
Abstract
Objective: To evaluate the functional outcome of individuals with transfemoral and contralateral transtibial amputations secondary to peripheral vascular disease.
Methods: A retrospective chart review followed by phone interview. The primary outcome measures were the discharge 2-minute walk test, Frenchay Activities Index, and the Houghton Scale.
Results: There were 31 dysvascular individuals identified to have a combination of transfemoral/transtibial (TF/TT) amputation admitted to our institution for rehabilitation from February 1998 to June 2007. The mortality at follow up was 68%. There were eight surviving amputees. The average 2-minute walk test score was 31.9 m at the time of discharge from our inpatient program. Of these, the average Frenchay Activities Index was 15.3. The average Houghton Scale score for use of the transtibial prosthesis alone was 2.1. The average Houghton Scale score for use of both prostheses was 1.5. Comparisons between groups based on initial amputation level revealed a significant difference of being fitted with a transfemoral prosthesis. Those whom initially had a TT amputation were less likely to ultimately be fitted with a TF prosthesis (X 2 1,n=31 = 4.76, p < 0.05).
Conclusion: The overall functional outcome of individuals with a combination of TF/TT amputation due to dysvascular causes is poor. These individuals have a low level of ambulation, activity, and prosthetic use.
Introduction
Amputations of the lower extremity have been reported as high as 97% of all amputations.1 Vascular pathology is attributable in 82% of lower extremity amputations.1 The five-year survival rate for this patient population has been reported to be 35–45%,2-5 with Ebskov reporting a 28% five-year survival rate, in the largest study (21,520 amputations) that has looked at this issue.6 In general, it is thought that bilateral amputees are more likely to have advanced vascular disease and co-morbidities that leads to a high mortality rate. However, it has been postulated that bilateral amputees actually have a longer life expectancy possibly due to unilateral dysvascular amputees not living long enough to have a bilateral amputation.7 Amputations of the contra-lateral limb in dysvascular individuals have been reported to be 11–20%.2,, 8,, 9 Combined transtibial and transfemoral amputations account for 25–35% of patients that undergo bilateral amputations.10 Despite this large population of bilateral amputees, there is a paucity of literature truly evaluating functional outcome. Clinicians need information to help create appropriate rehabilitation goals for their dysvascular TF/TT amputation patients.
In assessing functional outcome; it is important to examine an individual's activity level, prosthetic use, and mobility. Pohjolainen et al. assessed 20 bilateral amputees, with a questionnaire to examine their activity level. Only three of their group were TF/TT amputees.11 Therefore, this study provided uncertain data regarding functional outcome in the TF/TT amputation group. Shin et al. assessed activity level by using the Frenchay Activities Index (FAI). This group was composed of 43 traumatic bilateral amputees, of whom 13 were TF/TT amputees. The average Frenchay Activities Index for the 13 TF/TT amputees was 17.6 out of a possible total score of 45.12
It has proven to be difficult to assess successful prosthetic use in TF/TT amputees, as many studies reviewed define ‘success' differently. Sakuma et al. studied 15 TF/TT amputees secondary to PVD to evaluate prosthetic usage. Prosthetic ambulation was defined as the ability to walk short distances and perform activities of daily living using their prostheses and an upper extremity gait aid alone. Of the 15 TF/TT patients, 33% were able to achieve prosthetic ambulation.13 Volpicelli et al. examined the ambulation capacity of 20 dysvascular TF/TT patients. Four were deemed to be prosthetically rehabilitated as defined by the ability to ambulate with concomitant use of the prosthesis and an upper extremity gait aid. Of these four, one achieved limited community ambulation and three remained household ambulators. Out of the remaining 20, 10 used a wheelchair for ambulation and six were bedridden.14 Shin described three who achieved community ambulation; six were household ambulators and four remained wheelchair bound.12 Hunter et al. used the classification of Hamilton and Nichols to assess prosthetic usage in their subgroup of 14 TF/TT amputation patients, of which 13 were dysvascular. Their data showed that five patients reached wheelchair independence, six used their prosthesis minimally, one had reasonable use of their device, and two patients maintained good general use of their prosthesis.15 It is uncertain if all theses subjects were fitted with bilateral prostheses.
Of the studies that evaluate functional outcomes, TF/TT amputation patients are uniformly grouped together with all individuals with bilateral amputations, limiting the ability to make specific claims on functional improvement in the TF/TT amputation population.11,, 16 The literature that is available is limited by non-standardized definitions of prosthetic use, and the use of functional outcome measures that have not been validated.
This study investigated three outcomes measures that have been shown to be valid and reliable in the amputee population. First, we assessed activity level using the FAI. Secondly, we assessed prosthetic use, as measured by the Houghton Scale. Lastly, functional exercise capacity, using the 2-minute walk test.
Methods
A retrospective chart review was conducted at West Park Healthcare Centre. All charts from February 1998 until June 2007 of individuals with a combination of TF/TT amputations due to peripheral vascular disease were reviewed. Demographic and prosthesis related data was collected. A telephone interview was conducted to obtain further information pertaining to prosthetic use and the FAI, on average 2.99 years since the date of the second amputation. This study was approved by the Joint Bridgepoint-West Park Research Ethics board.
The three functional outcomes examined were activity level, mobility, and prosthetic use. Firstly, to assess activity level, the FAI was used (see Appendix 1). The FAI is composed of 15 items which measures participation in activities within and outside the home. The score is a cumulative score ranging from 0 (never) to 45 (very high participation). The scale depends on an individual's own report. This index has been shown to be reliable and valid for the amputee population.17 Secondly, mobility was assessed at the time of discharge from the rehabilitation hospital by the 2-minute walk test (2MWT). Obtaining a functional level of independence in self care and use of the prostheses is the goal for discharge from the rehabilitation hospital. The 2MWT assesses the distance an individual is able to ambulate in 2 minutes at their own self-selected speed. The 2MWT has been shown to be valid in the amputee population.18 Lastly, prosthetic usage was determined by the modified Houghton Scale (Appendix 2). The modified Houghton Scale is a three- question scale that uses a patient's self-report of lower extremity prosthetic use. This scale was shown to have good reliability and validity.19 The modified Houghton Scale has a maximum score of 9; with a higher score indicating higher performance. Two Houghton Scores were recorded; one for use of the transtibial prosthesis, and one for the use of the transfemoral prosthesis. In our opinion, if an individual was able to ambulate with both prostheses on a consistent basis, they were deemed to be successful. The FAI and Houghton Scale were obtained through the telephone interview.
Chi-square analysis was carried out to detect statistical significance between groups within the sample. Two by two contingency tables were used to assess if the following variables were correlated with receiving a transfemoral prosthesis; level of initial amputation (transtibial vs. transfemoral), age (older than vs. less than 65), and number of co-morbidities (greater than vs. less than four). A co-morbidity is considered a chronic medical diagnosis. A history of a deep vein thrombosis and/or pulmonary embolism was also considered a co-morbidity. The age of 65 and four co-morbidities was arbitrarily established. A multivariate analysis is used to assess correlations, however, was inappropriate in this study due to the small sample size.
Results
Subject demographics
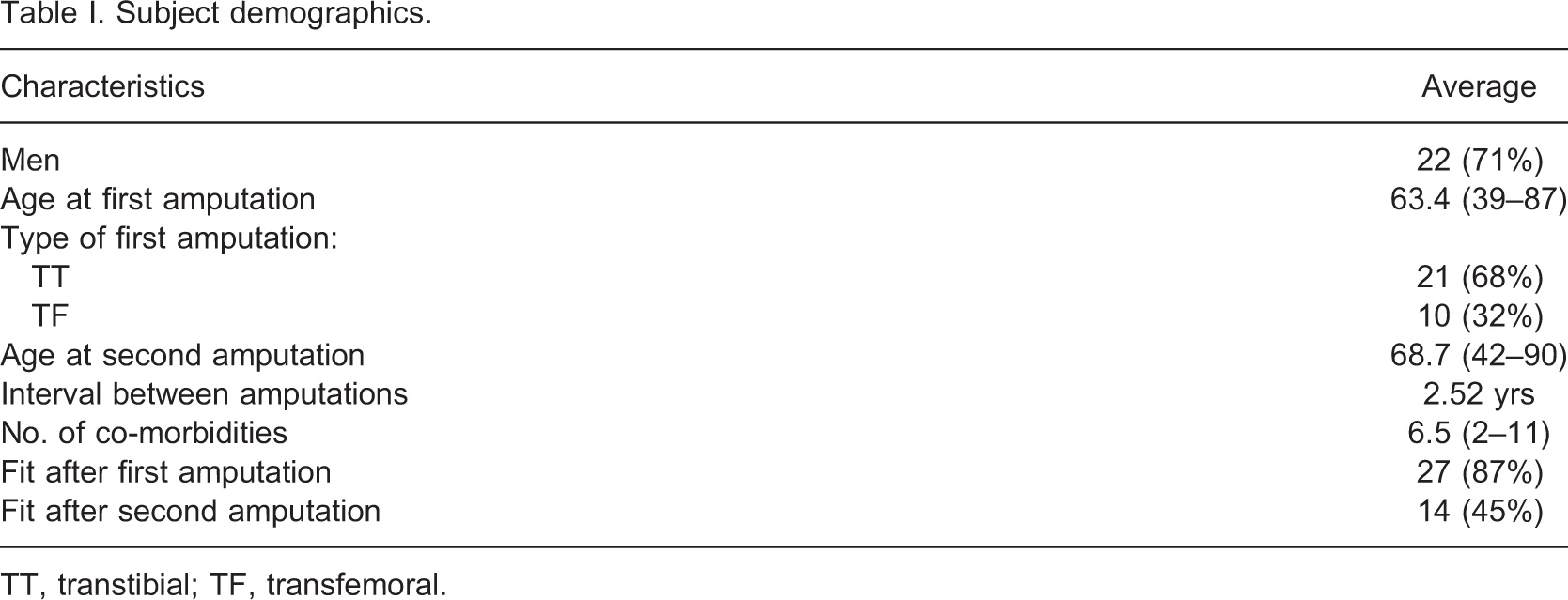
TT, transtibial; TF, transfemoral.
The contact information for 10 individuals was invalid. Eight individuals had not been seen for greater than five years at our institution. Two individuals were last seen three years ago. We were able to contact the family physician for four of these individuals; the last visit to the family physician correlated with the last visit to our institution. Due to the extensive co-morbidities in these individuals and lack of follow-up, it was presumed these individuals had died. By the time of the telephone interview, 67.7% of the sample had died.
Eight interviews were completed. One interview was taken through a family member, since the subject had severe cognitive decline and was unable to complete the interview. This family member was unable to answer the FAI, hence this data was not included.
The average interval between the amputations was 2.52 years, with a range of 45 days to 12 years. The sequence the individuals were fitted with a prosthesis is displayed in Figure 1.
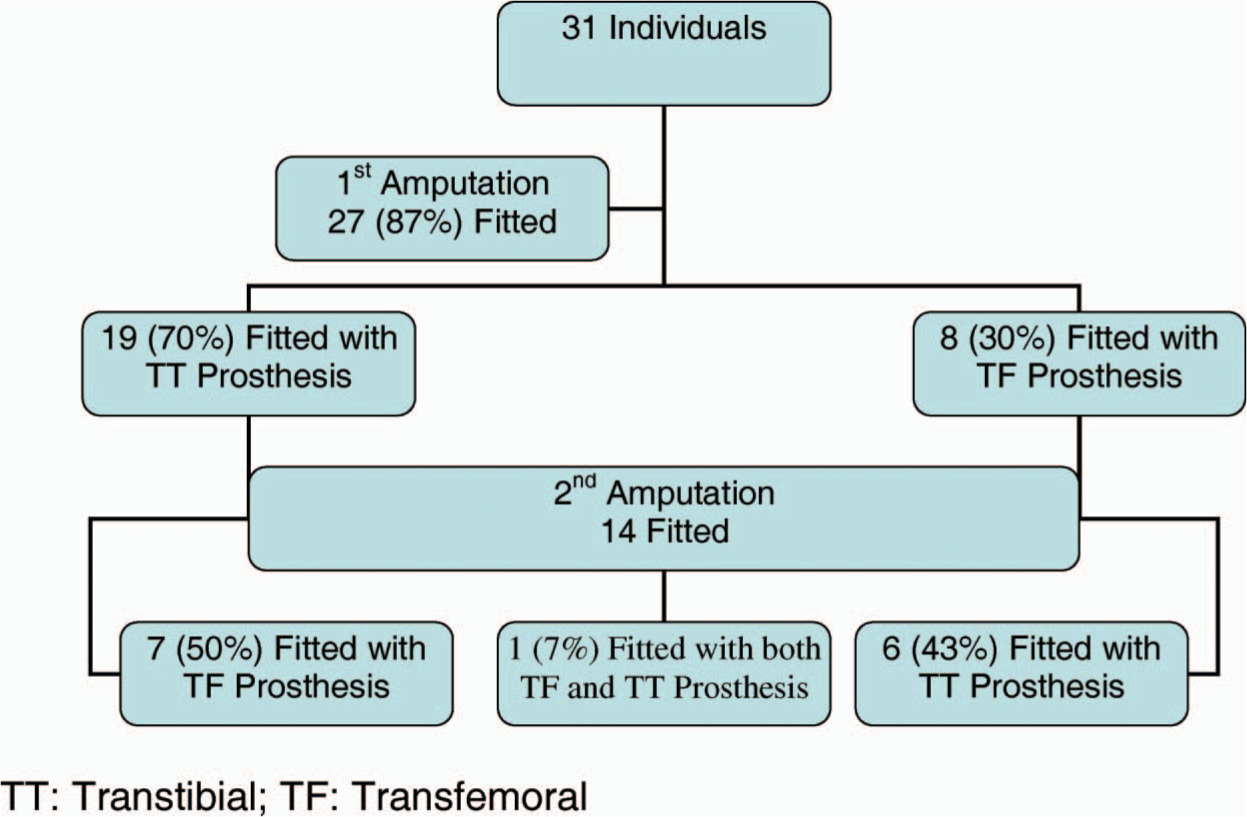
Sequence of being fitted with a prosthesis. TT, transtibial; TF: transfemoral.
Of the 31 individuals, the discharge 2-minute walk test was not applicable for 17 (54%) individuals, since they were either not fitted with a prosthesis or fitted with only one. We had incomplete data for three individuals. Four were unable to complete the test (13%). The average of the remaining seven individuals was 31.9 m, with a range of 15.1–56.5 m. The average length of stay in hospital from the date of the second amputation until discharge from rehabilitation in these patients was 55.8 days, with a range of 33–83 days.
We were able to obtain follow up information on eight cases. Of these; three did not use any prosthesis; one only used the TT prosthesis; three mostly used the TT prosthesis and occasionally the TF device; one used both TT/TF prostheses. Of the four who were able to ambulate with both TF/TT, three used a walker/rollater and one used crutches. The average Houghton scale score for use of a TT prosthesis was 2.1. The average Houghton score for use of a TF was 1.5. It must be noted when individuals used a TF prosthesis there was congruent use of the TT prosthesis. Hence, the Houghton Score for use of a TF could also be used for combined use of a TF and TT. Only one (13%) out of the eight that were followed up achieved successful use of both the TF and TT prostheses. The average FAI was 15.3.
The current living situation of those who were interviewed for five people was their private residence. The remaining three were residing in a long term care institution.
There was a significant difference between the initial TT and TF group of whether they were fitted with a transfemoral prosthesis (X 2 1,n=31 = 4.76, p < 0.05). If the initial amputation was a TT, they were less likely to ultimately be fitted with a TF prosthesis. The age at first and second amputation did not have a significant effect on being fitted with a prosthesis. Individuals with more than four co-morbidities had a propensity to not be fitted with a transfemoral prosthesis.
Discussion
The purpose of this study was to evaluate the functional outcomes of individuals with a combination of transfemoral and transtibial amputation due to a dysvascular etiology. The small sample size at follow-up due to the high level of mortality in these patients is comparable to other studies.10,, 13,, 20 We did assume 10 deaths, since we were unable to contact these individuals. Attempts were made to confirm that these 10 individuals had died, however, these attempts failed. Given the invalid contact information, the extensive list of co-morbidities, and lack of follow up for greater than three years, either at our institution or with their family physician, we assumed it to be safe to presume these individuals were deceased. Only eight surviving individuals were available to obtain information on activity levels and prosthetic use.
As expected, our average FAI score of 15.3 is lower than those reported for elderly individuals and unilateral dysvascular amputees. Schuling et al. reported a mean FAI of 40.86 out of 60 in a group of 216 elderly controls.21 They did begin their scoring in each of the categories with a ‘1 = never’, hence the possible scores for the FAI could range from 15 (never) to 60 (very good participation). Miller et al. had a group of 34 unilateral dysvascular amputees with a mean FAI of 25.8 out of a score of 45.17
The average FAI in our group is slightly lower than the average reported by Shin et al. of 17.6 for the TF/TT amputation group.12 However, most of the individuals in their study had amputations due to trauma. They did report a lower FAI for the dysvascular subjects compared to the non-dysvascular. The authors also reported there may have been a selection bias, as 16 of the amputees that were excluded from their study were mostly dysvascular amputees with the combination of TF/TT amputations. The average of the FAI in a study done by Datta et al. on 21 bilateral amputees was 11.7.22 However, this sample consisted of TF/TF and TT/TT amputees. It has been suggested that there may be a gender bias to the FAI as women tend to dominate in household chores and men in outdoor activities. Our sample, who we could interview, was composed entirely of men, and this may have an effect on the FAI average reported in this study. Overall, the FAI indicates a low level of activity in the TF/TT amputation population compared to normal individuals and unilateral amputees.
The definitions for successful prosthetic use vary in the literature. We used the Houghton scale score, and the individuals' ability to ambulate with both prostheses on a consistent basis. With this definition only 1 (13%) was deemed successful. If we used the same definition as Sakuma and Volipicelli, such that successful prosthetic usage is determined by the individual being able to ambulate short distances with the prostheses, then we would have a 50% success rate. However, even though these individuals are able to ambulate with bilateral prostheses, as they tend not to use both prostheses in their daily lives, we do not consider this a successful outcome. Our low rate of successful prosthetic use compared to other studies12-15 might also be explained by the exclusively dysvascular etiology of the amputations.
The discharge 2 MWT value of 31.9 m implies a low level of functional ambulation. In order to cross a traffic light one must be able to walk 1.2 m/sec. Our sample would not be able to cross a traffic light since they would be ambulating only 22% of the speed required. Even the fastest individual in our sample who had a 2MWT distance of 56.5 m would not be able to accomplish this task.
This group was sub-divided into type of first amputation to determine if there was any correlation with being fitted with a prosthesis. We had 27 individuals fitted after the first amputation, of whom 19 were initially TT level, and this number decreased to 14 being fitted after the second amputation. This decrease in the number of individuals being fitted after the second amputation is consistent with other studies. Wolfe et al. had a subgroup of 3 TF/TT amputation individuals, of which two were fitted after the first amputation and none were fitted after the second amputation.23 Sakuma et al. had 10 TF/TT amputees that were fitted after the first amputation, however after the second amputation only five were fitted.13 They did not find any difference between the groups based on whether their first amputation was a TF or TT. In our study, we found a difference between the groups based on initial level of amputation and being fitted with a transfemoral prosthesis. If the initial amputation was a transtibial amputation, these individuals were less likely to ultimately be fitted with a transfemoral prosthesis, compared to the group whose first amputation was at the transfemoral level. Since use of a TF prosthesis has a higher energy demand than a TT prosthesis, it may be speculated if they initially have a TF amputation they may have the energy reserve to use a TF prosthesis. However, if they already have a TT amputation, at the time of their contralateral TF amputation, their energy reserve may be too low to tolerate a TF prosthesis for ambulation. Due to the small numbers in this study we were unable to further quantify the characteristics of the individuals who were able to tolerate the use of both TF and TT prostheses. This would be recommended for future studies to aid practioners in identifying which individuals should be considered for a TF prosthesis.
The main limitation to this study is the sample size. We did presume 10 individuals to be deceased; however, we do not have any confirmatory reports of the deaths. Hence, it is possible these subjects were still alive. The high mortality in this population leads to a small sample size at the time of follow-up. It was not acceptable to do extensive statistical testing based on the small number of follow-up cases. Based on this small sample size, this study is primarily a descriptive study. However, the high mortality is also an element of the poor outcome in these individuals. It should also be noted that our study group only included those thought suitable for rehabilitation after their second amputation, and thus there is a selection bias present. There are limitations in data collection due to the retrospective nature of the study design. Another limitation in this study is that we were missing data that was instrumental to our main outcomes that should have been recorded, however was not available. Future research should be prospective multicenter studies. This will limit missing data and increase the sample size.
Conclusion
This study has solely evaluated the dysvascular TF/TT amputation population to assess their functional outcomes. We have shown that the outcome of these individuals is poor as measured by the mortality, low level of activity, prosthetic use and ambulation.
Footnotes
Appendix 1
The Frenchay Activities Index
Item
Code
In the last 3 months
1. Preparing main meals
0 = never
2. Washing up
1 = <1 time per week
2 = 1–2 times per week
3 = most days
3. Washing clothes
0 = never
4. Light housework
1 = 1–2 times in 3 months
5. Heavy housework
2 = 3–12 times in 3 months
6. Local shopping
3 = ≥1 time per week
7. Social outings
8. Walking outside > 15 minutes
9. Actively pursuing hobby
10. Driving car/bus travel
In the last 6 months
11. Outings/car rides
0 = never
1 = 1–2 times in 6 months
2 = 3–12 times in 6 months
3 = ≥1 time per week
12. Gardening
0 = never
13. Household/car maintenance
1 = light
2 = moderate
3 = all necessary
14. Reading books
0 = none
1 = 1 in 6 months
2 = <1 in 2 weeks
3 = >1 in 2 weeks
15. Gainful work
0 = none
1 = <10 hours/week
2 = 10–30 hours/week
3 = >30 hours/week
Appendix 2
Houghton Scale Questions
1. Do you wear your prosthesis:
0 – Less than 25% of waking hours (1–3 hours)
1 – Between 25% and 50% of waking hours (4–8 hours)
2 – More than 50% of waking hours (more than 8 hours)
3 – All waking hours (12–16 hours)
2. Do you use your prosthesis to walk:
0 – Just when visiting the doctor or limb-fitting center
1 – At home but not to go outside
2 – Outside the home on occasion
3 – Inside and outside all the time
3. When going outside wearing your prosthesis, do you:
0 – Use a wheelchair
1 – Use two crutches, two canes, or a walker
2 – Use one cane
3 – Use nothing