
Abstract
Background:
Improving ankle-foot orthosis design can best be done by implementing a user-centered approach.
Objective:
To provide insight into the ideas of ankle-foot orthosis users with flaccid ankle muscle paresis on the importance of activities and suggestions for an improved ankle-foot orthosis design.
Study design:
A focus-group discussion with eight ankle-foot orthosis users (57 ± 5 years, 50% female).
Methods:
Main inclusion criteria were as follows: ⩾18 years, unable to stand on tip-toe and unable to lift toes. Main exclusion criterion was spasticity of lower extremity muscles. Transcribed data were coded according to the International Classification of Functioning, Disability and Health. Thematic analysis with inductive approach was chosen to order and interpret codes.
Results:
Ankle-foot orthosis users ranked walking the most important activity followed by sitting down/standing up from a chair. Their opinion was that ankle-foot orthoses facilitate walking and standing. Ankle-foot orthosis users suggested that an improved ankle-foot orthosis design should balance between stability and flexibility.
Conclusion:
Current ankle-foot orthoses facilitate walking which was the most important activity according to ankle-foot orthosis users. An improved ankle-foot orthosis design should enable walking and should optimize between stability and flexibility dependent on the activity and the paresis severity.
Clinical relevance
Experienced users of ankle-foot orthosis agreed that matching ankle-foot orthosis functions to daily-life activities is a trade-off between stability and flexibility. An improved ankle-foot orthosis design should at least enable level walking.
Background
People with flaccid ankle muscle paresis generally experience problems during walking due to reduced dorsiflexion strength (needed for clearance and controlled plantarflexion during loading response) and/or plantarflexion strength (needed for push-off). 1 To improve functioning, an ankle-foot orthosis (AFO) can be prescribed. 2 The function of an AFO determines what it must do. 3 For people with flaccid paresis, the main AFO function is to compensate for muscle weakness, while for people with spastic paresis, this function is to re-align the joint. 2 Due to these function differences, different AFOs can be used depending on the paresis, and therefore, these paresis types should be evaluated separately.
AFOs prescribed for people with flaccid ankle muscle paresis can improve walking. 4 However, using an AFO can also come with disadvantages. 4 Dorsal AFOs, for example, limit ankle range of motion (ROM). 4 This can hamper activities that require a large ankle ROM such as slope walking. 5 Improving AFO design can be done best by implementing a user-driven design process as the factors that are most important to users will be taken into account. 6 User-driven design is more and more applied in product design to improve acceptance of an innovation by the user. 7 In this case, when an AFO fits the needs of users better, adherence to using AFOs can improve.8,9 Especially, a qualitative study design can reveal the most important factors since AFO users are not limited by pre-specified questions as is usually the case in quantitative study designs. 10 More specifically, a focus-group discussion allowing users to interact is likely to reveal common issues. 11 We found one study that evaluated experiences with AFOs. 9 However, as they included people with spastic paresis, findings may not be applicable to people with flaccid paresis.
The aim of this explorative study was to provide insight into the ideas of AFO users with flaccid ankle muscle paresis, on the importance of activities and suggestions for an improved AFO design. Providing insight into the importance of activities requires ranking activities according to importance and exploring experiences with these activities.
Methods
Participants
Inclusion criteria were as follows: aged ⩾18 years, unable to stand on tip-toe (without AFO), unable to lift toes (without AFO), use an AFO more than once a week in the last 6 months, able to understand and speak Dutch, able to adequately attend the focus-group discussion, and able to answer general questions on AFO use over the past 6 months. Exclusion criteria were as follows: spasticity of lower extremity muscles, diabetes mellitus, and the AFO was prescribed for night splinting. Client records from an orthopedic workshop (OIM) in Haren, were used to identify people eligible for inclusion. Client records of clients who received an AFO in the last 2 years were retrieved. OIM preselected records that complied with the selection criteria and sent these clients an information letter containing all selection criteria. Clients who indicated they met these criteria and gave permission to be called were called by the first author (D.W.) who re-checked all criteria with the client. Included participants were informed that they could withdraw any time without consequences. All participants provided written informed consent. The Ethics Committee of the University Medical Center Groningen approved the study (no. 2013/198).
Study design
An iterative process 12 was used to provide insight into the ideas of AFO users on the importance of activities, and suggestions for an improved AFO design. This process started with five explorative expert interviews: three patients (with dorsiflexor-, plantarflexor-, and combined paresis, respectively), a rehabilitation physician, and an orthotist. From these interviews, the key activities according to participants that needed to be included in the next stage were identified. These activities included the following: walking, driving a car (control of pedals), sitting down/standing up from a chair, riding a bike, climbing stairs, slope walking, and squatting.
The process continued with a questionnaire (Sup-plemental Material 1) to gain insight into the ranking according to the importance of previously mentioned activities and to add activities to be discussed in the focus group. The questionnaire was additionally used to collect participant characteristics (sex, age, self-reported body weight, self-reported body height, pathology, affected leg, years of AFO use, and AFO type) and generate open-ended questions for the focus-group discussion plan. All participants completed the questionnaire at home and returned it 1 week prior to the focus-group discussion. In the questionnaire, participants indicated whether they used their AFO to perform specific activities, how well they could perform this activity, measured using a 100-mm visual analogue scale (VAS), 13 and whether they found this activity important, also measured using a 100-mm VAS. 13 Participants could add extra activities in open-ended questions. These open-ended questions revealed further activities that participants identified, which following the iterative process, were included in the next stage. These activities included maintaining a standing position and choosing shoes.
Thereafter, the focus-group discussion was conducted to provide insight into the importance of activities and suggestions for an improved AFO design. This discussion was held at a university building in the evening and in the evening. Ms. D.W., orthotist and MSc, moderated the discussion and was assisted by the second author (Mr. J.H.M., PhD). Both authors had a research background and expertise in the area of human movement and orthotics. J.M.H. had experience conducting focus-group discussions. During the discussion, participants were sitting at a round table to allow face-to-face contact. 14 Each participant had a name tag in front of them. After a personal introduction round, the discussion started. A discussion plan (Table 1, translated from Dutch) with open-ended 15 questions was structured 16 to introduce the study aim, make the transition to in-depth questions, and to finalize the discussion. During the in-depth part, pages containing the activities (mentioned in the questionnaire) were displayed on the table. Participants discussed this list of activities and could add activities they thought were missing. This revealed one additional activity: walking in swimming pool. Participants then ranked the activities according to importance. The main in-depth questions were as follows: “Why are some activities more important than others?” and “What would you like to improve concerning your AFO?”. If a statement was unclear, open-ended questions were asked for clarification. Total duration of the discussion was 2 h (excluding 15 min of break). Audio-recordings were used for literal Dutch transcription of the full discussion.
Discussion plan.
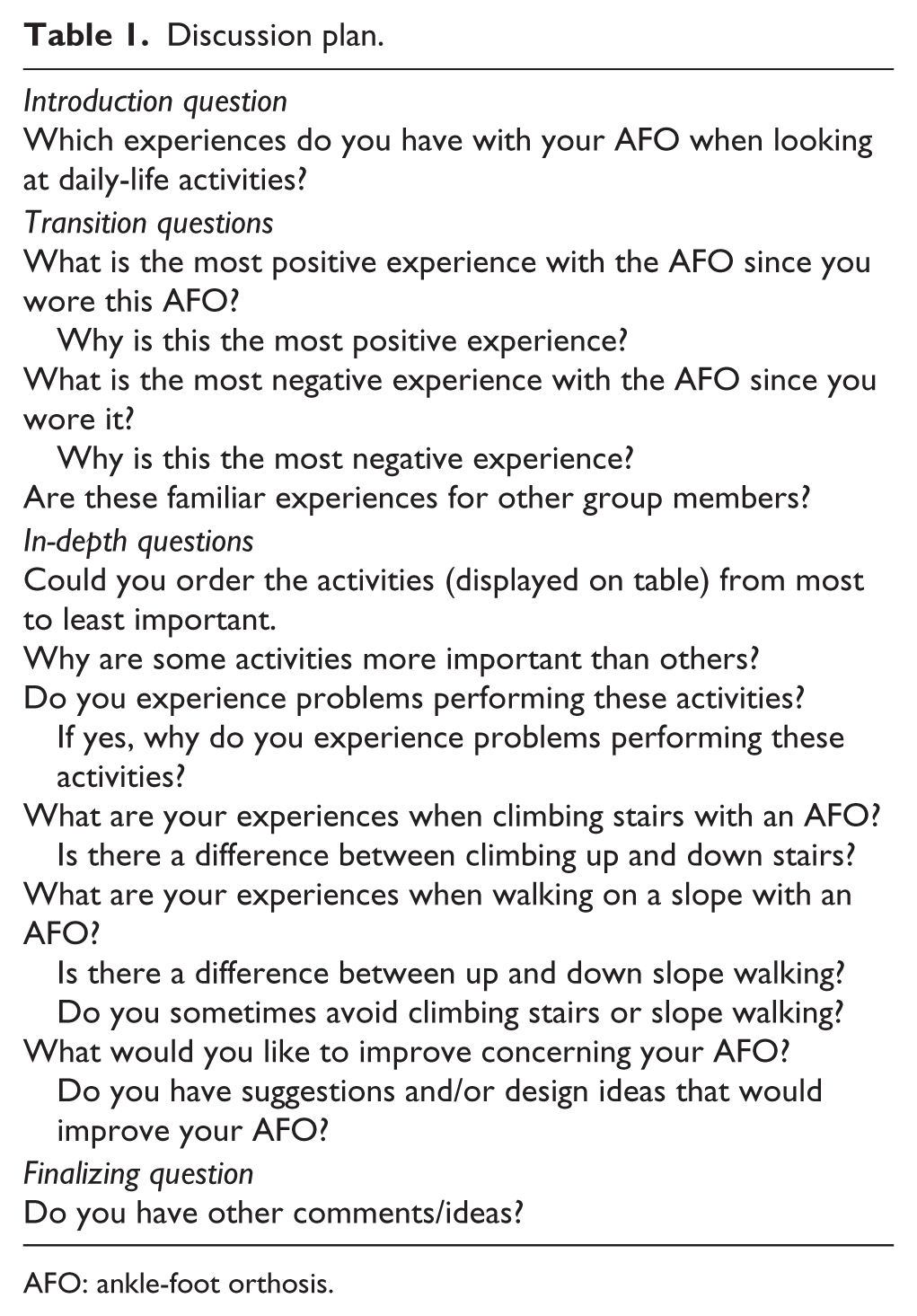
AFO: ankle-foot orthosis.
The iterative process was finalized by sending the discussion summary to all participants. In this letter, participants were invited to review again by providing additional remarks if something was missing. Participants had no remarks.
Thematic analysis
Previously proposed guidelines for thematic analysis were used as guidance. 17 As we aimed to study experiences with AFOs, 18 we used the Dutch version of the International Classification of Functioning, Disability and Health (ICF)19,20 to code the transcription and to order codes into a conceptual framework. An inductive approach was chosen to allow themes to arise from the transcription and by aiming to reduce the preconceptions of the two researchers who coded the data to a minimum.17,21 The transcription was analyzed as proposed previously. 17 This process consisted of three phases (Supplemental Material 2). The first phase was familiarization in which D.W. read and reread the transcription to get familiar with the data and to form ideas on initial codes. The second phase was code generation in which the transcription is coded, first using initial codes, followed by key codes (Supplemental Material 3). At 65% of the transcription, all key codes were formed. The third phase was theme generation during which first initial themes were generated based on the co-occurrence of key codes. These initial themes were revised into final themes to ensure these themes to be sufficiently unique and identifiable. At 94% of the transcription, all themes were formed. Thematic maps were used to visualize major and minor themes. Atlas.ti7© (version 7.5.6) was used to aid this analytical process. Quotes presented in the results were translated by a native English speaking person who is familiar with the Dutch language.
Results
Participants
In total, 153 invitations were sent. A total of 34 (22%) clients responded, of which 15 were unable to participate. Checking selection criteria resulted in the exclusion of 11 clients because of spasticity of lower extremity muscles (n = 6), diabetes mellitus (n = 2), inability to adequately attend the focus-group discussion (n = 2), and the ability to stand on tip-toe (n = 1). The remaining eight (Table 2) were included which is an optimal sample for a single focus-group discussion. 14 Participants were not acquainted with each other. Only participant 8 and the moderator had met before. All participants used custom made, non-hinged AFOs for 13 ± 3 h/day. Seven participants used their AFO daily. Participant 2 used his AFO 6 days/week. Participants 1 and 8 had experience with hinged dorsal AFOs. Participants 3, 6, and 7 were using more flexible dorsal AFOs.
Participant characteristics.
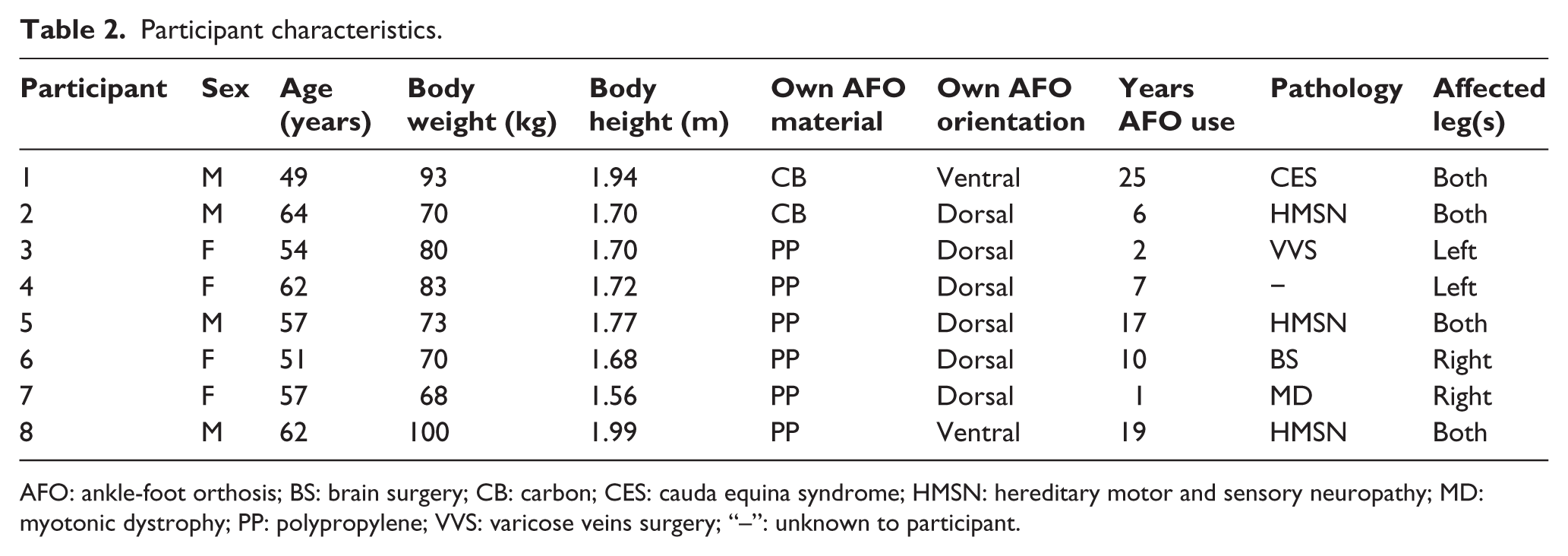
AFO: ankle-foot orthosis; BS: brain surgery; CB: carbon; CES: cauda equina syndrome; HMSN: hereditary motor and sensory neuropathy; MD: myotonic dystrophy; PP: polypropylene; VVS: varicose veins surgery; “–”: unknown to participant.
Importance of activities undertaken while using AFOs
AFO users ranked 11 activities from most (walking) to least important (standing up from/sitting down on the floor; Figure 1). AFO users were generally unable to squat and stand up from, or sit down on, the floor with their AFO. Therefore, they avoided these activities.
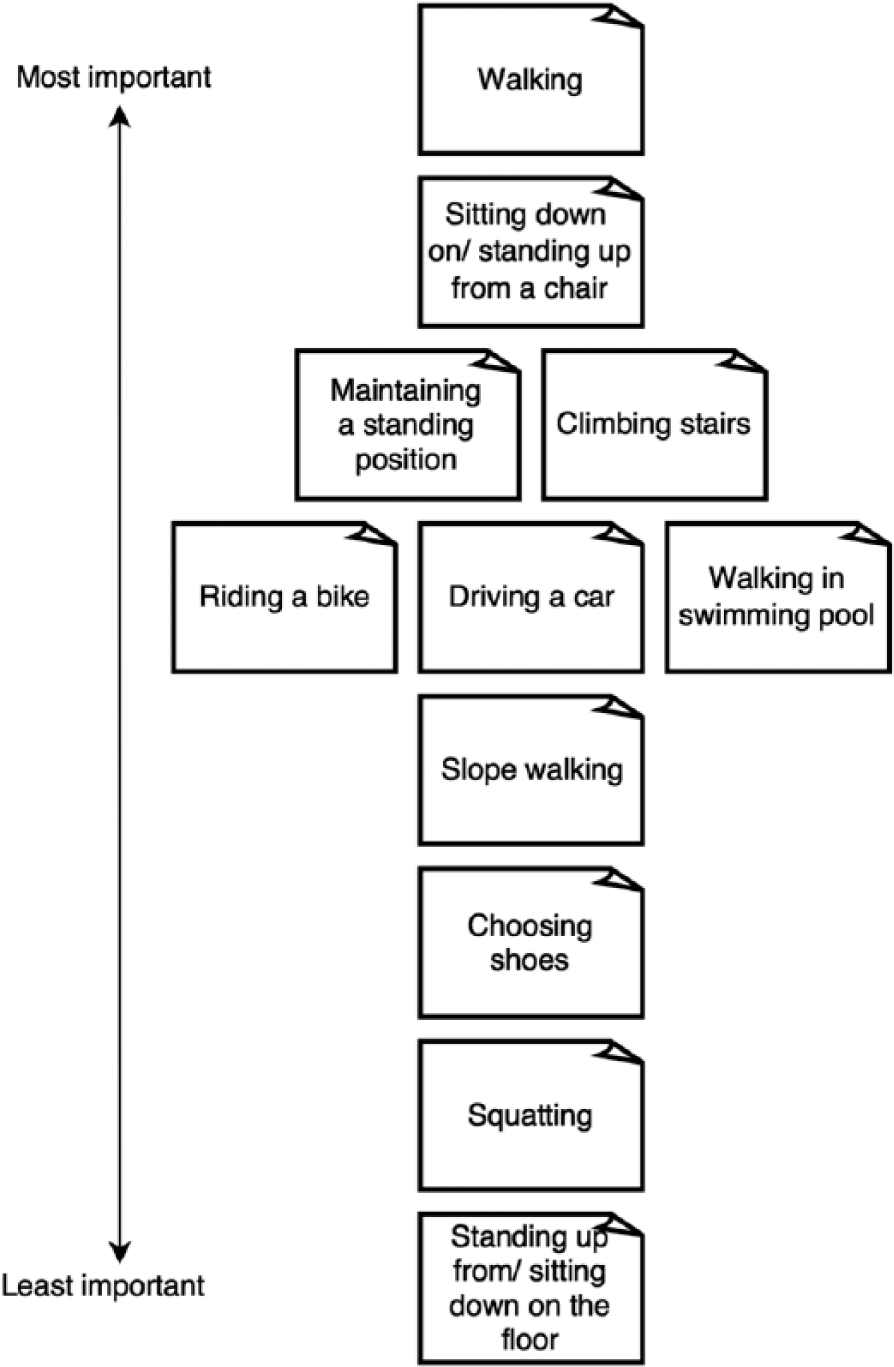
Ranking activities undertaken while using AFOs.
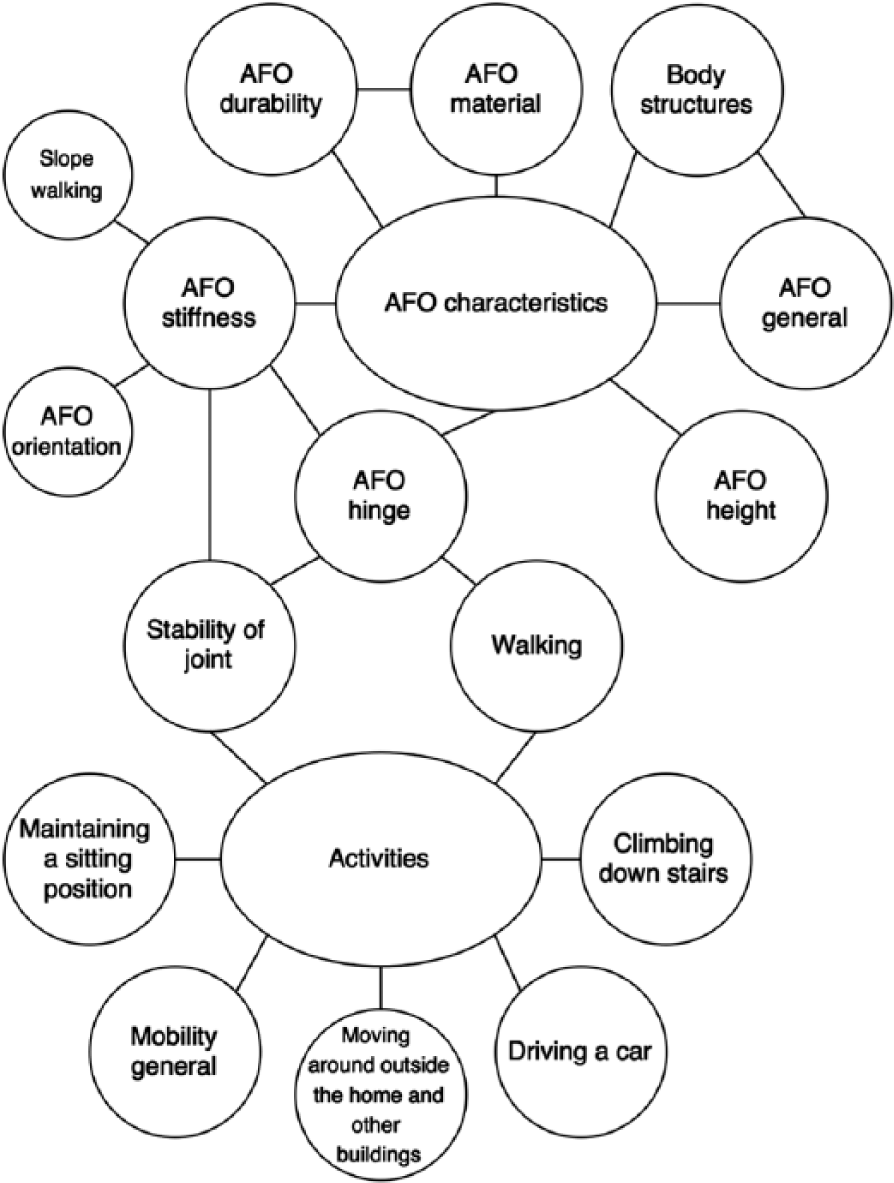
Thematic analysis of experiences with AFOs resulted in the generation of three major themes (Figure 2).
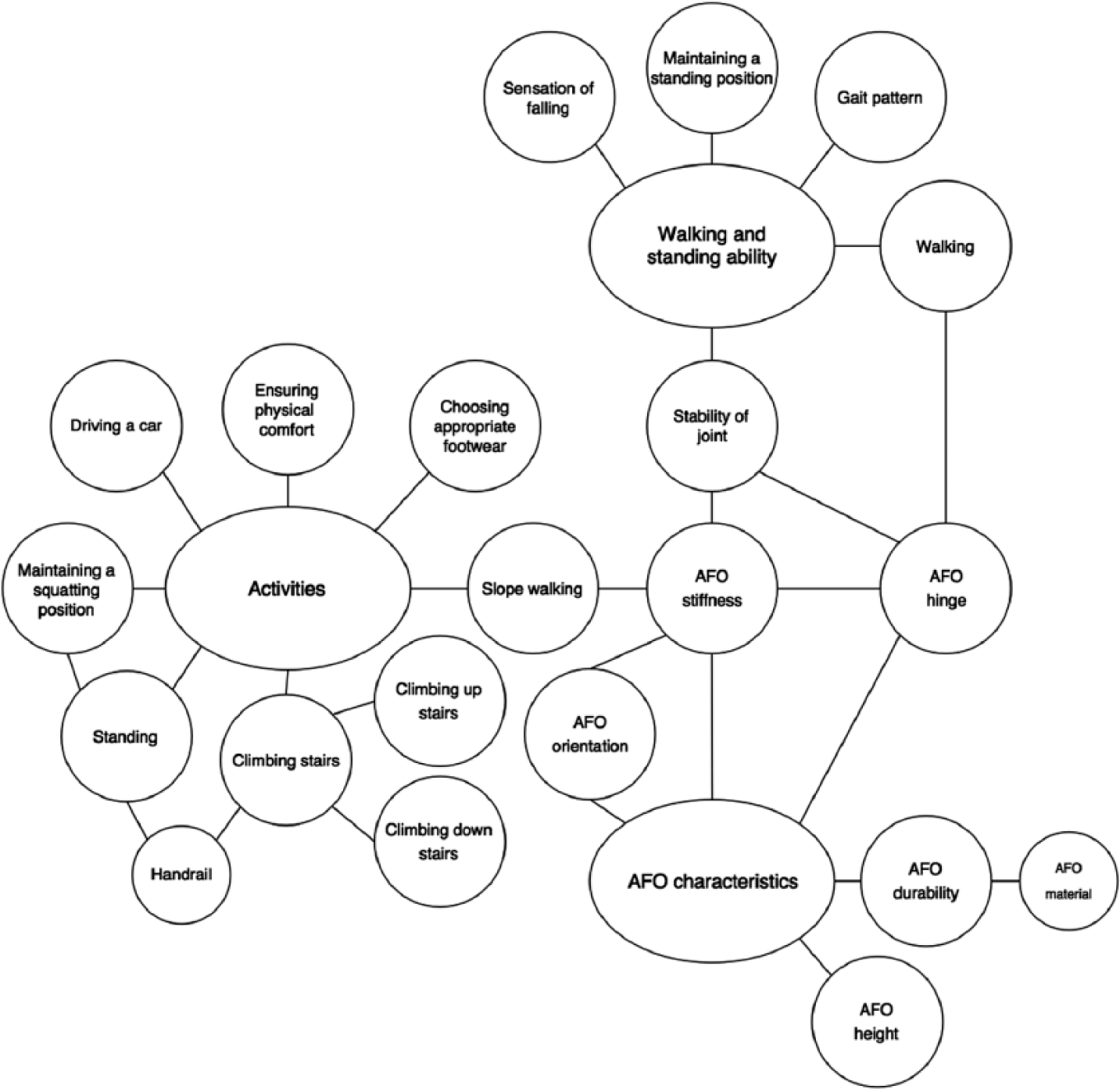
Thematic map on experiences with activities undertaken while using AFOs.
Walking and standing ability
AFO users mostly mentioned that walking improved with AFOs. They explained that the way they walked looked more normal with AFOs as they needed less compensatory strategies:
If you have that orthosis, you’re more robust. You walk safely, as normal. (Participant 2) [Without AFO, my legs] were going more upwards than forwards. (Participant 5)
Using AFOs enabled them to walk longer distances and made them more stable when walking and standing, with experiencing less falls:
[With AFO] you don’t stumble so easily any more. (Participant 7)
AFO characteristics
AFO characteristics are operationalized as an umbrella term for AFO category, mechanical stiffness, durability, and AFO height. AFO users found that having a hinged or flexible AFO, and not a static one, makes walking slopes and stairs easier as you need some flexibility:
[Hinged AFOs] enable you to extend your foot when climbing down the stairs. (Participant 1)
The disadvantage of having a hinged AFO, according to AFO users, was that it generally provided less stability during walking and it was less durable:
My mechanical hinges lasted seven months, after which they started to wear out. (Participant 8)
Users mentioned that the material of their static AFOs occasionally broke as it could not withstand climbing stairs or long-term use:
I walked stairs, however [my static ventral AFO] could not withstand this and broke. (Participant 3)
One AFO user found that shorter AFOs were more comfortable, but at the same time provided less stability, making walking more difficult as was predicted by the orthotist:
I have short AFOs which are far more comfortable, but the downside is that your walking ability diminishes. (Participant 6)
Some AFO users mentioned that ventral AFOs had the advantage that they decreased knee flexion during stance. This enabled these AFO users to walk longer distances without getting tired:
A ventral AFO prevents knee flexion which saves a lot of energy during walking. (Participant 1)
One AFO user mentioned that getting stuck with the top of a dorsal AFO behind the seating of their chair could not happen with ventral AFOs:
[With ventral AFOs] I can never get stuck [behind the seating of my chair]. (Participant 8)
Activities
Female AFO users mentioned that choosing shoes was difficult with AFOs:
I don’t like the fact that I always have to wear heavy shoes. I would also like to wear other types of shoes. (Participant 3)
AFOs were not very comfortable with several AFO users mentioning prints the AFO left on their legs after wearing it:
When you take [your AFO] off, you see exactly where it used to be. (Participant 6)
AFO users, in general, found that AFOs hampered controlling pedals in a car and standing up from the floor. Squatting was almost impossible with AFOs according to AFO users:
The clutch in the car is difficult to control [with solid AFOs]. (Participant 5) Getting up from the floor and squatting, I am not able perform either of those activities [with solid AFOs]. (Participant 1)
These same AFO users indicated that they were physically able to perform these activities without AFOs, some with the use of handrails. Especially climbing down stairs was difficult with AFOs and requires the use of handrails for most AFO users:
I think that without a banister no one would be able to climb the stairs. (Participant 2) Climbing up the stairs is still feasible, but climbing down the stairs is a disaster. (Participant 1)
Suggestions for an improved AFO design
Two major themes were generated for suggestions for an improved AFO design (Figure 3).
Thematic map on suggestions for an improved AFO design.
AFO characteristics
According to AFO users, an improved AFO design should balance between stability and flexibility:
Really, [improved AFO design] should enable a person to set when [the AFO] can flex and when it cannot. (Participant 6) [Improved AFO design] should balance between flexibility and stiffness. (Participant 1)
AFO users mentioned that for every individual with a different body weight and body height, and for every activity, this balance changes:
There’s a different solution for every individual. (Participant 8)
All modes should be combined into one design:
I want everything into one design. (Participant 2)
The material of an improved AFO design should be durable according to AFO users:
I hope they can find a stronger and more durable material. (Participant 1)
Activities
Improved designs should facilitate stability according to AFO users. It should enable an AFO user to perform all sorts of activities such as controlling the pedals in a car, for example, by putting the AFO into a different mode:
For example when you are going to drive a car, you click [your AFO] so it can flex. (Participant 5)
Discussion
The aim of this explorative study was to provide insight into AFO users’ ideas on the importance of activities and on their suggestions for an improved AFO design. AFO users indicated that the most important activities were as follows: walking and sitting down/standing up from a chair. AFOs generally improved walking while standing up from a chair was difficult with AFOs. AFO users suggested that an improved AFO design should balance between stability and flexibility dependent on the activity and paresis severity.
Importance of activities undertaken while using AFOs
We found no previous research in which AFO users ranked daily activities. Yet, a majority of previous research that evaluates AFO users with flaccid ankle muscle paresis focusses on walking and finds improvements with AFO use. 4 Walking was also incorporated in the core set of outcomes for studies examining AFO effects. 22
Remarkably, sitting down/standing up from a chair was not incorporated in this core set. 22 We only found studies on AFO users with spastic ankle muscle paresis standing up from a chair.23,24 Both studies found a better weight distribution with AFOs23,24 but did not report participant’s ideas on the importance or difficulty of standing up from a chair, which is an opportunity for future research.
Suggestions for an improved AFO design
Improved AFO design should provide stability and flexibility and should at least enable walking as existing AFOs do. People with severe ankle muscle paresis may require more AFO stability during level walking. 25 An activity such as standing up from a chair may require more flexibility. 26 Using a hinged ventral AFO with varying stiffness, such as a Neuro Swing placed on a ventral AFO, 27 could provide stability during walking 28 and possibly provide sufficient flexibility to stand up from a chair without getting stuck behind the seating. The problem with hinged AFOs is that they consist of a fixed stiffness and thereby are unable to mimic the stiffness profile of a normal ankle. 25 Therefore, we are developing a novel AFO that provides stability and flexibility depending on the activity and paresis severity.
Methodological considerations and study limitations
The most important limitation is that a single focus-group discussion was performed, and all participants used non-hinged AFOs. Therefore, generalizability of our results is limited. To improve generalizability, we aimed to recruit a heterogeneous group in terms of participant characteristics. We succeeded in most characteristics; however, there were no participants aged <49 years or participants who were using hinged AFOs. Therefore, new key codes and themes may arise if multiple focus-group discussions were performed with different AFO users. Despite this limitation, our results contribute to the developmental process of an improved AFO design and provide insight into the importance of activities in AFO users with flaccid ankle muscle paresis.
Data saturation was partly reached. Following completion of 65% of the transcription, all key codes had been formed, while all themes had only been formed, following completion of 94% of the transcription. Therefore, more themes could be formed in a second focus group with the same participants. Triangulation of the questionnaire and focus-group results showed similar trends. The two lowest performance scores (Supplemental Material 1) were squatting and standing up from/sitting down on the floor, which are consistent with the focus-group results. The highest impact scores were walking on the street, cycling, hobbies, and sitting down/standing up from a chair which is also comparable to the focus-group results. These similarities between questionnaire and focus-group results demonstrate the validity of our results.
We chose to only include regular AFO users as they have extensive experience with AFO functioning. People who do not use an AFO regularly are generally less impaired and do not depend on an AFO. 29 Performing a focus-group in non-regular AFO users will give other insights, as well as including AFO users with spastic paresis.
It can be questioned if self-reported characteristics are valid selection criteria. These criteria and the possibility that only people with mainly positive AFO experiences replied to the request to participate may have caused selection bias. This bias was probably the case as AFO users argued about the group in general:
Everyone is so positive here. When I was in the [rehabilitation center], I found it awful … they all had these long faces. And when I come here, most people are positive. I was not expecting this. (Participant 1) I think most people that are like you describe, did not respond. (Participant 3)
We chose a dependent moderator to lead the focus-group discussion. In contrast, it is suggested that an independent moderator is preferred as they are supposed to be more objective. 30 In our opinion, the dependent moderator was suitable as she had a technical and scientific background and was therefore able to ask technically oriented questions if a statement was unclear.
Future research
To aid generalizability, multiple focus-group discussions should be performed with different AFO users. It could be valuable to spread a validated questionnaire evaluating the importance of activities with AFOs and suggestions for an improved AFO design among a larger group of AFO users.
Conclusion
In this study, thematic analysis was used to gain insight into AFO users’ ideas on the importance of activities and on their suggestions for an improved AFO design. One focus-group discussion among AFO users with flaccid ankle muscle paresis was performed. These AFO users found walking the most important, followed by sitting down/standing up from a chair. They found that AFOs, in general, improved walking, while standing up from a chair was difficult with AFOs. Improved AFO design should at least enable walking and preferably sitting down/standing up from a chair. AFO users suggested that an improved AFO design should balance between stability and flexibility depending on the activity and paresis severity.
Footnotes
Acknowledgements
The authors would like to thank all participants for their contribution in this study. Also many thanks to the time invested by Steven Bos and Frank van de Streek.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by the University Medical Center Groningen, the SNN (grant number T1015) the alliance of Northern Netherlands and OIM Orthopedie.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.