
Abstract
Background:
A well-fitting and comfortable ischial containment socket relies on accurately replicating the transverse plane angle of the ischium and ischial ramus angle, inside the medial socket brim. Prediction of the ischial ramus angle, may provide a way to determine the ischial ramus angle without in vivo measurement.
Objectives:
To determine the accuracy with which the ischial ramus angle could be predicted and identify which variables contributed significantly to the prediction.
Study design:
Cross-sectional study.
Methods:
Computed tomography scans were randomly sampled from a cadaveric database (n = 200). Standard multiple regression models were developed to predict the ischial ramus angle based on pelvic measures.
Results:
The regression model explained 10.5% of the variance in ischial ramus angle (p = 0.018). The standard error of the estimate was 11.32°. While regression models by sex explained a larger proportion of the variance, the resulting accuracy was not improved.
Conclusion:
The regression models explained a small proportion of variance in ischial ramus angle. The average error associated with the prediction was too large to accurately predict the ischial ramus angle for use in clinical practice. Contrary to commonly held beliefs, there was no statistically significant difference in ischial ramus angle between sexes.
Clinical relevance
Prediction of ischial ramus angle does not have sufficient accuracy to be clinically useful, but descriptive data may help clinicians identify casting errors and correct these in a plaster positive, knowing that the average ischial ramus angle was 32.65°±5.59° (relative to mid-sagittal plane) and does not vary between sexes.
Keywords
Introduction
Since the early 1990s, the ischial containment socket has been a common socket geometry for people living with transfemoral amputation.
A well-fitting and comfortable ischial containment socket relies on accurately encapsulating the medial ischium and ischial ramus inside the medial socket brim.
Accurately capturing the three-dimensional (3D) shape and orientation of the ischium and ischial ramus occurs during the process of casting the residual limb and pelvis. While there are many different approaches to casting the residual limb and pelvis, this illustrative example 1 highlights that during casting, after the residual limb and pelvis are wrapped in plaster bandage (Figure 1(a)), a prosthetist endeavours to place the palmar surface of the index and middle fingers along the medial aspect of the ischium and ischial ramus, as well as the lateral side of the third finger inferior to, and along the length of, the ischium to capture the shape and transverse plane orientation of the ischium and ischial ramus (Figure 1(b)). Prior to removing the cast, the prosthetist draws a straight line on the distal end of the cast, parallel to the mid-sagittal plane, to preserve the transverse plane orientation of the medial ischium and ischial ramus (Figure 1(c)) through to the subsequent stages of cast modification and socket alignment.
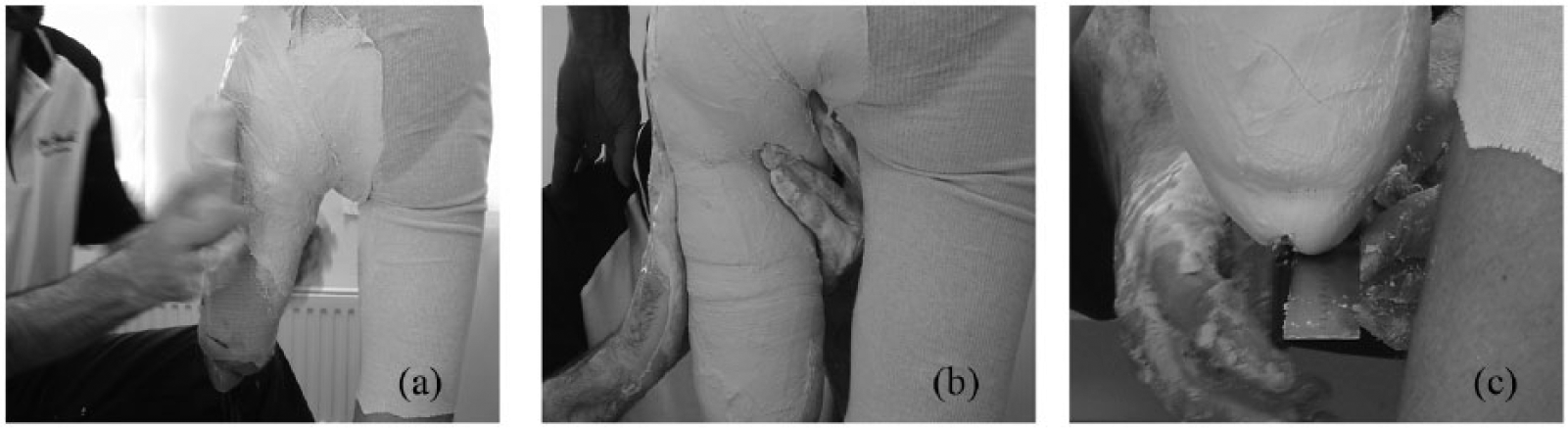
Images showing the sequence of: (a) posterior view showing wrapping the residual limb and pelvis in plaster, (b) posterior view showing palpation and hand placement on the medial and inferior ischium and ischial ramus and loading along the lateral shaft of the femur and (c) posterior view showing the prosthetist drawing a straight mid-sagittal line on the distal end of the cast to preserve the transverse plane alignment of the cast. L: lateral. Images reproduced with permission from Dillon. 1
Given this understanding of the casting process, it is perhaps not surprising that it can be difficult to produce a socket that accurately mirrors the 3D shape and transverse plan orientation of the ischium and ischial ramus. Even small discrepancies in the transverse plane orientation of the ischial containment relative to the ischium and ischial ramus can result in discomfort; particularly given that there is very little subcutaneous adipose tissue overlying the medial ischium and ischial ramus that can accommodate discrepancies.
To improve the reliability with which a well-fitting and comfortable ischial containment socket can be made, prosthetists have sought to measure the transverse plane orientation of the ischium and ischial ramus relative to the mid-sagittal plane (hereafter known as the ischial ramal angle, IR angle). Measurement of the IR angle in vivo helps engender confidence in the accuracy of the negative cast and can help correct casting errors during the process of modifying the plaster positive.
Measurement of the IR angle was popularised by Marlo Ortiz through demonstration of the ‘Marlometer’ in his courses (Figure 2(a)). To use the Marlometer, the prosthetist would hold one arm of the calliper in place along the medial aspect of the ischium and ischial ramus while the client stood with both anterior superior iliac spines (ASIS) pressed against parallel bars. The other arm of the Marlometer was then rotated into the mid-sagittal plane, perpendicular to the parallel bars. Once removed from the patient, the angle between the two arms of the Marlometer could be measured. In later years, and in partnership with Marlo Ortiz, Ossur subsequently developed the transfemoral toolset (Figure 2(b)). Based on ostensibly the same measurement approach, a small plastic mould (Figure 2(b), A) was designed to cup the medial and inferior ischium. The prosthetist would hold the plastic mould in situ on the ischium and rotate the ‘fitting connector’ into the mid-sagittal plane (Figure 2(b), B) and read the transverse plane angle between the medial ischium and mid-sagittal plane from the pointer and angle gauge (Figure 2(b), C).
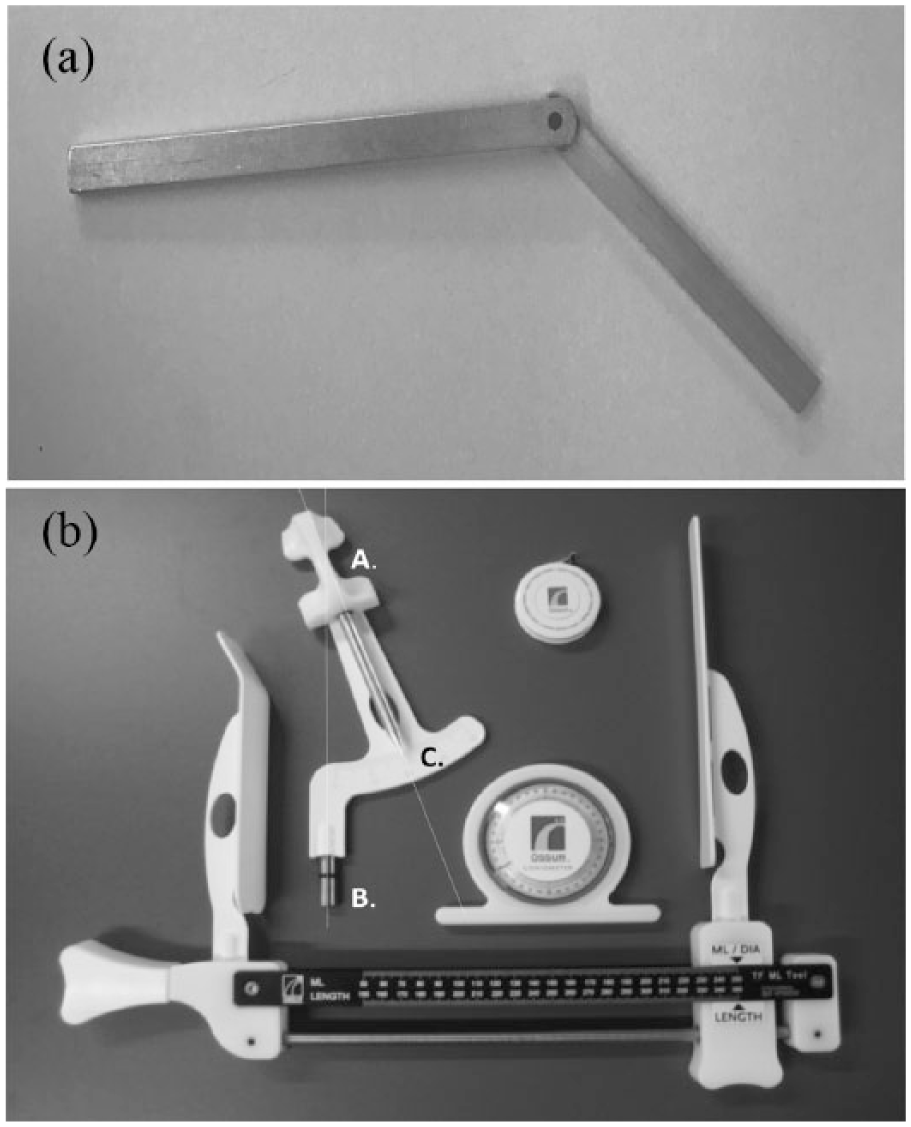
(a) ‘Marlometer’. To measure the transverse plane angle between the medial ischium and mid-sagittal plane, the prosthetist would hold one arm of the calliper in place along the medial aspect of the ischium and ischial ramus. The other arm of the calliper was then rotated into the mid-sagittal plane. Once removed from the patient, the angle between the two arms of the calliper could be measured. Image courtesy of Marlo Ortiz and published with permission. (b) Ossur transfemoral toolkit: a multipurpose tool for measuring residuum length, skeletal ML, soft tissue ML as well as the transverse plane angle between the medial ischium and mid-sagittal plane. A small plastic mould was designed to cup the medial and inferior ischium (A). The prosthetist would hold the plastic mould in situ on the ischium and rotate the ‘fitting connector’ into the mid-sagittal plane (B) and subsequently read the transverse plane angle between the medial ischium and mid-sagittal plane from the pointer and angle gauge (C). Once the transverse plane angle between the medial ischium and mid-sagittal plane had been established, the piece could be fitted into the calliper to allow measurement of the skeletal ML. Image courtesy of Ossur and published here with permission.
Given an understanding of the way prosthetists have endeavoured to measure the IR angle, we argue that the technique is unlikely to be accurate or reliable given errors commonly associated with goniometric or calliper measurements; even in comparatively idealistic scenarios where bony landmarks can be more readily observed and palpated compared to the ischium and ischial ramus.2–4 Hence, we wondered whether the IR angle could be predicted using reliable and less intrusive measures in the same way investigators have recently sought to accurately predict the skeletal medio-lateral (ML). 5 We suggest that many of these same independent variables that have been used to predict the skeletal ML – sex, age, stature, body mass and pelvic height and depth, as well as the distance between the ASIS, posterior superior iliac spine (PSIS), iliac crests and greater trochanters (GT) – may also serve as useful predictors of the IR angle, given they can be easily measured in clinical practice and likely explain variation in pelvic geometry (Figure 3).
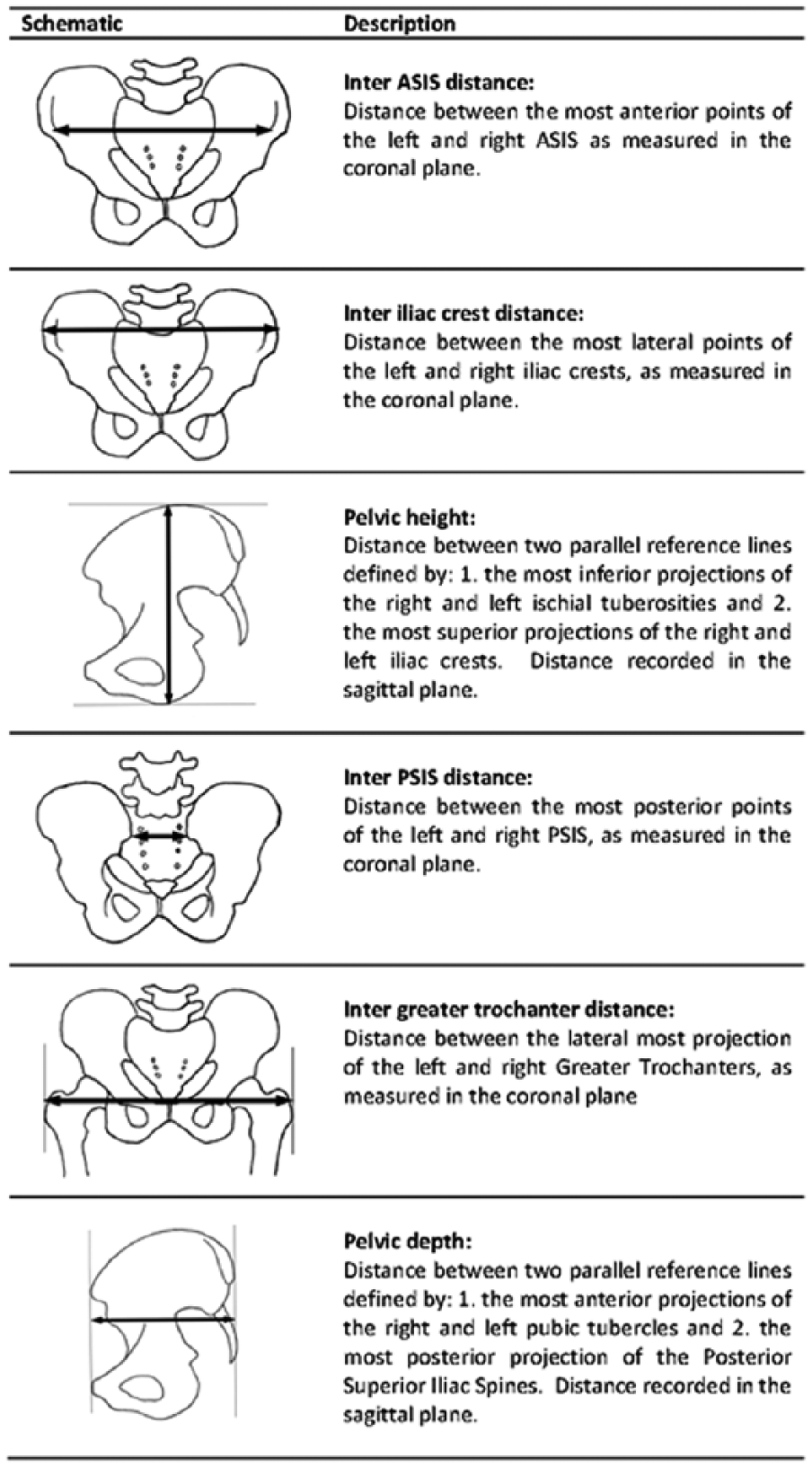
Schematic representation of pelvic measurements used as independent variables in predictive model. ASIS: anterior superior iliac spine; PSIS: posterior superior iliac spine. Figure originally published in Journal of Rehabilitation Research and Development. 5
Hence, the aim of this study was to determine the accuracy with which the IR angle could be predicted and if so, which of the aforementioned independent variables contributed significantly to the prediction.
Methods
The methodology of this study has been described in detail previously 5 and as such, a summary has been reported here.
Selection of computed tomography scans
Whole body computed tomography (CT) scans were obtained from a database of deceased persons held by the Victorian Institute of Forensic Medicine, Melbourne, Australia. Ethics approval was provided by the Victorian Institute of Forensic Medicine, Research Advisory and Ethics Committee, as well as the La Trobe University Human Ethics Committee. The database included all persons whose death was reported to the Coroner within the state of Victoria, Australia; hence, it was believed to be representative of the Australian population. 5 Cases were randomly sampled and subsequently vetted against the following exclusion criteria until 200 cases – sufficient to meet the minimum sample size requirement 5 – were obtained. Cases were excluded if: younger than 20 years of age, mass or stature outside of Australian population norms, 6 evidence of osteological trauma, orthopaedic implants, body growths (e.g. osteophytes) or lower limb alignment atypical of standing anatomical position (e.g. hip abduction). 5
Apparatus
CT scans were measured using Vitrea, version 3.1 (Vital Images Inc; Minnetonka, MN, USA). Each frame/graduation corresponded to a 2-mm transverse slice thickness. The software included a rendered 3D image showing the CT cross-section being simultaneously displayed in each anatomical plane of reference.
Procedure
Case demographics reported with each CT scan allowed extraction of sex, age, stature and body mass.
Anatomical planes of reference were established for each scan. The transverse plane was defined by the most inferior aspect of the left and right ischial tuberosities. The coronal plane was defined by a plane passing through the most anterior part of the right and left ASIS and the pubic tubercles. The sagittal plane was perpendicular to the coronal plane. This made it possible to pan through sequential slices of the CT scans in anatomical planes of reference and record measurements with respect to these planes (e.g. the inter-ASIS distance was measured in the coronal plane).
A variety of techniques were used to record measurements from the CT scans using the Vitrea ruler and angle tools. For example, to obtain the IR angle, it was necessary to first define the posterior and anterior parts of the medial ischium (i.e. the most posterior part of the ischium and the most posterior part of the obturator foramen, Figure 4 dotted lines) as well as the transverse plane slice at which this angle would be measured (i.e. midway between the most inferior part of the ischial tuberosity and most inferior part of the obturator foramen, Figure 4 dashed lines). With these landmarks and planes identified, the Vitrea angle tool was used to measure the IR angle (Figure 4 solid line) as illustrated in the transverse plane (Figure 5). Similarly detailed descriptions have been reported previously 5 describing how each of the independent variables were measured from the CT scans.
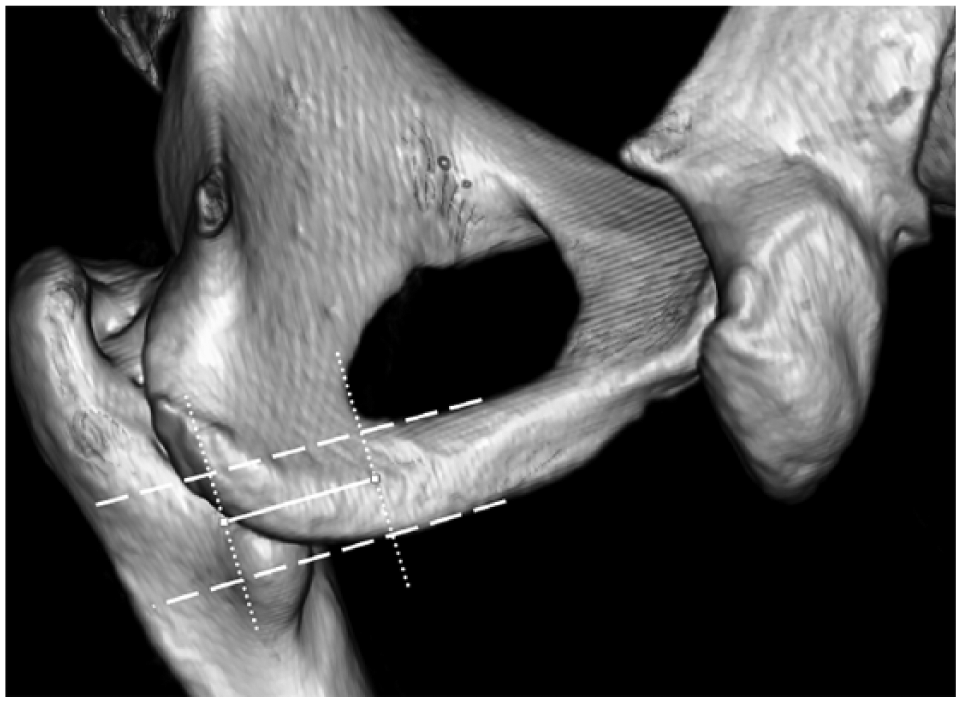
Posterior-medial view defining the medial ischium (i.e. the most posterior part of the ischium and the most posterior part of the obturator foramen, dotted lines) and slice (i.e. mid-point between the most inferior part of the ischial tuberosity and most inferior part of the obturator foramen, dashed lines) at which the transverse plane angle of the medial ischium and mid-sagittal plane was measured.
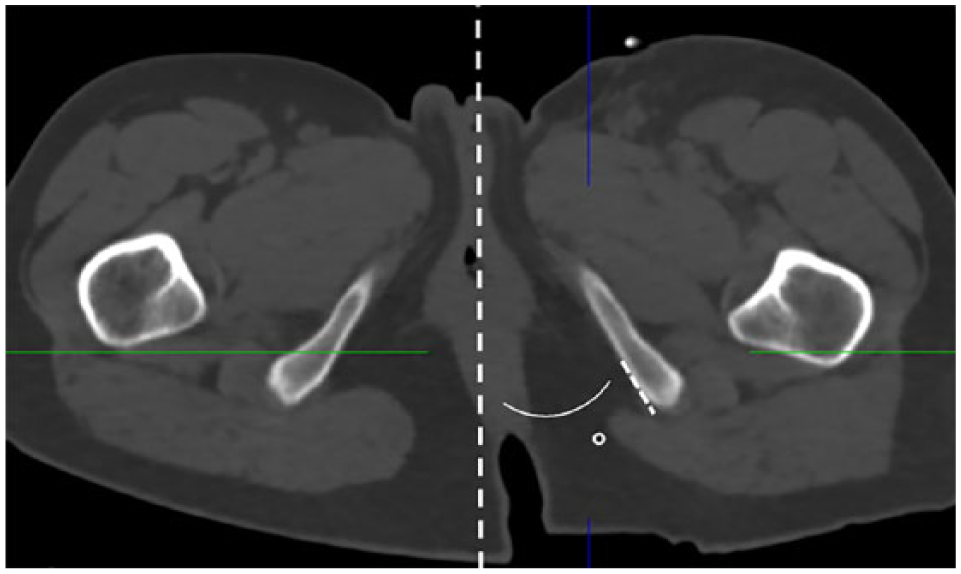
Ischial ramal angle, as shown on transverse section of CT scan relative to mid-sagittal line. The section of the ischium used to determine the IR angle was identified by the dashed line.
The author (MQ) was trained to use Vitrea, and reliability of the measurement protocol was demonstrated prior to the commencement of the study. 5
Data reduction and analysis
Descriptive statistics characterising the sample were reported using measures of central tendency and variability appropriate to the data type.
Preliminary analyses and assumption testing were conducted to establish the validity of the regression model. 7 Standard multiple regression models were developed in accord with the techniques described by Pallant 7 to predict the scalar-dependent variable (i.e. IR angle) using 10 independent variables: age, sex, stature, mass, inter-ASIS distance, inter-PSIS distance, pelvic depth, inter-iliac crest distance, pelvic height and inter-GT distance. While sex was a categorical variable, all other independent variables were scalar data. All independent variables were simultaneously entered into the model, given there was no a priori knowledge about the hierarchy with which these should be entered. We subsequently developed separate regression models or included interaction terms as appropriate to understand the true effect of each independent variable. The results were presented as standardised coefficients (beta) to allowed direct comparison of which independent variables had the greatest effect on the IR angle. A two-tailed p-value of 0.05 was considered to be significant. All analyses were conducted using SPSS 24 (IBM Corporation; Armonk, NY, USA).
Results
Demographic data from the sample describe a diverse population as evidenced by the wide range of measures for age, stature, body mass, body mass index (BMI) and IR angle (Table 1).
Demographic characteristics of sample (n = 200).
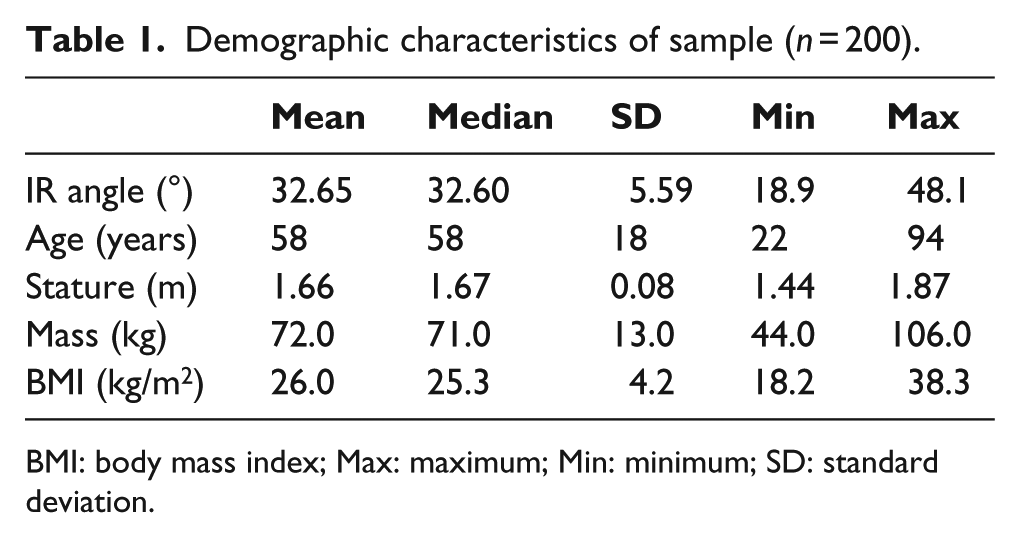
BMI: body mass index; Max: maximum; Min: minimum; SD: standard deviation.
The multiple regression model explained 10.5% of the variance in IR angle (r2 = 0.105) which was statistically significant (F10, 189 = 2.224, p = 0.018). Only pelvic height made a unique and statistically significant contribution (beta = 0.367, p = 0.003, Table 2), explaining 4% of the total variance as determined by the square of the part correlation coefficients (Table 2). 7 The standard error associated with the prediction of the IR angle was 11.32° (SEE = 11.32).
Estimated coefficients from multiple regression model of ischial ramal angle (n = 200).
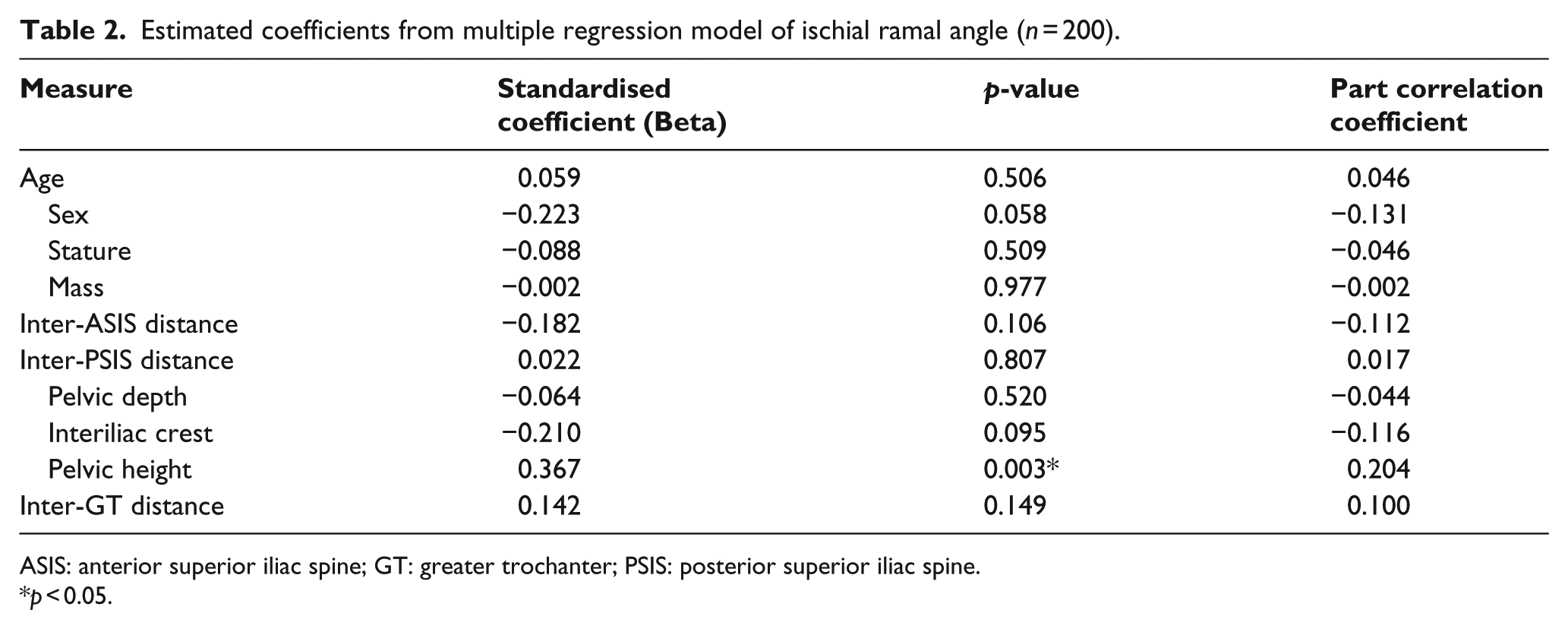
ASIS: anterior superior iliac spine; GT: greater trochanter; PSIS: posterior superior iliac spine.
p < 0.05.
Given the effect of sex approached significance (beta = –0.223, p = 0.058, Table 2), and the potential for sex to confound the effect of the other independent variables, we reported demographic data (Table 3) and developed separate regression models for females and males (Table 4).
Demographic data for the female (n = 89) and male (n = 111) subsamples.
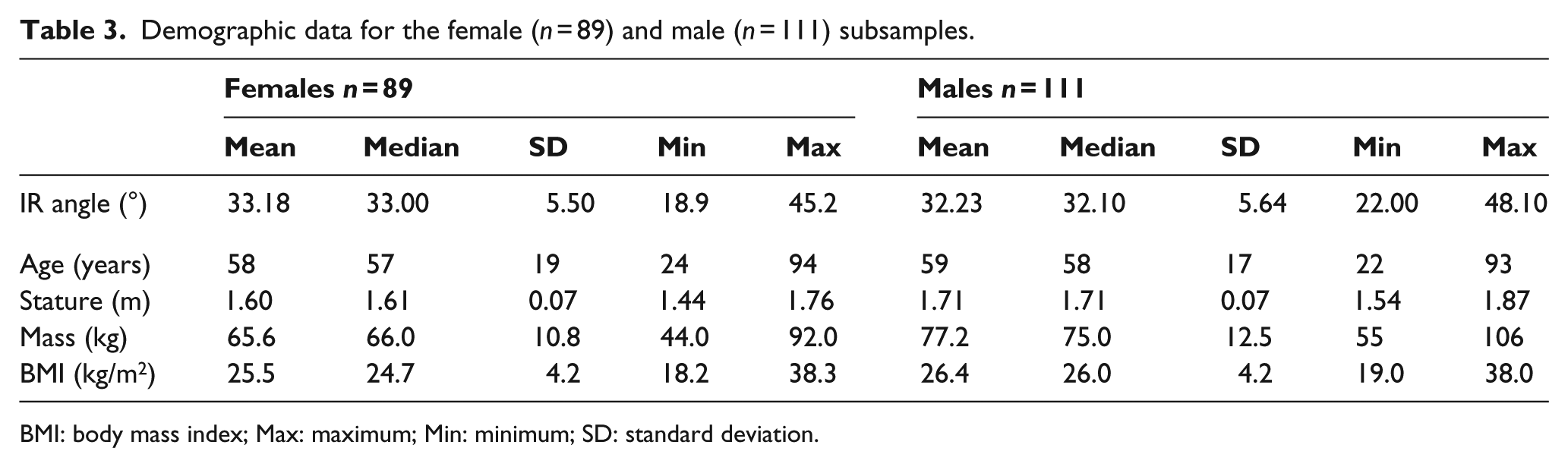
BMI: body mass index; Max: maximum; Min: minimum; SD: standard deviation.
Estimated coefficients from multivariate linear regression of ischial ramal angle in females and males.
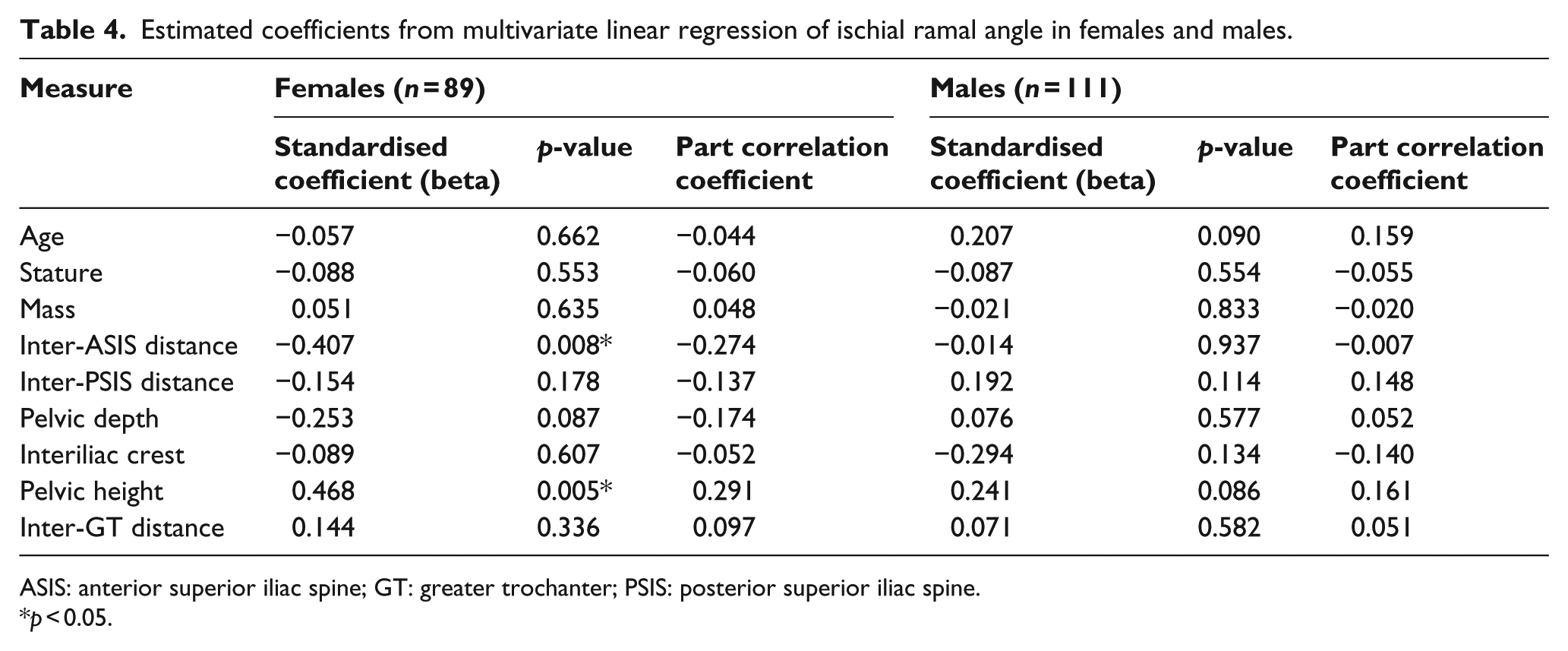
ASIS: anterior superior iliac spine; GT: greater trochanter; PSIS: posterior superior iliac spine.
p < 0.05.
In the female cohort, the regression model explained 19.9% of the variance in IR angle, which was statistically significant (F9, 79 = 2.182, p = 0.032). Variables that contributed significantly to the prediction in the female cohort were: pelvic height (beta = 0.468, p = 0.005) and inter-ASIS distance (beta = −0.407, p = 0.008; Table 4). In the male cohort, the regression model explained 13.1% of the variance, which was not statistically significant (F9, 109 = 1.687, p = 0.102). These regression models based on sex were able to predict the IR angle with a similar standard error in females (SEE = 16.37) and males (SEE = 16.32).
Discussion
This study sought to estimate how accurately the IR angle could be predicted using measures that were able to be recorded easily in clinical practice and to determine which of these measures contributed significantly to the prediction.
Given the regression models explained a small proportion of the variance in the IR angle, and the average error associated with the predicted IR angle was large, the models were not able to predict the IR angle with sufficient accuracy to be of use clinically.
Given that well-known references describing ischial containment design8–12 suggest that the IR angle is larger in females than in males, we were surprised that sex did not explain a significant part of the variance in the IR angle; something most easily observed in the similarity of the mean IR angle in females (33.18°± 5.50°) and males (32.23°± 5.64°). It seems that authors have inferred that there are sex-based differences in the IR angle based on literature showing that the subpubic angle is larger in females than males.13,14 Studies of sexual dimorphism suggest that bone deposition and resorption along the ischio-pubic ramus and ischium differs in adolescent females and results in a wider subpubic angle compared to males.13–15 However, we were unable to find any evidence to suggest that these mechanisms influence the morphology of the medial ischium or ischial ramus which may explain why there is no sexual dimorphism in the IR angle. We were also unable to find previous peer-reviewed literature describing the range of IR angles.
While sex did not have a statistically significant influence on the IR angle, sex did confound the effect of pelvic height and inter-ASIS distance. In the initial regression model pelvic height had a statistically significant influence on the IR angle (beta = 0.367, p = 0.003, Table 2). The separate regression models by sex showed that pelvic height only had a significant effect in the female cohort (beta = 0.468, p = 0.005, Table 4), not in the male cohort (beta = 0.241, p = 0.086, Table 4). In other words, pelvic height was only a significant factor for the prediction of the IR angle among females.
Clinical implications
The descriptive data reported in this study, specifically the average IR angle (32.65°± 5.59°), could be used by clinicians to assess the negative cast or to make modifications to a plaster positive, where the IR angle was not well captured in the plaster cast. While the average IR angle may provide an average with which to judge the plaster negative, it must be acknowledged that there is considerable variation across a population, given IR angles vary between 16° and 49° (mean IR angle ± 3SD).
We encourage those who teach ischial containment to highlight to their students that the IR angle – and therefore, the transverse plane angle of the ischial containment in the socket – does not vary by sex.
Limitations
There are a number of limitations that should inform how the results are interpreted and used.
Although our sample included a wide cross-section of the adult population, there is no evidence to suggest that the average IR angles reported in this study would be applicable to adolescents or children, given that the pelvis does not reach skeletal maturity until early adulthood.16,17
Our sample included a larger proportion of males, reflective of the cases referred to the Victorian Institute of Forensic Medicine for autopsy. Hence, care should be taken interpreting the results of the regression models stratified by sex, given the study was not powered for the development of sex-specific regression models.
While a hierarchical regression model may be typical for such prediction, there was not sufficient research to inform an a priori understanding about which independent variables might explain the largest variance in the IR angle; information important to determine the rank order in which variables are included (or removed) in hierarchical regression. We hope that the rationale for our statistical approach helps engender confidence in the statistical method.
To obtain reliable measures of the IR angle from CT scans, it was necessary to precisely define anatomical landmarks. We have endeavoured to identify anatomical landmarks on the CT scans in keeping with contemporary ischial containment literature1,8,11 which suggests, for example, that the most posterior part of the ischial containment should align with the most posterior part of the ischium. Similarly, we used the most posterior part of the obturator foramen to define the anterior point of our measurement of the IR angle, given this landmark could be reliably identified on CT scans and was consistent with the relationship to palpable anatomical landmarks (e.g. adductor longus tendon, ischial tuberosity and pubic ramus) used by clinicians to design the geometry of the medial socket brim and the socket’s ischial containment.1,8 We hope that by defining these measurement points using the same anatomical landmarks that clinicians use to design the medial socket brim, the IR angles reported here will be useful for clinicians in practice. However, we are aware that variation in the definition of these landmarks will alter the IR angle – such as measuring the angle of the whole ischium, ramus and pubis relative to the sagittal plane – that does not provide data appropriate for the design of the transfemoral socket’s ischial containment. 18
Future research
We suggest that there is likely little value in pursuing further research to predict the IR angle, given that we were able to explain only a small part of the variance in the IR angle despite using a comprehensive range of factors that could be easily measured in clinical practice. While there may be other factors that might explain significant variation in the IR angle (e.g. subpubic angle), and therefore, make useful predictors of the IR angle, these factors would need to explain a significant part of the unique variance in the IR angle and be able to be easily and reliably measured in everyday clinical practice.
Conclusion
This study sought to estimate how accurately the IR angle could be predicted using measures there were able to be easily recorded in clinical practice. Given the regression model(s) explained a small proportion of the variance in the IR angle and the average error associated with the predicted IR angle was large, the model was not able to predict the IR angle with sufficient accuracy to be useful in clinical practice. While the regression model was not sufficiently accurate to be clinically useful, the average IR angle reported in this study could be used by clinicians to assess the negative cast or to make modifications to a plaster positive; acknowledging that IR angles will vary between 16° and 49° (mean IR angle ± 3SD). Perhaps the most important finding of this research was that contrary to popular ischial containment literature, the IR angle does not vary by sex.
Footnotes
Acknowledgements
The authors wish to thank the Victorian Institute of Forensic Medicine for their collaboration on this project.
Author contributions
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by the Research Focus Area in Sport, Exercise and Rehabilitation, La Trobe University (grant/award no.: 830079).