
Abstract
Background:
Until recently, no study had compared the quality of life of persons with transfemoral amputation treated with osseointegration to socket prosthesis users.
Objectives:
Comparison of quality of life in two types of prostheses users: a cohort of patients with osseointegration and patients equipped with a socket prosthesis who were group-matched for age, body mass index and mobility grade.
Study design:
A cross-sectional study that compared
Methods:
The quality of life of 39 participants (22 in the osseointegration group and 17 in the socket prosthesis group) was measured using the Questionnaire for Persons with Transfemoral Amputation (Q-TFA) and European Questionnaire 5-dimension 3-level (EQ-5D-3L) surveys.
Results:
Compared with the socket prosthesis group, the osseointegration group had a significantly higher ‘Global’ score (p = 0.022) and a significantly lower ‘Problem’ score (p < 0.001) of the Q-TFA. The ‘Mobility’ (p = 0.051) and ‘Use’ scores (p = 0.146) of the Q-TFA, the EQ-5D-3L index (p = 0.723), and EQ-5D visual analog scale (p = 0.497) showed no significant differences between groups.
Conclusions:
Patients with osseointegration experienced less prosthesis-associated problems than socket prosthesis users and had a higher prosthesis-associated quality of life when assessed with the Q-TFA. General quality of life, as assessed with the EQ-5D-3L, was not different between groups.
Keywords
Background
Amputation of an extremity is a life-changing event for each patient and has a negative impact on their quality of life (QoL) due to physical barriers and psychological distress. 1 When discussing a patient’s QoL after an amputation, the reason for the amputation, the level of amputation, and physical and psychological conditions, as well as the patient’s comorbidities have to be taken into consideration. In Germany, trauma and tumours are the most common causes of transfemoral amputation (TFA) in adults aged younger than 60 years. 2 Vascular disease is the most common cause of TFA in older individuals and is often accompanied by several comorbidities. However, non-elderly adults with TFA are relatively healthy if the sudden loss of a limb is not taken into account. 3 Therefore, it is important to provide non-elderly persons with TFA the best available care in order to improve their outcomes.
The daily use of a prosthesis is closely related to an improvement in the QoL of patients. 4 In order to use the prosthesis for the whole day, it is important that the prosthesis fits the patient well and the residual limb is pain-free.1,5 If the socket does not fit well, walking is difficult, the risk of falling is increased, energy consumption is increased and QoL is reduced.4,6,7 Common side effects of socket prostheses (SPs) include pressure-related skin problems, hyperhidrosis, eczema, lymphedema, candidiasis, and pain while wearing the prosthesis.8,9 Long-term users of SPs are also likely to develop skin problems.10,11
A new treatment option for persons with TFA, osseointegration, became available in the 1990s. 12 Since then, different osseointegrated implants have been developed. 13 Currently, osseointegration is offered in approximately 17 facilities worldwide. 14 The exact description of the surgical procedure for osseointegrated prosthesis (OIP) implantation can be found elsewhere. 15 As osseointegration is performed in several hospitals in Germany, the exact number overall is unknown but is expected to be in the lower 100s.
This treatment option is especially useful for patients who have a very short residual femur or for those who have difficulties finding a socket that fits properly. 15 The reported advantages of osseointegration are osseoperception, better hip range of motion, increased mobility, and improved QoL.12,16–18
However, it remains unclear whether there is a difference in QoL between patients equipped with a conventional SP and those treated with an OIP. There is a need for studies that provide a broader overview of the available treatment options. Therefore, this study aimed to identify the differences in QoL between a cohort of patients treated with osseointegration and a control group of patients treated with SPs.
Methods
Participants
All participants provided written informed consent. Patients were recruited according to the following inclusion criteria: persons between ages 18 and 65 years with a TFA, sufficient language skills to be able to complete the questionnaires, and Medicare Classification Levels (K-levels) of at least 3 or 4. 19 Furthermore, participants had to be equipped with their current prosthesis (OIP or an SP) for at least 1 year and supplied with a microprocessor-controlled knee (MPK).
Exclusion criteria included any amputation distal to the transfemoral level, vascular or diabetic disease as a cause of the amputation, pregnancy, disabilities of the remaining leg, and pain while wearing the prosthesis. Transfemoral amputation level was measured using the residual limb ratio, which was measured through the residual limb length divided by the intact limb length.
Twenty-five patients who had successfully undergone osseointegration using the same OIP (ESKA Endo-Exo-system, ESKA Orthopaedic, Lübeck, Germany) and who matched our inclusion criteria were invited to participate (OI group). 15 22 of the 25 subjects agreed to participate. The mean time since osseointegration was 66.8 ± 42.4 months in the OI group. To achieve a cohort-matched control group, we recruited participants from a group of 178 patients who underwent TFA using a conventional SP from our institution’s database considering the following in order: exclusion criteria as mentioned above, age, body mass index (BMI), and K-level. Seventeen of 25 eligible patients equipped with an SP agreed to participate. Therefore, a total of 39 patients were recruited, of which 22 were equipped with an OIP and 17 with an SP.
Questionnaires
The Questionnaire for Persons with Transfemoral Amputation (Q-TFA) is a self-report questionnaire for non-elderly persons with TFA, containing 70 questions. In order to determine the current QoL status of a person with TFA, 54 of the 70 questions of the Q-TFA are used to calculate four scores reflecting prosthesis use, prosthetic mobility, prosthesis-related problems and global health. 20
Each score ranks from 0 to 100 points. The ‘Prosthetic Use’ score reflects the average duration the prosthesis is normally worn during a week. A score of 100 points is given if the prosthesis is used for more than 15 hours every day. The ‘Prosthetic Mobility’ score is an average of the subcategories ‘walking habits’, ‘use of walking aids’, and ‘capabilities with the prosthesis’. The ‘Problem score’ contains problems commonly described among patients with TFA. A score of 0 indicates the absence of problems, whereas a higher score indicates some sort of problem. The ‘Global score’ reflects the general current situation of a person with TFA with regard to their prosthesis. 12
The European Questionnaire 5-dimension, 3-level (EQ-5D-3L) is a widely used descriptive instrument in clinical studies to measure mental, physical and social QoL. 21 The first part is the EQ-5D-3L index, which contains the five dimensions: ‘mobility’, ‘self-care’, ‘usual-activities’, ‘pain/discomfort’ and ‘anxiety/depression’. Each dimension could be answered using one of the following levels: ‘no problems’, ‘some problems’ and ‘extreme problems’.
The EQ-5D-3L index combines the answers for all five dimensions and is calculated either through the ‘time trade-off value set’ (TTO-VS) or through the ‘visual analog scale value set’ (VAS-VS) method, which differ regarding the evaluation of the value sets. Since both evaluation methods are available in the German population, both were used. 22 The EQ-5D-3L index ranges from 0 to 1, with a higher score indicating a better health status. 23 The second part of the EQ-5D-3L consists of a 20-cm visual analog scale (EQ-VAS) where the patient is asked to state their current self-rated health status on a scale from ‘worst imaginable health state’ to ‘best imaginable health state’. 23 Surveys were administered by paper to the participants after they were equipped with their current prosthesis (OIP or a socket prosthesis) for at least 1 year.
Statistical analysis
Sample size calculation was based on published means and standard deviations of the ‘Global’ score of the Q-TFA.16,24,25 The standard deviation was calculated to be 24, and the effect size was assumed to be 24. The level of significance and power were set at α = 0.05 and 80%, respectively. Calculation of the minimum sample size was two-sided and resulted in 17 participants. To test for the presence of a normal distribution, the Shapiro–Wilk test was used. If data were normally distributed, the Student t test was used. In case of a significant deviation from the normal distribution, the Mann–Whitney U test was used. The chi-square test was used for categorical variables. Normally distributed data are presented as mean ± SD, while non-normally distributed data are presented as median and range. In addition, t-, W-, or χ2-statistics, and the degrees of freedom are included. The level of significance was set at α = 0.05. All data were analysed with SPSS Statistics version 25 (IBM Corp, Armonk, NY, USA).
Results
Regarding sex (χ2 = 0.225, df =1, p = 0.635), age (t = 0, df = 37, p = 0.609), body height (in cm) (t = 0, df = 37, p = 0.921), body weight (in kg) (W = 211, df = 37, p = 0.487), and BMI (t = 0, df = 37, p = 0.335), no statistically significant differences were found between groups (Table 1).
Demographic data and prosthetic components of the groups: relative frequencies, mean ± SD, and p values.
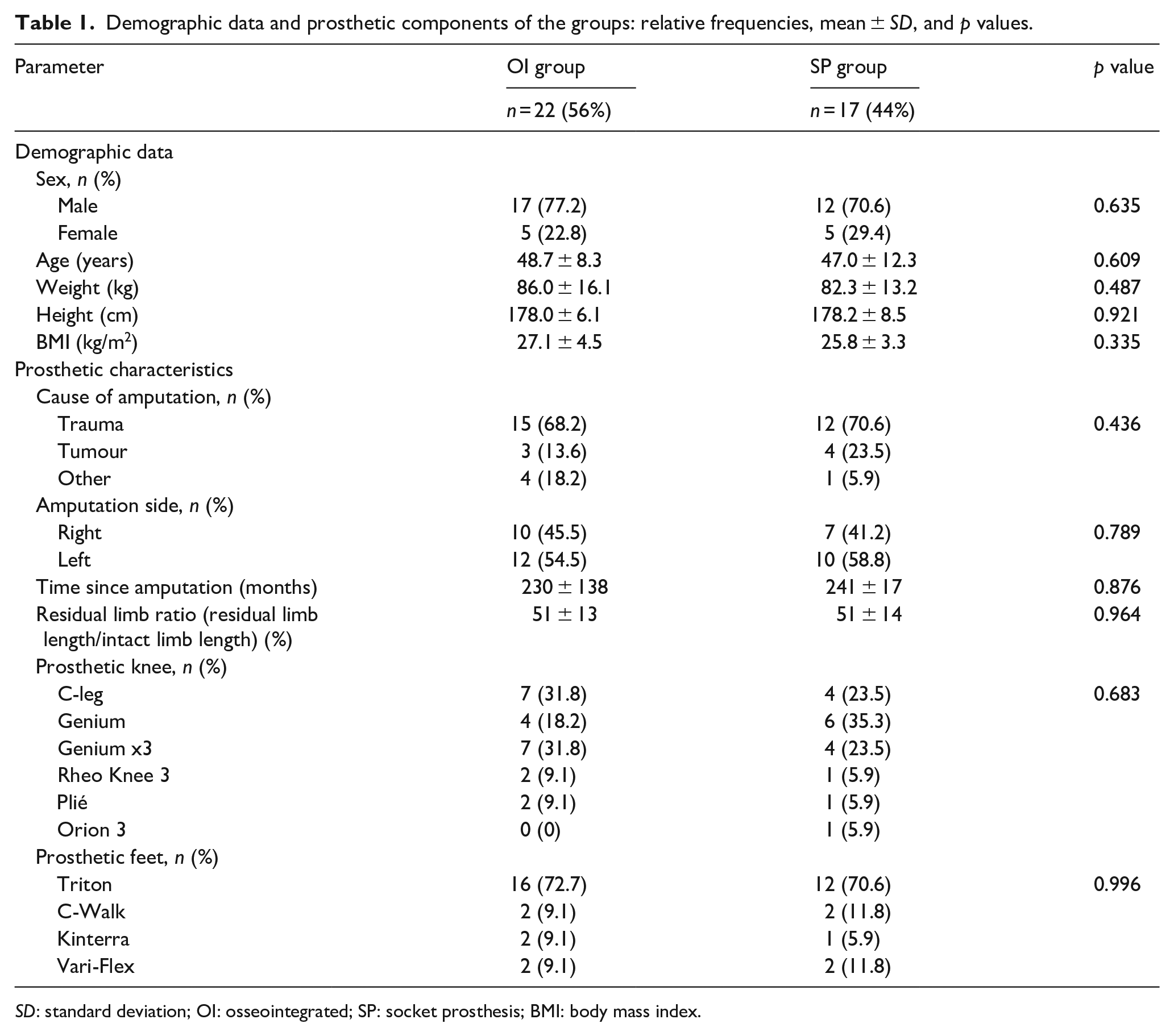
SD: standard deviation; OI: osseointegrated; SP: socket prosthesis; BMI: body mass index.
Regarding cause of amputation (χ2 = 1.662, df = 2, p = 0.436), amputation side (χ2 = 0.071, df = 1, p = 0.789), relative residual limb length (W = 88, df = 37, p = 0.964), time since amputation (W = 192, df = 37, p = 0.876), prosthetic knee (χ2 = 3.113, df = 5, p = 0.683), and prosthetic feet (χ2 = 0.268, df = 3, p = 0.996), no statistically significant differences were found between groups (Table 1).
The difference in the ‘Mobility’ score of the Q-TFA between the OI group and SP group were not statistically significant (W = 256, df = 3, p = 0.051; Table 2). The ‘Use’ score of the Q-TFA was not significantly different between the two groups (W = 235, df = 37, p = 0.146). The Q-TFA ‘Problem’ score suggested significantly fewer problems in the OI group as compared with the SP group (W = 56, df = 37, p < 0.001). The ‘Global’ score of the Q-TFA was significantly higher in the OI group than in the SP group (W = 266, df = 37, p = 0.022) (Table 2).
Questionnaires: mean ± SD, medians (min–max), degrees of freedom, W-statistics and p values.
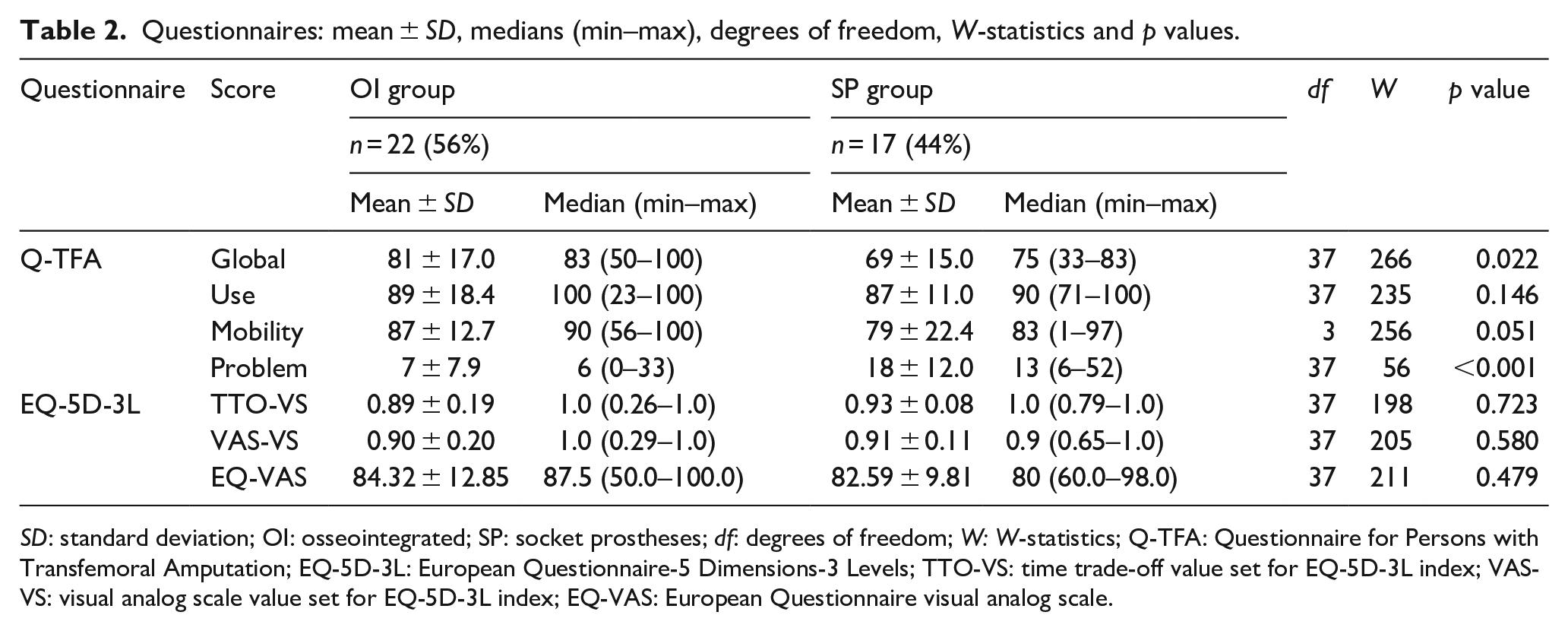
SD: standard deviation; OI: osseointegrated; SP: socket prostheses; df: degrees of freedom; W: W-statistics; Q-TFA: Questionnaire for Persons with Transfemoral Amputation; EQ-5D-3L: European Questionnaire-5 Dimensions-3 Levels; TTO-VS: time trade-off value set for EQ-5D-3L index; VAS-VS: visual analog scale value set for EQ-5D-3L index; EQ-VAS: European Questionnaire visual analog scale.
There were no statistical differences between the groups with regard to the results of the EQ-5D-3L (Table 2).
Discussion
In this study, the OI group reported a significantly lower rate of problems associated with the prosthesis compared with the SP group as indicated by the ‘Problems’ subscale of the Q-TFA. In addition, the OI group reported significantly higher scores than the SP group on the Q-TFA ‘Global’ score, indicating higher overall satisfaction. Several authors have shown similar results when using the Q-TFA to evaluate QoL before and after osseointegration of the prosthesis.12,16,24,26 Yet, it should be noted that these studies mostly involved patients with TFA who were no longer satisfied with the fit of a standard SP and wished for an improvement. This could be seen from the low preoperative baseline values. However, in our study, the controls were group-matched and were satisfied with their prosthetic components. In both the OI and SP groups, the ‘Mobility’ and ‘Use’ scores of the Q-TFA were higher than in other studies, maybe because our patients were more active and that use of the prosthesis did not restrict them.12,16,24,26 When comparing the results of the ‘Problem’ score of the Q-TFA in the SP group with results from other studies, only Hagberg et al. reported higher scores, whereas other authors reported slightly lower problem scores in the OI group.12,16,24,26
It should be noted that the Q-TFA ‘Problem’ score contains some questions that are only relevant to SP users. 18 Questions regarding the most commonly reported problems of SP users, such as skin irritations and sweating, are included in the ‘Problem’ score of the Q-TFA.7,18,20 The most common complication of osseointegration is the risk of infection of the stoma.26–28 As it seems to be a relevant prosthesis-associated problem, it is surprising that it is not included in the ‘Problem’ score of the Q-TFA. However, it should be pointed out that the Q-TFA was originally developed and validated for non-elderly patients with SPs. 20 Taking this into account, the Q-TFA ‘Problem’ score of the Q-TFA might not be a sufficient tool to measure problems associated with an OIP. Branemark et al. included two extra questions regarding problems specifically encountered in patients treated with osseointegration. Therefore, additional questions, such as issues with the stoma and complications with the bone anchorage, might be useful tools for gaining knowledge about prosthesis-associated QoL. 26 Another score previously used to estimate the QoL of persons with TFA treated with an OIP is the Short Form-36 Health Survey (SF-36). A prospective study by Branemark et al. 26 showed statistically significant improvements in physical functioning, role functioning and physical component scores after osseointegration. These findings are in agreement with the findings of the Q-TFA ‘Problem’ and ‘Use’ scores of the Q-TFA in our study.
In contrast to the Q-TFA, the EQ-5D-3L is a general measure of QoL. In our study, a statistically significant difference was not found between groups in the EQ-VAS or in the EQ-5D-3L index. This result contradicts the findings of the ‘Global’ score of the Q-TFA, which assigned the study group a higher global QoL. One possible explanation for these findings could be that almost all users of OIPs were not satisfied with the SP beforehand. Therefore, OIP users might overrate their prosthesis-associated QoL compared with SP users. This hypothesis is also supported by the findings of the EQ-5D-3L, as it showed no significant difference between groups with regard to general QoL. However, as the ‘Global’ score of the Q-TFA is a targeted measure, this could also explain our findings.
In a study by Giannoudis et al., 29 persons with transtibial amputation scored 66.6 points on the EQ-VAS. Cutti et al., 30 as well as Gerzeli et al., 31 determined the QoL of an active Italian TFA test sample equipped with an MPK using the EQ-5D-3L index and obtained values of 0.77 and 0.75, respectively. Our cohort of test subjects showed higher mean EQ-5D-3L scores, suggesting a better overall QoL. Sex- and age-independent norm values for the German population have a mean of 77.1 for the EQ-VAS, and 0.85 for the TTO-VS and 0.90 for the VAS-VS of the EQ-5D-3L index. 23 Surprisingly, our study cohort showed higher EQ-5D-3L values than that of the general German population in both groups. However, a comparison with the general population was not the aim of the investigation and will not be discussed further. Nevertheless, it is surprising that persons with TFA report such high scores concerning their QoL. Participants in both groups were highly active prostheses users, and all were equipped with modern prosthetic components such as MPK. Since all patients with an OIP are equipped with an MPK in Germany, the use of an MPK was chosen as an inclusion criterion. 15 Persons with TFA who use an MPK have been shown to benefit from higher mobility, increased gait safety, and a possible reduction in energy consumption. 32 Beyond that, none of the test subjects had an injury of the residual limb, which may have interfered with their mobility. Factors such as increased mobility and use of prosthesis have been shown to have a positive influence on QoL. 32 It appears that persons with TFA are especially sensitive to their QoL when it comes to their experienced mobility and limitations in mobility.26,33 According to Chen et al. 4 and Sinha et al., 34 the use of prostheses and the problems associated with the use of prostheses were the greatest influencing factors on the physical QoL.
Therefore, the Q-TFA is an important tool for reflecting specific aspects of the QoL of a person with TFA, especially regarding prosthesis use and prosthesis-associated problems. However, if it comes into question whether osseointegration generally results in better QoL, the use of the EQ-5D might be a suitable addition.
Limitations
Several limitations have to be taken into account when discussing this study. As the inclusion and exclusion criteria limited the representativeness of the cohort, the findings are not applicable to all persons with TFA. However, the inclusion and exclusion criteria were chosen with regard to the medical indications for OIP. 15 Participants used different types of MPK, which might have influenced the study results. Nevertheless, QoL does not seem to be influenced by the use of different types of MPK. 32 Therefore, our findings are applicable to healthy non-elderly persons with TFA not caused by vascular disease, and with high mobility. As our outcome measures were self-reported measurements, there is always the possibility of subjectivity. In addition, our sample size was relatively small. Further research with larger sample sizes is required to confirm our findings. With regard to statistics, there were many paired comparisons in this investigation and, subsequently, a greater risk for a type one error. Another limitation is the use of the EQ-5D-3L since the EuroQol Group has released the EQ-5D-5L, which has been reported to be more sensitive and likely to reduce ceiling effects because of its five, instead of three, response options. 35 Yet, various studies have used the EQ-5D-3L to assess the QoL of persons with TFA.29–31 In order to compare our findings with these previous results, the EQ-5D-3L was used.
Conclusions
Regarding different treatment options for persons with TFA, patients with osseointegration appeared to have a better prosthesis-associated QoL compared with a matched control group equipped with SPs considering the ‘Problems’ and ‘Global’ scores for the Q-TFA. QoL, as assessed with the EQ-5D, was not different between groups. In order to confirm these findings, further studies including larger samples are needed.
Footnotes
Author Contributions
The author(s) disclosed the following roles as contributors to this article: P.T.P., R.W., H.-H.A., and A.P.S. were responsible for conceptualization and validation; P.T.P., R.W. and A.P.S. were responsible for data curation; P.T.P. and R.W. were responsible for formal analysis; A.P.S. was responsible for funding acquisition, project administration and supervision; P.T.P. and A.P.S. were responsible for investigation; P.T.P., R.W., and A.P.S. were responsible for methodology; P.T.P., H.-H.A., and S.Z. were responsible for resources; R.W. was responsible for software; P.T.P. was responsible for visualization; P.T.P. and A.P.S. were responsible for writing – original draft, and writing – review & editing.
Ethics Review and Approval
The study was approved by the ethics committee of the University of Lübeck (file reference 16-161).
Declaration of Conflicting Interests
The author(s) disclosed no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed that they received no financial support for the research, authorship and/or publication of this article.