
Abstract
This paper reviews and summarizes the evidence for important observations of normal and pathological gait and presents an approach to rehabilitation and orthotic management, which is based on the significance of shank and thigh kinematics for standing and gait. It discusses normal gait biomechanics, challenging some traditional beliefs, the interrelationship between segment kinematics, joint kinematics and kinetics and their relationship to orthotic design, alignment and tuning. It proposes a description of four rather than three rockers in gait; a simple categorization of pathological gait based on shank kinematics abnormality; an algorithm for the designing, aligning and tuning of AFO-Footwear Combinations; and an algorithm for determining the sagittal angle of the ankle in an AFO. It reports the results of research on Shank to Vertical Angle alignment of tuned AFO-Footwear Combinations and on the use of ‘point loading’ rocker soles.
Keywords
Introduction
Since 1997, the Child Development Centre, Bangor, UK, has routinely used the ORLAU Video Vector Gait Laboratory to analyze children's gait and optimize AFO-Footwear Combination (AFOFC) prescriptions. This has allowed the development of a coherent model for understanding normal and pathological gait and the designing, aligning and tuning of AFOFCs.
Normal gait
Understanding biomechanics of normal gait is a prerequisite for successful orthotic management. Normal and pathological gaits of adults and children have been described in depth. 1–5 ” While early work described both segment and joint kinematics 2 most modern clinical and research gait analysis has focused on joint kinematics. However giving equal weight to the kinematics of both the jonts and the segments has wide importance.
Measurement of joint and segment kinematics
During the gait cycle (GC), movements of the joints of the lower limb are measured as a continuous series of angles between two segments relative to each other. 1,3 When measuring segments during the GC, their movement needs to be measured in relation to some position in space. 2,5–7 Measurement relative to the vertical can be most helpful as when standing or walking we have to achieve alignment of the segments relative to the force of gravity, which is acting vertically. The angle of the segment relative to the vertical can be measured and described in degrees of incline or recline from the vertical 8 (Figures 1). The term Shank Angle to Floor has been used to describe this angle. 8,9 A more accurate term would be Shank to Vertical Angle 10 (SVA). The same terminology would apply to segment kinematics of the thigh and other segments.
Segment and joint kinematics, traditional beliefs versus reality
Objective measurement of segment kinematics challenges some traditional beliefs. Our beliefs have pervaded clinical practice and may be one reason why some methods of intervention are often unsuccessful. Such beliefs may originate from lack of objective data prior to the availability of slow motion film and other gait analysis systems. The lack of ability to observe gait accurately may have led us to translate the observed kinematics that we could see when a subject stands still into beliefs about walking kinematics. However, evidence suggests the following:
(a) During stance, as seen from the right side, the thigh, shank and foot segments move in a clockwise direction but not with a uniform angular velocity. 2,3,5–7,11–16 During stance the shank and thigh segments move from a reclined to an inclined position, passing through vertical. The angular velocity of the shank slows during its movement into forward inclination in midstance (MST). While the shank is slowing, the thigh angular velocity increases. The foot becomes stationary in a horizontal position, during MST.

Measurement of segments relative to the vertical.
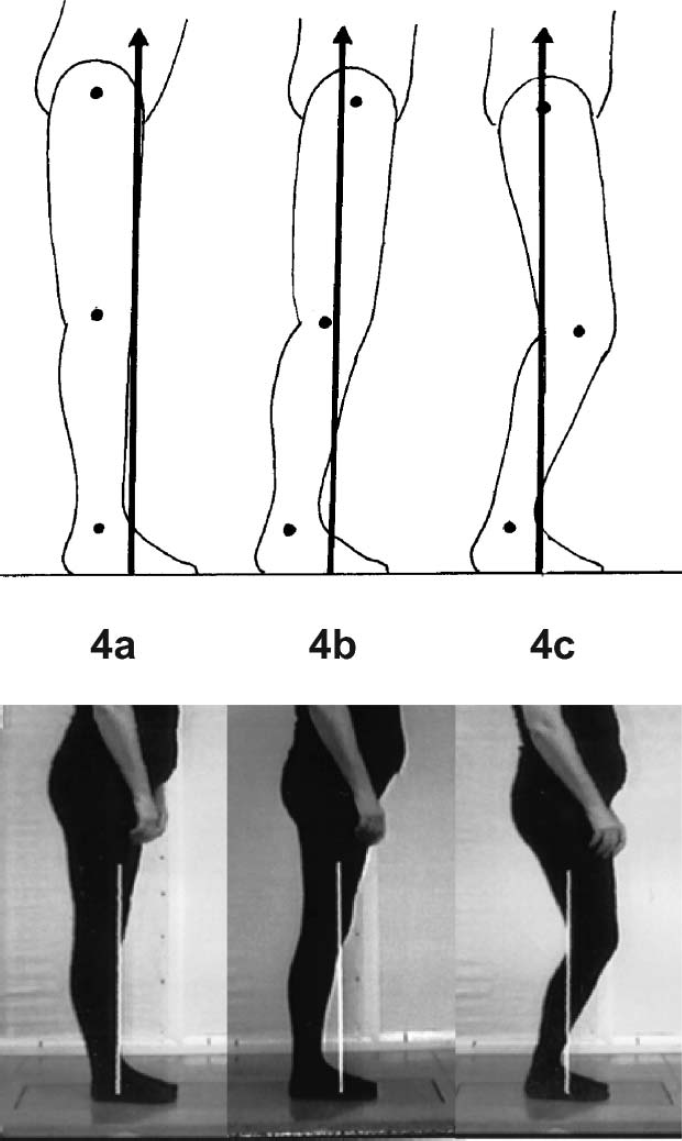
(b) The shank is not vertical at midstance and there is no place in the gait cycle when both the shank and thigh are vertical. 2,3,5–7,13–16 A common belief is that the shank is vertical at midstance (MST). This is often combined with a belief that the thigh is also vertical at this time, and that this is the place in the GC when maximum knee extension occurs. 17 Actually, there is no place in the GC when both the shank and thigh are vertical (Figures 2). It is, however, possible to demonstrate this scenario in standing. If we wish to demonstrate standing with fully extended knees we often brace the shank segment to a vertical position and place the thigh vertically above the shank. This produces extended knees but, as the hip and knee joint centres are now directly over the ankle joint, to maintain balance in standing with ease we have to excessively anteriorly tilt the pelvis, flex the hips and forward lean the trunk. This keeps the ground reaction force (GRF) in the middle of foot and base of support 8 (Figures 3b, Figures 4a). Those of us with normal balance ability and strength are able to obtain, with effort, a vertical trunk over the vertical thigh and shank but the GRF at the foot has to move to the extreme posterior of the base of support. Those with pathology are predominantly unable to access this option and will have to either adopt the forward trunk lean posture or recline the thigh whilst also forward leaning the trunk, imposing hip and knee flexion 8 (Figures 3a). Normal gait requires an approximately vertical trunk.
Another way to demonstrate standing with fully extended knees is achieved by inclining the shanks to about 10–12° incline and then moving the pelvis forward so the thighs are also inclined. The knees will become fully extended and the hips also extend. The pelvis will remain in normal alignment and the trunk can remain vertical 8 (Figures 3f, Figures 4b and Figures 5c). Knee extension is combined with inclined shank and thigh in normal gait.
(c) The slowing of the shank, in an inclined position of 10–12° incline, during midstance is important to gait. Midstance is a difficult phase of the GC. The limb is in single stance and many changes in both kinematics and kinetics occur. The kinematics of the shank in regard to both its position of incline and its slowed angular velocity during MST is important for a number of reasons 8 (Figures 6).
(1) It contributes to stability in stance (Figures 6). A 10–12° inclined position of the shank places the knee joint centre over the centre of the foot, which is horizontal and still at this time. 8 This creates a stable distal support mechanism in the form of a triangle. The concurrent slowing of the shank angular velocity increases this distal stability. 8 Stability in stance is one of the five attributes of normal walking 1 and is vital in MST.

Normal gait. Images taken from Video Vector Generator

Shank kinematics dictate proximal segment kinematics and GRF alignment. 8
(2) It facilitates ballistic movement of the thigh, pelvis and trunk. Soleus is restraining the forward movement of the shank and, with the shank now relatively stationary, momentum carries the thigh, pelvis and trunk forward to extend the knee. 16,18 Perry aptly described this movement as ‘trunk glide’. The angular velocity of the thigh increases at the time that the angular velocity of the shank decreases. 2,6
(3) It dictates thigh, pelvis, trunk and head kinematics. 8 An SVA of 10–12° incline is the optimum position of the shank that allows the thigh to become inclined and the pelvis and trunk to move forward in a vertical position 8 (Figures 3d-f, 5 and 6). If the shank is vertical the thigh cannot move to an inclined position, unless you can hyperextend the knee (Figures 3c). If the shank is too inclined then the thigh cannot become inclined, as the centre of mass within the pelvis would have to move outside the base of support and balance is lost (Figures 3i, 4c). There is only a small range of SVA where it is possible to incline the thigh, maintain a vertical trunk, and balance. It is 7–15° inclined, 10–12° being the optimum position 8 (Figures 3f, 4b and 5c).
(4) It facilitates appropriate ground reaction force alignment to the knee and hip and switching of moments, from flexion to extension moments, at the knee and hip. 8,10 The movement of the pelvis and trunk from a position behind the knee to one in front of the knee, during the trunk glide, moves the centre of mass which is situated within the pelvis. This facilitates switching of the moments, created by the GRF, at
Positions of the shank and resultant Ground Reaction Forces in standing. Still images taken from ORLAU Transportable Video Vector Generator. 8 (a) SVA vertical/0°. Excessive knee extension moments and hip flexion moments. (b) SVA 10–12° inclined. Appropriate knee and hip extension moments. (c) SVA 20° inclined. Loss of knee and hip extension moment.
the knee and hip, from flexing to extending moments (Figures 3d-f, 4b and 5a-5c). Extending moments at the knee and hip are essential for the stability in stance required at the end of MST and through TST (Figures 7). Appropriately inclined shanks ensure that appropriate, rather than insufficient or excessive, moments are created (Figures 3 and Figures 4).
(5) It may contribute to conservation of energy. The inclined position of the shank shortens the stance limb and lowers the vertical excursion of the centre of mass, at the time when it is at its highest, which has been linked to conservation of energy. 2,19–22 The flexed knee created at this time from the shank inclination is one of the six determinants of gait for conservation of energy 22 (Figures 6).
(d) Maximum knee extension does not occur in midstance. It occurs at 40% of the gait cycle in terminal stance, with an inclined shank and thigh. The knee is flexed in midstance, with an inclined shank. A common belief that the shank and thigh are vertical in MST with a fully extended knee is erroneous. Maximum knee extension occurs later in the gait cycle, at 40% GC, in terminal stance (TST) 1,3 (Figures 7a). Maximum hip extension occurs at 50% GC (Figures 7b). The ankle is relatively rigid through TST, in dorsiflexion, and it is the quasi stiffness of the ankle that permits maximum hip and knee extension and GRF alignment anterior to the knee and posterior to the hip, creating stabilizing knee and hip extension moments. Such stability of the stance leg in TST facilitates full terminal swing of the swing limb and the creation of ‘the BIG V’ (Figure 7b). Achieving the ‘BIG V’ has consequent benefits of stretching and strengthening, 8,23 ‘therapy while walking’, so improving quality of life (Figure 8).
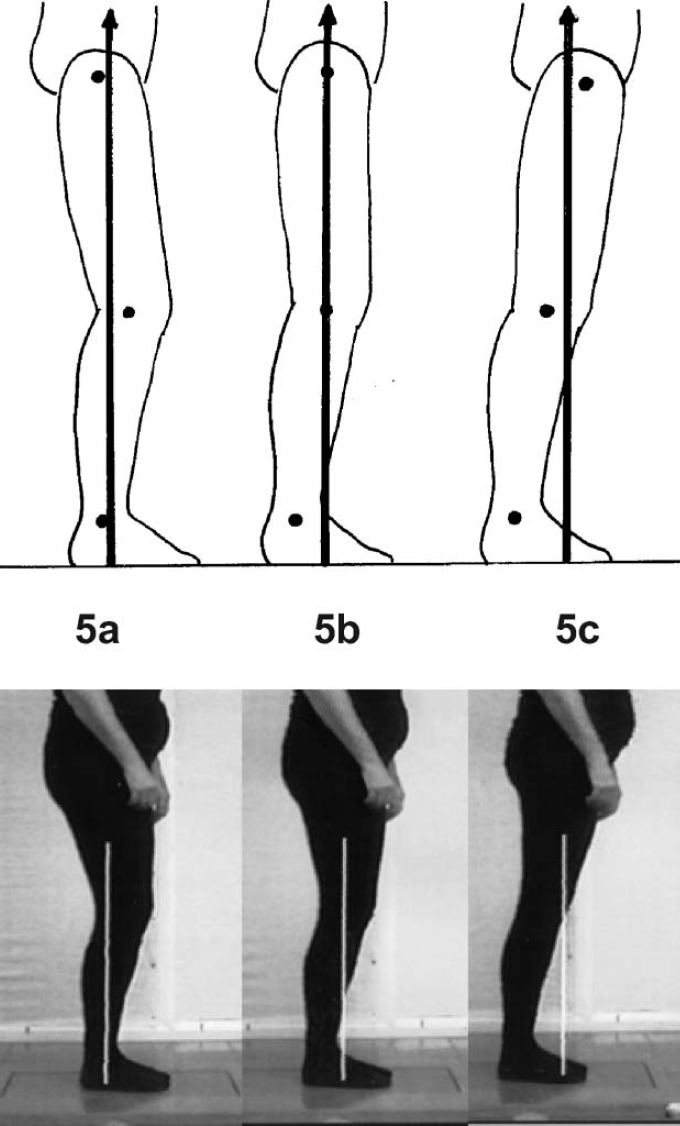
SVA 12° inclined (a, b, and c) allowing posterior (a) and anterior (c) translation of a vertical trunk. Still images taken from ORLAU Transportable Video Vector Generator. 8 (a) Posterior translation of trunk. Reclined thigh. Knee flexion and hip flexion moments. Point of application of Ground Reaction Force aligned at posterior foot. (b) Vertical thigh. Neutral knee and hip moments. Point of application of Ground Reaction Force aligned at centre of foot. (c) Anterior translation of trunk. Inclined thigh. Knee extension and hip extension moments. Point of application of Ground Reaction Force aligned at anterior foot.

Knee over middle of foot and slowing of shank. ‘Stability in stance’. 8
(e) Shank kinematics are independent of ankle kinematics. The kinematics of the ankle will adjust to a variety of heel heights automatically. 24 However, the shank kinematics remain the same 8 (Figure 9). The exception to this is if one wears very high heels, when the horizontal projection of the foot becomes shorter.

(a) 40% gait cycle, maximum knee extension. (b) 50% gait cycle, maximum hip extension with knee extension, inclined shank and thigh, the ‘Big V’.
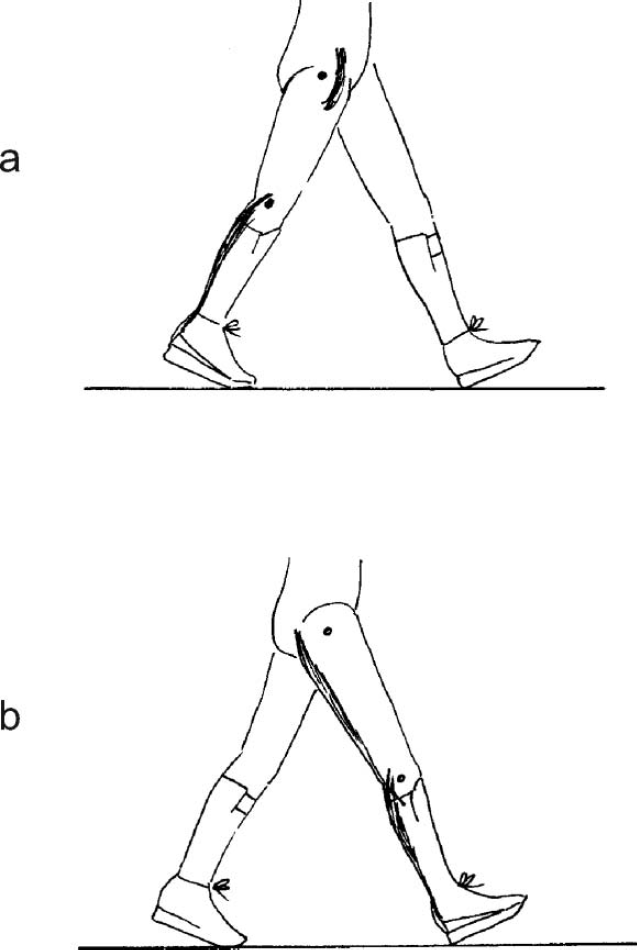
The ‘Big V’ of terminal stance and terminal swing producing muscle stretches. 8 (a) Ankle-Foot Orthosis Footwear Combination worn on right leg facilitating Terminal Stance and stretching hip, knee, hip flexors and gastrocnemius. (b) Ankle-Foot Orthosis Footwear Combination wom on left leg facilitating Terminal Stance on left and consequently Terminal Swing on right and stretching knee, hamstrings and gastrocnemius.
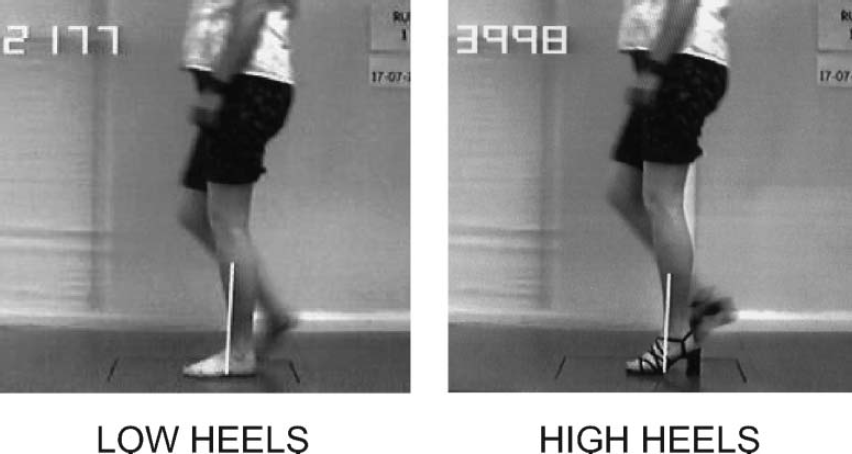
Shank kinematics are independent of ankle kinematics. 8
(f) It is helpful to describe four, rather than three, rockers in normal gait. 25 Replication of normal shank kinematics in gait, by orthotic and other interventions, is essential. We have been taught that the forward progression of the shank is produced by ‘three rockers’, which require movement at the ankle for the first and second rocker and at the metatarsophalangeal joints (MTPJs) for the third rocker 3 (Figures 10a). The first (heel) rocker occurs during loading response (LR), the second (ankle) rocker occurs during MST and the third (forefoot) rocker occurs during both TST and preswing (PSW). 3 In TST the MTPJs extend and this movement is coupled with ‘quasi stiffness’ of the ankle in dorsiflexion, with hardly any movement 3 (Figure 7b). It is this stiffness of the ankle that facilitates heel rise. 3,26 However, in PSW the MTPJs continue to extend but this is coupled with very rapid movement of the ankle, from the dorsiflexed position at the end of TST to a plantarflexed position at the end of PSW. 3 Dividing the forefoot rocker into a third rocker in TST and a fourth rocker in PSW 25 recognizes the difference in ankle kinematics in TST compared to PSW.
In pathological gaits all or any of the rockers can be insufficient or excessive. An ideal design of orthosis would correct the abnormal rocker movements at both the ankle and MTPJs, during each subdivision of the GC. Because of the different requirements of these joints during each of the four rockers this is not yet easily possible and compromises have to be made. We therefore often have to fix the ankle joint and also sometimes the MTPJs. This prevents use of anatomical rockers and allows us to gain control of the production of the
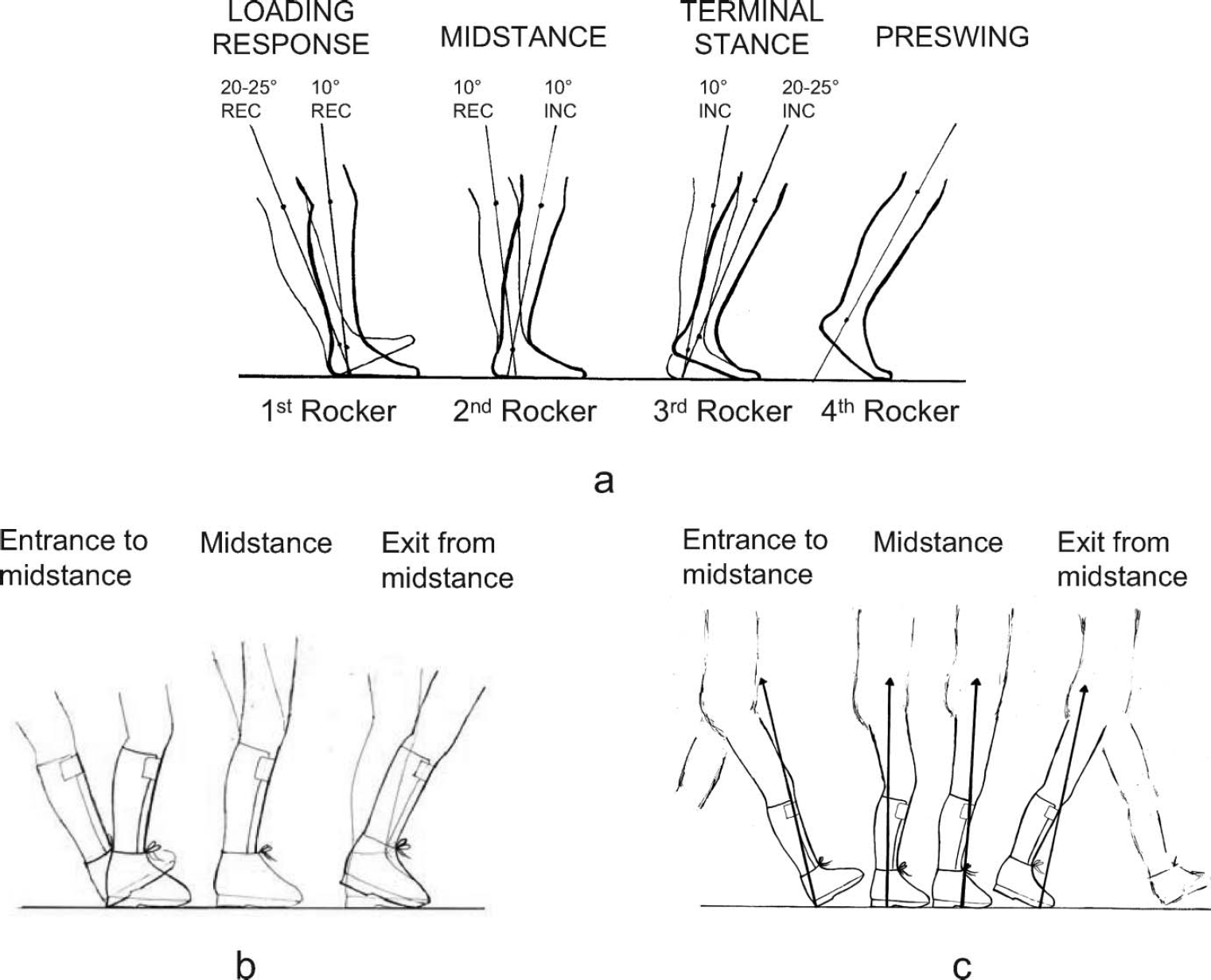
(a) Forward progression of shank produced by the rockers. (b) Producing normal shank kinematics with an AFOFC. (c) Producing normal segment and joint kinematics and kinetics with an AFOFC.
shank kinematics by the use of simulated rockers, created by the design of the footwear that is combined with the ankle-foot orthosis (AFO) 8,27 (Figure 10b, 10c). The footwear is therefore an equally important part of the orthosis and the significance of the part the footwear plays can be recognized by calling the overall orthosis an AFO-Footwear Combination. 8,28,29
Categorizing the abnormal shank kinematics of pathological gait
Current categorizations of pathological gait are based on joint kinematics. 30–37 However, it is manipulation of the shank segment kinematics, by the AFOFC design, to produce as near normal shank kinematics as possible, that will be the key to a successful orthotic intervention. 38 Normalization of shank kinematics will facilitate most normal thigh, pelvis and trunk kinematics and subsequently most normal knee and hip kinematics and kinetics 8 (Figure 10b, 10c).
When pathological gait is observed in the sagittal plane there are two basic categories of abnormal shank kinematics 8,27 (Figure 11). These are insufficiently inclined shanks or excessively inclined shanks during some or all of the subdivisions of the GC. In addition, some pathological gaits may even combine these abnormalities in one GC, for example excessive incline followed by insufficient incline.
Following the principle that different designs of AFOFCs will be needed to normalize such different gait abnormalities, it is possible to create an algorithm for the design and tuning of an AFOFC based on shank kinematics 27 (Figure 12). The importance of basing the algorithm on shank kinematics is that we concentrate on correcting insufficient or excessive shank incline, at the times in the GC that these abnormalities occur. This is a different approach to that of concentrating on correcting the movement of the joints, which will not necessarily correct shank kinematics.
An algorithm for design and tuning AFO-footwear combinations based on shank kinematics 27
This algorithm is based on 11 years of experience of designing and tuning AFOFCs for a population of children with cerebral palsy, spina bifida and other conditions on the ORLAU transportable Video Vector Generator Gait Laboratory. This provides a video recording of gait together with simultaneous visualization of the GRF which is superimposed on the video image. It has freeze frame and slow motion facilities. 39–41 Pathological gait can be analyzed and AFOFC designs optimized to produce objective normalization of both the kinematics and kinetics of gait. Some aspects of the algorithm and research results challenge traditional beliefs. It also introduces AFOFC designs that make prescriptions more effective.
(a) Hinged versus fixed. The algorithm starts with observation of the stance phase of gait, to determine whether shank kinematics are normal. If not, a fixed ankle AFO is recommended because strong orthotic control of the ankle is required if the shank kinematics are to be controlled sufficiently to enable control of more proximal segment and joint kinematics and kinetics. AFOFCs with hinges are inadequate, when the shank kinematics cannot be controlled, and superfluous, when the hinges are not used once the AFOFC is tuned.
(b) The Angle of the Ankle in the AFO (AA-AFO) and the Shank to Vertical Angle of the AFOFC are independent. It is theoretically possible to create any SVA with any AA-AFO by alteration of the pitch/‘heel sole differential’ of the footwear 8 (Figures 12
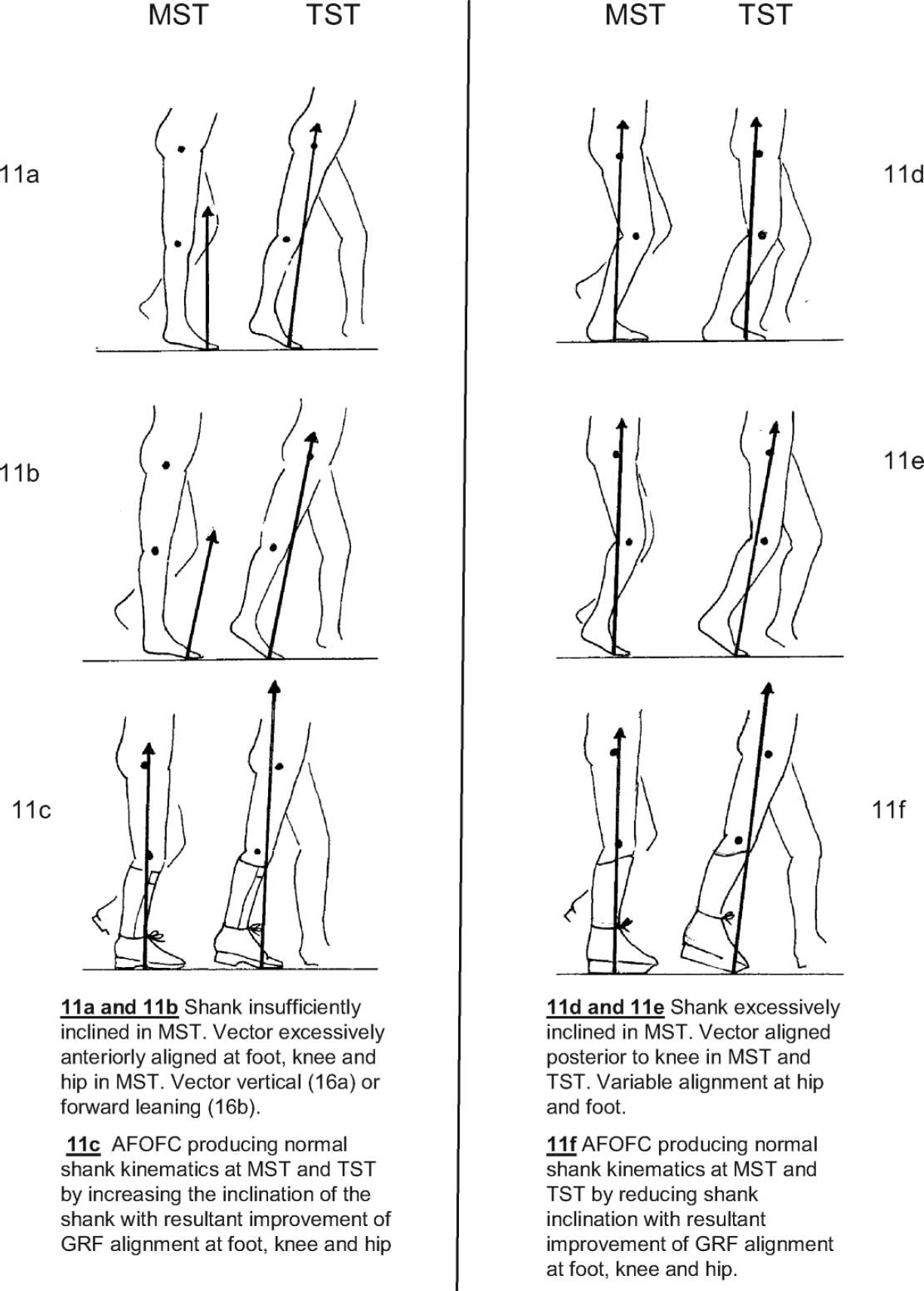
Abnormalities of shank kinematics in pathological gait. 8
and Figures 13). There is often a belief that the SVA and AA-AFO are inextricably linked, it being assumed that it is only possible to alter one by altering the other (Figure 13a, 13e, 13i). This belief can confound and invalidate research.
(c) There is poor recognition of the differentiation between AA-AFO and the SVA in the literature. A search of 310 publications 8 found that only nine differentiated and contained sufficient information to determine the SVAs used. 28,42–48 Of these only three included gait trials of a variety of SVAs to support their findings. 28,45,48
(d) A prerequisite for successful interventions and tuning of AFOFCs is an optimal AA-AFO. Common beliefs are that the AA-AFO must always be 90° or that dorsiflexion and plantigrade positions are acceptable, but not plantarflexion. The belief about 90° may have come from the belief that the shank must be vertical to obtain straight knees when walking. Optimal AFOFCs use a variety of AA-AFO and the use of plantarflexion may be essential. 49 In addition, a plantarflexed AA-AFO may increase musculotendinous unit length, facilitate knee extension in gait, allow the musculotendinous unit to be at

A clinical algorithm for the design and tuning of ankle-foot orthosis footwear combinations (AFOFCs) based on shank kinematics.
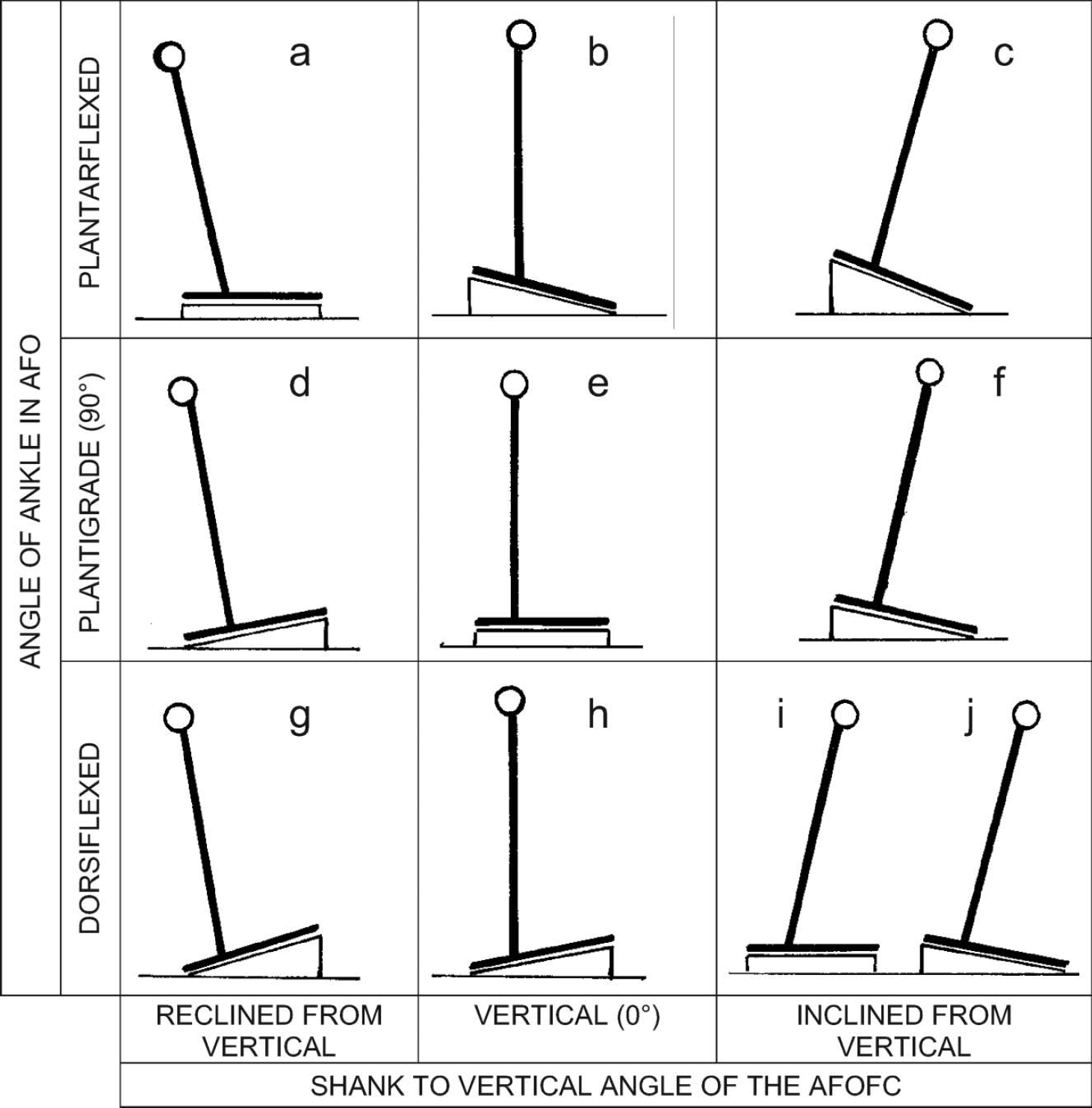
Nine theoretical configurations of the Angle of the Ankle in the Ankle-Foot Orthosis and the SVA of an Ankle-Foot Orthosis Footwear Combination. 8
the optimum length for force production and prevent the development of bony foot deformities caused by enforced supination or pronation within the AFO 49 (Figure 14). The use of plantarflexed AA-AFO to gain musculotendinous unit length is counter-intuitive but does occur. 20,21 There are a number of considerations that are involved in determining the optimal angle. These have been described in a separate algorithm. 49 The starting point of the algorithm is the measured length of the gastrocnemius muscle, measured with the knee extended and the foot dorsiflexed. This measure will vary according to whether the foot is pronated, supinated or neutral. The algorithm recommends that the position with the least amount of range is chosen as a starting measure. For feet that ‘escape’ into pronation, the supinated range will be the starting measure. For feet that escape into supination, the neutral position will often be the measure. The algorithm incorporates opportunities for interventions but frequently clinicians are left with difficult decisions that are very individual for each leg of each patient.
(e) Shank alignment needs to be more inclined than it has been traditionally, for children at least. Our work has been the only study that has optimally tuned, using combined kinematics and kinetic gait analysis, the SVAs of the AFOFCs of a population of independently ambulant children, walking without aids, with cerebral palsy, spina bifida and other, mainly neurological, conditions. 8,9 The study showed that the tuned SVAs of 74 children using 112 AFOFCs, range from 7–15° incline with a mean of 11.36° (Figures 15). There is therefore a match between the mean SVA of the tuned AFOFCs and the mean SVA in MST of barefoot normal gait and 10–12° is a good place to start when tuning the SVA. No children had optimal SVA of 0–6°. The SVAs were more inclined than the traditional 0–7° setting. Other studies are now concurring with our findings. 7,50,51 Tuned AFOFCs place the SVA in the optimal position in MST and also provide the slowing of the angular velocity of the shank, both of which are required to replicate the distal stability of normal shank kinematics.
(f) The literature does not recognize the importance of tuning/optimizing the SVA of an AFOFC. A search of 310 publications 8 found that only 22 alluded to the importance of the SVA of an AFOFC and/or tuning. 19–21,43–48,52–61
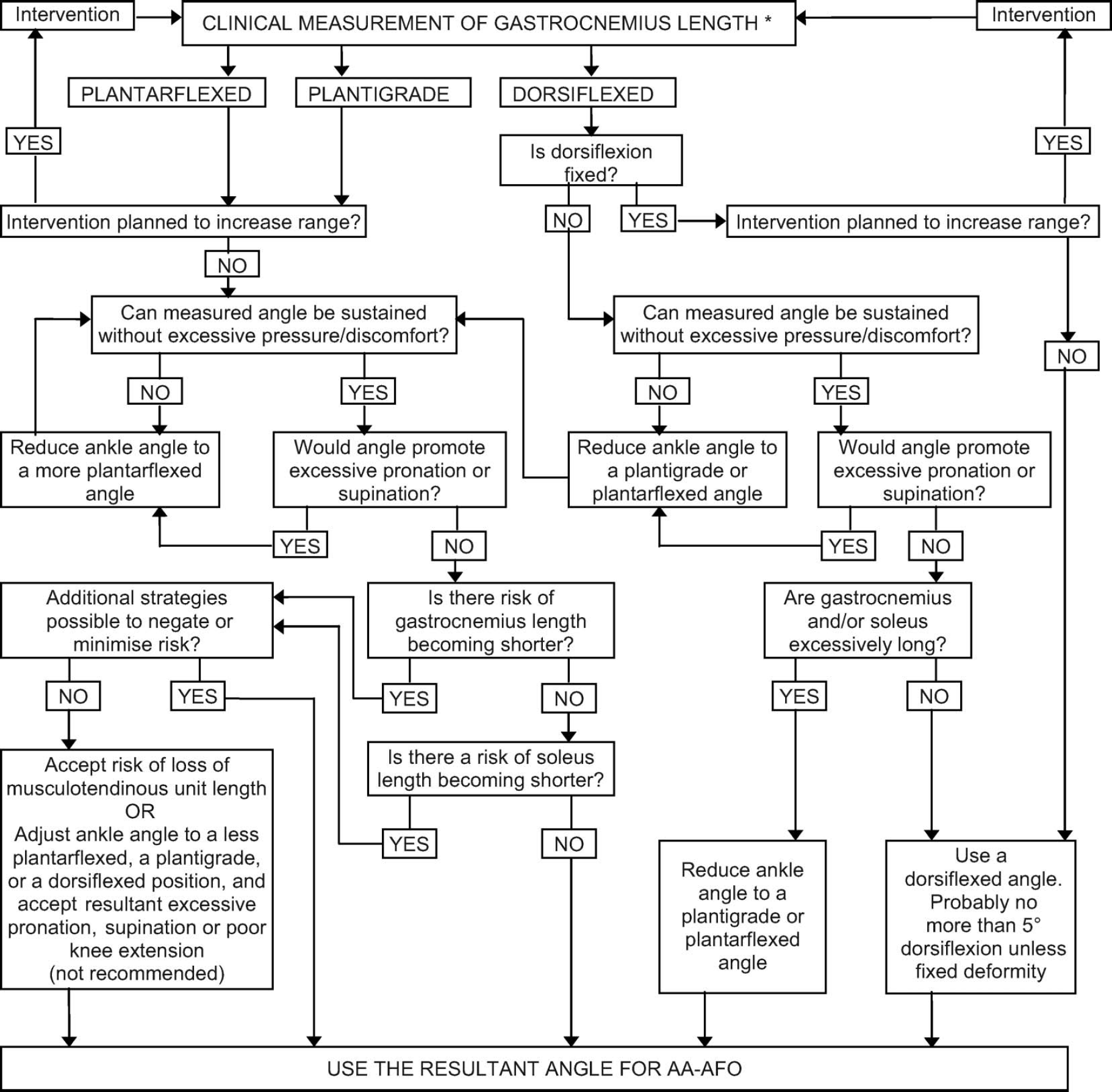
Proposed clinical algorithm for deciding the sagittal angle of the ankle in an ankle-foot orthosis footwear combination.
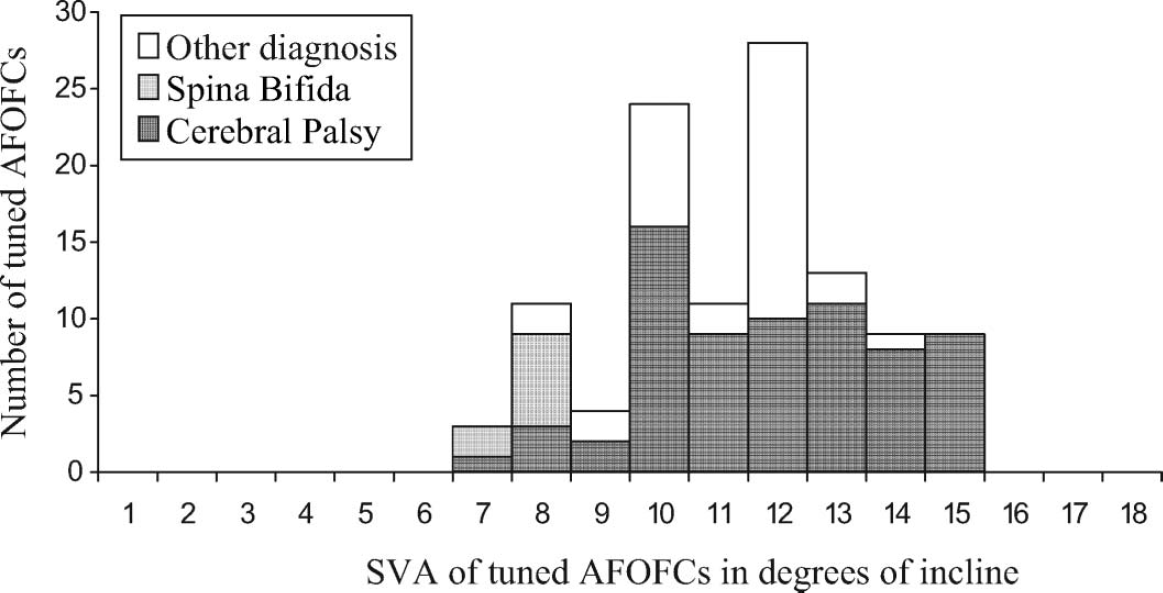
Frequency distribution graph of SVA of tuned AFOFCs by diagnosis. 8
(g) Point Loading Rockers 27,28,45,62,63 are almost always essential if gait with excessively inclined shanks is to be controlled. For a ‘Point Loading Rocker’ (PLR) to be effective, the sole must be very stiff and completely flat until the rocker, there must be an acute angle at the position of the rocker and sufficient toe spring angle 27,62,63 (Figure 12). The position of PLRs, and the accompanying toe spring angles, optimized by kinematic and kinetic tuning, has been determined for AFOFCs used on 23 legs of children with disability. 62 The PLR length mean was 78% (range 70–88%). So, when tuning a PLR a good starting point is to position it at 80/85% along the length of the footwear and move it backwards or forwards as required. Mean toe spring angle was 33° (range 18–50°).
Conclusion
This paper has attempted to show why it is important to be earnest about shank and thigh kinematics, especially when using AFOFCs, whatever the objectives for their use. These may include improvement in standing balance, gait, activity and participation; development of normal segment kinematics and motor learning; 48,52,53,58 prevention or improvement of bony and joint deformity; normalization of muscle length, strength and stiffness.