
Abstract
Background:
One intervention often used to address physical impairments post stroke is an ankle–foot orthosis. Ankle–foot orthoses may improve walking speed, stride length, and gait pattern. However, effects on balance, crucial for safe ambulation, are thus far inconclusive. One aspect of balance shown to contribute to functional ability is self-efficacy. Self-efficacy, defined as the belief in one’s ability to succeed in particular situations, has been shown to be more strongly associated with activity and participation (as defined by the International Classification of Functioning, Disability, and Health) than physical performance measures of gait or balance.
Objectives:
We investigated whether self-efficacy, or balance confidence when referred to in the context of balance capabilities, is improved with ankle–foot orthosis use.
Study design:
Repeated measures study design.
Methods:
Balance confidence was measured using the Activities-specific Balance Confidence Scale in 15 persons with chronic poststroke hemiplegia, with and without their regular ankle–foot orthosis.
Results:
Activities-specific Balance Confidence Scale scores were significantly higher (p ≤ 0.01) for the ankle–foot orthosis condition compared to no ankle–foot orthosis.
Conclusions:
One mechanism by which ankle–foot orthosis use may influence balance is improved balance confidence. Future work should explore the specific mechanisms underlying this improvement in self-efficacy.
Clinical relevance
Self-efficacy may be an important factor to consider when evaluating functioning post stroke. Rehabilitative interventions that improve balance confidence may help restore participation and overall functioning in pathological populations, particularly in the fall-prone poststroke population. Study results provide evidence for improvements in balance confidence with ankle–foot orthosis use.
Keywords
Background
Stroke, affecting about 795,000 people each year, is the leading cause of serious long-term disability in the United States. 1 Rehabilitative efforts commonly focus on the physical consequences of stroke. 2 In addition to extensive physical therapy efforts to address physical impairments, orthotic intervention is often prescribed. For example, one common consequence of stroke is an equinovarus deformity of the hemiparetic foot. An ankle–foot orthosis (AFO) can be used to address this deformity with the intent of improving standing and walking. 3
While there are no randomized controlled or controlled clinical trials that unequivocally support the use of AFOs in the poststroke population to improve walking, reviews of the literature indicate that AFO use in adults with hemiplegia may result in improved walking speed, stride length, and gait pattern.4,5 Additionally, research participants report that AFOs are comfortable and improve their gait.6–8
Evidence regarding biomechanical effects of AFOs on balance post stroke is inconclusive and less strong than for the effects of AFOs on gait. 9 The maintenance of balance is multidimensional, requiring the coordination of cognitive, proprioceptive, cerebellar, vestibular, and motor mechanisms. 9 One aspect of balance that may be affected by AFO use and particularly relevant to functioning post stroke is self-efficacy.2,10 Self-efficacy has been shown to be more strongly associated with activity and participation (as defined by the International Classification of Functioning, Disability, and Health (ICF), where activity is performance of a task or action and participation is partaking in a life situation) than physical performance measures of gait or balance. 10 Self-efficacy has also been shown to be a stronger predictor of basic activities of daily living (ADL) performance than balance capacity in persons with stroke living in the community. 11 Therefore, it is reasonable to propose that self-efficacy may be an important factor to consider when evaluating balance post stroke.
The Activities-specific Balance Confidence (ABC) Scale was designed to measure fall-related self-efficacy. 12 The ABC Scale, an extension of the Falls Efficacy Scale (FES), 13 addresses a wider range of activities and is suggested to be more responsive for use in populations with varying levels of functioning, such as individuals with stroke. 14 The ABC Scale has high test–retest reliability (intraclass correlation (ICC) = 0.85), excellent internal consistency (Cronbach’s α = 0.94), and moderate correlation with both the Berg Balance Scale (BBS) and gait speed as measured by the 8-m comfortable walk test in individuals at least 1 year post stroke. 14
Given the lack of conclusive information regarding the effect of AFOs on balance in persons post stroke and the potential importance of self-efficacy with regard to balance, the purpose of this study was to investigate whether balance confidence, as measured by the ABC Scale, is improved with AFO use and whether this improvement positively correlates with walking speed, a variable often used to classify the functioning of individuals post stroke. 15 We hypothesized that (1) balance confidence would increase when subjects were asked to imagine performing each activity with an AFO as compared to when they were asked to imagine performing the activities without an AFO, and (2) the change in walking speed with the AFO compared to without would be directly proportional to the change in balance confidence.
Methods
Persons with poststroke hemiplegia were recruited from a local rehabilitation hospital, the research subject database maintained in our center, and the surrounding community. Research subjects were required to be more than 1 year post stroke, 18 years of age and older, able to understand simple instructions, and currently wearing a nonrigid AFO. Nonrigid AFOs were targeted based on results from a review, 9 suggesting that more flexible AFOs seem to be better for dynamic balance conditions than rigid AFOs.
Subjects were excluded if they had other comorbidities that would affect gait or if they could not ambulate without assistive devices. This study was approved and subjects provided written informed consent prior to participation in the study.
Data for this study were collected as part of a larger study that involved two study-related visits. AFO data were collected at one visit, and No AFO data were collected at the other visit. The order in which each research subject completed the two visits was randomized. As part of the larger study, a passive retroreflective marker was placed over the sacrum. An eight-camera Eagle Digital RealTime motion capture system (Motion Analysis Corporation, Santa Rosa, CA, USA) tracked the sacral marker position while subjects walked back and forth across the laboratory floor. Position data were post-processed in Cortex and OrthoTrak software (Motion Analysis Corporation), and forward walking speed was calculated as the average velocity of the sacral marker for each gait cycle.
Following collection of walking speed data, the ABC Scale was administered by the same person each time. While a revised version of the ABC Scale was recently published, 16 it is important to note that the original ABC Scale developed by Powell and Myers 12 was used for this study. The instructions, as written on the ABC Scale form, 12 were read to each subject. An example response was also provided and explained to ensure that the instructions were appropriately understood. Subjects were then asked to respond to each item with their confidence in performing the activity without falling or losing their balance on a Scale from 0% to 100%, where 0% indicated no confidence and 100% indicated complete confidence in performing the activity without a fall. Per the ABC Scale instructions, subjects were also informed, “… if you do not currently do the activity in question, try and imagine how confident you would be if you had to do the activity.”
Depending on the visit, subjects were instructed to imagine completing the activities described in the ABC Scale with or without an AFO, but with no other assistive device. At the first visit, subject-specific data including gender, age, time since stroke, affected side, type of AFO, and other assistive devices regularly used (e.g. cane or scooter) were also obtained (Table 1).
Subject characteristics.
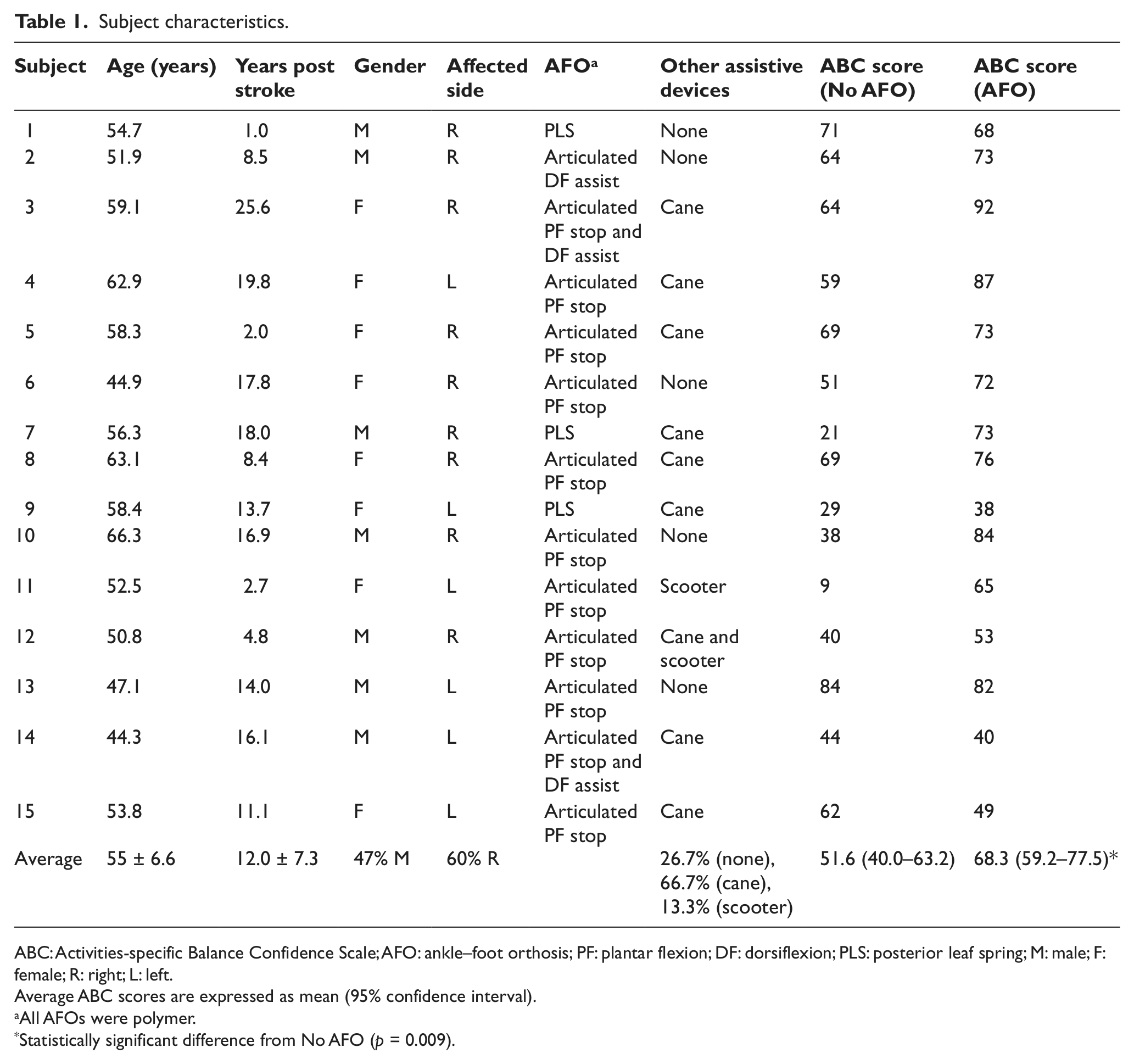
ABC: Activities-specific Balance Confidence Scale; AFO: ankle–foot orthosis; PF: plantar flexion; DF: dorsiflexion; PLS: posterior leaf spring; M: male; F: female; R: right; L: left.
Average ABC scores are expressed as mean (95% confidence interval).
All AFOs were polymer.
Statistically significant difference from No AFO (p = 0.009).
As specified by the original instructions, 12 an average score for the 16-item ABC Scale was calculated for each subject by dividing the sum of their total score by 16. Statistical analyses were performed using SPSS version 20 (SPSS Inc., Chicago, IL, USA). ABC scores for the AFO and No AFO conditions were examined for normality using the Shapiro–Wilk test (p ≥ 0.05). A paired t-test was used to examine differences in ABC scores between AFO and No AFO conditions with α set at 0.05. Pearson’s correlation coefficient was used to quantify the correlation between change in walking speed and change in ABC scores between the No AFO and AFO conditions.
To better understand the ABC scores, two secondary outcomes were examined. First, the 16 questions on the ABC Scale were analyzed individually to determine which activities were perceived as being most improved by AFO use. Next, each subject’s mean score was classified using cutoff scores proposed by Myers et al.: 17 individuals with ABC scores lower than 50% have low physical functioning as is typical of persons in home care, ABC scores between 50% and 80% are indicative of moderate physical functioning as is typical of patients in retirement homes and individuals with chronic health conditions, and individuals with ABC scores higher than 80% have high physical functioning as is typical of persons in community exercise programs. These cutoff values were determined from a study of 475 older adults 17 but have been previously used to contextualize ABC scores in the poststroke population.14,18–20
Results
In total, 15 participants completed the study. The mean age of subjects was 55 ± 6.6 years (mean ± 1 standard deviation), and the mean time post stroke was 12.0 ± 7.3 years. Of the participants, 47% were male and 60% had right hemiparesis (Table 1).
ABC scores for the No AFO and AFO conditions (Table 2) and the difference between the scores were normally distributed (p > 0.12). Balance confidence as measured by the ABC Scale was significantly greater with an AFO compared to without (p ≤ 0.01) (Figure 1).
Mean scores for individual ABC Scale items.
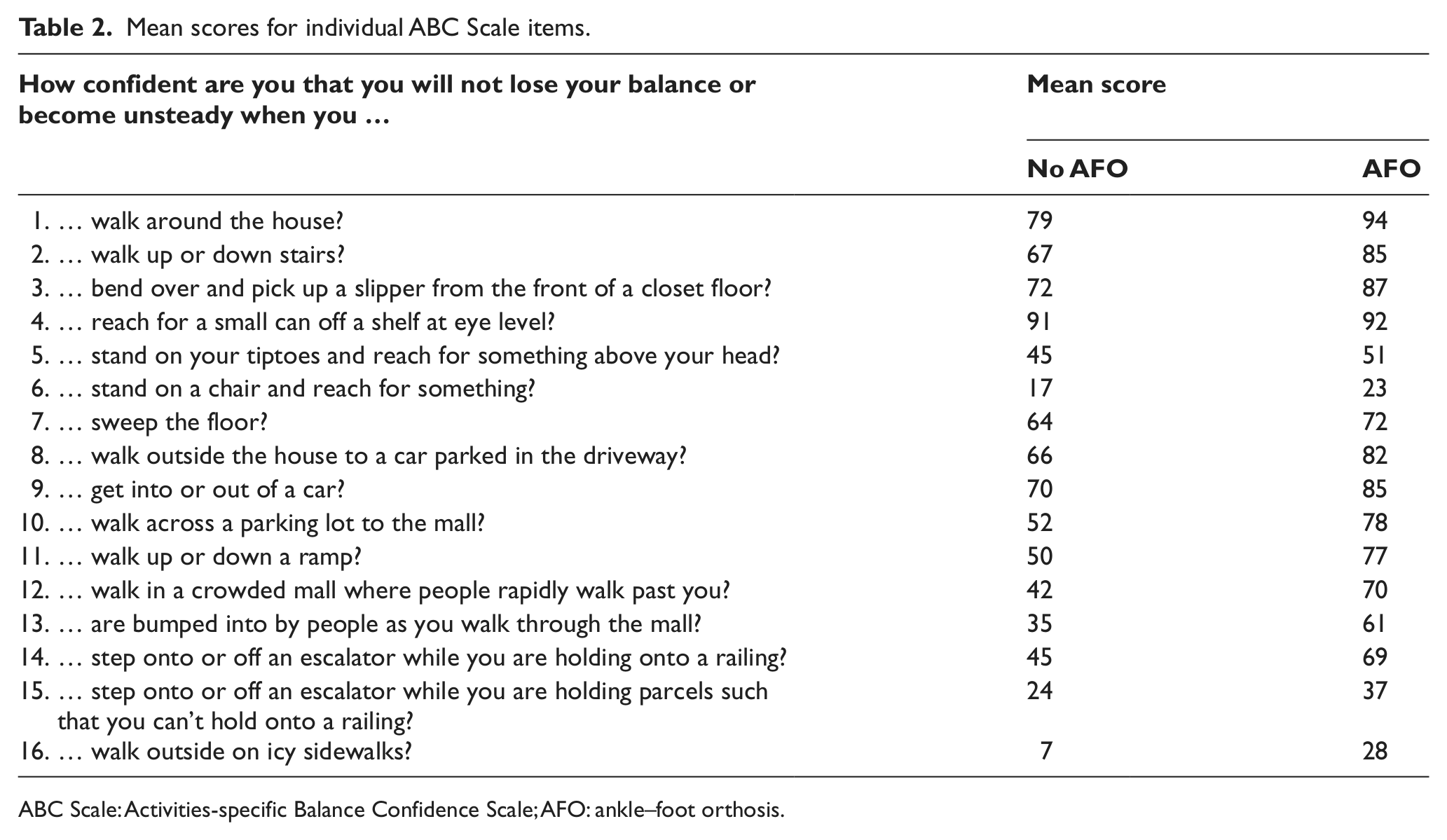
ABC Scale: Activities-specific Balance Confidence Scale; AFO: ankle–foot orthosis.
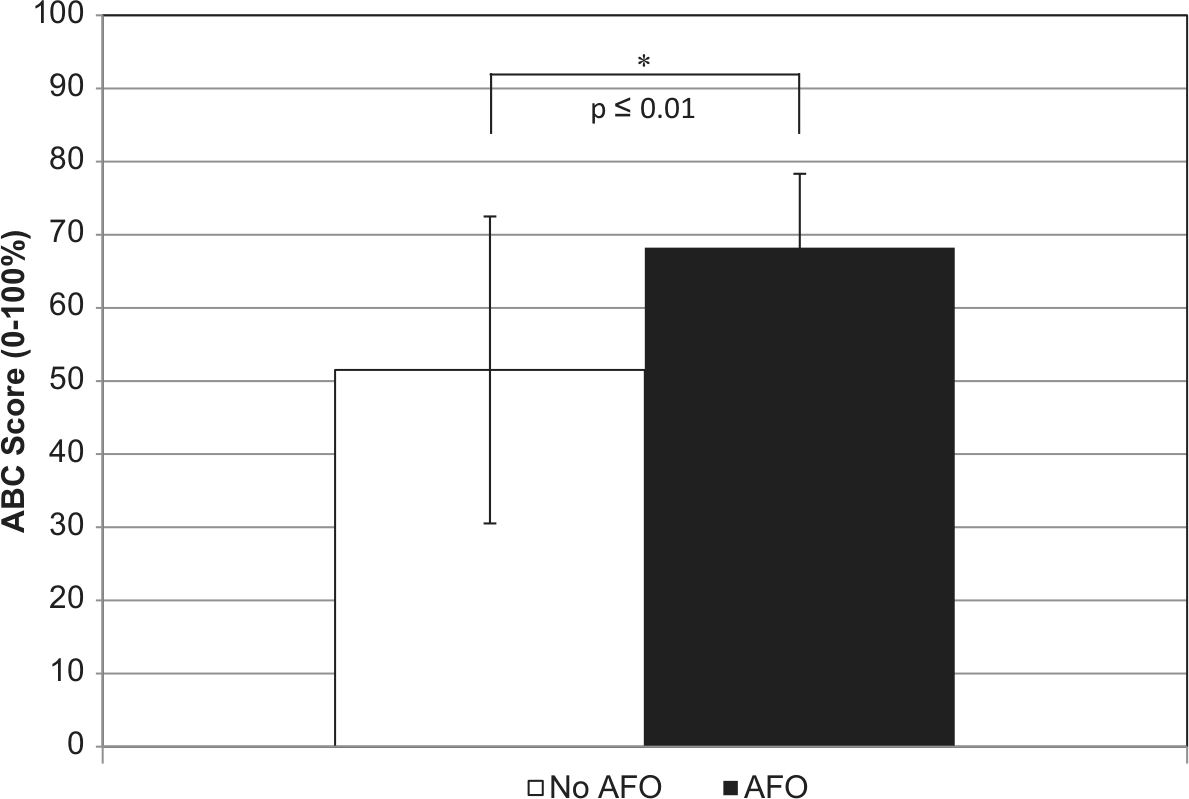
Mean ABC Scale score (n = 15) for AFO and No AFO conditions. Error bars indicate 1 standard deviation above and below the mean.
The change in walking speed from No AFO to AFO was positively correlated with the change in ABC score from No AFO to AFO (Figure 2, r = 0.506, p = 0.054).
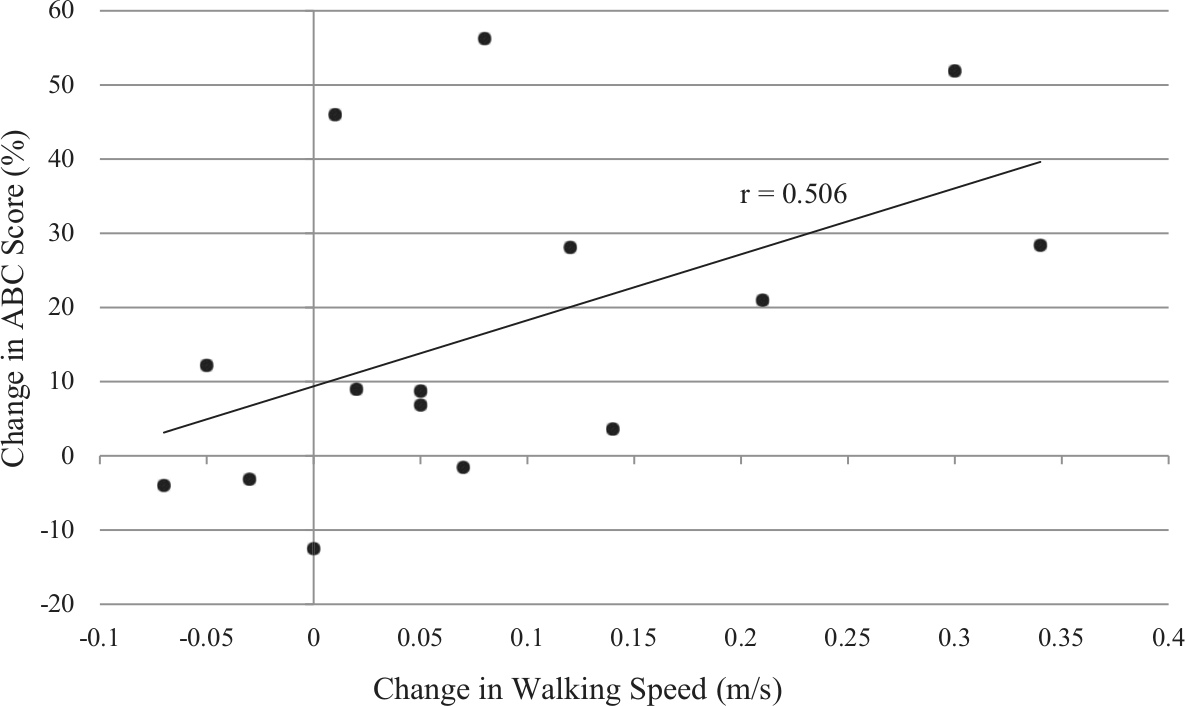
Correlation between change in ABC Scale score and change in preferred walking speed with AFO use.
A third of participants (5/15) reported an improvement in balance confidence of 50% or greater with AFO use for questions 12 (“walking in a crowded mall where people rapidly walk past”) and 16 (“walking outside on icy sidewalks”). Finally, using the cutoff percentages proposed by Myers et al., 17 when performing activities without an AFO, 7% of participants would be classified as high functioning, 53% moderate, and 40% low functioning. Conversely, when walking with an AFO, 27% of participants would be classified as high functioning, 53% moderate, and 20% low functioning (Figure 3).
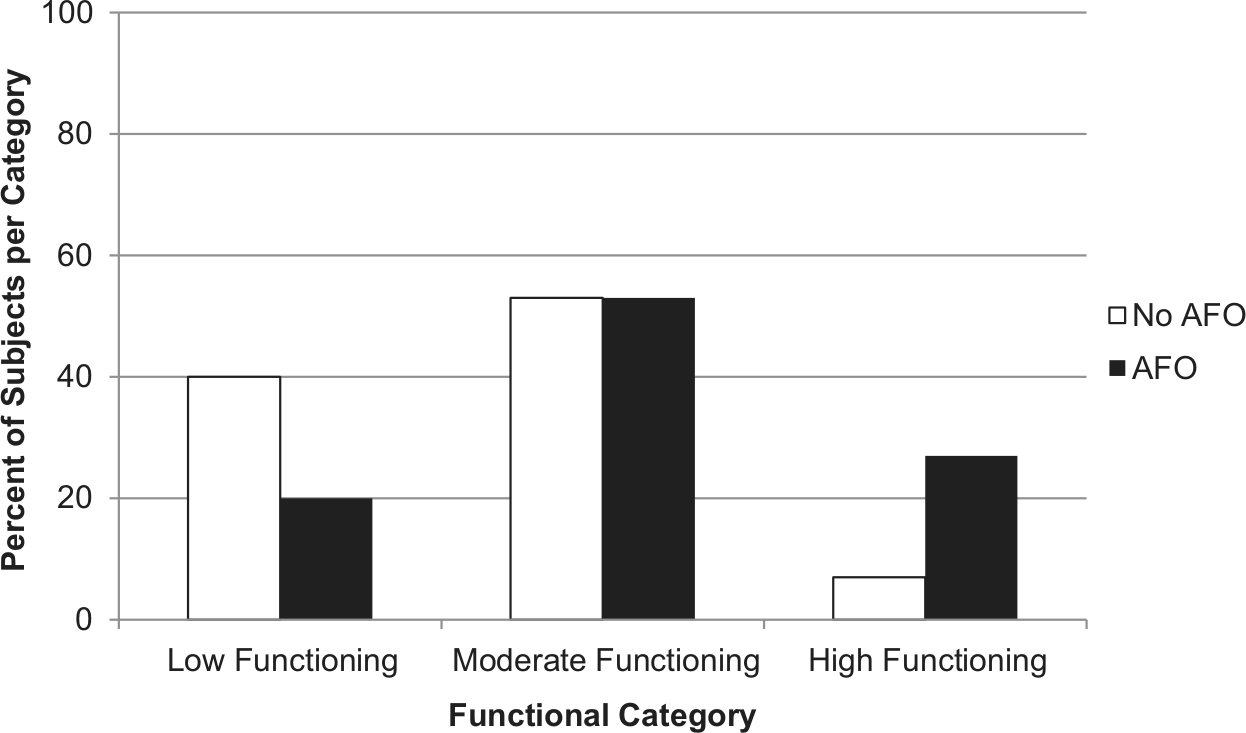
Classification of subjects based on ABC Scale score. 17
Discussion
This study examined balance confidence in persons with chronic poststroke hemiplegia with and without their AFOs. Our results support the hypothesis that balance confidence improves with use of an AFO (p ≤ 0.01). We are not aware of any other studies that have reported the effect of AFOs on balance confidence using the ABC Scale.
The results of this study corroborate anecdotal reports of improved balance confidence with use of AFOs by persons post stroke.7,8 While biomechanical effects of AFOs on balance performance remain inconclusive, 9 our results suggest that AFOs can improve balance confidence. Furthermore, since perceptions of ability may be as important as actual ability in determining functioning and mobility, 11 these findings suggest that one mechanism through which an AFO influences mobility is through improved balance confidence of the user.
While the primary objective of this study was to examine changes in balance confidence with AFO use, previous research has suggested that ABC Scale scores may be indicative of overall functioning. 17 Using the cutoffs proposed by Myers et al., 17 the percentage of subjects who are high functioning increases from just 7% without an AFO to 27% with an AFO, while the percentage of subjects who are low functioning decreases from 40% without an AFO to 20% with AFO use. This finding is intriguing given that the percentage of participants who are moderately functioning remains the same (53%). These results suggest that there may be a positive shift in functioning with AFO use. These categories are based on the ABC Scale, whereas classification based on walking speed is often used as an indicator of overall walking ability post stroke. 15 However, ABC Scale scores are only moderately correlated with walking speed, perhaps because it encompasses a wider array of functional capabilities. Future research should investigate other gait parameters that might contribute to changes in ABC Scale scores with AFO use post stroke, particularly those related to balance such as foot placement.21,22
There are several noteworthy limitations to our approach. First, this study population comprised a relatively small convenience sample of chronic poststroke individuals, and our results cannot be generalized to acute poststroke individuals nor can they be generalized to persons using rigid AFOs or other assistive devices.
Second, individuals in this study were, on average, more than a decade post stroke (12.0 ± 7.3 years) and presumably used an AFO for almost the same amount of time. This may have influenced subjects’ ability to accurately comment on their balance confidence while performing activities without an AFO. Underestimation of No AFO balance confidence could artificially inflate reported improvement with AFO use. However, our data do not suggest that time since stroke is correlated with larger differences in ABC scores with and without the AFO (ρ = 0.26).
Third, based on their walking speed, all participants except one were classified as limited community or community ambulators, 15 and therefore, it could be argued that the study population was more homogeneous than the general poststroke population. However, as described previously, we were able to stratify subjects into all three levels of physical functioning (low, moderate, and high) described by Myers et al. 17 These categories take into account other physical functioning characteristics in addition to walking speed and may therefore be a more robust classification of overall functioning. While these results suggest that balance confidence may contribute to mobility more broadly, and may be sensitive to orthosis use, this idea needs to be explored further in future research.
Conclusion
Growing evidence indicates that self-efficacy may be an important factor to consider when evaluating poststroke functioning. The results of this study support the hypothesis that balance confidence improves with AFO use in a chronic poststroke population.
Footnotes
Acknowledgements
The authors would like to acknowledge Rebecca Stine, MS, lab manager of the Jesse Brown VA Medical Center Motion Analysis Research Laboratory (JBVAMC-MARL) for assistance with data collection. The authors also acknowledge Richard Harvey, MD, and Elliot Roth, MD, at the Rehabilitation Institute of Chicago (RIC) Center for Stroke Rehabilitation, and Lynda McCracken, CPO, and Christopher Robinson, MBA, CPO, ATC, FAAOP at the RIC Prosthetics and Orthotics Clinical Center for their assistance with post-stroke subject recruitment.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Orthotic and Prosthetic Education and Research Foundation [grant # RFA OPERF-2010-FA-1] and the National Institute on Disability and Rehabilitation Research (NIDRR) Department of Education [grant # H133E080009] (Principle Investigators: Steven Gard and Stefania Fatone). The opinions contained in this publication are those of the grantee and do not necessarily reflect those of the Department of Education.