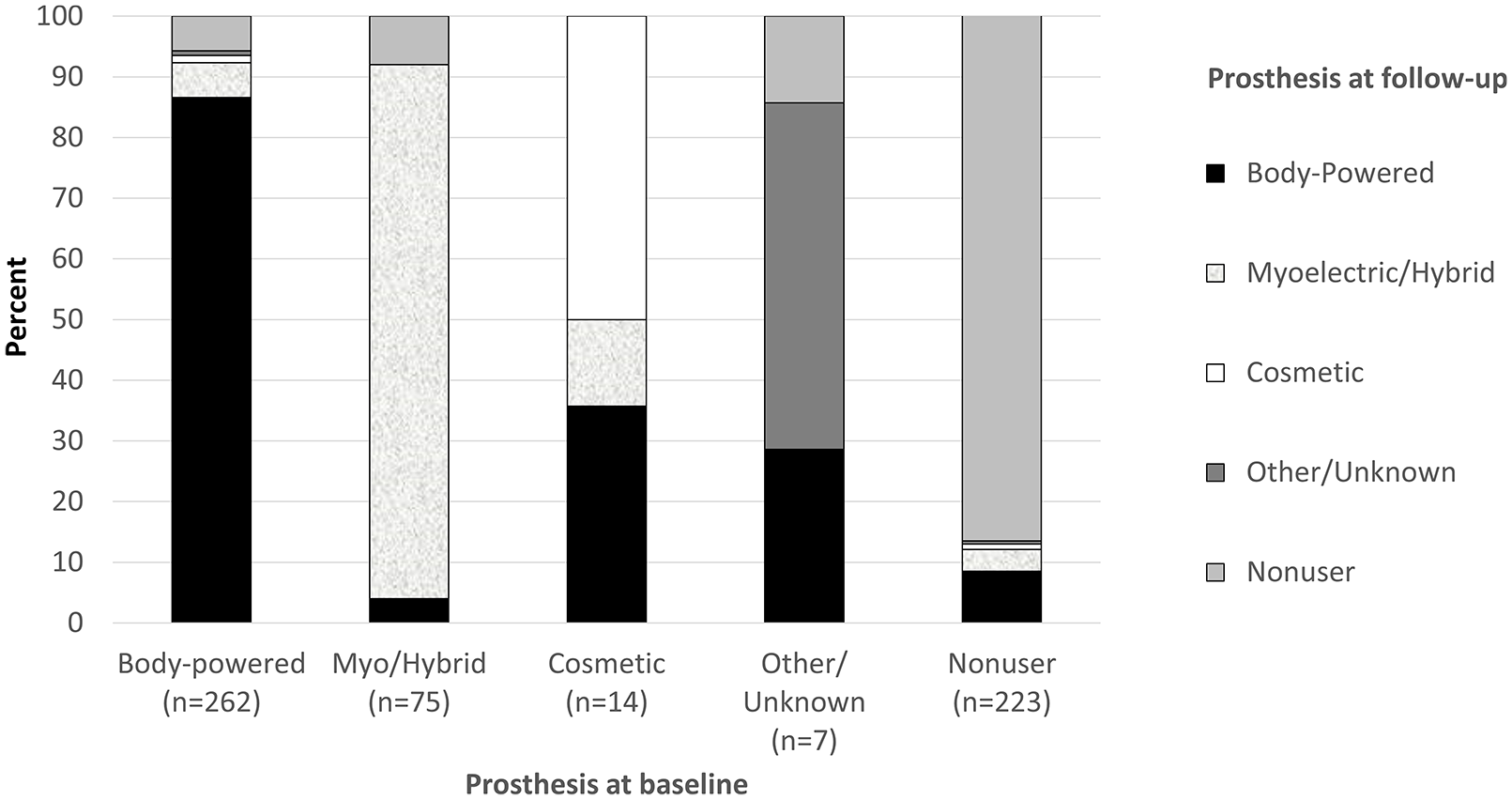
Primary prosthesis type at baseline and follow-up: respondents with unilateral or bilateral amputation (n = 581).
Overall, 24.0% of respondents used a different primary terminal prosthesis type at follow-up and baseline (Figure 4). Specifically, 20% of body-powered users, 40% of sensor speed users, 43% of powered hook users, 50% of unknown type, 58% multi-degree of freedom (DOF) users, and 67% of Greifer users reported using a different type of terminal device at follow-up than baseline. A significantly higher proportion (χ2 = 13.5, P = 0.0002) of body-powered users transitioned to myoelectric devices as compared with myoelectric users transitioning to body-powered prosthesis.
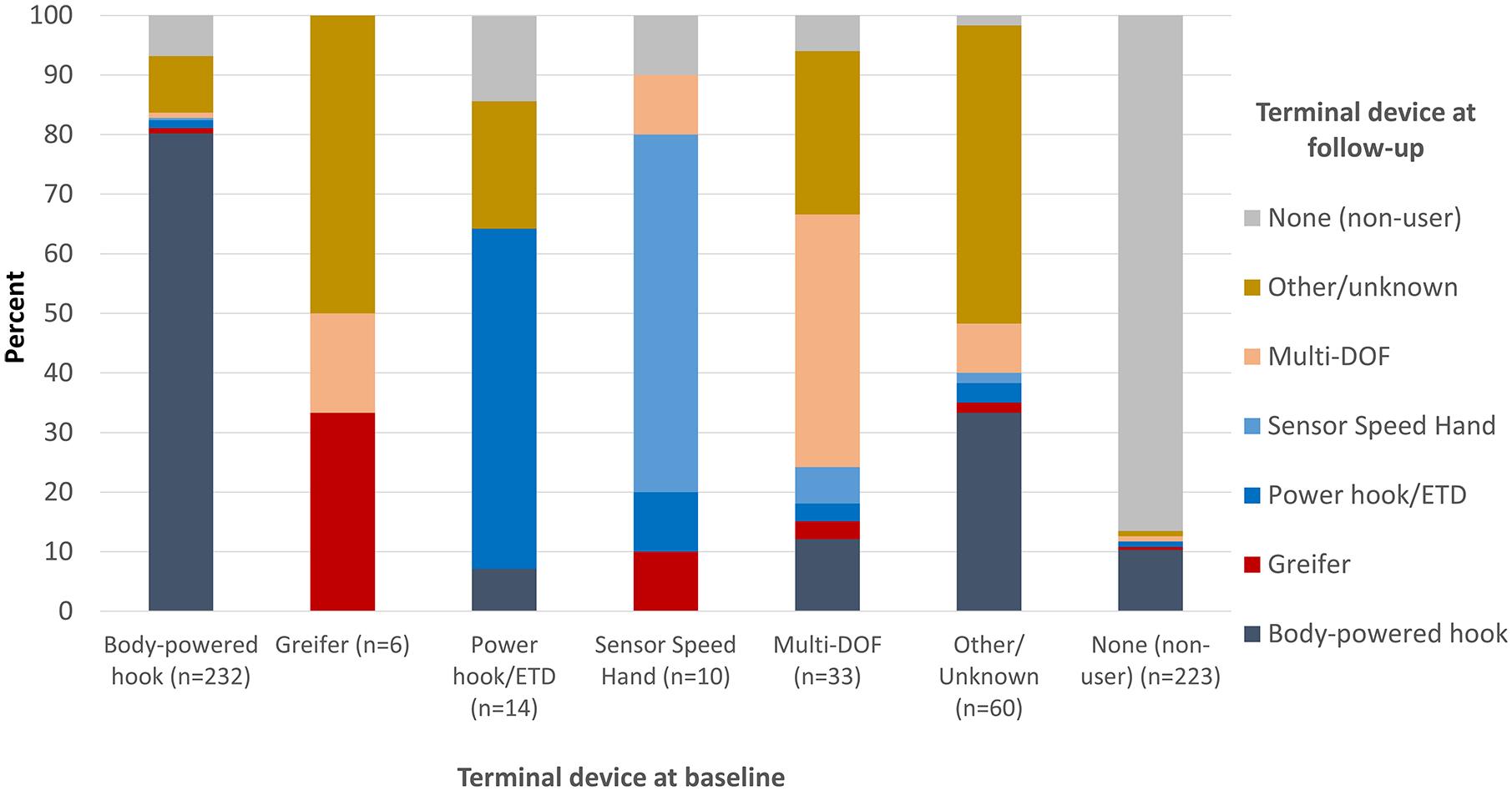
Primary terminal device type at baseline and follow-up: respondents with unilateral or bilateral amputation (n = 578).
Receipt of new prosthesis in prior year
At baseline, 15.1% (n = 122) of participants had received a new prosthesis in the prior year; at follow-up 14.4% (n = 84) had received a new prosthesis. Among follow-up participants who received a new prosthesis, 34.5% (n = 29) received a different prosthesis type than they reported using at baseline.
Training for new prosthesis recipients
Among those who received a new prosthesis at follow-up, rates of training with the new prosthesis were higher among those who received a prosthesis type that was different than any of the types they had reported using at baseline (52%) compared with those who received a previously reported type (31%);
Satisfaction with prostheses
TAPES scores were significantly higher at follow-up (M = 4.0, SD = 0.7) than at baseline (M = 3.6, SD = 0.6) for new prosthesis recipients (S = 466.5, P = 0.002). However, OPUS CSD scores were similar at follow-up (M = 38.2, SD = 17.7) and baseline (M = 40.2, SD = 15.5) with no significant difference (S = -115, P = 0.34). There were no differences in satisfaction scores between baseline and follow-up for those who used the same type of primary prosthesis at both time points (TAPES S = 1701.5, P = 0.18; CSD S = 549.5, P = 0.58). Those who ceased the use of a prosthesis between baseline and follow-up had 0.4 lower TAPES scores at baseline (M = 3.5, SD = 0.8) than those who continued to use a prosthesis at follow-up (M = 3.9, SD = 0.6; S = 2756, P = 0.03). There was no statistically significant difference in baseline OPUS CSD scores between prosthesis abandoners and continued users (U = 4062, P = 0.11).
Discussion
Many cross-sectional studies have examined prosthesis use and abandonment.3,7,16,17 However, no prior study had followed a large cohort of persons with upper limb amputation (including 23 persons with bilateral upper limb loss) over time to observe changes in prosthesis use and satisfaction. Our study followed Veterans with upper limb amputation for 1 year to examine changes in prosthesis use, as well as rates of receipt of new prostheses and terminal devices.
We found that prosthesis use, use of more than one prosthesis, types of prostheses used, terminal device and suspension used, and rate of new prosthesis receipt were relatively stable over 1 year. However, a small proportion of body-powered and myoelectric users (12%–13%) switched primary prosthesis types and more than a third of cosmetic users began using a functional prosthesis. A higher proportion of body-powered users transitioned to myoelectric devices as compared with myoelectric users transitioning to body-powered prostheses. While the small numbers of respondents who transitioned device types precluded further analysis, we believe that studying transitions between prosthesis types may be of interest in future studies.
Respondents who received a new prosthesis type were more likely to receive prosthetic training as compared with those receiving a prosthesis of the same type. However, only 52% of persons receiving a new type of prosthesis received training, which is somewhat surprising, given that prosthetic training is fundamental to rehabilitation of persons with upper limb amputation.18,19 We do not know whether respondents had been offered training and declined it, or if they were never offered training.
We found 14% to 15% of participants received a new prosthesis in the prior year. This figure is almost twice as high as the incidence rate estimated in an earlier study. 10 That study used VA national prosthetics prescription data from 2000 to 2010 and did not include any prostheses received from sources not associated with VA care. 10
Although primary terminal device type was stable across all terminal device types, more than half of participants who reported using a multi-DOF terminal device and more than two-thirds of those who used a Greifer at baseline switched primary terminal device types during the 1-year period. The results related to Greifers should be interpreted cautiously due to the small sample size of Greifer users (n = 6). Given that multi-DOF terminal devices are costly, future studies examining satisfaction with these devices and reasons for discontinuing their use as the primary terminal device are needed.
Our prior analysis of baseline data found no significant differences in prosthesis satisfaction between persons who used body-powered and myoelectric/hybrid devices, and no differences in satisfaction ratings by terminal device used. 20 The current study adds to our understanding of prosthesis satisfaction and its impact on continued prosthesis use. We identified individuals who abandoned a prosthesis between baseline and follow-up and compared intensity of prosthesis use and prosthesis satisfaction with those who continued prosthesis use. Those with lower intensity prosthesis use or poorer device satisfaction scores at baseline were more likely to report abandoning a prosthesis at follow-up. Together, these findings suggest that prosthesis abandonment may not be a sudden act, but instead, is predicated by dissatisfaction with the device, as well as irregular wearing patterns. If those at risk for prosthesis abandonment could be identified in advance, perhaps through regular prosthetic check-ups, targeted efforts to improve their prosthetic experience could be initiated.
Limitations
This is the first longitudinal study of upper limb prosthesis use and utilizes a large, and nationally representative US Veteran population. However, findings are limited to Veterans who received care at the VA and therefore may not be generalizable outside of the Veteran population and the VA system of care. Second, there are some limitations to the interpretation of prosthesis hours of use. Our survey question asked, “How many hours a day do you typically use a prosthesis?” We found that among persons who abandoned their prosthesis during the year, 40% reported using the prosthesis less than 2 hours per day, while 62% reported daily use. While it is evident that the device abandoners were less intense and less frequent prosthesis users, we cannot say with certainty how respondents interpreted this question: whether they reported the hours that they were wearing their device, or the hours that they were actively engaging their device during activities. Our study also did not examine the association between training receipt and outcomes. Future studies are needed to understand the impact of training to use a new prosthesis on prosthesis abandonment and prosthesis satisfaction.
Although we asked respondents about the receipt of a new prosthesis in the prior year, we did not collect data on why a new prosthesis was received, and do not have granular data on device make and model. We expect that many persons who received the same overall type of device had obtained the new device as a replacement for a device that was broken or worn out. However, new devices may have had new or different features and may have been obtained to offer improved or new functionality.
Conclusion
Rates of upper limb prosthesis use, frequency and intensity of use, and types of primary prostheses used by Veterans were stable over 1 year. At follow-up, 15% reported receiving a new prosthesis, 13% used a different primary prosthesis type, and 6% had discontinued prosthesis use. New prosthesis receipt resulted in improved prosthesis satisfaction. Findings suggest that prosthesis abandonment is predicated on dissatisfaction with the device, as well as irregular wearing patterns. These findings can be used to identify those at risk for prosthesis abandonment to improve their prosthesis experience.
Supplemental Material
10.1177_0309364620957920_Supplemental_material – Supplemental material for Longitudinal study of prosthesis use in veterans with upper limb amputation
Supplemental material, 10.1177_0309364620957920_Supplemental_material for Longitudinal study of prosthesis use in veterans with upper limb amputation by Linda Resnik, Matthew Borgia, Sarah Biester and Melissa A Clark in Prosthetics and Orthotics International
Footnotes
Author contributions
The author(s) disclosed the following roles as contributors to this article: LR obtained the funding, designed study methodology, and led data analyses and manuscript draft and revision writing. MB assisted in study methodology, formal analysis and visualization, and wrote portions of the manuscript. SB assisted in study methodology, was responsible for project administration and supervision, and participated in discussions of data analyses and manuscript writing. MAC participated in study methodology, supervised data curation, and participated in data analyses and manuscript writing.
Declaration of conflicting interest
The author(s) disclosed no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded through the Orthotics and Prosthetics Outcomes Research Program Prosthetics Outcomes Research Award under Award No. W81XWH-16-0794 and by A9264S Department of Veterans Affairs Rehabilitation Research and Development Service. The sponsors did not play a role in study design, data collection, analysis, or publication. Opinions, interpretations, conclusions, and recommendations are those of the author and not necessarily endorsed by the Department of Defense or the Department of Veterans Affairs.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.