
Abstract
Background:
In the existing literature, there is scarce information about subjects with upper limb amputation and driving.
Objectives:
The aim of this study was to find out how frequently subjects following upper limb amputation have problems when driving; most frequently proposed adaptations and, when possible, factors that influence driving ability.
Study design:
Retrospective clinical study.
Methods:
Medical records were reviewed of all subjects following upper limb amputation who had been amputated in the last 5 years and those with congenital upper limb deficiency who in the last 5 years turned 17.
Results:
Out of 37 subjects, 7 did not attend the clinic for assessment of driving abilities. They were significantly older at the time of the amputation (p < 0.001). To the remaining 30 who attended driving assessment, zero to four car adaptations (two on average) were proposed. There were no correlations between the number of suggested car adaptations and the age at the time of the amputation, amputation level, education and severity of phantom limb pain. Type of prosthesis also did not influence the number of car adaptations.
Conclusions:
Most people following upper limb amputation need at least one car adaptation for safe driving.
Clinical relevance
Most people following upper limb amputation need car adaptations for safe driving. Assessment of driving abilities has to be a part of comprehensive rehabilitation of these persons.
Background
Within the European Union (EU), around three million driving licence holders are disabled. 1 This figure represents nearly 1% of all EU drivers. As a part of the modern lifestyle, ability to drive enhances a person’s participation. It enables people to drive to work, to friends, to visit different places as tourists or for recreation, go to shopping malls, doctor’s offices and other places. For persons with disability, driving preserves their independence and improves their self-esteem. 2 Smurr et al. 3 recommended driver’s training as a part of advanced prosthetic training and rehabilitation. It has to include driver’s evaluation, identification of appropriate vehicle modification equipment and training with adaptive driving equipment. 3
Literature search based on terms ‘amputations and driving’ resulted in 32 articles, with 9 of them not being related to driving at all, 1 on finger injury in a car crash, 11 on driving abilities of persons following lower limb amputation, 3 generally on amputation and 3 generally on driving. We reviewed five articles on driving and upper limb amputation (Figure 1). One of them is a case presentation of a triple amputee 4 who acquired his driver’s licence after 2 weeks of driving practice; however, no further details were given. The article by Davidson et al. 5 is about management of multiple limb amputees. She made recommendations on resumption of independent driving and suggested using a steering ball (spinning knob) on the steering wheel.
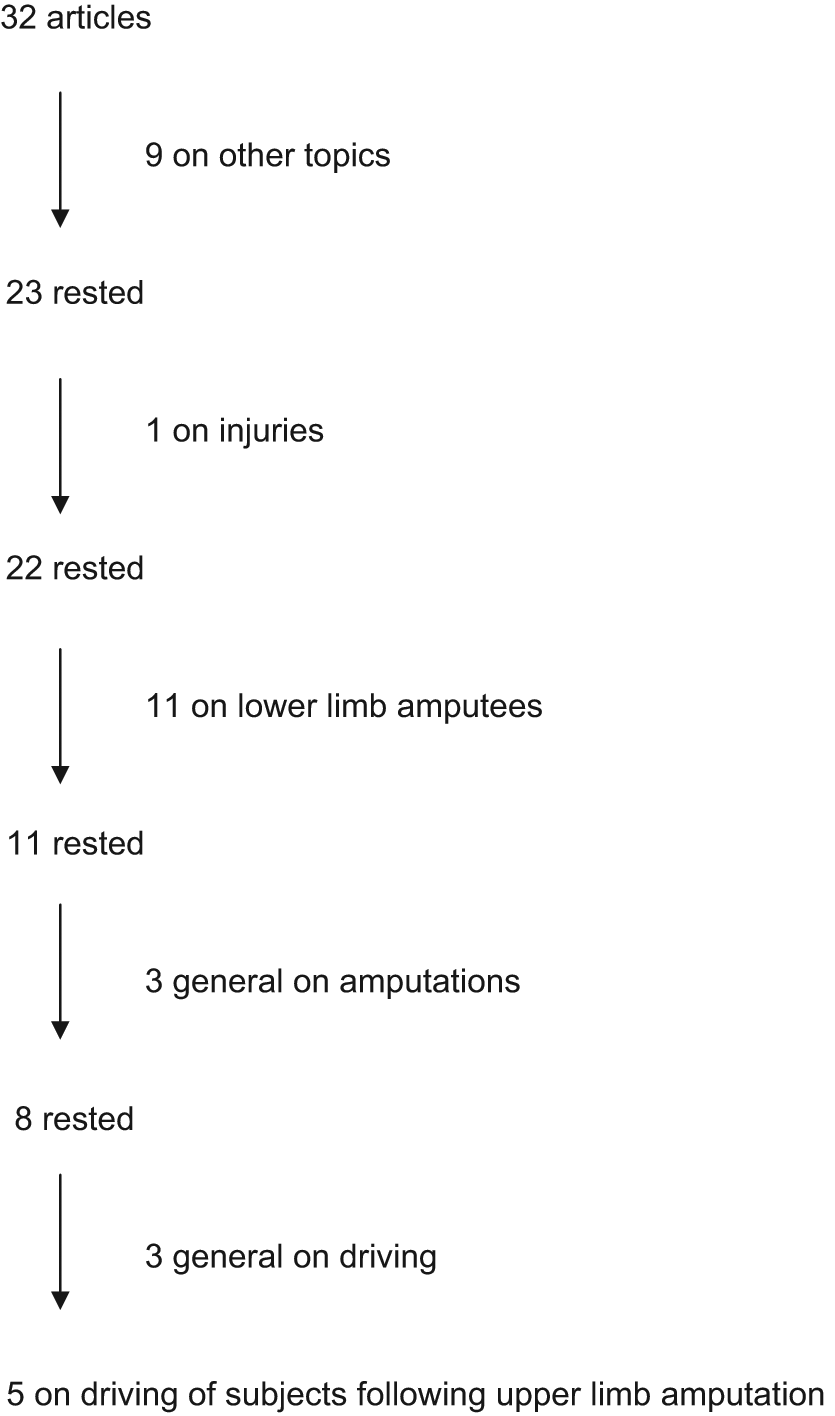
Results of literature search.
The existing literature gives no evidence on how many subjects following upper limb amputation have problems when driving. Fernández et al. 6 found that more subjects with upper limb amputation drive than those with lower limb amputation, but they need more vehicle adaptations. Adaptations are best described by Verrall and Kulkarni 7 on the basis of a questionnaire answered by 60 adults following upper limb amputation. They found that vehicle adaptations are rare. Automatic gear box, steering ball and changes to switch control were the most frequent. 7 The steering ball can be operated by hand, prosthetic hand or special terminal device for driving.5,7,8 Recommendations for car adaptations are best described by Hunter and De Vries 1 in the handbook developed by members of the European project PORTARE.
The access to mobility is the right of all European citizens. In the current driving licence directive (91/439/EC) as well as in the new one (2006/126/EC), which will be applicable from January 2013, it states that ‘specific provisions should be adopted to make it easier for physically disabled persons to drive vehicles’. In several countries, subjects and/or their medical doctors have to inform the agency responsible for driving licences of any physical change in a person’s condition that may influence their driving ability. Subjects have to be assessed in a special clinic for assessment of driving abilities of persons with disabilities. 7 During the assessment, the level and the side of the amputation and the possibility of functional prosthesis used for driving need to be considered. 1 The types of required technical solutions are described in European code form, embedded fully in already mentioned EC driving licence directives. For example, code for automatic transmission is 10.02, for electronically operated transmission is 10.03 and for transfer of control layout from left to right is 35.04.
In Slovenia, we strictly follow the above directive, and codes are printed on the disabled driver licences. This is still not yet accepted in all European Commission (EC) countries as part of their national driving legislation. In most countries, including Slovenia, medical assessment of disabled drivers is under control of Ministry of Health and free of charge. There are few European countries where (expensive) car adaptation is covered by social funds, what is at the moment not yet implanted in Slovenia, in spite of accepted legislation.
The aim of this study was to find out how frequently subjects following upper limb amputation have problems when driving; most frequently suggested adaptations and, when possible, factors that influence driving ability.
Methods
In the retrospective clinical study, we reviewed medical records of all subjects following upper limb amputation who had been amputated in the last 5 years in Slovenia and all subjects with congenital upper limb deficiency who turned 17 in the last 5 years. This study included subjects with partial hand amputation, while finger amputations only were excluded.
This study aimed at following three groups of data.
General (age, gender, education, work and other disabilities);
Amputation-related data (amputation level, side of amputation, dominance, cause of amputation, type of prosthesis and phantom limb pain);
Assessment of driving abilities and suggested adaptations.
Data were statistically analysed by SPSS software (version 15.0 for windows; SPSS Inc., Chicago, IL, USA, 2007). Descriptive statistics, t-test and correlations were used. This study was approved by the Ethics committee at the University Rehabilitation Institute.
Results
Thirty-seven subjects (27 men (73%)) 38 years old on average (standard deviation (SD) = 19.8 years, from 17 to 86 years) met the inclusion criteria. Of them, 1 (2.7%) had partial hand amputation, 5 (13.5%) had wrist disarticulation, 15 (40.5%) had trans-radial amputation, 14 (37.8%) had trans-humeral amputation and 2 (5.4%) had shoulder disarticulation. Nineteen (51.4%) had amputation of the left upper limb and 20 (54.1%) had amputation of the non-dominant hand. Seven (18.9%) had congenital upper limb deficiency; 24 (64.9%) were amputated due to injury (9 of them (37.5%) had work-related injury) and 2 (5.4%) of each due to tumour, disease and complication of chemotherapy. Six (16.2%) completed elementary schooling, 17 (45.9%) graduated from secondary school, 3 (8.1%) from high school and 4 (10.8%) from university, and for seven (18.9%) data were not available.
All except 2 (5.4%) used prosthesis, 7 (18.9%) used passive prosthesis, 23 (62.2%) used body-powered prosthesis and 5 (13.5) used myoelectric prosthesis. Nineteen (51.4%) had no phantom limb pain, other assessed pain with points 7.5 on visual analogue scale (VAS) on average (SD = 1.85, from 5 to 10).
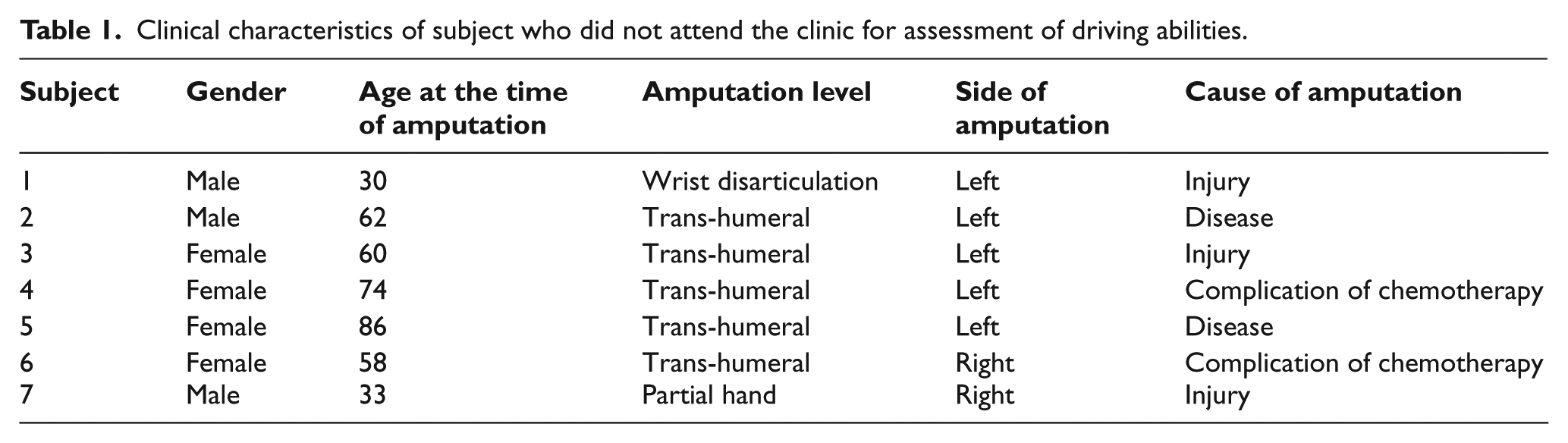
Seven (18.9%) did not attend the clinic for assessment of driving abilities of persons with different disabilities. Their clinical characteristics are presented in Table 1. They were significantly older at the time of the amputation (Figure 2, p < 0.001). The education level and phantom limb pain did not have any influence on this decision. The amputation level may have had an influence (Figure 3).
Clinical characteristics of subject who did not attend the clinic for assessment of driving abilities.
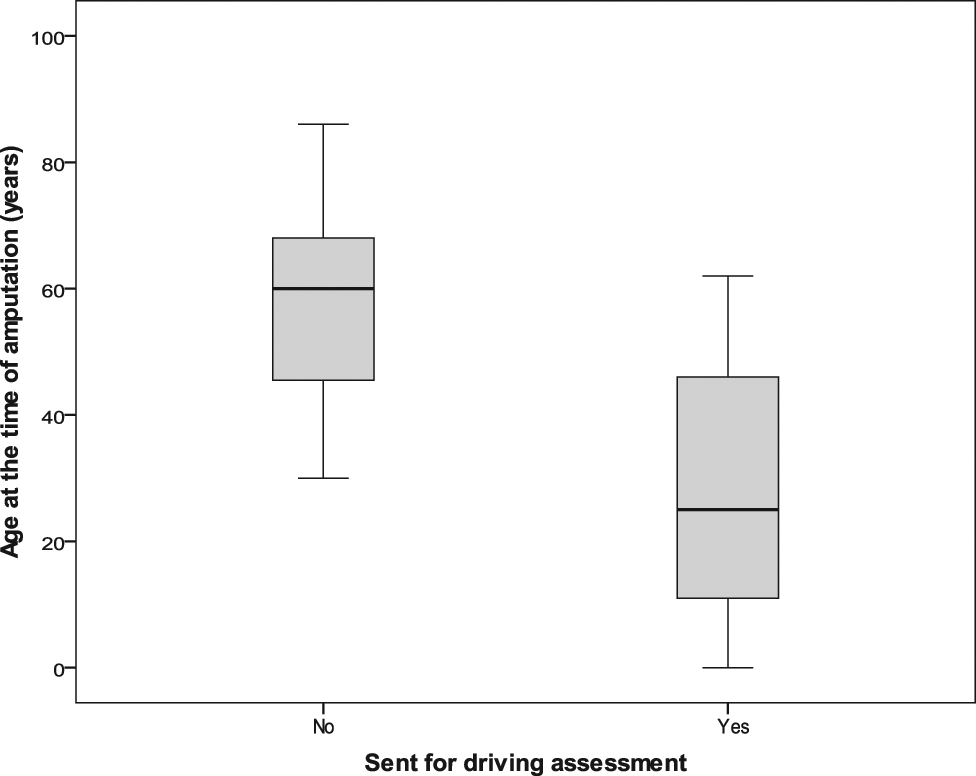
Influence of age at the time of amputation on those referred to driving assessment.
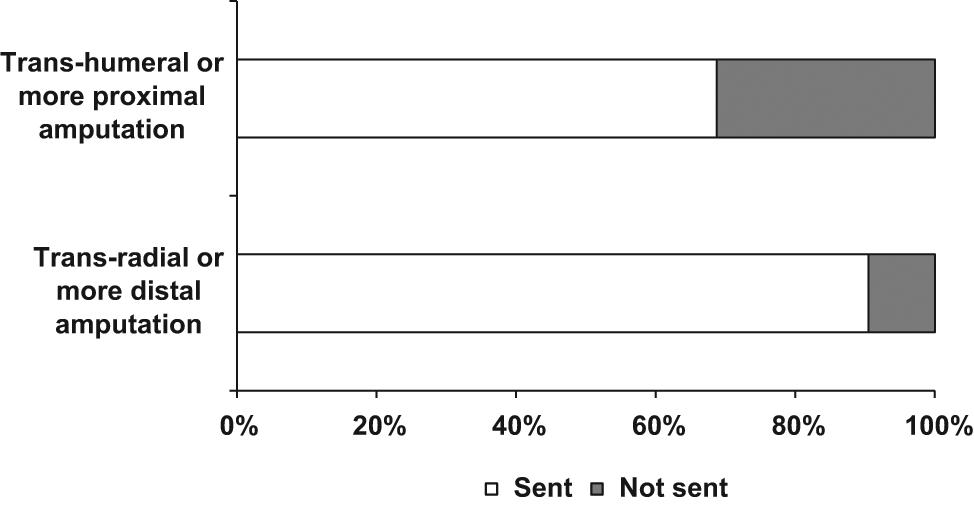
Influence of amputation level on subjects referred to clinic for assessment of driving abilities (p = 0.107).
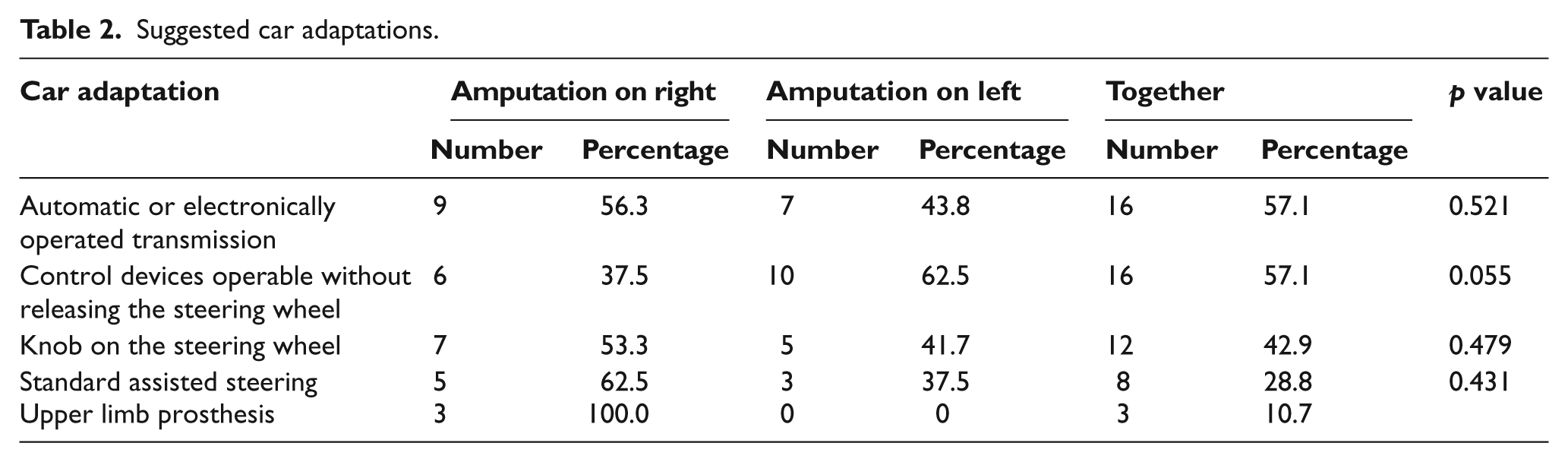
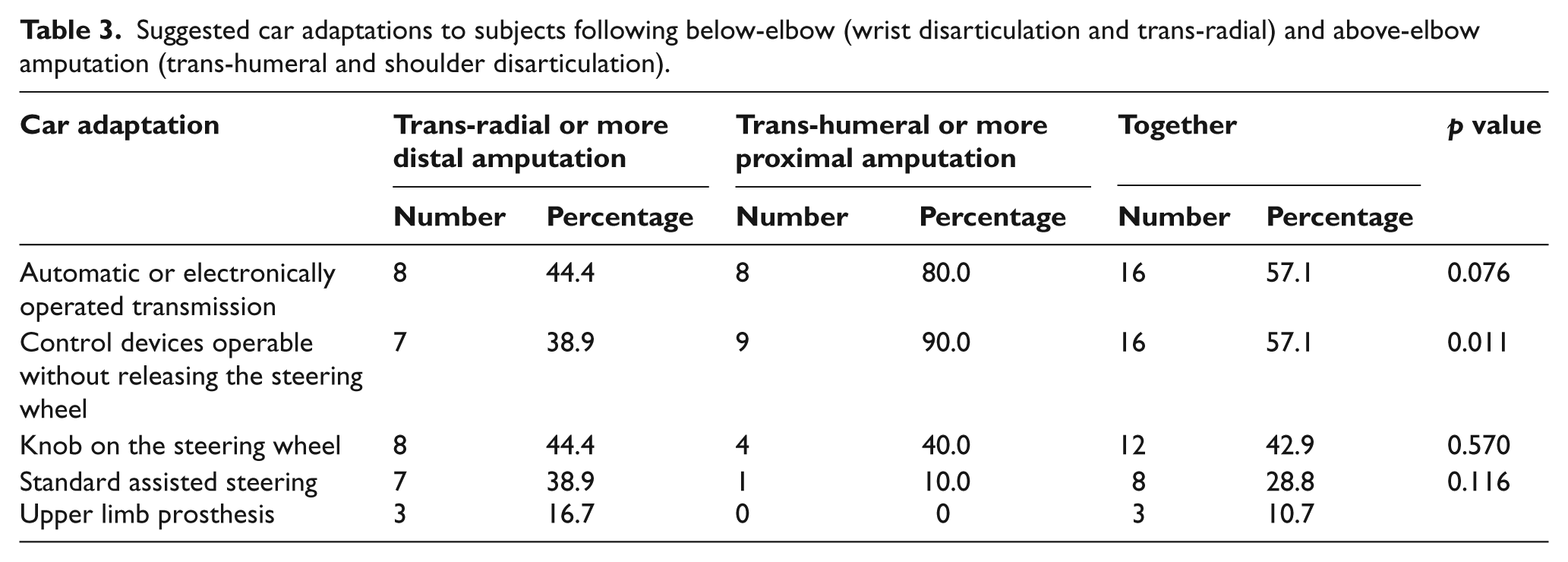
To the remaining 30 who attended the driving clinic, zero to four car adaptations (two on average) were suggested. To 1 subject (3.3%), no car adaptation was suggested; to 7 subjects (23.3%), one car adaptation was suggested; to 13 subjects (43.3%), two car adaptations were suggested; to 6 subjects (20%), three car adaptations were suggested and to 3 subjects (8.1%), four different car adaptations were suggested. The suggested adaptations and their frequency are presented in Table 2. A knob on the steering wheel was more frequently suggested to the left upper limb amputees (p = 0.055). Automatic or electronically operated transmission and a knob on the steering wheel were more frequently suggested to subjects following trans-humeral or more proximal amputation than to those following trans-radial or more distal amputation (Table 3). There were no correlations between the number of suggested car adaptations and age at the time of the amputation, amputation level, education and severity of phantom limb pain. Type of prosthesis also did not influence the number of car adaptations. The number of car adaptations and their frequency did not differ between persons with congenital upper limb deficiencies and those amputated due to other causes.
Suggested car adaptations.
Suggested car adaptations to subjects following below-elbow (wrist disarticulation and trans-radial) and above-elbow amputation (trans-humeral and shoulder disarticulation).
Discussion
We found out that most subjects following upper limb amputation attended assessment of their driving abilities, and almost all subjects following upper limb amputation needed, at least, one to four car adaptations. The most frequently suggested adaptations were automatic or electronically operated transmission, control devices operable without releasing the steering wheel and the most common was a knob on the steering wheel. The first two were at a higher percentage suggested to subjects following trans-humeral or higher amputation, similarly as suggested by Hunter and De Vries. 1
The subjects who did not attend driving assessment were on average older and had higher levels of amputations than those who had been referred to assessment. Two of them were elderly women not driving even before amputation, and there was one who did not want to drive any more. Most of these subjects were amputated due to tumour or complications of chemotherapy.
The frequency of suggested car adaptations in our study is similar to findings by Fernández et al. 6 who reported that almost 90% of subjects following upper limb amputation used car adaptations. The most frequent car adaptations are the same as found and recommended by Fernández et al., 6 Verrall and Kulkarni 7 and Davidson et al. 5 The only marginally significant differences in car adaptations were for control devices operable without releasing the steering wheel, which in this study were more frequently suggested to subjects following amputation on the left upper limb, similarly as suggested by Hunter and De Vries. 1 For right-side driving and changing gears, stump or prosthesis is not safe enough for steering. Automatic transmission solves most of the problems.
In the scarce literature about driving following upper limb amputation, findings about the influence of the level of amputation are inconclusive. Verrall and Kulkarni 7 found that subjects following trans-humeral amputation more frequently use automatic transmission than those following trans-radial amputation. However, Fernández et al. 6 did not find that the level of amputation had an influence on driving. The results of this study are more similar to those of Verrall and Kulkarni. 7 In our sample, those following trans-humeral or more proximal amputation less frequently attended driving assessment. To others, automatic or electronically operated transmission and control devices operable without releasing the steering wheel were normally suggested.
Surprisingly, only three subjects, all following amputation on the right upper limb (two wrist disarticulation and one trans-radial amputation), were suggested to use their prosthesis for driving. All three had body-powered prosthesis. According to Hunter and De Vries, 1 such prosthesis can be used for gear changing and occasionally for steering the wheel (e.g. for hill starts when releasing the handbrake). Fernández et al. 6 found that 66.6% drivers were prosthetic users, but it was not clear whether they used their prosthesis for driving and for which activities. Datta et al. 8 found out that 25% of subjects found their prosthesis beneficial for driving. Similar is also our experience from the outpatient clinic, where several subjects who had been amputated before we started the clinic for assessing driving abilities told us that they used their prosthesis for driving, especially for changing gears, and that some prosthetic hands were better shaped for doing it than other. It seems that there is still no conclusion on how safe it is to use an upper limb prosthesis for driving.
The main limitation of this study is a small number of included subjects, but due to some organisational changes, there may have been a bias if others were included. In last few years, we have been strictly following the EU regulations, and all new patients are sent for driving assessment, whereas before, the patients had the possibility to decide whether to go for assessment or not. However, this study included all subjects who were amputated in the last 5 years and those with congenital deficiencies who reached driving age. Since our institute is the only setting in Slovenia for rehabilitation of persons following upper limb amputation and children with congenital upper limb deficiencies, we have included all newly amputated subjects from the entire country.
Conclusion
Most people following upper limb amputation need at least one car adaptation for safe driving. Assessment of driving abilities has to be part of a comprehensive rehabilitation of these persons. Inability to drive may result in participation restrictions, also among the elderly. In the future, more effort has to be put into discussing driving with persons following a recent higher level upper limb amputation. More studies are needed to determine how safe different prostheses are for driving.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.