
Abstract
Background:
The evaluation of ankle–foot orthoses is primarily focused on biomechanical performance, with comparatively less studies pertaining to users’ quality of life and experiential factors.
Objectives:
To investigate how child users regard acquisition and use of ankle–foot orthoses through the perspectives of child users, parents/carers and practitioners.
Study design:
Inductive content analysis of secondary data.
Methods:
Child user and parent/carer perspectives, as communicated by them and by practitioners, were collected from online platforms and formal publications. Data and themes were analysed through an inductive approach. Investigator triangulation was used to increase trustworthiness and reduce bias.
Results:
We found and analysed 223 data points from 30 informal online platforms and 15 formal publications. These data clustered into five key themes relating to user experience with ankle–foot orthoses, including materials, structure, aesthetics, service and impact. Child users had mixed opinions about ankle–foot orthoses, reporting satisfaction with the functional improvements resulting from ankle–foot orthosis wear, while noting negative feelings from the experience of acquiring and using the device.
Conclusion:
This research suggests that considering the five themes in ankle–foot orthosis provision could improve the child user experience, inform future ankle–foot orthosis design, and improve clinical outcomes.
Keywords
Background
Ankle–foot orthoses (AFOs) are braces designed to compensate for weakness in the foot and ankle, correct deformities and improve walking ability. These devices offer non-surgical management strategies for patients with walking difficulties that emerge from conditions such as cerebral palsy, 1 inherited neuropathy, 2 and brain and spinal cord injuries. 3 Using AFOs can improve mobility, maintain surgical correction, and prevent the recurrence of deformities.4,5 While AFOs represent a comparatively affordable and common rehabilitation treatment for many musculoskeletal and neuromuscular conditions, the evidence surrounding AFO acceptance among child users is mixed. Some studies suggest that children readily accept AFOs as they assist them to stand, walk and run.6,7 However, other studies observe resistance towards AFOs and a reduction in use resulting from physical irritation, discomfort and poor fit.8–10 Reduced wear is undesirable, as poor adherence can lead to patients’ tripping and falling, or not receiving other treatment benefits.
Much of the literature concerning orthoses surrounds the biomechanical performance of AFOs,7,11,12 with literature concerning experiential considerations seemingly nascent. Little is known about how the paediatric user’s experience with an AFO can be optimised. Qualitative methods have shown promise in gathering paediatric perspectives relating to the use of medical devices.13–15 While qualitative studies may inform AFO research, studies on the experiential aspects of AFO devices for child users are lacking. Such experiential studies could significantly aid in optimising the child user experience, enhancing satisfaction and well-being.
The aim of this study was to explore, through qualitative content analysis, how children regard the acquisition (i.e. the process of prescription, consultation and fitting) and use of an AFO from the perspectives of child users, their parents/carers and practitioners.
Methodology
The study followed a qualitative content analysis methodology in order to describe, code and make inferences about AFO child user issues and experiences. A qualitative approach offers an established method for replicating and validating inferences from data and clustering abstract concepts. 16 Content analysis allowed for the understanding and inclusion of complex, dynamic and multi-dimensional themes that might otherwise be excluded in quantitative research.17,18
We organically derived the overarching themes from the information space using an inductive approach. An inductive approach proved useful as the data set was largely fragmented19,20 – that is, the literature concentrated primarily on biomechanical aspects of AFOs, and secondary data (relating to the experiential aspects of the device) lacked formal analysis. An inductive approach allowed themes to emerge from the data as opposed to being formed pre-emptively by the researchers involved in coding.21,22 We used investigator triangulation to increase study credibility and address potential bias. 23 D.L. (a male higher degree research candidate (PhD) with a background in Industrial Design) and C.H.E.T. (a female User Interface[UI]/User Experience [UX] designer with a Bachelor of Design Computing [Hons]) independently researched and analysed formal and informal sources to identify emergent themes. Neither D.L. or C.H.E.T. had familiarity with orthotics prior to the study, nor any affiliation with data sources or contributors. The researchers were supervised by E.N. and C.W. (experts in qualitative research and conducting content analysis in medical contexts), and J.B. and T.L.C. who provided subject matter expertise (clinical expertise in personalised assistive devices for children and expertise in development of medical devices for children, respectively). Themes were then confirmed among all six authors.
Data sources included formal sources (e.g. journal articles, conference proceedings and panel transcripts) and informal sources (e.g. online web platforms such as parenting forums, community bulletin boards, manufacturer support networks and personal blog sites) of information. Theoretical sampling 21 determined data selection, with the following criteria required for inclusion:
Subject matter: only data pertaining to AFOs (not orthoses in general) were included.
Age: data were required to convey a child user’s AFO experience (either authored by an AFO user within the age range, specifically mentioning a child AFO user in third person as a parent/carer or associated health professional, or otherwise referencing experiences pertaining to an AFO user within the defined age range), wherein a child is defined as a person under 18 years of age. Authors inferred the general age range of the AFO user through the data or through other data posted by the same online user.
Timeliness: to reduce data describing legacy devices and designs, only information published in the last 10 years was included.
Detail: sources required sufficient detail to derive relevant data. This meant sources had to detail (at the least): the approximate age of the AFO user, the relationship with the AFO user (if not the AFO user themselves) and the subject/opinion/perspective being shared. Formal and informal sources needed to be free of bias or conflicting interests over the data presented (such as overt advertising or promotion of a product).
Authorship: informal sources were included if the author could be identified as the primary or secondary source (e.g. the AFO user, carer or practitioner). This was done to mitigate hearsay and ensure that the data were authentic to users’ needs.
The keywords ‘AFO’, ‘ankle-foot orthosis’, ‘orthoses’, ‘orthosis’, ‘orthotic’, ‘child’, ‘kid’, ‘experience’, ‘issue’, ‘benefit’, ‘improve’, ‘pain’ and ‘problem’ were used to search for data. The MeSH terms (‘Qualitative’, ‘Method’, ‘Ankle Foot Orthoses’, ‘Qualitative Research’, ‘Lower Extremity’, ‘Adolescent’ and ‘User-driven’) were also included in the search. As research progressed, other keywords relevant to emergent themes were used to expand the scope of data and explore the emerging themes: these terms included ‘hot’, ‘cold’, ‘sweat’, ‘blisters’, ‘pressure sore’, ‘footwear’ and ‘shoe’.
The researchers utilised Miro (San Francisco, CA, USA) visualisation software to organise the collected data points into an abstraction diagram so that data could be coded and reorganised, as required. D.L. and C.H.E.T. individually analysed the same set of consolidated data. Collected quotes and representative excerpts from the sources were placed into the diagram and clustered thematically, and clustering informed new search terms of interest for each researcher to investigate.
D.L. and C.H.E.T. researched the various sources with the listed search terms and then gathered quotes and excerpts into a data set for analysis. Duplicates of sources or data points that both authors found were merged at this stage.
Analysis of the data and themes occurred over three stages using guidelines proposed in similar studies.22,24 During stage 1, both D.L. and C.H.E.T. individually read over the consolidated data set to identify any obvious patterns or overarching themes among the data points. Stage 2 involved each author individually refining the data set into smaller, more specific themed clusters. Stage 3 involved D.L. and C.H.E.T. comparing and merging the analyses. Themes and data clusters were then reviewed by the research team for validation. This review ensured that the themes identified were contextually relevant, distinguishable and not overlapping. Data collection and analysis occurred iteratively over three rounds of collection and analysis, and stopped when saturation was reached 25 – that is, when no new themes were emerging from the data and when only existing themes appeared in new sources.26–28
Themes emerging from each author’s analysis were mostly congruent, with minor debates relating to the titles of themes and subthemes. The literature was consulted to resolve these discussions, ensuring that appropriate titles were ascribed.
The data were categorised across two dimensions as follows: (1) experiential aspects of service and impact (i.e. data relating to child-patient experiences) and (2) device-related dimensions of aesthetics, materials and structure (i.e. data pertaining to perspectives on the appearance, design and construction of AFOs). These dimensions are illustrated in Figure 1.
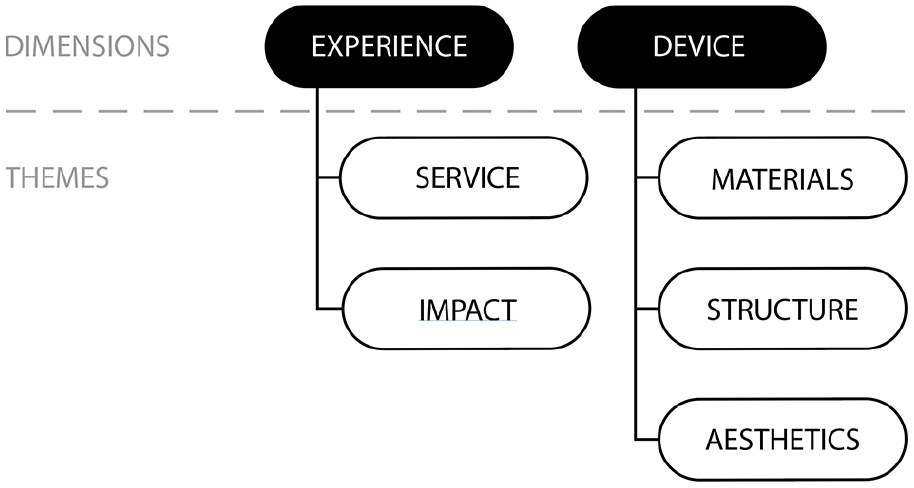
Dimensions and themes emerging from analysis of child user perspectives on AFOs.
Results
Data from 30 informal online platforms and 15 formal publications5–7,10–12,24,29–36 were selected for analysis, with 223 individual data points extracted from these sources. Most individual data sources contributed to multiple data points – that is, individual messages, anecdotes, quotes or comments found in the data. The sources and data are described in Table 1.
Description of the data and sources.
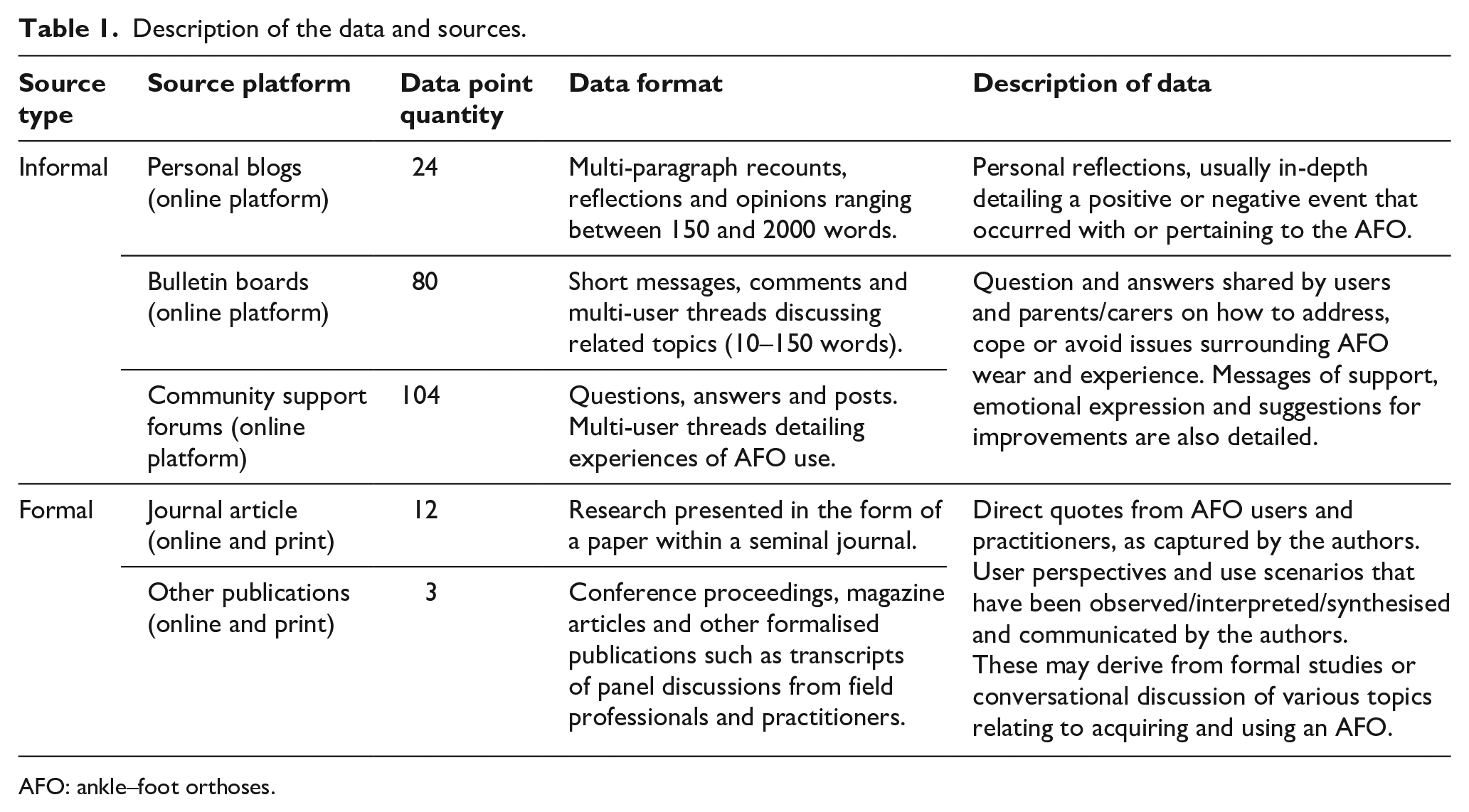
AFO: ankle–foot orthoses.
Data analysis revealed five first-order themes and 14 second-order themes. Theme descriptions and example quotes are detailed in Table 2. The examples of informal sources in Table 2 are a representative sample of the larger data set and were modified to preserve source anonymity (and therefore do not appear in quotations). Each of the themes is further detailed in the following sections.
Child user perspectives on AFOs.
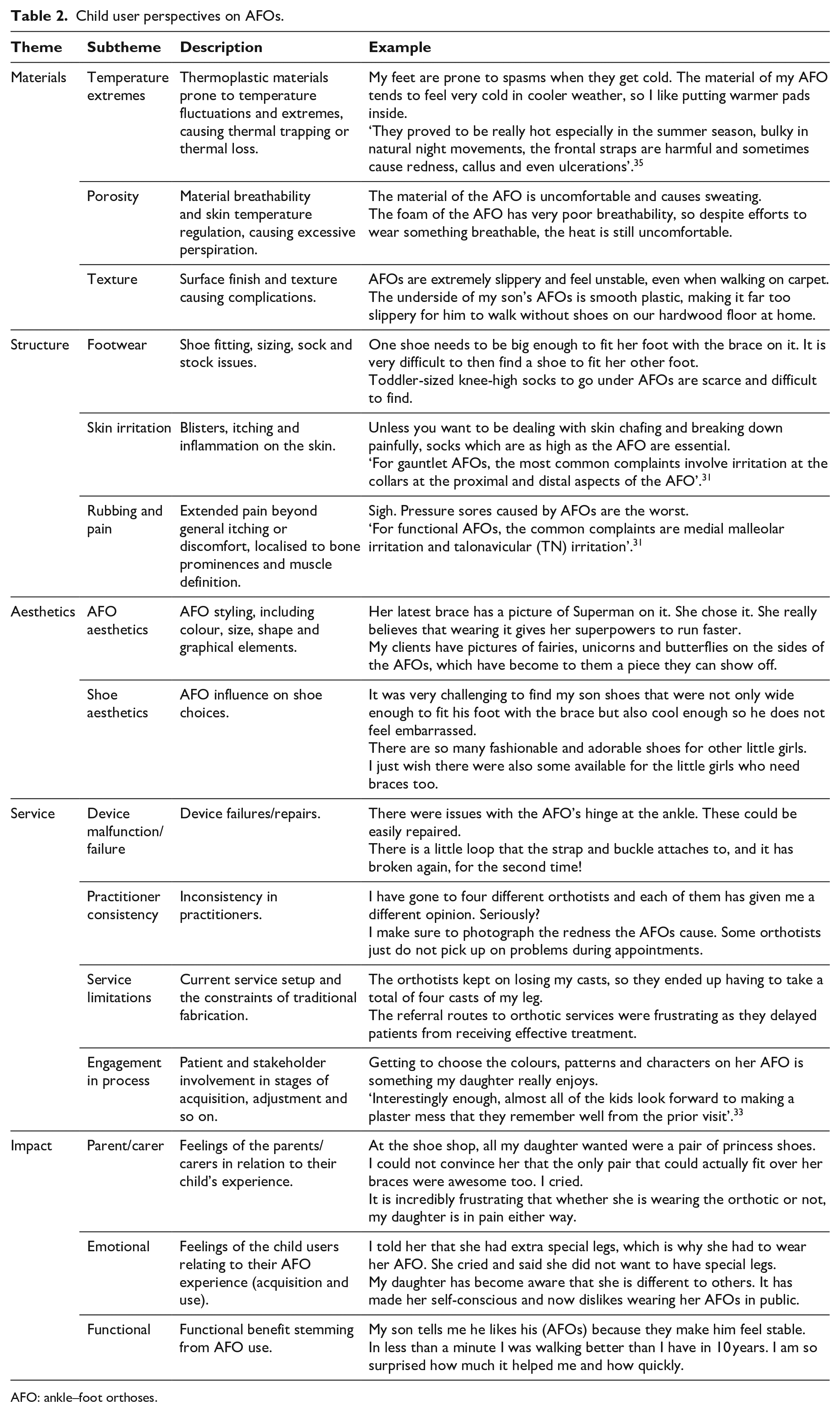
AFO: ankle–foot orthoses.
Materials
This theme details implications of AFO material choice (i.e., texture, porosity and temperature). The analysis indicated that some users are dissatisfied with materials that lack breathability and stable thermoregulation properties. Issues such as thermal trapping, excessive perspiration and pain from the cold correlate with mention of temperature extremes, such as summer/winter seasons and hot/cold days.
AFOs must be worn with shoes for optimal biomechanical performance. Subsequently, users express frustration about where/when their AFO can be worn given the low friction (i.e. poor grip) on the AFO sole. In such instances, users must decide to either wear AFOs with their shoes or otherwise forego AFOs in environments where shoes would not ordinarily be worn (e.g. at home or at the beach).
Structure
The theme of structure pertains to the physical design of the AFO (i.e. flexibility, mobility and the physical interaction between the AFO and its user). AFO child users suggest that rigidity surrounding the medial/lateral malleoli can cause pressure sores and superficial skin irritation, as well as difficulty with mobility. Some users mentioned terms such as ‘clunky’, ‘bulky’ and ‘lack of mobility’. Users also expressed that an AFO’s structure limited choice in footwear due to the difficulty of finding an appropriate size/fit, availability of stock, and discomfort from shoes and socks.
Aesthetics
The theme of aesthetics includes the outward appearance, styling and colour of the orthosis. A small number of (typically younger) users expressed a desire to highlight the aesthetics of AFOs and joy in AFO customisation (via colour, graphic design, buckles, texture, etc.). However, most users (typically older) expressed a preference for the design to be as ‘discreet as possible’, recounting efforts to conceal their AFOs, correlating to research linking an increase in self-perception and appearance. 37 Footwear aesthetics also represent a notable theme in the data set, with reports of parents/carers having difficulties buying desirable shoes for the wearer, particularly so for unilateral AFO wearers.
Service
The theme of service pertains to the processes, protocols and systems surrounding AFOs, including device malfunction, orthotist reliability, service limitations, and practitioner–patient communication and engagement. The data indicate overall dissatisfaction in the process of being prescribed an AFO, with child users experiencing disappointment and frustration. Some sources report lengthy delays when acquiring the AFO, attributed to reasons such as practitioner error in measurement, fabrication errors from the manufacturer and/or unreliable delivery times. Other sources indicate inconsistencies in fit between AFOs (e.g. when an AFO is replaced due to breakage or a child’s growth). These inconsistencies were attributed to different orthotist skills, or clinical practitioner approaches and opinions. Sources also indicated instances of confusion or disappointment with the repair and adjustment process, citing repeat malfunctions, total failure of the device or lengthy repair times as contributing to being reluctant to engage in device maintenance. Not all data indicated negative experiences, with some parents/carers and practitioners 33 indicating that children (typically pre-teen) enjoyed the traditional, tactile plaster processes during the initial casting.
Impact
The theme of impact describes the emotional and functional outcomes of AFO use by children. AFOs were perceived to offer significant functional benefits (such as improved physical movement or increased walking abilities) which translated to positive emotional gains. However, the data revealed emotional suffering and dissatisfaction of parents/carers with words such as ‘hopeless’, ‘frustrating’, ‘helplessness’ and ‘cried’ used when recounting their child’s AFO experiences. Negative emotions of ‘looking different’ and ‘embarrassment’ were also described in the data. These emotions were often associated with feelings of self-consciousness and concern surrounding others’ perceptions of the child user.
Discussion
The data imply that the designs of AFOs may prioritise function over experience. While the discontent of child users is readily expressed through informal channels, formal literature appears to focus on the biomechanical performance of AFOs. This is to be expected, given that the field of prosthetics and orthotics has focused predominantly on functional improvement thus far. Indeed, research surrounding the patient experience with AFOs is relatively nascent, particularly in contrast to other professions.
Nevertheless, user preferences are increasingly being accommodated in the design of children’s assistive devices, specifically through the introduction of frameworks that incorporate child users’ needs during medical device development.38–41 The FEA2 framework, in particular, highlights the necessity to incorporate function, expressiveness, aesthetics and accessibility in rehabilitative device design. 40
Design of a prosthetic or orthotic device often impacts child user acceptance. The importance of incorporating sociocultural and aesthetic inputs into the design of prosthetic legs for children in the developing world was found to outweigh a technological or economic focus. 42 Child user input has also been sought in the design of a prosthetic knee, enabling prioritisation of functional aspects of the device. 43 For adolescent users of scoliosis braces, the visual aesthetics of the device and engagement in the design process were able to improve adherence and acceptance. 14 An AFO design that incorporates child user feedback has been proposed, 44 however the impact of changes to design on adherence has yet to be explored.
Each of these studies highlights the importance of improving the holistic experience of acquiring and using a wearable assistive device. Irrespective of device type, this study found that users have experiential needs that span beyond their devices’ biomechanical performance. Experiential needs, if unmet, form obstacles that can significantly impede adherence and reduce treatment efficacy. Leveraging patient perspectives presents an opportunity to directly address these often-unmet needs.
In Table 2 we listed the key issues emerging from the data. These key issues and representative quotes embody user needs and requirements, and were presented as points of consideration to inform future research and novel child-specific AFO concepts. Addressing these issues may help improve some of the overlooked experiential deficits spanning the service, impact, materials, aesthetics and structural aspects of AFOs.
The United States Food and Drug Administration is increasingly recognising the importance of patient reported outcomes in clinical outcome assessments. 45 Instruments, such as the Orthotics and Prosthetics Users’ Survey (OPUS), were developed to evaluate the quality and effectiveness of orthotic and prosthetic practitioners’ services and have greatly improved the scope of assessable outcomes, 46 but specific details regarding the AFO experience may not be captured by these surveys. This article identifies thematic focal points for consideration in the design of AFOs and highlights experiential factors that could be assessed in future clinical studies to improve child-patient outcomes. Expanding this study to include larger data sets (via additional languages, communication platforms, etc.) could potentially uncover other or more diverse child-patient perspectives. Given the nature of secondary data, there are also opportunities to supplement the findings through primary research (e.g. focus groups and in-depth interviews) seeking deeper and more definitive insights. Such research would aid in providing more accurate and specific recommendations for various AFO models for child users. Application of this research to novel AFO design for children may yield improvements in adherence, treatment effectiveness and child user satisfaction.
Methodological considerations and study limitations
While blogs, online forums and other similar platforms have the benefit of being mediums through which a range of individuals can freely express opinions without response, bias is common in informal secondary research. Key limitations include the inability to fully verify the author, credibility and reliability of such sources. However, the researchers used language cues and examined other content authored by the same entity (e.g. though their account/profile) to reduce ambiguous data being included in the data set and to increase confidence in the subject matter and author background.
As comments are generally posted by a parent/carer rather than the child user of the AFO, they are subject to the posters’ interpretation. Likewise, the authors acknowledge that child or parent/carer perspectives, as conveyed by practitioners in this data set, may differ or not accurately represent the original intent of the patient, nor share the same perspectives of what is considered a successful treatment based on the desired outcomes. 47
The nature of the sample body means that the data are subject to misinterpretation based solely on the researchers’ understanding of the limited text – in contrast to an interview where verbal or non-verbal cues can be observed. Among the secondary data, there remains a degree of ambiguity regarding the type(s) of AFO referred to in the sources due to its colloquial nature. As such, the considerations highlighted in this article are broader and do not refer to specific AFO models or designs, nor can the findings be directly extrapolated to all AFO users (especially those in other age groups). Finally, it is important to note that when reviewing services, people are more likely to leave an extreme opinion (either positive or negative) and less likely to report a neutral/average opinion.48,49 These factors should be considered when reviewing and drawing conclusions from this research.
Conclusion
This study employed a qualitative content analysis to investigate the acquisition and use of AFOs by children. Five factors were found to contribute to child user satisfaction with the device: materials, structure, aesthetics, service and impact. While the functional improvements of AFOs were appreciated by child users, a number of these factors (largely pertaining to the aesthetics, service and impact) were found to have a negative impact. The thematic focal points that emerged from this research have the potential to affect AFO design and child user satisfaction with AFOs. It is possible that addressing these five areas of the AFO experience may increase adherence of child AFO users and result in better clinical outcomes.
Footnotes
Author Contributions
All authors contributed equally in the preparation of this manuscript.
Ethics Review and Approval
The research was approved by The University of Sydney Ethics Committee (application no. 2019/119).
Declaration of Conflicting Interests
The author(s) disclosed no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The team acknowledges funding from Sydney Musculoskeletal, Bone and Joint Health Alliance. J.B.’s research and clinical activities are funded by the Australian Department of Health (Medical Research Future Fund), the US National Institutes of Health, Charcot-Marie-Tooth Association of Australia, Charcot-Marie-Tooth Association (USA), Diabetes Australia, Elizabeth Lottie May Rosenthal Bone Bequest, Perpetual Limited and Humpty Dumpty Foundation.