
Abstract
This is the first report on prospective outcome for individuals treated with bone-anchored trans-femoral amputation prostheses (OI-prostheses) using the method of osseointegration. The aim was to analyze general and condition-specific health related quality of life (HRQL) at 2-year follow-up as compared to the preoperative situation. The study population consists of the first 18 consecutively treated patients (8 male/10 female, mean age 45 years) in a clinical investigation with amputations mainly caused by trauma and tumour. At inclusion the mean time since the amputation was 15 years (10 months – 33 years). Two self-report questionnaires were answered preoperatively and at follow-up: the SF-36 Health Survey (SF-36) and the Questionnaire for persons with a Transfemoral Amputation (Q-TFA). At follow-up 17/18 patients used the OI-prosthesis; one did not due to pain and loosening of the implant. Four of the scales of the SF-36 (Physical Functioning, Role Functioning Physical, Bodily Pain and Physical Component Score) and all four scores of Q-TFA (Prosthetic Use, Prosthetic Mobility, Problems and Global Health) were statistically significantly improved at follow-up showing superior general physical HRQL, increased prosthetic use, better prosthetic mobility, fewer problems and a better global amputation situation. Thus, osseointegrated prostheses represent a promising development in the rehabilitation of individuals with transfemoral amputation and increase their quality of life.
Introduction
Following lower limb amputation (LLA) quality of life is highly related to the ability to use a prosthetic limb (Pernot et al. 2000). The conventional way to attach a prosthetic limb to the body is with a socket (Kapp 1999). Discomfort and other problems related to the fit of the socket are common and have been shown to negatively affect quality of life and mobility (Hoaglund et al. 1983; Legro et al. 1999; Dillingham et al. 2001; Hagberg and Branemark 2001; Pezzin et al. 2004). A specific subgroup with LLA is the group of non-elderly persons having had an amputation for reasons other than vascular disease with or without diabetes mellitus. This group is a clear minority, but constitutes a substantial portion of those with limb loss due to trauma or tumour and contrary to the dysvascular cases, this group has long life expectancy (Ebskov 1994; Pohjolainen and Alaranta 1998; Dillingham et al. 2002). It has been stated that among US war veterans, a substantial portion could not use the prostheses adequately and that “there are significant problems with current methods for attaching prostheses that need to be addressed” (Sherman 1999). A new way to attach prostheses is via bone-anchorage to the residual bone. Treatment with bone-anchored prostheses (OI-prostheses) using the method of osseointegration has been performed in Sweden since 1990 (Branemark et al. 2001) and more recently also in United Kingdom (Sullivan et al. 2003; Robinson et al. 2004). Osseointegration means that there is a direct anchorage of an implant, made of pure of titanium, “by the formation of bony tissue around it without growth of fibrous tissue at the bone-implant interface” (Dorland and Anderson 2003). The concept of osseointegration has been in clinical practice for dental applications since 1965 (Brånemark et al. 1977).
The decision on patient selection for treatment with an OI-prosthesis is taken by an expert team of professionals and is based on both medical and physical examinations including, for instance, computerized tomography of the residual bone and analyses of the perceived problems to use a socket prosthesis. In 1999 a prospective clinical investigation named OPRA (Ossseointegrated Prostheses for the Rehabilitation of Amputees) was started at the Sahlgrenska University Hospital in Göteborg, Sweden on patients having a trans-femoral amputation (TFA). In accordance with the OPRA protocol, patients are treated with two surgical sessions followed by rehabilitation, with a total treatment period of approximately 12 months. At the first surgery (S1), a titanium implant (fixture) is inserted in the residual bone and left unloaded for about six months. At the second surgery (S2) a titanium rod (abutment) is inserted into the distal end of the fixture and is then penetrating the skin (Figures 1 and 2). After S2 the patient undergoes a period of rehabilitation for about six months with gradually increased weight-bearing and prosthetic activity (Hagberg 2005). The OPRA protocol includes a wide range of assessments performed prior to S1 and at defined time points after S2 until 2-year follow-up; e.g. radiography, registration of complications, hip range of motion, energy cost while walking, computerized gait analyses as well as general and specific health related quality of life (HRQL) measurements.
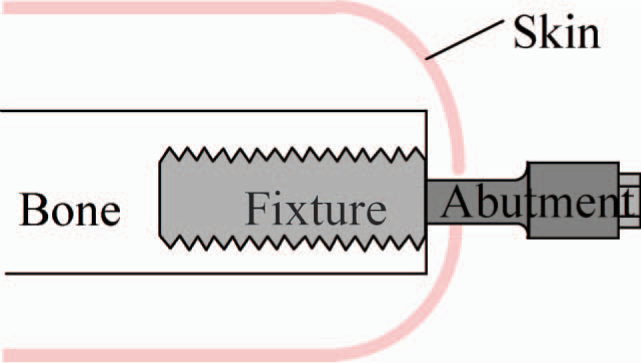
Schematic view of the implant system.
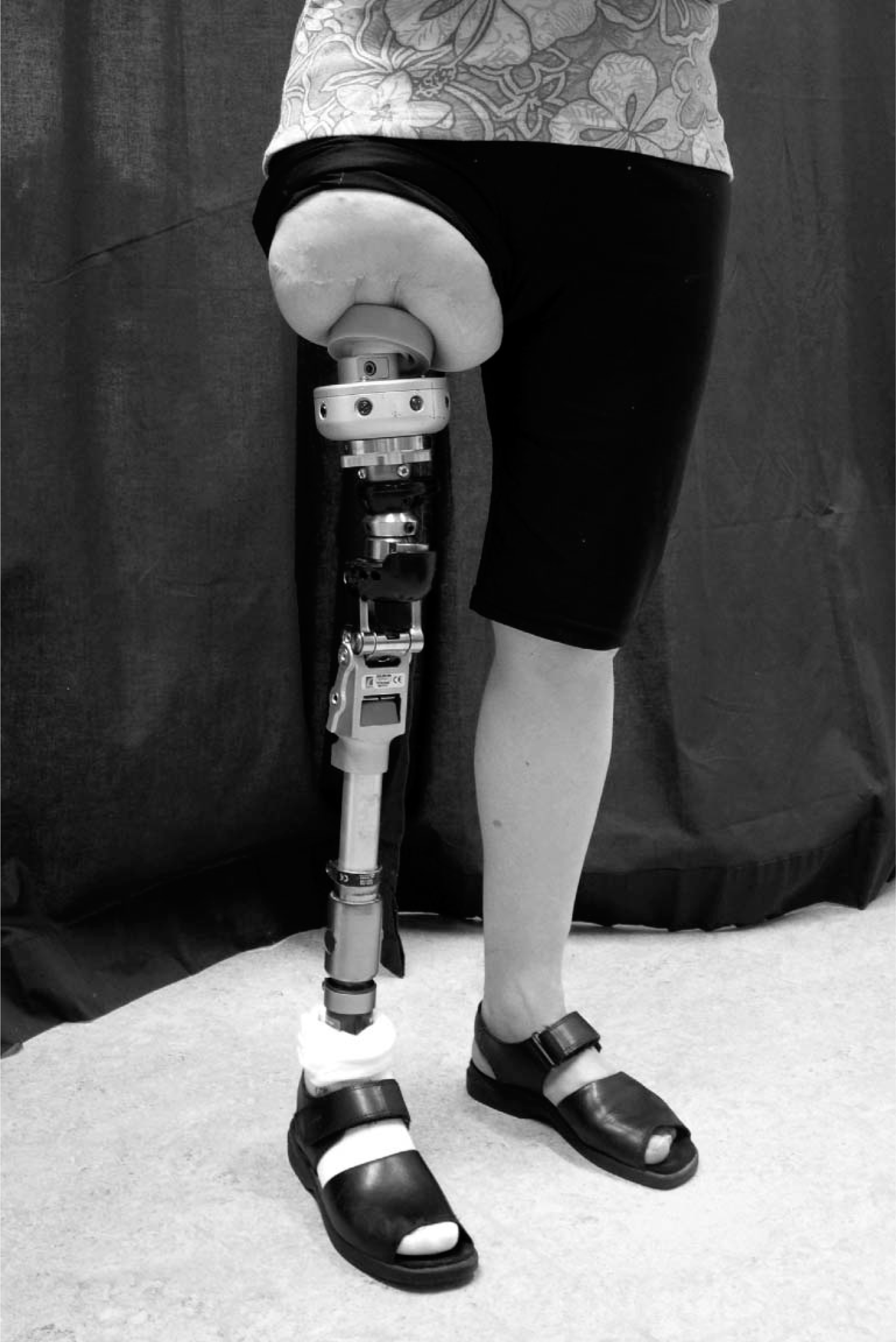
Patient with an OI-prosthesis.
The concept of HRQL refers to those aspects of quality of life that could be supposed to be affected directly by a health condition and reflects the perception of the individual of his or her degree of physical, psychological and social well-being (Fayers and David 2000; Patrick and Chiang 2000; Beaton and Schemitsch 2003). There are two main types of HRQL measures; generic measures and disease- or condition-specific measures (Fayers and David 2000). The generic tool reflects a broader perspective and could be used on healthy persons as well as on persons with different kinds of health problems which render comparisons between different groups. The condition-specific tool is made for a targeted group of patients or conditions and gives a more detailed perspective of HRQL. In studies of health outcome the advice is to use both kinds of measures to best capture the overall situation and change in health (Beaton et al. 1997; Hays et al. 2002; Beaton and Schemitsch 2003).
The aim of the study was to present outcome of general and condition-specific HRQL for the first 18 individuals included in the Swedish OPRA study at 2-year follow-up.
Material and method
Study population and procedure
Inclusion criteria for the OPRA study are: TFA with problems using a conventional socket prosthesis, completed maturation of the skeleton as well as normal skeletal anatomy, age below 70 years and to be suitable for surgery based upon the medical and physical examinations. Exclusion criteria are: severe peripheral vascular disease with or without diabetes mellitus, treatment with specific drugs (e.g. chemotherapy, corticosteroids), excessive body weight (around 100 kg) and pregnancy.
The current report includes the first 18 consecutive patients (8 male, 10 female) treated with surgery S1 during the period May 1999 to October 2003 and S2 from February 2000 to April 2004. Sixteen had unilateral TFA (11 right, 5 left) and two had bilateral TFA. One of the patients having bilateral amputations was successfully treated with an OI-prosthesis on the contralateral limb in 1998, prior to the present study. The other patient could not be supplied with a prosthetic socket nor be treated with an OI-prosthesis on the contralateral side due to extreme shortness of the residual femur. The cause of amputation was in 12 cases trauma, 5 tumour and 1 arterial embolus. Mean age at the time of the amputation was 31 years (14 – 60). At study inclusion (S1) the mean age was 45 years (22 – 62) with a mean time since the amputation of 15 years (10 months–33 years). The patients had a mean height of 171 cm (155 – 194 cm) and a mean weight of 77 kg (47 – 115 kg). Three of the 18 patients were not prosthetic users preoperatively (a prosthetic user was defined as a person who wears a prosthesis at least once a week (Grise et al. 1993)). Two of the non-users had been supplied with several prosthetic sockets but no one that resulted in an adequate fit resulting in prosthetic use and one had never tried an artificial limb. Of the 15 prosthetic users 13 had a prosthetic socket suspended with vacuum and two had a silicon liner. At inclusion, 11 were working, one was sick-listed and 6 had permanent disability pension.
The patients answered two self-report questionnaires prior to S1 and two years after S2; the time between the assessments was thus 2.5 years. The OPRA study is approved by the Human Research Ethics Committee at the Sahlgrenska Academy, Göteborg University, Sweden and all patients received oral and written information and gave their written informed consent before inclusion. All the patients invited to take part in the study agreed to be included.
Questionnaires
In the OPRA study two self-report questionnaires are used; the SF-36 Health Survey (SF-36) (Ware and Sherbourne 1992) for evaluation of general HRQL and the Questionnaire for persons with a Transfemoral Amputation (Q-TFA) (Hagberg et al. 2004) for the condition specific assessment.
SF-36 is a widespread generic measure with documented validity and reliability (Ware and Sherbourne 1992; Beaton et al. 1997; Andresen and Meyers 2000). The results are presented in eight separate scales each one representing different dimensions of HRQL; Physical Functioning (PF), Role functioning from a Physical Perspective (RP), Bodily Pain (BP), General Health (GH), Vitality (VT), Social Functioning (SF), Role functioning from an Emotional perspective (RE) and Mental Health (MH). Each scale can take a value between 0 and 100 and a higher figure represents better health. By using an algorithm the results from the eight scales can also be presented in two summary measures; the Physical Component Score (PCS) and the Mental Component Score (MCS) (Ware et al. 1995) in which the results are standardized to the general population with a mean score of 50 and a standard deviation (SD) of 10. The SF-36 is the most commonly used patient-based measure within orthopaedic research (Beaton and Schemitsch 2003) and has previously been used in studies on individuals with amputations and following limb sparing surgery (Smith et al. 1995; Dagum et al. 1999; Davis et al. 1999; Legro et al. 1999; Pezzin et al. 2000; Hagberg and Branemark 2001; Hoogendoorn and van der Werken 2001; Malo et al. 2001; van der Schans et al. 2002; Dougherty 2003). The validated Swedish version of the instrument was used (Sullivan et al. 1994).
The Q-TFA is a condition specific outcome measure that reflects current prosthetic use, mobility, problems and global health (Hagberg et al. 2004). Primarily designed for non-elderly persons using trans-femoral prostheses, the Q-TFA was also developed to study outcome when changing from socket prostheses to OI-prostheses. Initial validity and reliability have been established on 156 individuals using socket prostheses in Sweden. The results of Q-TFA are presented in four scores; Prosthetic Use score (2 items), Prosthetic Mobility score (19 items), Problem score (30 items) and Global score (3 items) each one ranging from 0 – 100. A Prosthetic Use score of 100 score points means that the prosthesis is worn for more than 15 hours daily. The Mobility score constitutes the average of three sub-scores (each 0 – 100); use of walking aids (Walking-aid sub-score, 2 items), prosthetic capability (Capability sub-score, 12 items) and walking habits outdoors (Walking habit sub-score, 5 items). The Problem score consists of 30 questions to assess the extent of perceived problems related to the amputation and the prosthesis and their impact on the quality of life during the last four weeks. The score is reversed which means that a higher figure indicates more problems with a larger reduction of quality of life and a lower score reflects a better situation with less reduction of quality of life. The Global score addresses the general perception of function and problems with the current prosthesis and the perception of the current overall situation related to the amputation. For individuals not using a prosthesis the only results of Q-TFA that can be registered and compared are the Prosthetic Use score and the single overall question of the Global score asking “How would you summarize your overall situation as an amputee?” with five response alternatives; extremely poor, poor, average, good or extremely good.
For statistical analyses of differences between the pre- and postoperative situation the Wilcoxon's non-parametric test was used except for analysis of the reported overall situation in the single question of the Global score for which the sign test was used. All tests were two-tailed and statistical significance level was set to p < 0.05.
Results
Seventeen of the 18 patients were using the OI-prosthesis and ambulated with unrestricted weight-bearing at 2-year follow-up. One patient could not use the bone-anchored prosthesis due to severe pain and was later shown to have loosening of the implant. At follow-up, 10 patients were working, 3 were retired by age, 4 had permanent disability pension and 1 was sick listed. For seven of the patients the employment situation was changed between the assessments (3 changed from disability pension to retirement by age, 1 changed from sick listed to work, 1 increased the amount of working hours, 1 changed from work to sick listed and 1 changed from work to disability pension). Demographic data for each individual is shown in Table I.
Patient data with results of the scores of Q-TFA
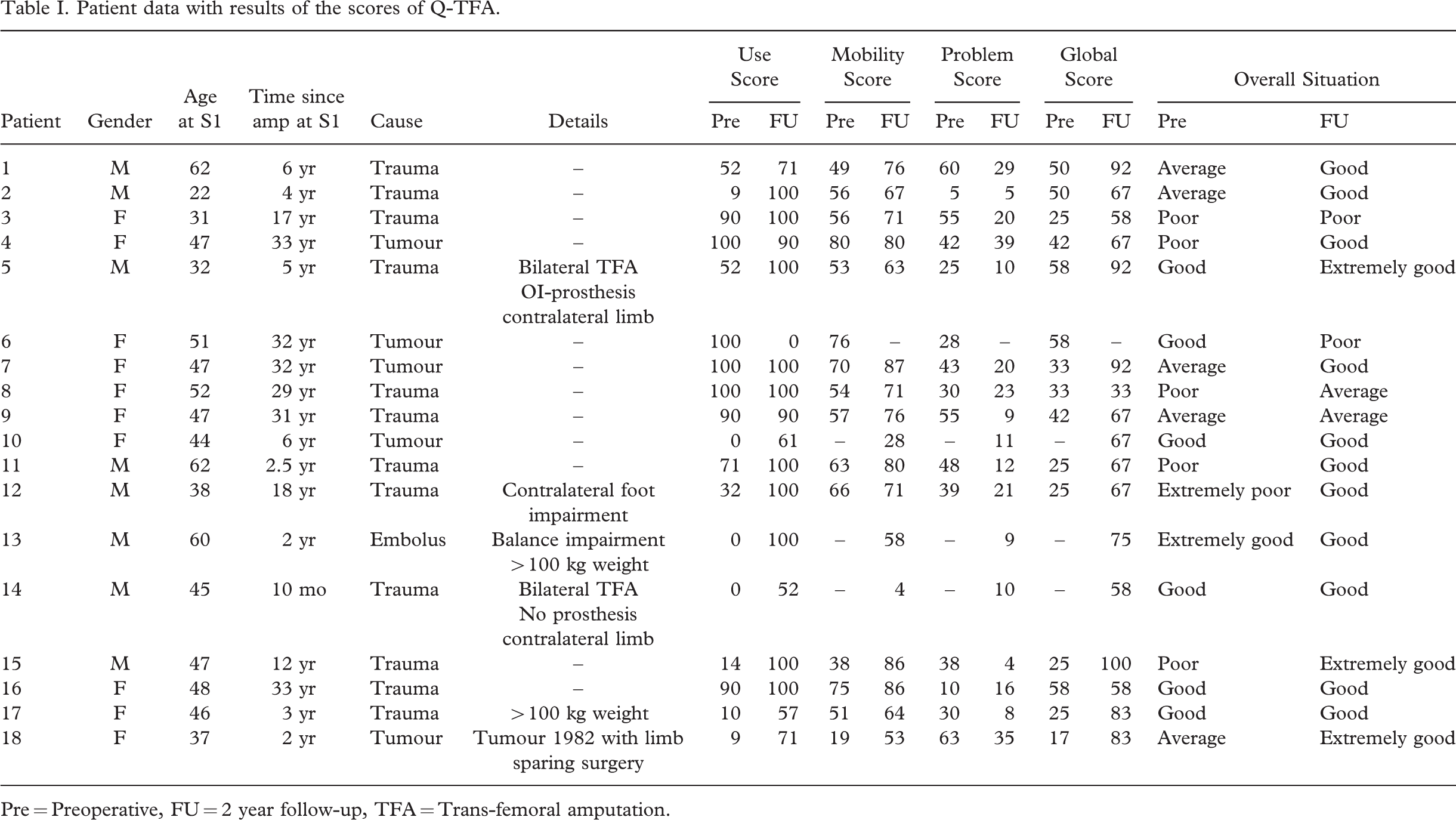
Pre = Preoperative, FU = 2 year follow-up, TFA = Trans-femoral amputation.
SF-36
The prospective results of the SF-36 are presented for the 17 cases that were using the OI-prosthesis at the 2-year follow-up. Statistically significant improvements were observed in three scales (PF p = 0.001, RP p = 0.003 and BP p = 0.029) and the Physical Component Score (p = 0.001). No other score was statistically significantly different between the assessments.
Q-TFA
All four scores of Q-TFA were improved at follow-up (Figure 4A–4D). Results for each patient and their answer to the global overall question are shown in Table I. The Use score (n = 18) was improved by a mean of 32 score points (p = 0.013). At follow-up 16 patients reported daily prosthetic use (nine > 15 hours/day, three 13 – 15 hours/day, four < 12 hours/day), one reported to use the prosthesis for six days a week (10 – 12 hours/day) and one patient reported no prosthetic use (Table I, patient 6 with pain and implant loosening). Preoperatively 5/15 prosthetic users reported that they had to refrain from wearing their socket prosthesis due to bad fit, skin problems or phantom limb pain during the last three months (1 for one day, 1 for 4 – 7 days, 2 for 8 – 15 days, 2 for >15 days). At follow up 6/17 prosthetic users reported that they had been forced to abstain the OI-prosthesis: 4 for 1 – 3 days (1 because of pain when loading the prosthesis, 1 had fallen with subsequent pain, 2 due to a superficial infection at the skin penetration area) and 2 for 4 – 7 days (1 had broken prosthetic components, 1 had phantom limb pain and pain in stump muscles). The mean improvement in the Mobility score, Problem score and Global score (n = 14, all individuals being a prosthetic user pre- as well as postoperative) were 17 (p = 0.001), 21 (p = 0.002) and 36 (p = 0.002) score points respectively. Within the Mobility score the mean Walking-aid sub-score improved from 70 to 76 points (p = 0.168), the mean Capability sub-score from 60 to 88 points (p = 0.001) and the mean Walking habit sub-score from 39 to 57 points (p = 0.013). At 2-year follow-up the overall situation, as reported in the single question of the Global score, was improved (p = 0.039) (Table I).
Discussion
Treatment with TFA bone-anchored amputation prostheses has been performed in Sweden since 1990 and preliminary results have been reported (Brånemark et al. 1997; Robinson et al. 2004; Ward and Robinson 2005) but few original articles presenting outcome of such treatment have been published (Sullivan et al. 2003; Hagberg et al. 2005). There was a clinical development period of almost 10 years before the OPRA study started; this was critical in order to standardize the procedures of the treatment. The selection of patients is crucial and for this reason the inclusion of patients in the OPRA study has been prolonged. The prospective results relating to HRQL improvements are very encouraging and there is international interest in learning more about this treatment which justifies the current report, even if the study is still ongoing. However, conclusions drawn from statistical analyses in the current report should at this stage be evaluated with some caution. Nevertheless, this study demonstrates that the majority of individuals treated with a TFA OI-prosthesis describe considerable improvement of their general as well as condition-specific HRQL at 2-year follow-up as compared to the preoperative situation.
Among the 18 patients there was one patient that could not use the OI-prosthesis at follow-up due to severe pain during weight bearing (patient 6, Table I and Figure 4A). This patient was found to have loosening of the implant possibly related to osteoporosis from being an amputee for 32 years. Yet, she asked if she could be treated again, and in year 2003 the surgical sessions were repeated followed by an individually designed rehabilitation protocol. Her outcome will be presented in the final report of the OPRA study.
Previous studies on individuals with LLA have shown that the physical dimensions of SF-36 are influenced to a higher degree than those measuring the mental components of health (Smith et al. 1995; Legro et al. 1999; Pezzin et al. 2000). For this reason, the improvements in the PF, RP, BP, and PCS scales shown in the present study are reasonable. The authors noted lower scores, but with non-significant changes, at follow-up for some patients in the scales reflecting the mental health (VT, SF, RE, MH, MCS), most notably in the RE scale (Figure 3). The time from the preoperative assessment to follow-up in the current study was about 2.5 years. During such a long period other circumstances affecting HRQL could of course appear. This was the case for three of the patients (one got divorced, one had a close relative developing a lethal disease, one was forced to change work situation) which could explain their lower scores and thus affecting the mean of the group. In order to present prospective results of SF-36 for patients using the OI-prosthesis the one patient that did not use the prosthesis at follow-up was excluded and the analysis is based on 17 patients (Figure 3). The SF-36 is not suitable for individual comparison between assessments, which means presenting data for a single patient is not appropriate. For this reason the data was also analysed for all 18 patients and still the same scales (PF, RP, BP and PCS) showed to be statistically significantly improved.
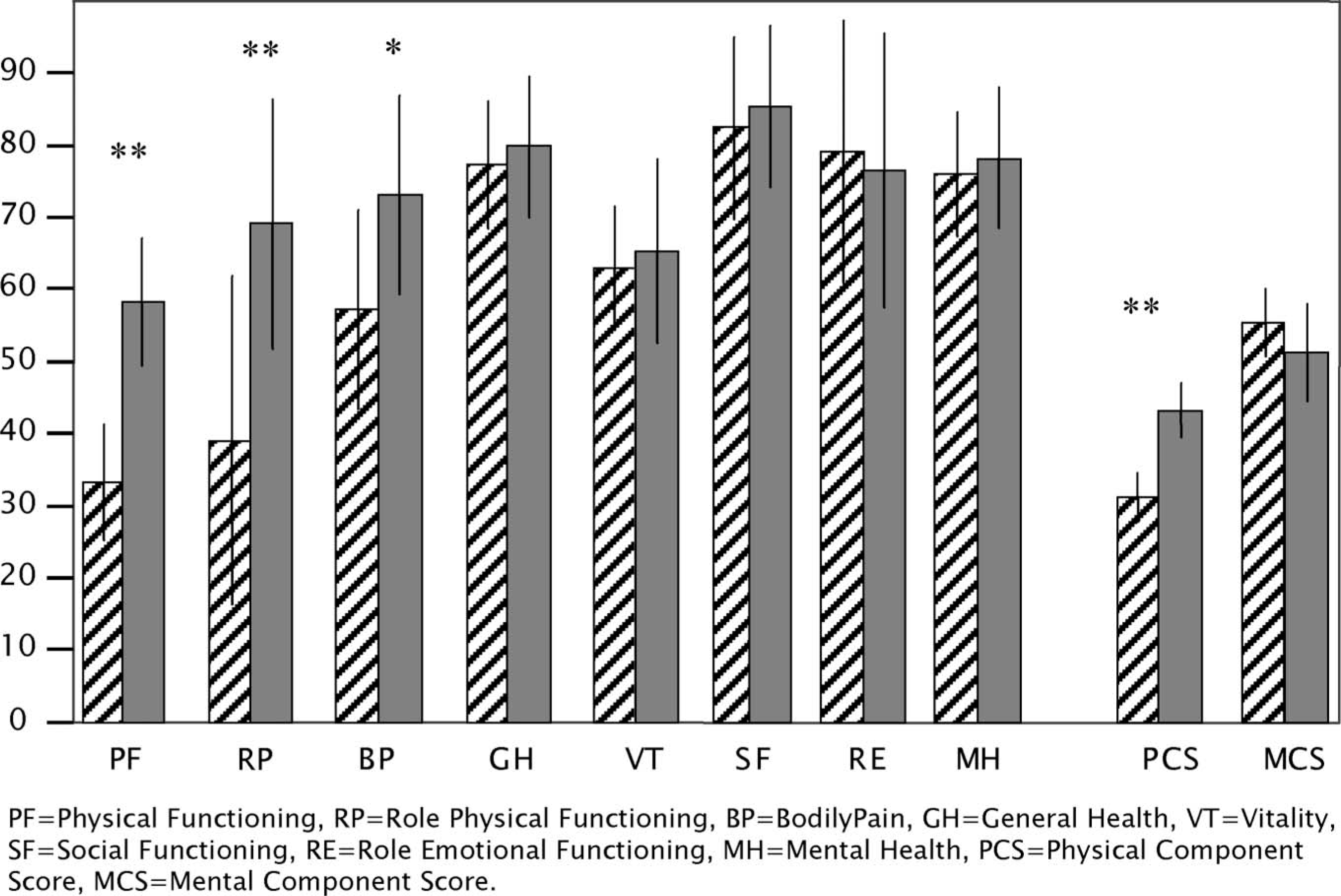
Results of SF-36 preoperatively (striped bar) and at 2-year follow-up (grey bar) for the group of patients using OI-prostheses at follow-up (n = 17). Bar represents mean and line represents 95% confidence interval. ∗p < 0.05, ∗∗p < 0.01
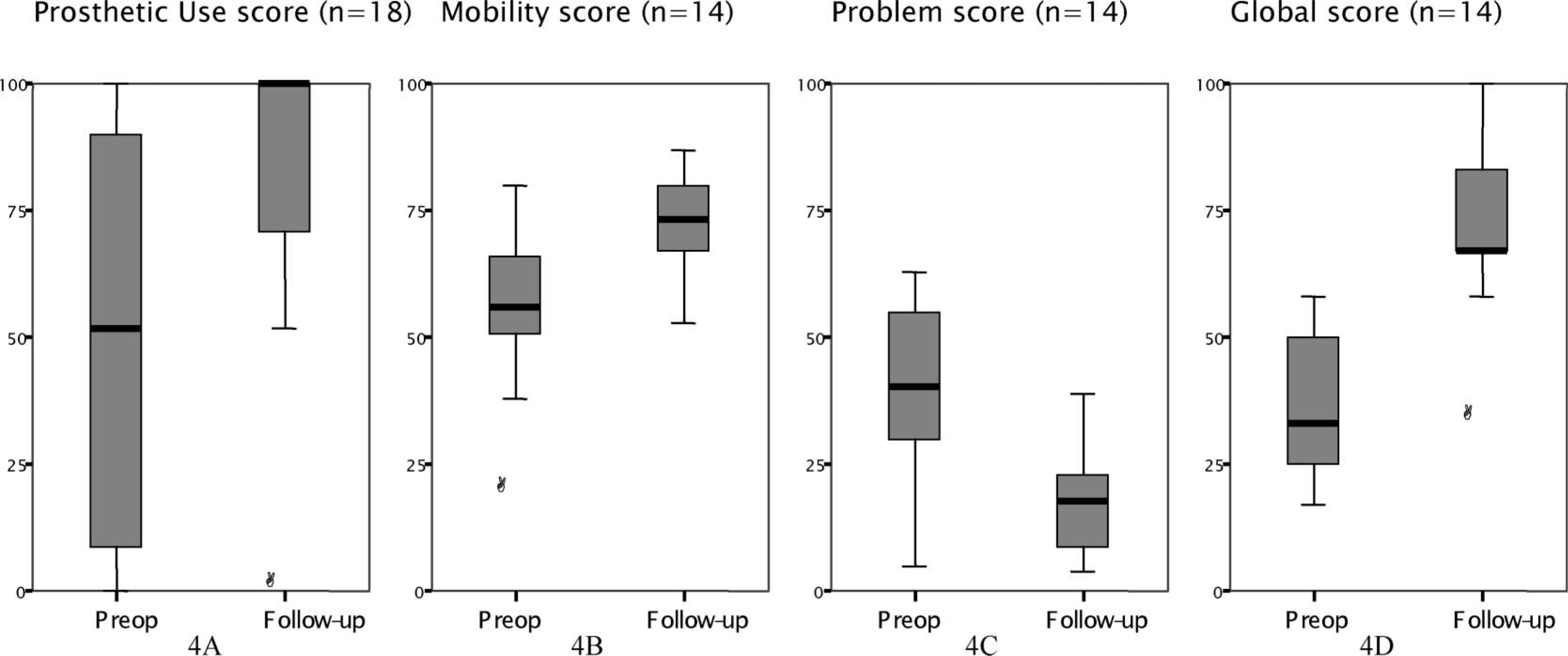
-4D. Distribution for score points for the four scores of Q-TFA preoperatively and at 2-year follow-up. The box indicates 50% of all values, the bold line the median value. Each circle represents a single outlier.
One of the objectives for choosing a generic HRQL instrument is the possibility to compare results between different groups. For this reason, the authors extracted the subgroup consisting of patients with unilateral amputations using OI-prostheses at follow-up (n = 15) to compare with previously published data on patients with unilateral amputations or limb sparing surgery. Results of SF-36 from six studies (Dagum et al. 1999; Davis et al. 1999; Hagberg and Branemark 2001; Malo et al. 2001; Conroy et al. 2003; Dougherty 2003) and the current subgroup have been compiled to illustrate such a comparison (Table II). It is interesting to note how the scales reflecting physical dimensions for the 15 patients are equal to, or better, than the results from several of the other investigations. Such observations can be important as they may influence the indications for amputation versus limb salvage.
Previously published results for SF-36 compared with the current study
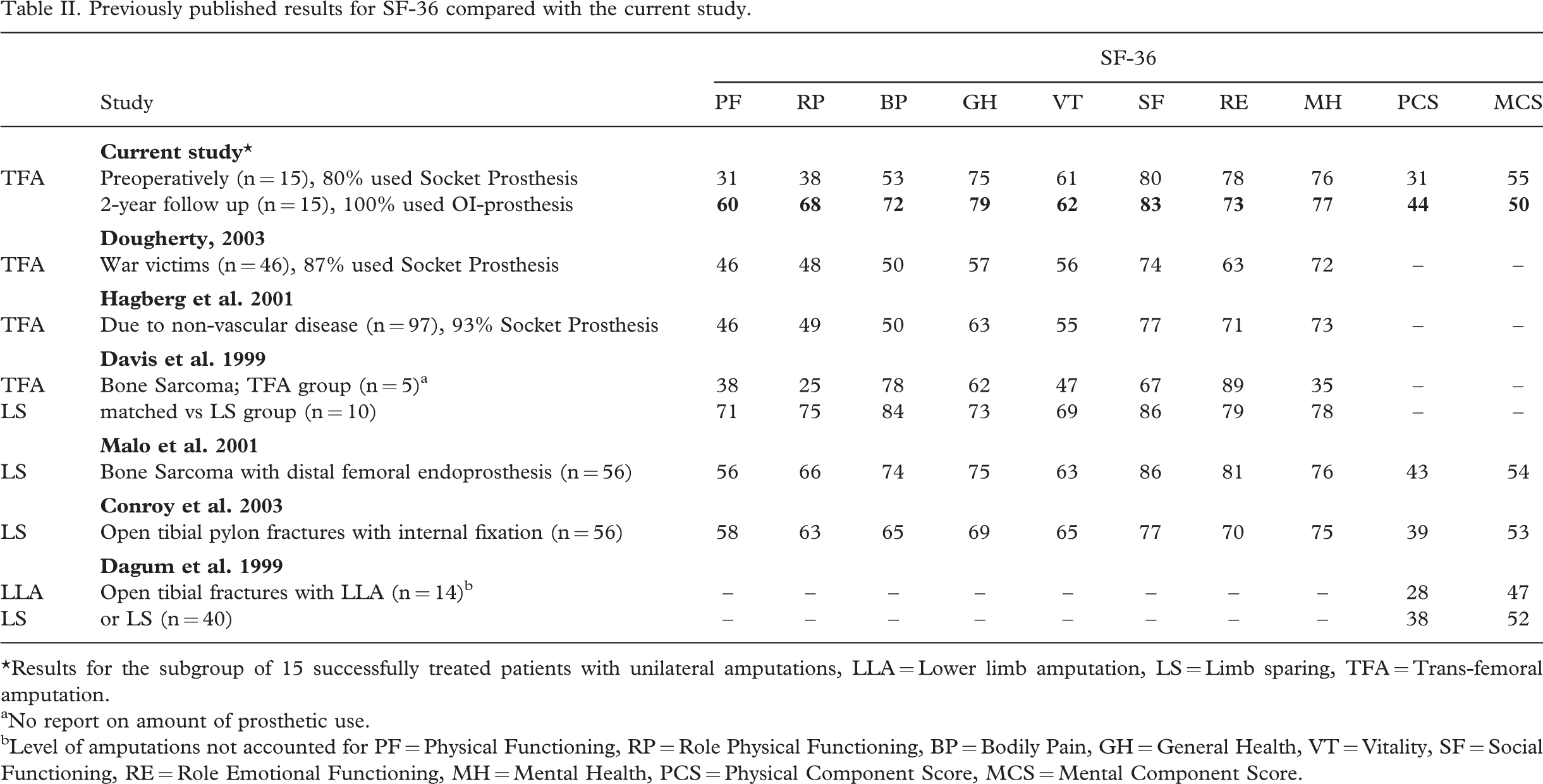
∗Results for the subgroup of 15 successfully treated patients with unilateral amputations, LLA = Lower limb amputation, LS = Limb sparing, TFA = Trans-femoral amputation.
aNo report on amount of prosthetic use.
bLevel of amputations not accounted for PF = Physical Functioning, RP = Role Physical Functioning, BP = Bodily Pain, GH = General Health, VT = Vitality, SF = Social Functioning, RE = Role Emotional Functioning, MH = Mental Health, PCS = Physical Component Score, MCS = Mental Component Score.
The Q-TFA was designed to capture the situation for individuals using prostheses. Hence, the Mobility, Problem and Global scores can not be reported when no prosthesis is used. Test-retest reliability of the scores has been established on individuals using socket prostheses. The measurement error was 12 score points in the Prosthetic Use score, 10 in the Mobility score, 16 in the Problem score and 19 in the Global score (Hagberg et al. 2004). The present results show that each one of the four Q-TFA scores improved beyond their respective measurement error. In addition to demonstrating an improved situation for the group of patients, the results also tell that the scores of Q-TFA are responsive to detect changes when shifting from socket prostheses to OI-prostheses.
Of the 17 patients using the OI-prosthesis, 12 scored 90 or above on the Prosthetic Use score which means prosthetic use for at least 13 hours every day. High levels of prosthetic use has earlier been reported among non-elderly individuals using conventional prostheses (Walker et al. 1994; Burger et al. 1997; Dillingham et al. 2001; Hoffman et al. 2002). However, extensive problems related to the use of socket prostheses have also been reported (Walker et al. 1994; Legro et al. 1999; Dillingham et al. 2001; Gallagher et al. 2001; Hagberg and Branemark 2001). The general finding in the current study was that the patients reported an increased use of the artificial limb without an increase in reported problems (Table I). Yet, there are still occasions when the patient may have to abstain from wearing the prosthesis. Broken prosthetic components and phantom limb pain could appear with socket prostheses as well as with OI-prostheses. Two patients reported that they had to abstain from the OI-prosthesis for a few days due to a superficial infection at the skin penetration area. In general, infections did not constitute a major problem. Details of this very important issue, and other potential complications within the OPRA protocol, will be reported separately. Referring to stump pain, our clinical experience is that a more active lifestyle is achieved with the OI-prosthesis, which can explain overloading and pain in the residual musculoskeletal structures. A more active life has been stated among patients treated according to this method in the UK (Sullivan et al. 2003) and this is supported by the improvements in prosthetic capability and walking habits demonstrated within the Mobility score in the current study. However, the improvement in the Walking-aid sub-score was not statistically significant. Normally, we recommend the patient to use a stick when walking longer distances outdoors to optimize the gait pattern. Consequently, 14/17 OI-prosthetic users reported that they normally used a walking aid outdoors.
Among the 18 patients treated ten were females. In the literature reporting on patients with LLA the majority of patients are males. It has been shown that female patients rate the importance of a variety of issues in regard to prosthetic use higher than males (Legro et al. 1999). Moreover, within the general Swedish population females report less good health than males on all scales of the SF-36 (Sullivan et al. 1994). The relatively high number of female cases in the current report should for this reason be noted when comparing this study's results with others.
The decision if a patient is suitable for this treatment is a consensus taken by the expert team which includes orthopaedic surgeons, physiotherapists and prosthetists. To be included in the OPRA study a number of parameters have to be fulfilled, which will be described separately. Two of the patients in the current report had a body weight above 100 kg (Table I). Both were included, in spite of their weight, based on good skeletal conditions and very limited possibilities to use a socket prosthesis along with low expected postoperative activity level. The important aspect for exclusion is not the body weight alone, but the preoperative skeletal condition in conjunction with expected bending forces over the implant system.
No clear tendency in change of the work situation at follow-up could be seen in this material. As presented in Table I three patients were at the age of 60, or above, already at inclusion and eight had been amputees for more than 15 years. Maybe, it is not realistic to anticipate going back to work or increase the working hours among individuals with higher age or a long time since the amputation. Hopefully, treatment with OI-prosthesis with reduction of socket related problems can help the individuals to maintain their working capacity. The one person changing her situation from work to sick listed was again the patient with loosening of the implant.
One limitation of the current study is the modest number of patients that have been followed for two years, which is a fairly short period in this context. However, this is the first prospective study reporting on patients with OI-prostheses. The authors continue to follow all the patients included in the OPRA protocol, with the aim of reporting the entire protocol, as well as long term results, in a large group of patients over the coming years. The OPRA study started already in year 1999, which means that seven of the patients reported on here have also passed 3 years and five have passed 5 years since S2, all still using their OI-prosthesis. Altogether, the initial prospective results presented here show improved quality of life for patients using an osseointegrated amputation prosthesis indicating the potential of this treatment.
Footnotes
Acknowledgement
The work was supported by Johan Jansson Foundation, FRN Foundation and Integrum AB, all of Sweden.