
Abstract
Background:
Many persons with upper limb amputation reject prostheses, and many are not satisfied with their devices. Research is needed to understand modifiable factors related to device satisfaction. Myoelectric devices with multiple degrees of freedom are now available; however, no studies have examined whether they lead to greater device satisfaction. Prosthetic training contributes to more skillful prosthesis use and greater likelihood of long-term use; however, the relationship between training and device satisfaction is unclear.
Objectives:
(1) To describe and compare satisfaction by prosthesis and terminal device type and (2) to identify factors associated with satisfaction.
Study design:
Cross-sectional study.
Methods:
Participants were 449 persons with unilateral upper limb amputation who used a prosthesis. Participants described their prostheses, prosthetic training, device repairs, visits to a prosthetist, and rated device satisfaction using two standardized measures (Trinity Amputation and Prosthesis Experience Scales Satisfaction scale and Orthotics and Prosthetics Users’ Survey - Client Satisfaction with Devices scale). Multivariate generalized linear regression models examined the relationship between prosthesis and terminal device type and satisfaction, controlling for covariates that were meaningful in bivariate analyses.
Results:
There were no differences in satisfaction by prosthesis type or terminal device degrees of freedom. Satisfaction was associated with receipt of training to use the initial prosthesis, amputation level, age, and race.
Conclusion:
No differences in satisfaction by device or terminal device type were observed. Worse satisfaction was associated with more proximal amputation level, younger age, and black race. The association between receipt of initial prosthetic training and device satisfaction points to the critical role of occupational or physical therapy in the early stages of prosthetic care.
Clinical relevance
Prosthetic satisfaction did not vary by device or terminal device degrees of freedom. Proximal amputation level, younger age, and black race were associated with lower prosthetic satisfaction. Receipt of initial prosthetic training was associated with greater device satisfaction, pointing to the critical role and lasting impact of early training.
Background
Many persons with upper limb amputation abandon or reject their prostheses, and a substantial proportion of prosthesis users are not satisfied with their devices.1–5 Surveys have identified factors associated with dissatisfaction such as problems with function, comfort, fit, and device weight.1,5–7 Many wish their prostheses had features such as powered wrist movement and multiple grip patterns.8,9 Limited powered wrist movement is available through some myoelectric/hybrid devices, and myoelectric devices with multiple degrees of freedom (DOF) have become commercially available. However, no studies have examined whether greater functionality offered by new technologies is associated with greater device satisfaction.
Some data suggest that individuals using prostheses with advanced technologies are not more satisfied with their prostheses than individuals using older technologies. For example, Veterans who lost their limbs in combat in Operation Enduring Freedom and Operation Iraqi Freedom, a group with greater access to prostheses with more advanced technologies, are not more satisfied with their prostheses than Vietnam era combat Veterans with amputations. 10 Additional research is needed to understand influences on device satisfaction, particularly factors that might be modified to improve patient experience and enhance device adoption. Prosthetic training is an essential aspect of rehabilitative care 11 and contributes to more skillful prosthesis use 12 and greater likelihood of long-term use.13,14 However, the relationship between training and device satisfaction has not been studied.
A recent study of Veterans with upper limb amputation collected detailed data on prosthesis satisfaction. Results about satisfaction with prostheses, comparing satisfaction ratings of persons with unilateral and bilateral amputation, 15 and device satisfaction by gender 16 have been reported. However, these studies have not compared satisfaction by prosthesis configuration or examined the relationship between initial prosthesis training and device satisfaction. Thus, the objectives of this study were to (1) describe and compare device satisfaction by device type in a national sample of Veterans with upper limb amputation and (2) identify factors that are associated with device satisfaction. We hypothesized that prosthesis satisfaction would be associated with primary device type, terminal device DOF, and receipt of training to use the device.
Methods
Study design
The study, approved by the Department of Veterans Affairs (VA) Central Institutional Review Board (IRB) and the University of Massachusetts Medical School IRB, was a telephone administered survey, described in detail elsewhere. 15 Participants, identified from the VA’s Corporate Data Warehouse (CDW) sources, were Veterans with major upper limb amputation who received any type of medical or clinical care in the VA between 2010 and 2015. 15 Eligible participants were alive, with valid telephone numbers and addresses with no significant cognitive or hearing deficits preventing participation by telephone. Participants gave verbal informed consent before participating in the survey. Results reported here are for the subset of respondents with unilateral amputation using a body-powered, myoelectric, hybrid, or cosmetic prosthesis.
Measures
Dependent variables
We used two measures of prosthesis satisfaction: the Trinity Amputation and Prosthesis Experience Scales Satisfaction scale (TAPES-SAT) 17 and the Orthotics and Prosthetics Users’ Survey (OPUS) Client Satisfaction with Devices scale (OPUS-CSD). 18 The 10-item TAPES-SAT addresses color, shape, noise, appearance, weight, usefulness, reliability, fit, comfort, and overall satisfaction. 17 Respondents rate items on a 5-point scale (1 = very dissatisfied, 5 = very satisfied). The TAPES-SAT content and scoring were developed for persons with lower limb amputations; however, its structural validity was examined and scoring modified for persons with upper limb amputation. 17 The TAPES-SAT summary score is the average of item ratings.
A variety of studies have evaluated the measurement properties of non-English (translated) versions of the 11-item OPUS-CSD,19–25 with some recommending removal of several items. 22 Additional research on the structural validity of the OPUS-CSD is needed. We administered the original OPUS-CSD in the survey, but decided to use a modified version after conducting Rasch analysis (using Winsteps version 4.4.2) of the original version. We removed two items (affordability of purchase and repair costs) due to dimensionality issues. We also dropped an item addressing wear and tear on clothing because of item misfit (Mms outfit > 2.0). The eight items in the modified scale address satisfaction with: fit, weight, comfort, donning ease, appearance, durability, skin irritation, and pain. Respondents use a 4-point scale (1 = strongly agree, 4 = strongly disagree) with higher OPUS-CSD scores indicating less satisfaction. The 8-item OPUS-CSD Rasch measure had a person separation of 0.82 and 10.7% of unexplained variance in the first residual factor from a principal component analysis (PCA). The Rasch score can be calculated from the total score using the complete score-to-measure table shown in the Supplemental Appendix Table 1. We evaluated the three items dropped from the 8-item summary scale separately.
We also administered seven new items, which we believed were important elements of prosthesis satisfaction not addressed in the TAPES-SAT or OPUS-CSD. These items addressed satisfaction with terminal device size, prosthesis size, self-consciousness wearing the prosthesis, desire to change to another prosthesis type, inability to wear the prosthesis because of fit, satisfaction with device movement, and unintended movement. Respondents used a 4-point scale (1 = strongly agree, 4 = strongly disagree).
Independent variables: prosthesis type, characteristics, and training
Primary prosthesis type was categorized as body-powered, myoelectric/hybrid, or cosmetic based on responses to items about primary prosthesis and terminal device type.
Respondents also answered questions about number of devices and terminal devices used, when the most recent device was received, and whether they received training with the initial and/or current device (yes/no).
Frequency of prosthesis use was classified as daily, weekly, monthly, every few months, and 1–2 times/year. Intensity of prosthesis use was categorized as <2 h, 2 to <4 h, 4 to <8 h, 8 to <12 h, and >12 h. The most recent date a prosthesis was received was categorized as <2 years, ⩾2 years, and unknown. Number of prostheses and terminal devices used was categorized as 1, 2 or more, or unknown.
Respondents indicated whether their primary terminal device was a body-powered hook, Greifer, powered hook, sensor speed hand, I-Limb/Michaelangelo or Bebionic hand, Cosmetic hand, or unknown. Because of small sample sizes, we collapsed terminal device categories based on device DOF. Cosmetic devices were classified as 0 DOF, while hooks, electronic terminal devices (ETDs), Greifers and sensor speed hands, and unknown myoelectric terminal devices types were categorized as 1 DOF, and I-Limb/Michaelangelo or Bebionic hand were categorized as Multi-DOF. Secondary type of prosthesis was classified as body-powered, myoelectric, hybrid, cosmetic, sports/recreation, or unknown.
Receipt of training for initial and for current prosthesis were classified as yes, no, or unknown. The number of times the prosthesis was repaired and number of visits to a prosthetist for socket adjustment in the prior 12 months were classified as 0, 1, 2–3, ⩾4, and unknown.
Participant characteristics
Participant age was evaluated as a continuous variable and categorized as: 18 to <45, 45 to <65, 65 to <75, and ⩾75 years. Gender was self-reported as male or female. Race was classified as white, black, other (which included > 1 race), and unknown. Hispanic ethnicity was classified as yes, no, and unknown. Employment was self-reported as: employed full-time, employed part-time, student, retired but employed after amputation, retired but not employed after amputation, on medical leave, other, or unknown. Marital status was self-reported as married/living together, divorced/separated, widowed, never married, or unknown.
Amputation level was collapsed into a three-category variable for analysis: (1) shoulder (forequarter or shoulder disarticulation), (2) TH (transhumeral or elbow disarticulation), and (3) TR (transradial and wrist disarticulation). Participants indicated the etiology of their amputation using seven yes/no variables: combat injury, accident, burn, cancer, diabetes, infection, and other. The majority (94%) of 244 respondents who indicated “other” etiology provided a description of the etiology. We examined these descriptions among respondents who did not endorse any of the seven provided etiologies and were able to classify etiology in all but two cases. Therefore, we dropped “other” etiology from comparative analyses. Amputation of one or both lower limbs was categorized as yes or no. Participants reported time since initial amputation in years.
Statistical analyses
We described the participant characteristics and prosthesis use characteristics for the overall analytic sample and by type of primary prosthesis used. Descriptive analyses examined the proportion of missing/unknown responses; however, these responses were excluded from subsequent analyses, with the exception of race (which had a high proportion of missing values) and terminal device DOF (classification described above).
Number of repairs and visits to a prosthetist for socket adjustment by primary device type were compared using Kruskal–Wallis tests. TAPES-SAT and OPUS-CSD scores were compared across prosthesis types using one-way analyses of variance (ANOVAs), and Kruskal–Wallis tests were used to compare ordinal ratings of individual items. Tukey’s method was used as a post hoc comparison of any differences in summary scores. Simple general linear regression models (GLM) for TAPES-SAT and the OPUS-CSD were used to examine bivariate relationships with the following participant and prosthesis characteristics: age, gender, race, marital status, amputation etiology, amputation of lower limb, amputation of dominant side, recency of prosthesis receipt, number of prostheses and terminal devices, DOF of primary device, training with initial and current prosthesis, number of prosthesis repairs and adjustment visits in prior year, and frequency and intensity of prosthesis use.
We then constructed multivariate GLM models of (1) TAPES-SAT and (2) the OPUS-CSD score including prosthesis type, and simultaneously controlling for all variables with bivariate association at p < 0.20 with either satisfaction score. We did not include frequency and intensity of prosthesis use because we believed that they were strong consequences of prosthesis satisfaction. Persons who used cosmetic prostheses were excluded from the multivariate analysis due to the small subgroup size (N = 22). We examined assumptions of GLM. Residual plots supported homoscedasticity, specification tests did not reject the assumption of identical and independent error terms, and Durbin–Watson’s statistics also supported the independence assumption. Examination of Q-Q plots supported normality of residuals. Pearson correlations between independent variables were all below 0.4 and the variance inflation factors were below 5.
Results
Sample
Eighty-three percent (N = 808) of those screened eligible were recruited into the main study (Figure 1). The survey response rate and cooperation rate were 47.7% and 63.3%, respectively, as calculated using the American Association for Public Opinion Research methodology. 26 The analytic sample for this report was 449 persons. We excluded 20 participants for whom we had incomplete information on prosthesis use or type of prosthesis, and one participant with conflicting data on type of device used. Nine participants who self-identified as myoelectric or hybrid prosthesis users but specified that they used a body-powered hook as their terminal device were reclassified as users of a body-powered prosthesis type.
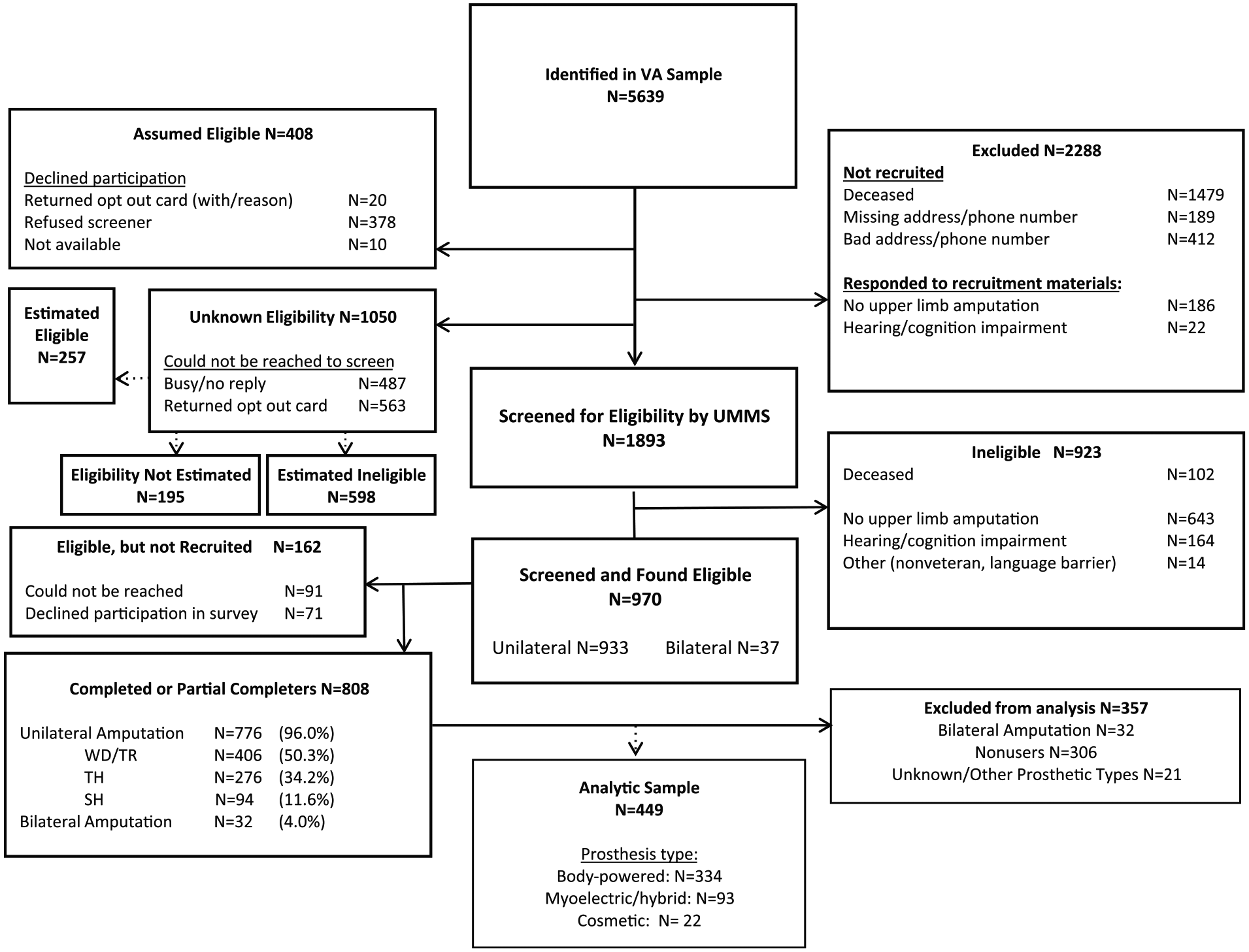
Flow diagram.
The final analytic sample of 429 included 334 (74.4%) body-powered, 88 myoelectric (19.6%), 5 (1.1%) hybrid, and 22 (5%) cosmetic users.
Demographic characteristics
Participants were on average 63.4 years (standard deviation (SD), 13.8) of age, with myoelectric users being the youngest group (mean = 55.6, SD = 15.7) (Table 1). Participants reported an average of 33.5 (SD = 18.2) years since amputation, with myoelectric users having more recent amputations (mean =23.7 years, SD = 17.5). The sample was 98% male. A greater proportion of females were in the cosmetic prosthesis group (13.6%), compared to 1%–2% of females in other groups. The sample was 75% white. A greater proportion of black participants were in the cosmetic group (36.4%) compared to 10% in other groups. Almost 17% of respondents in the myoelectric group were employed full-time versus 10.2% and 9.1% for body-powered and cosmetic users, respectively. Most participants were married or cohabitating (66.4%).
Demographics and amputation–related characteristics by primary device type.
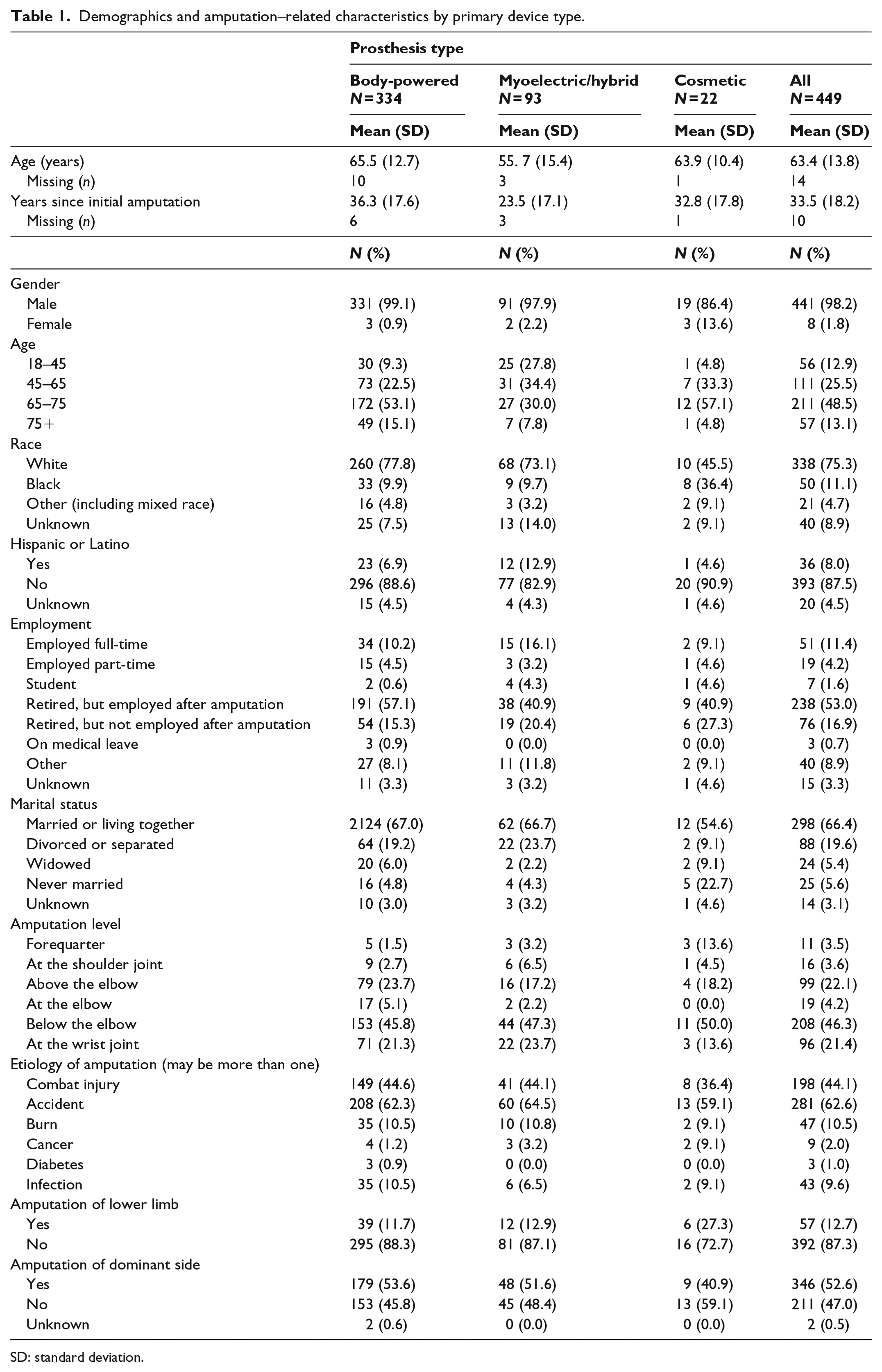
SD: standard deviation.
Amputation level of respondents was 46.3% transradial, 22.1% transhumeral, 21.4% wrist joint, 4.2% elbow disarticulation, 3.6% shoulder, and 3.5% forequarter amputation. A greater proportion with amputation at the forequarter or shoulder level were cosmetic users. The most common amputation etiology was “accident” (62.6%) followed by “combat injury” (44.1%).
Forty percent of body-powered users, 57.0% of myoelectric users, and 27.3% of cosmetic users received their device within the prior 2 years (Table 2). A greater portion of myoelectric users reported use of two or more prostheses (55.9%) or terminal devices (64.5%). Among myoelectric users, 32.3% reported a single DOF terminal device, 43.0% a multi-DOF terminal device, and for 24.7% the terminal DOF was unknown.
Prosthesis use characteristics.
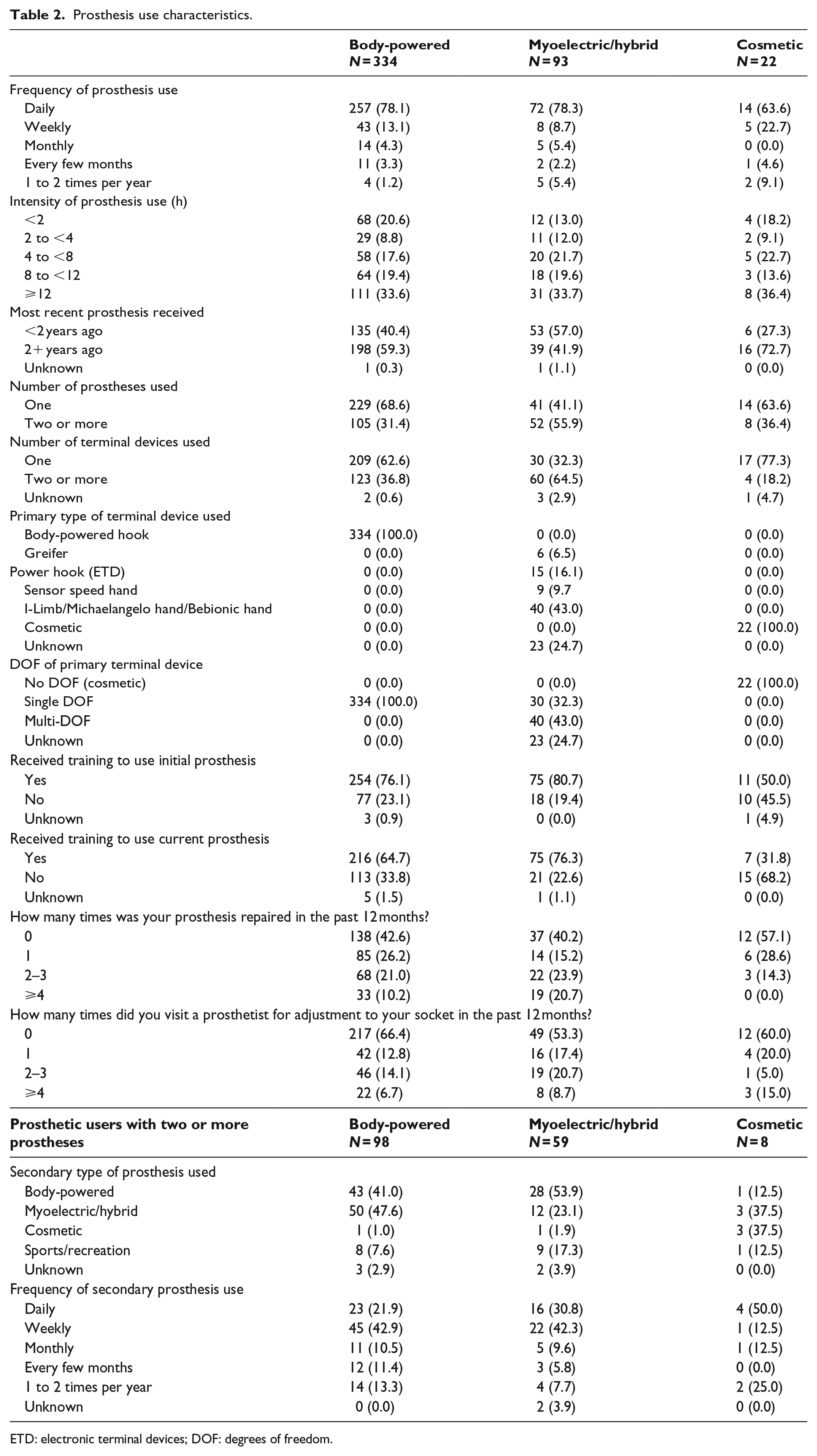
ETD: electronic terminal devices; DOF: degrees of freedom.
Eighty-one percent of myoelectric users reported receiving initial prosthetic training and 76.3% received current device training. In contrast, 76.1% of body-powered users received initial training and 64.7% current training, while among cosmetic users 50.0% received initial training and 31.8% current training.
Myoelectric users were more likely to report two or more repairs in the past 12 months as compared to other device type users, and cosmetic users reported the fewest. There was no meaningful association between prosthesis type and visits for socket adjustments. Among respondents using two or more prostheses (N = 165), the most common secondary devices for body-powered users were myoelectric prostheses (48%), while the most common secondary devices for myoelectric users were body-powered prostheses (54%). Secondary devices of cosmetic users were distributed between myoelectric and additional cosmetic prostheses (37.5% each). There was no significant difference in prosthesis use intensity or frequency by primary prosthesis type, with 63.6%–78.3% reporting daily device use (Supplemental Appendix Table A.2).
Satisfaction outcomes
Results of bivariate analyses show that TAPES-SAT summary scores (Supplemental Appendix Table A.3) varied by prosthesis type (DF = 2, F = 3.42, p = 0.03) though post hoc analysis revealed no significant group differences. Ratings of color, noise, appearance, weight, reliability, and overall satisfaction items also varied by prosthesis type; body-powered users reported the highest satisfaction. Ratings were lowest among myoelectric users for items assessing weight, reliability, and overall satisfaction. Satisfaction ratings for color and noise were lowest among cosmetic users.
The OPUS-CSD summary scores did not differ by prosthesis type in bivariate analyses; however, there were differences in two items. Cosmetic users disagreed more with “my prosthesis looks good,” while users of body-powered devices agreed most with “my prosthesis is durable.” Body-powered users disagreed most with the original OPUS-CSD item, “my clothes are free of wear and tear.” Cosmetic users disagreed most with “I am self-conscious about wearing my prosthesis,” and with “I am satisfied with the way my primary prosthesis and terminal device moves.” Myoelectric users agreed most with, “my primary prosthesis sometimes moves in a way that I do not intend it to.”
Bivariate analyses identified the following variables as associated (p < 0.20) with either the TAPES-SAT or OPUS-CSD scores: amputation level, type of prosthesis, age, race, marital status, etiology of amputation (burn, cancer, and diabetes), amputation of lower limb, training with initial prosthesis, number of prosthesis repairs, number of visits to a prosthetist for socket adjustment, frequency of prosthesis use, and intensity of prosthetic use. Terminal device DOF was not associated with either the TAPES-SAT or OPUS-CSD scores in the full sample (Supplemental Appendix Table A.4) or in the subsample of myoelectric device users.
Multivariate GLMs of outcome measures (Table 3) show that, after controlling for other covariates, there were no differences in summary satisfaction scores for body-powered versus myoelectric device users. TAPES-SAT scores were lower (worse) for those with SH and TH level amputation compared to those with TR. TAPES-SAT scores were higher for older respondents and those who received training with their initial prosthesis. OPUS-CSD scores were higher (worse) for those with SH level amputation compared to those with TR level amputation, and for those who identified as black compared to white, and lower (better) for older versus younger respondents.
Multivariate linear regression models predicting device satisfaction (N = 379).
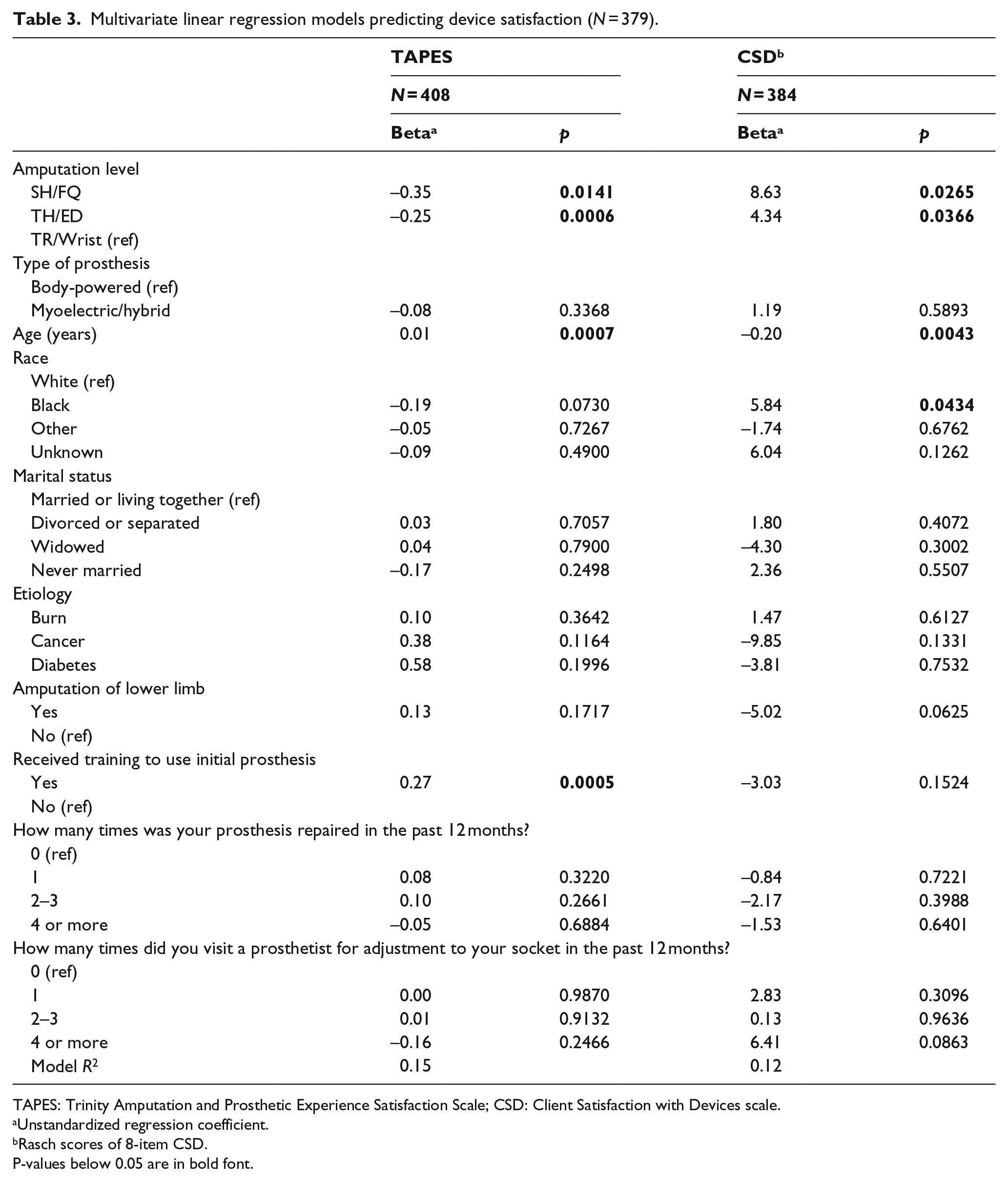
TAPES-SAT: Trinity Amputation and Prosthesis Experience Scales Satisfaction scale; OPUS-CSD: Orthotics and Prosthetics Users’ Survey - Client Satisfaction with Devices scale
Unstandardized regression coefficient.
Rasch scores of 8-item OPUS-CSD.
P-values below 0.05 are in bold font.
Discussion
We analyzed data from 449 unilateral upper limb prosthesis users to assess satisfaction by prosthesis type and identify factors associated with satisfaction. Our study used two primary measures of satisfaction, the TAPES-SAT and an adapted version of the OPUS-CSD. Results contribute new knowledge on prosthesis satisfaction as well as a new version of a prosthesis satisfaction measure for use with persons with upper limb amputation.
When controlling for multiple covariates in regression models, prosthesis type was not associated with device satisfaction as measured by TAPES-SAT or OPUS-CSD. Bivariate comparisons of individual satisfaction items across prosthesis types largely mirrored results of systematic reviews comparing body-powered and myoelectric devices.27,28 Body-powered users were more satisfied with reliability, durability, and lower weight, but not with wear and tear on clothes. Myoelectric users were less satisfied with weight and unintended movement. Cosmetic users were least satisfied with device color and noise, but reported lower levels of self-consciousness.
We had expected to see greater satisfaction for persons using multi-DOF terminal device, a newer technology that promises greater functionality and which is more anthropomorphic. Over 43% of the 93 myoelectric users reported using a multi-DOF terminal device, a prevalence that is likely higher in the VA than in the civilian sector, given the high costs for these devices and the limitations on prosthetic coverage outside of the VA. Bivariate analyses found no differences in device satisfaction for myoelectric device users of multi-DOF versus single-DOF terminal devices, and thus we did not add terminal device DOF to the multivariate models. Further research is needed on consumer satisfaction with multi-DOF terminal devices.
We found that receipt of training to use the initial prosthesis, amputation level, age, and race were independently associated with device satisfaction. Current device training was not added to the multivariate models because it was not associated with device satisfaction in bivariate analyses. These findings point to the importance of providing initial training and its role in promoting device use, consistent with earlier reports on the association between device abandonment and prosthesis training.13,14
Differences observed in prosthesis satisfaction by amputation level are consistent with the literature reporting greater dissatisfaction and abandonment in persons with proximal amputations.7,13,29 Persons with TR amputation had the lowest rate of rejection (6%), followed by TH (57%) and SD (60%). 2 These findings highlight the need for continued research to improve prosthetic options and care for persons with proximal amputations.
We also found that older persons were more satisfied with their prostheses, perhaps because, on average, they had been prosthesis users for the longest period of time and perhaps had come to value their devices. Finally, our models found that black respondents were less satisfied with their devices than were white respondents, a finding which needs further exploration to understand the root causes.
Limitations
The sample included Veterans who had received care at the VA between 2010 and 2015; nearly 62% was 65 years or older, with a minority under age 45 years, reflecting the age distribution of the US Veteran population. Thus, findings may not be generalizable to the larger Veteran population, to non-Veterans with upper limb amputations who have limited access to prosthetic care, or to younger persons with upper limb amputations. Although the study had a high response rate, there were few women and cosmetic devices users, limiting our ability to compare these prosthesis users. That said, this sample is one of the largest reporting device satisfaction and provides strong evidence about device satisfaction in older individuals with good access to prosthetic care.
The sample included current prosthesis users, so it is likely that persons who were most dissatisfied with prostheses were excluded. Thus, conclusions are limited to prostheses users only.
Although we used two measures of prosthesis satisfaction, we acknowledge that they address limited facets of prosthesis use. Both measures focus on device attributes and neither addresses satisfaction with prosthesis function. Only one item in the TAPES-SAT addresses usefulness which may be related to function, while no items in the 8-item OPUS-CSD address function. Studies that use other satisfaction measures or that compare satisfaction with device function are needed.
Conclusion
We evaluated satisfaction with upper limb prostheses using data from a national survey of Veterans. Users of body-powered, myoelectric, and cosmetic prostheses were equally satisfied with their devices. We did not observe meaningful differences in overall device satisfaction between users of multi-DOF terminal devices and users of single-DOF terminal devices. Lower device satisfaction was observed among individuals with more proximal amputations (TH and SH), younger age, and black race. Receipt of initial prosthetic training was associated with greater device satisfaction, pointing to the critical role of occupational or physical therapy in the early stages of prosthetic care.
Supplemental Material
10.1177_0309364619895201_Supplemental_material – Supplemental material for Prosthesis satisfaction in a national sample of Veterans with upper limb amputation
Supplemental material, 10.1177_0309364619895201_Supplemental_material for Prosthesis satisfaction in a national sample of Veterans with upper limb amputation by Linda Resnik, Matthew Borgia, Allen W Heinemann and Melissa A Clark in Prosthetics and Orthotics International
Footnotes
Author contributions
L.R. obtained funding, designed the study, led data analyses, and wrote the manuscript. M.B. assisted in study design, performed data analyses, and wrote portions of the manuscript. A.W.H. assisted in design of analyses of the OPUS-CSD data, participated in reviewing analytical results, and participated in manuscript writing. M.A.C. participated in study design, supervised data collection, and participated in data analyses and manuscript writing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the U.S Army Medical Research Acquisition Activity, W81XWH-16-2-0065 Department of Veterans Affairs, Rehabilitation Research and Development, A9264-S. Opinions, interpretations, conclusions and recommendations are those of the author and not necessarily endorsed by the Department of Defense or the Department of Veterans Affairs.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.