
Abstract
Background:
Research is needed to understand how upper limb prosthesis users take advantage of multiple grip options.
Objectives:
To quantify usage of DEKA hand grip patterns during home use and compare patterns of usage at home to test sessions.
Study design:
Observational study design.
Methods:
Data were collected from 21 subjects. Engineering data on grip were downloaded at various intervals. Proportion of time in each grip was calculated for the first 4 weeks of home use, later months, and test sessions (testing use) and compared statistically across intervals. Exploratory analyses compared grip proportion by DEKA Arm level and prior prosthesis use.
Results:
Three most commonly used grips during home use were power, pinch open, and lateral pinch. There were no significant differences between grip use during the first month and later months. Power grip was used 55% of the time at home and 23% of the time in testing use. Pinch closed, lateral, and chuck grip were used less at home than in tests. Comparisons were by configuration level and prosthetic use and no significant differences were found.
Conclusion:
Patterns of DEKA hand grip usage differed between home and test environments, suggesting that users relied on fewer grip patterns at home.
Clinical relevance
These findings have implications for prosthetic training with multi-articulating terminal devices.
Background
The human hand can make over 30 grasp patterns,1,2 yet until recently most prosthetic terminal devices allowed only one degree of freedom (DOF): simply opening and closing. Recently, terminal devices with multiple degrees of freedom (multi-DOF) have been introduced, allowing users to select from multiple grips. Despite increased availability, there has been little research comparing the functional benefits of single-DOF and multi-DOF devices and no studies examining prosthesis use in persons with multi-DOF devices. Several investigators have compared the overall functionality of specific devices,3–5 but have not examined how having a multi-DOF terminal device impacted the time a prosthesis was used or how often users selected from available grip patterns. Nor have prior studies evaluated prosthesis users’ selection of grips over an extended time periods.
Evaluation of prosthesis use at home has been predominantly conducted through surveys6–15 and to a lesser extent through direct observation and video analysis.16,17 Given the proliferation of multi-DOF terminal devices, research is needed to understand how users take advantage of multiple grip options. A new multi-DOF prosthesis, the DEKA Arm, 18 has been the subject of extensive study, and considerable data are available on its usage. Thus, the purposes of this study were to quantify usage of the six grip patterns of the DEKA hand during home use and to compare usage at home and during structured test activities.
Methods and materials
The DEKA arm
The DEKA Arm—available in three configuration levels, radial configuration (RC), humeral configuration (HC), and shoulder configuration (SC)—has six powered hand grips which provide options for precision as well as conformable “power” grips. 19 Three grips (fine pinch closed, lateral pinch, and tool grips) have a detent that allows users to separate the positioning/stabilizing and grasping aspects of grip from the precision portion (Figure 1). In these grips, users must activate two successive signals to open or close fully. The first activation closes (or opens) to the first detent and the second closes (or opens) the rest of the way.
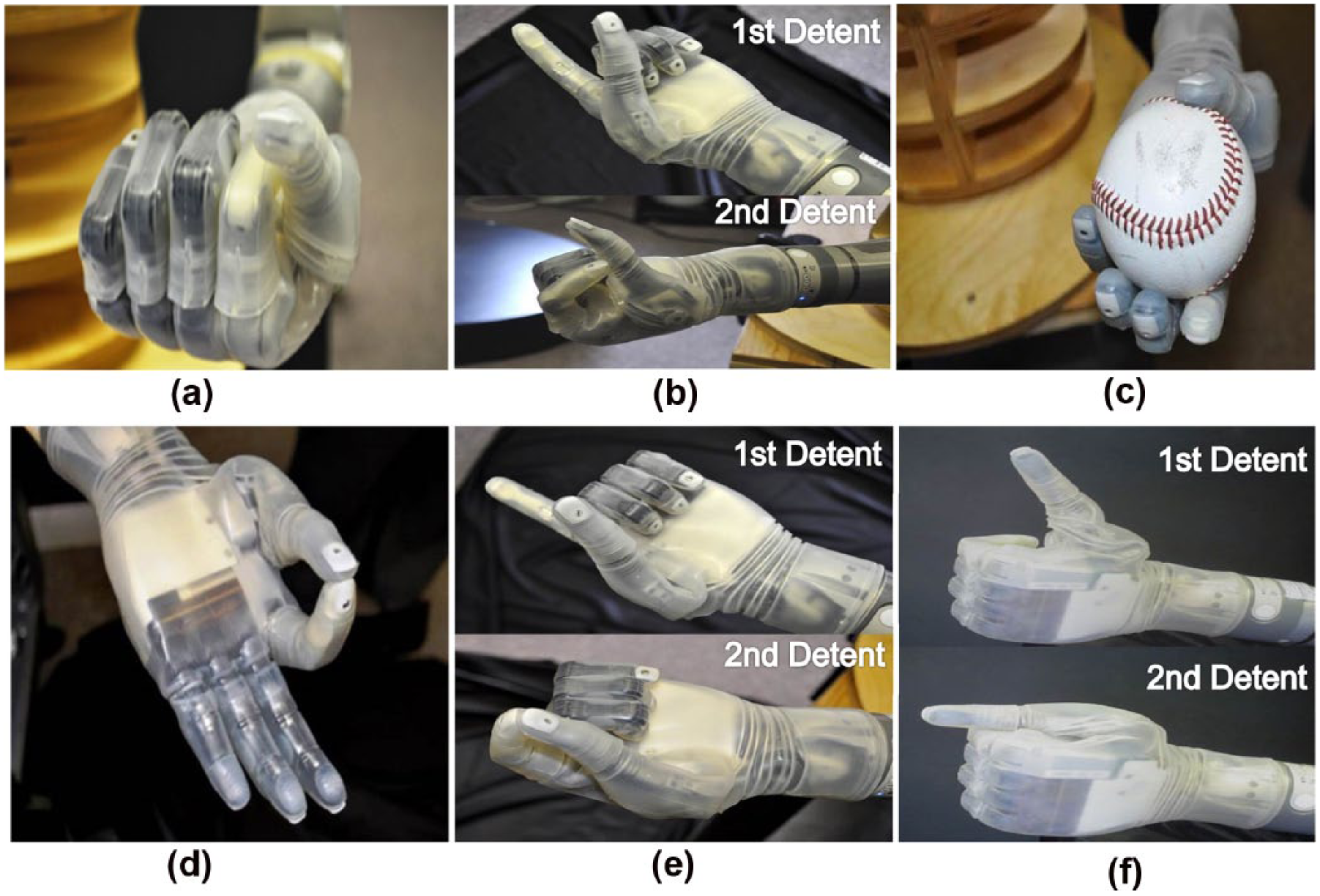
Six grips of the DEKA arm: (a) power, (b) tool, (c) chuck, (d) fine pinch open, (e) fine pinch close, and (f) lateral pinch. (b), (e), and (f) grips demonstrate hand closed to the first detent (first detent) and hand closed to the second detent (second detent).
In power grip, digits 3–5 flex while the distal thumb closes against the distal lateral index finger. In fine pinch open, the distal tip of the index finger opposes the distal thumb pad, while other fingers remain extended. Fine pinch closed uses the same pinch of index and thumb as fine pinch open, but digits 3–5 flex close instead of remaining extended. In fine pinch, the first detent command flexes digits 3–5, and the second flexes the index finger tip to close against the distal thumb pad. In chuck grip, the thumb opposes the pads of the distal index, while the middle, fourth, and fifth fingers flex. In lateral pinch, the radial aspect of the index finger flexes against the distal volar aspect of the thumb, while digits 3–5 also flex. The first detent command flexes digits 2–5, while the second flexes the thumb against the index finger. In tool grip, the index finger flexes to touch the proximal phalanx of the thumb, while fingers 3–5 flex. Because of the detent, the first closure will close digits 3–5, while the second command closes the index finger.
Users select the desired grip by toggling using their assigned “grip selection” controls. If the DEKA Arm is powered off and then on again or put into standby and then taken out, the hand defaults to whatever grip was previously selected.
Study design
Data were collected from subjects in the VA Home Study of an Advanced Upper Limb Prosthesis. The study was approved by the Institutional Review Boards at the Providence VA, NY VA, Tampa VA, and Center for the Intrepid. The study had two portions: in-laboratory (in–lab) and home study (Figure 2). All participants enrolled in the in-lab study, a subset continued to the home study which involved up to 3 months of home use. In-lab training included training on grip patterns and determining the most appropriate grip for specific tasks. Subjects practiced using grips during training which progressed from simple to complex activities. 20 During the home study, subjects were asked to wear the DEKA Arm for at least 2 h a day during their first 4 weeks. After that time, they used the DEKA Arm as much or as little as they chose. Subjects who participated in the home study returned to the study site every 4 weeks for test sessions.
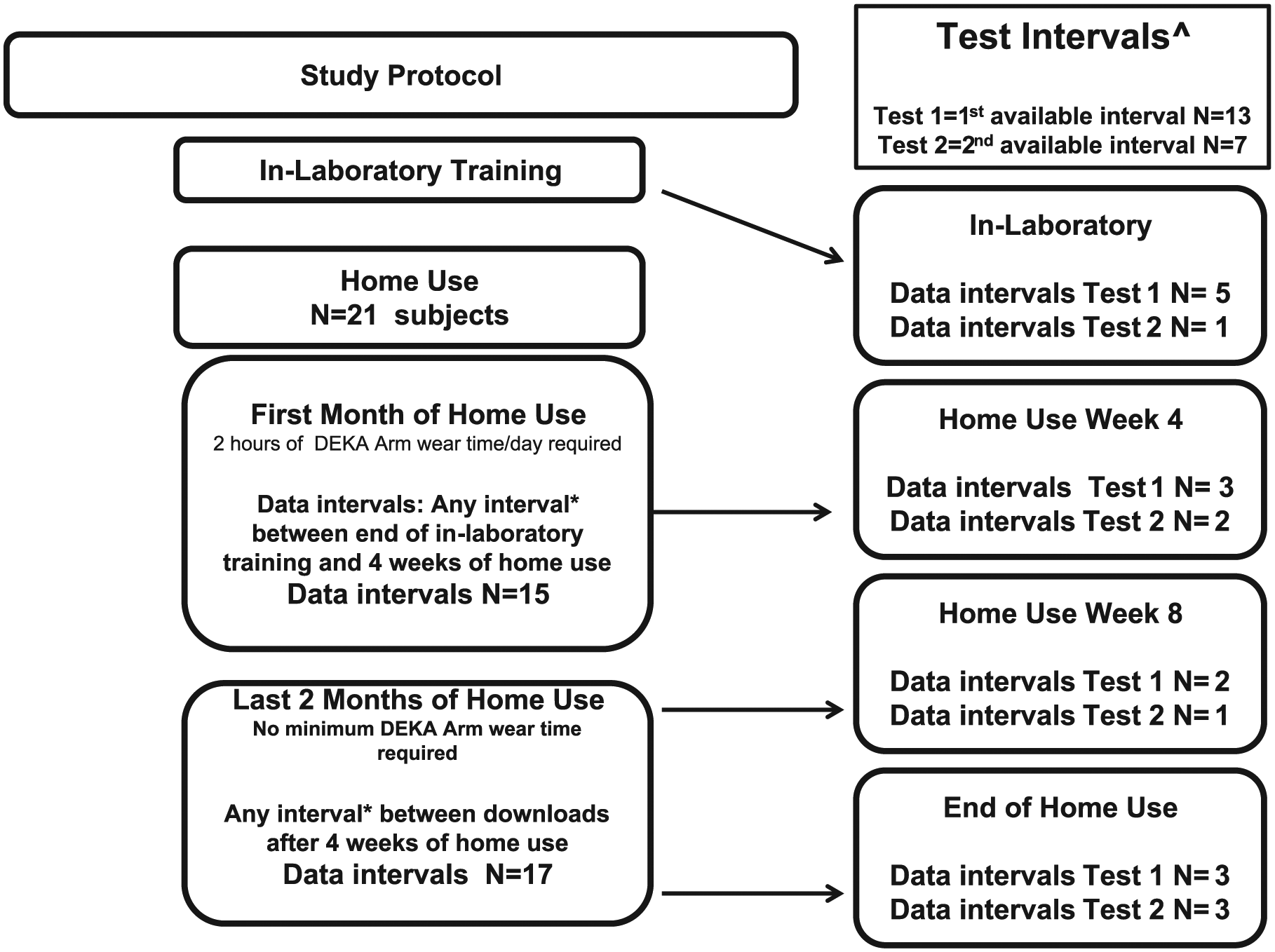
Flow Diagram showing study design, testing intervals, and data intervals analyzed.
Test sessions occurred midway through in-lab training, at the end of in-lab training (prior to home use), and at 4-week intervals. Test sessions consisted of a standardized protocol: the modified Jebsen-Taylor Hand Function Test; 21 a subtest of the University of New Brunswick Test of Prosthetic Function (UNB); 22 the Activities Measure for Upper Limb Amputation, the BAM-ULA, a brief measure of activity performance; 23 and the timed measure of activity performance (T-MAP). 24 Test sessions lasted about 2.5 h (Table 2) and were completed in 1 day, unless scheduling or unforeseen circumstances required 2 days.
Subjects
Subjects were eligible for the in-lab study if they were ≥18 years old and had an amputation at the transradial, transhumeral, shoulder disarticulation, or scapulothoracic level. Subjects were required to have control over one or both ankles or be able to control enough functions to operate the DEKA Arm using other controls (electromyography sensors (EMGs), pressure transducers, and linear transducers). Subjects were excluded if their amputation level or skin conditions prohibited socket fitting or they had serious health conditions.
Eligible subjects for the home portion demonstrated independent problem solving for common technical problems, had at least fair functional performance (judged by study occupational therapist and Principal Investigator based on performance during training), and demonstrated consistent safety awareness. Subjects included in this analysis were a subset who utilized the DEKA Arm system’s updated data logging capabilities.
Engineering data
Usage was collected using on-board software which tracks time the device is powered on, position of motors for each joint, and logs the time that motors are in the positions used for each grip. Using DEKA’s sequencing algorithm, the range of motion for each grip is segmented into individual logs (bins) denoting a change in joint positioning chronicled at different phases from the start to the end of the grip movement. Time of the device in each individual grip pattern is divided for eight bins, representing eight combinations of joint positions within each grip pattern (Appendix 1). The logs are cumulative, meaning that they include only total values from all days of use. The DEKA software allows the clinician to download and save these engineering logs. Logs can only be reset by DEKA during certain types of repairs.
Data collection procedures
The protocol called for study staff to download usage logs at the end of in-lab study (to obtain a baseline prior to home use), and monthly during home use and before and after test sessions. Data were also sometimes downloaded before and after test sessions that happened mid-way through in-laboratory training.
Missing data
Subjects included in this analysis are shown in Table 1. Data from every interval were not available for all. Sometimes data were lost if the device was replaced and logs not downloaded or logs from the replacement-device were not downloaded prior to device issuance. Data were occasionally lost during repairs if logs were not downloaded prior to the repair and cumulative logs were reset. A protocol change was made mid-way through the study requiring staff to download data logs prior to and after test sessions. Thus, earlier subjects did not have data from test intervals. Finally, there were occasions when staff did not download the data logs at the appropriate time, making it impossible to calculate the interval data.
Characteristics of participants over the course of the study for whom satisfactory logged data over at least a 2-week period at home use were available.
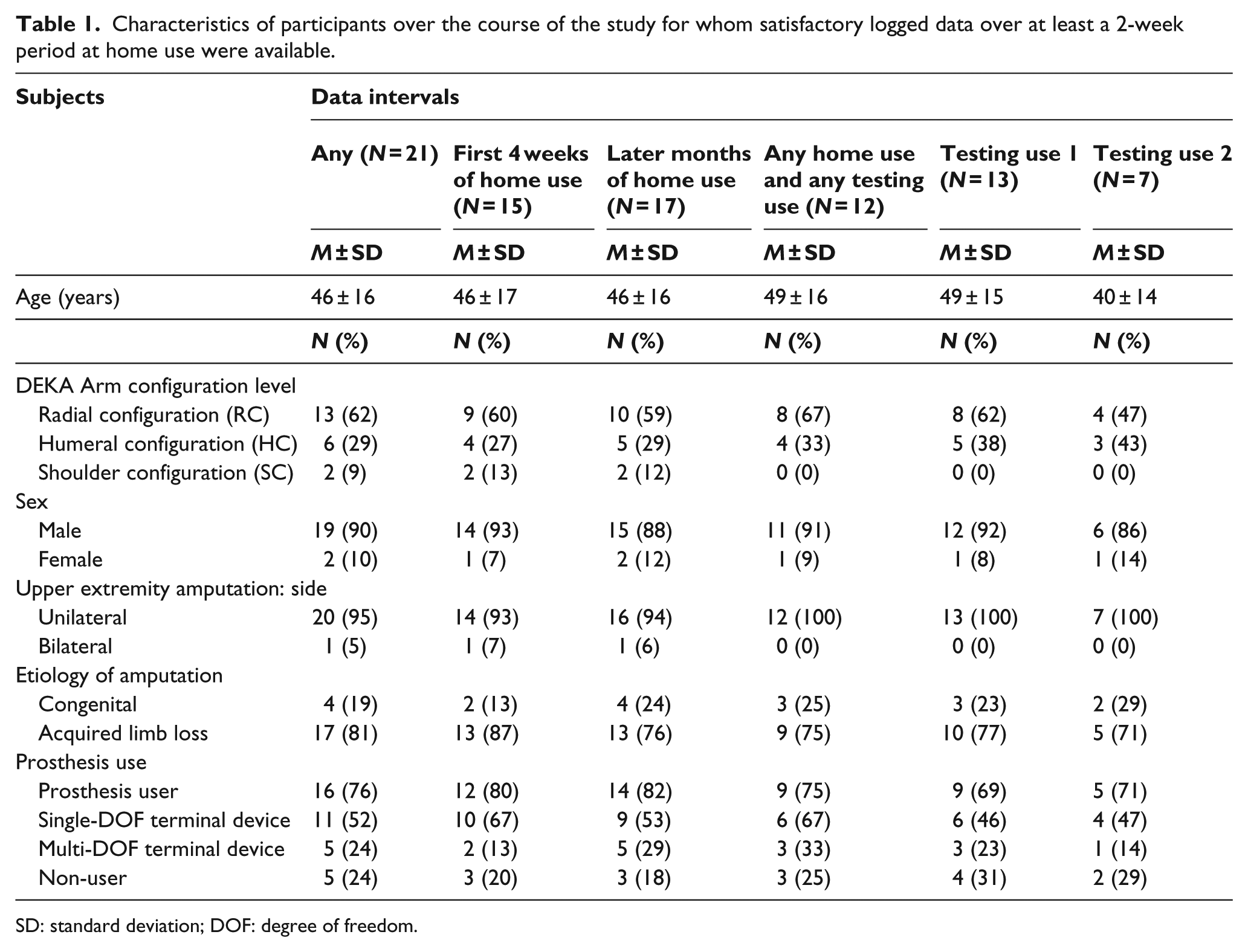
SD: standard deviation; DOF: degree of freedom.
Selection of data logs for analytical dataset
Data intervals for the home use period were created (Home Use) using consecutive logs separated by a minimum of 2 weeks. Intervals in which there had not been a reset or a new prosthesis issued were selected. Data intervals for the test session were created (Testing Use) when logs were available from before and after test sessions. The first available testing use interval for each subject was identified as Testing Use 1, and the second available test interval was identified as Testing Use 2.
Data analyses
Total hours the DEKA Arm was powered on were calculated for each interval and divided by number of interval days to estimate median hours of use per day during home use (use hours/day). Total minutes spent in each grip were calculated by adding time spent in each grip bin. Proportion of grip use was calculated by dividing total time spent in a specific grip by total amount of time any grip was used. Descriptive statistics were used to evaluate grip use for the first 4 weeks of home use, later weeks of home use, and testing use. Comparisons across intervals were made using nonparametric Wilcoxon signed-rank tests because of small sample size. The proportion of time spent in each grip was compared for the first 4 weeks of home use and later months. Additionally, the proportion of time spent in each grip during the first available Testing Use interval was compared to that spent during Home Use. To examine consistency of grip use during Testing Use, the proportion of grip use during Testing Use 1 and Testing Use 2 was also compared using Wilcoxon signed-rank tests.
Patterns of grip use were compared using Kruskal–Wallis tests by device configuration level, prosthesis use prior to Home Study enrollment (user or non-user), and DOF of the terminal device of the personal prosthesis: single-DOF (e.g. Greifer, motion control hand, electric terminal device (ETD), and work hook), multiple-DOF/function (e.g. I-Limb, BeBionic, Michelangelo, and Touch Bionics), or no DOF (non-prosthesis users). SAS version 9.1 was utilized for all statistical analyses, except Wilcoxon signed-rank tests which were performed in SPSS Statistics 20.
Results
Characteristics of 21 included subjects (2 SC, 6 HC, and 13 RC) are shown in Table 1: 16 were prosthesis users and 5 were not before enrollment. Data for the first 4 weeks of Home Use were available for 15 subjects; later Home Use weeks were available for 17, and Testing Use data were available for 13.
Median values for length of Home Use intervals, hours powered on, and average use hours/day are shown in Table 2. During the first 4 weeks of Home Use, median use hours/day was 1.2. During the later months, median use hours/day was 1.1.
Interval length, power on time, and proportion of time spent in each grip pattern.
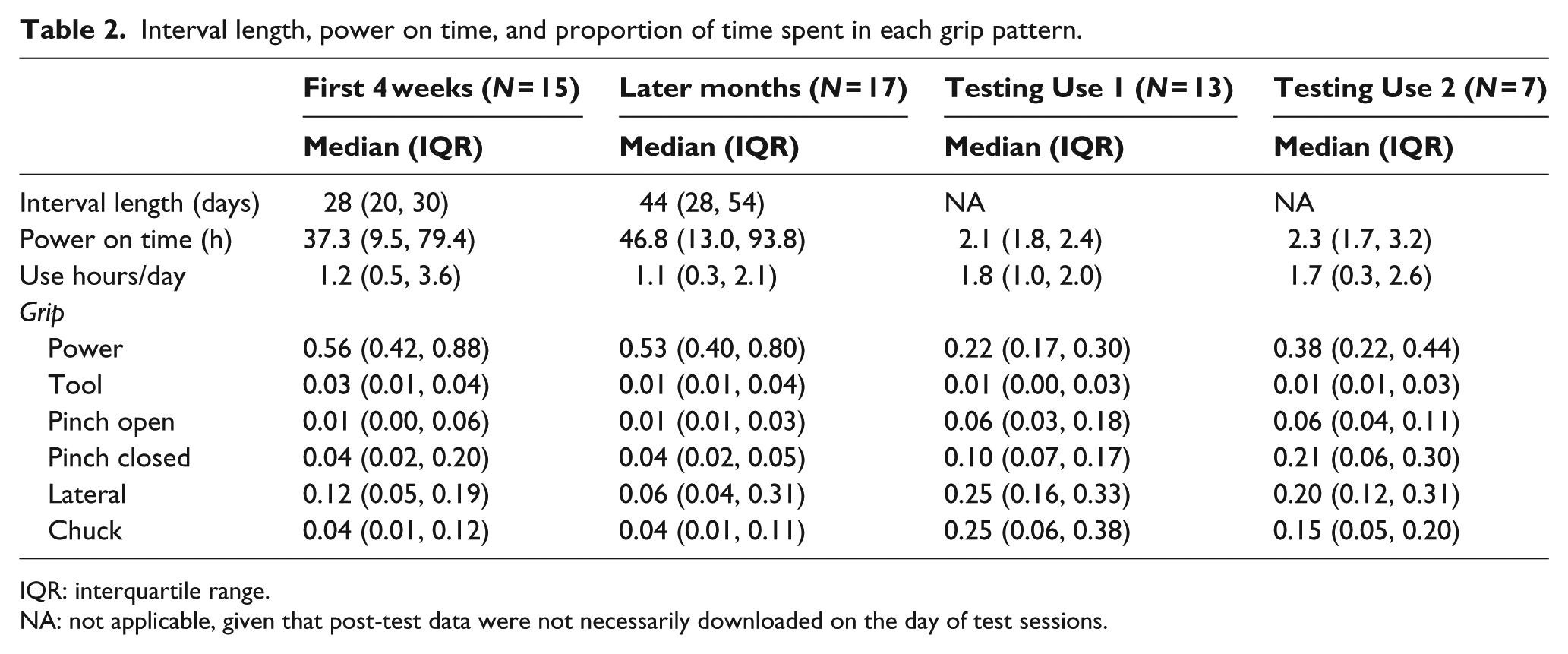
IQR: interquartile range.
NA: not applicable, given that post-test data were not necessarily downloaded on the day of test sessions.
The three most commonly used grips during Testing Use were power, pinch open, and lateral pinch (Table 2). There were no significant differences between proportions of time spent in each grip during home use in the first month as compared to later months (results not shown). There were no statistically significant differences in proportion of grips used in Testing Use 1 and Testing Use 2 (results not shown). However, Wilcoxon signed-rank tests revealed that proportions of grips used at home use were significantly different than during Testing Use for four grip patterns (p < 05; Table 3). A greater median proportion of grip time spent in the power grip was observed during Home Use (0.52) compared to Testing Use (0.21), and a smaller median proportion in pinch closed, lateral, and chuck grips at home (0.04, 0.14, and 0.06, respectively) compared to during Testing Use (0.11, 0.25, and 0.19, respectively).
Comparison of grip usage at home and during test (N = 12).
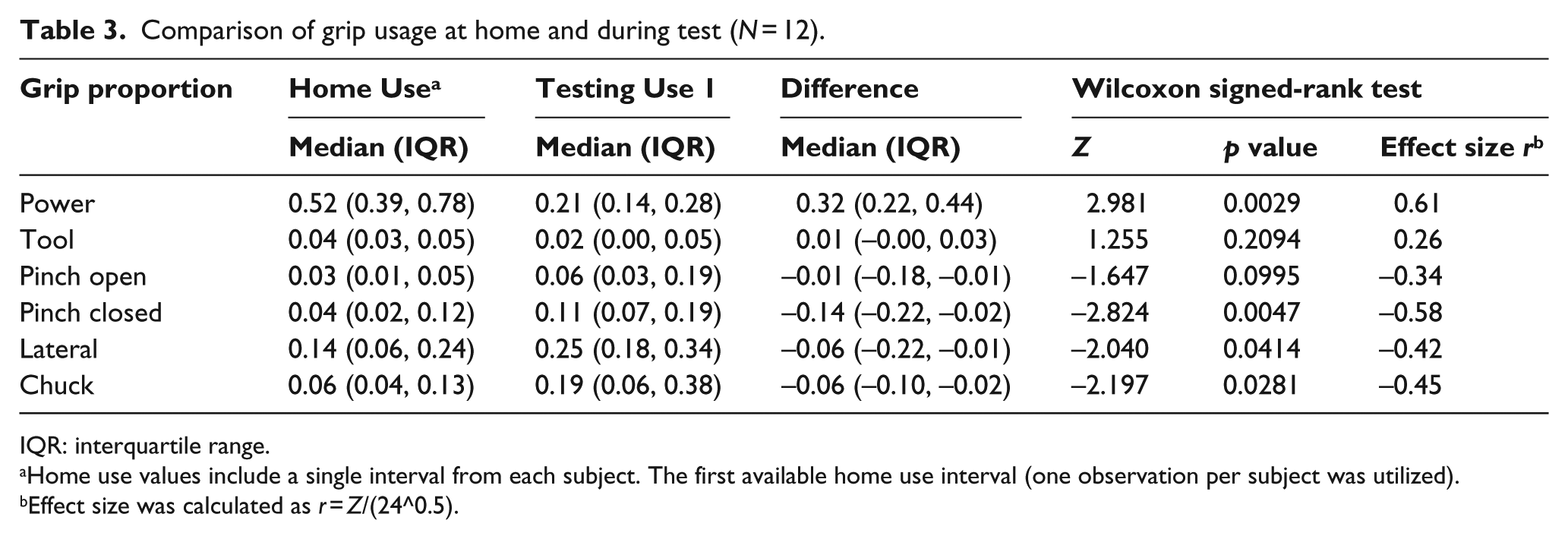
IQR: interquartile range.
Home use values include a single interval from each subject. The first available home use interval (one observation per subject was utilized).
Effect size was calculated as r = Z/(24^0.5).
Results of Kruskal–Wallis comparisons found no significant differences in proportions of grip use by configuration level (H(2) ≤ 2.39, p ≥ 0.30 for all six grips), prosthetic use (H(1) ≤ 1.87, p ≥ 0.19), and DOF of personal device (H(2) ≤ 2.06, p ≥ 0.36). Power grip was the most frequently utilized grip for all subgroups.
Discussion
We described the proportion of time users of the DEKA Arm employed each of six grip patterns and compared home use to use during standardized testing. During home use, power grip was used more than half the time and lateral pinch was the second most frequently used grip. Together, these grips were used more than 75% of the time. Other grips were used less often, with pinch grip (open and closed combined) used between 12% and 17% of the time during home use.
We observed substantial variation (i.e. large standard deviations) in proportion of grip time between subjects. This finding is consistent with literature describing variability in grasps in anatomically intact individuals performing housekeeping and machinists activities, 25 suggesting that variability in grip use is a matter of both personal and occupational/lifestyle demands. Based on these results, we recommend that future iterations of the DEKA Arm incorporate design modifications enabling the prosthetist to eliminate grips that users do not use regularly or do not want. This design enhancement could shorten the time it takes to select a desired grip.
We also found that the pattern of grip use differed at home and in testing. These differences suggest that while at home, participants did not utilize the DEKA hand the way that they did in the laboratory setting. These differences were not unexpected, given that others have commented that the prosthesis is seldom used in unilateral tasks outside of the clinical environment. 26 That said, our study training program emphasized use of the prosthesis as more than a “helper hand.” 27 At home, participants may have returned to pre-existing habits of using the prosthesis as a helper hand, seldom engaging it to perform skilled activities. This may be because prosthesis engagement in activities slows down activity performance,28,29 and use of the sound hand (for persons with unilateral amputation) is easier and more expedient. Prosthesis use, even with the DEKA tractor which provides crude grip force feedback, 18 lacks sensory feedback making users susceptible to dropping or crushing items, 30 and creating a reliance on vision to modulate force and object placement. 31 Furthermore, the purposeful selection of a grip pattern is cognitively demanding, and even when the prosthesis is engaged for grasping, it may be easier to remain in a single grip than to toggle to another grip, because the toggling process adds additional time to task performance.
Quantifying prosthesis use is challenging. Our method of quantifying use is more precise than methods involving self-reported surveys that ask subjects to reflect on average use over time6–13,15 and hence are subject to recall bias. 32 However, our method has some limitations. We calculated hours of use from engineering data but were unable to calculate hours of wear. Although prior studies report that 58–77% of prosthesis users used their device more than 8 hours a day,10–12 most do not distinguish between wear time and use time. One study, conducted in the 1980s, reported that myoelectric users wore their devices but did not turn them on 26–45% of the time. 7 Although this report is from an older, small study, if a similar patterns existed in our sample we would expect that subjects wore the DEKA Arm about 26–45% more hours than they actually used it. Furthermore, our estimation of use/day did not account for days that users did not use the DEKA Arm. Prior evidence suggests that prosthesis users do not use their device daily, with one study reporting a mean of 24.45 (approximately 80%) of days of wear per month. 9
Few studies have attempted to quantify prosthesis use or terminal device use without using self-reported data. One study of users of single-DOF body-powered devices utilized head mounted cameras and video analyses to develop a taxonomy of use, but did not report on hours of use. 33 More recently, investigators employed wearable sensor technologies to measure prosthesis movement.26,34 Chadwell et al. 34 utilized accelerometers to measure overall prosthetic limb use, to calculate the “bilateral magnitude” (magnitude of activity across both arms) and “magnitude ratios” (contribution of each arm to an activity). Their method quantified overall upper limb engagement but not whether the terminal device was used actively or passively. In contrast, Sobuh used accelerometry to classify type of terminal device activity, but not type of grip utilized.
Our use of on-board engineering data from the prosthesis has some advantages. It allows quantification of hours that the prosthesis is powered on as well as proportion of time spent in each grip. Downloadable data logging, if embedded into design of other types of multi-function terminal devices, would facilitate additional studies on grip in various environments.
While our study provides important new information, it also has several limitations. First, we studied grips of one multifunction terminal device. We cannot be certain whether there would be similar patterns for other devices. Further research is needed to expand this work. This study examined proportion of time spent in grips, but not whether grip was opened or closed fully or how detents were used. Therefore, we cannot draw conclusions about how grips were utilized. Although some intervals between data downloads were longer than others, our methodology of calculating proportion of total time spent in a grip eliminated differences attributable to length of the observation period.
Our study was limited because logs from every potential data interval were missing. We do not believe that missing data intervals biased results because missingness was unrelated to subject behavior. Although we saw no differences in grips used by participants with prior experience with a multi-DOF prosthetic hand and those without, and no differences by device configuration levels, findings should be interpreted as preliminary. Further research with larger samples is needed.
Another study limitation is that some test data were included in home use logs. At test visits, usage data were sometimes downloaded before and after the session and sometimes only after. Inclusion of this information would have biased comparisons towards the null. Therefore, the true magnitude of difference in proportion of grips used at home versus in test sessions was likely greater than what we observed.
Conclusion
This study quantified proportions of time that users of the DEKA Arm spent in each of six grasp patterns during periods of home use and during test sessions. The three most commonly used grips at home were power grip, pinch open, and lateral pinch. Grip use at home differed significantly from during test sessions suggesting that while at home users relied on fewer grips and were likely not engaging the prosthesis in the same manner they did during tests.
Footnotes
Appendix 1
Acknowledgements
The information in this manuscript does not necessarily reflect the position or policy of the government; no official endorsement should be inferred. The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of the US Government. The authors would like to acknowledge the contribution of Katherine Korps Foley, OTR/L, OTD who assisted with framing the introduction to the manuscript.
Author contribution
L.R. secured the funding, led the data collection efforts and directed the analyses, and took the lead on manuscript writing. F.A. was the project coordinator for the study, he coordinated data collection efforts, participated in selection of data intervals, and assisted with manuscript writing. M.B. was the biostatistician who cleaned the data, conducted the analyses, and assisted in interpretation and manuscript writing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding sources from Department of Veterans Affairs (Grant/Award Number: RR&D A9226-R).