
Abstract
Background: Bone-anchored prosthesis is still a rather unusual treatment for patients with limb loss.
Objectives: The aim of this study was to improve our understanding about the experience of living with an osseointegrated prosthesis (OI-prosthesis) compared to one suspended with a socket, through the use of qualitative research methodology.
Study design: A qualitative phenomenological research method.
Methods: Thirteen Swedish patients (37–67 years) with unilateral upper or lower limb amputation (10 transfemoral, 2 transhumeral, 1 transradial), who had been using OI-prostheses for 3 to 15 years, were recruited by means of purposive sampling. An audio-taped in-depth interview was performed. The guiding question was ‘How do you experience living with your osseointegrated prosthesis compared to your earlier prostheses suspended with sockets?’. The empirical phenomenological psychological method was used for data analysis.
Results: The results showed that all participants described living with an OI-prosthesis as a revolutionary change. These experiences were described in terms of three typologies, called ‘Practical prosthesis’, ‘Pretend limb’ and ‘A part of me’.
Conclusions: The most important finding was that the change went beyond the functional improvements, integrating the existential implications in the concept of quality of life.
This qualitative in-depth interview study on patients using bone-anchored prosthetic limbs showed that all described a revolutionary change in their lives as amputees and the meaning of that change went beyond the functional improvements, integrating existential implications in the concept of quality of life.
Background
Direct skeletal attachment of prostheses has been pointed out as an important development in the future of artificial limbs. 1 This type of attachment can solve problems related to a prosthetic socket, such as poor suspension, chafing, pain and discomfort frequently described among prosthetic limb users. 2,3 To date, clinical results from two different treatment solutions for bone anchorage of artificial limbs have been published; one from Sweden 4– 6 and another from Germany. 7 During the last decades, hundreds of patients with major amputations perceiving socket-related problems have been treated with this type of prosthesis worldwide. In addition, other similar treatment methods are currently under development. 8,9
The Swedish treatment is performed by osseointegration of an implant in living bone, a method which was first applied in dental care. 10 An implant made of pure titanium is inserted into the residual skeleton in a two-stage surgical procedure. The artificial limb, the osseointegrated prosthesis (OI-prosthesis), is secured to the protruding implant by an attachment device without the need of any prosthetic socket. The total treatment time, including surgeries and rehabilitation, is about 6–18 months, depending on the level of amputation and quality of the residual bone. Primarily, individuals with transfemoral amputations due to trauma or tumour have been treated thus far. 6 A smaller number of individuals with major upper extremity amputations (i.e. transhumeral and transradial amputations) have also been treated. Complications related to OI-prostheses include risk of infections, mechanical complications of implant components and loosening of the implant. 6,11 – 13
Patients who have been treated in Sweden are followed regularly for clinical check-ups as well as for research purposes. Until now, research has included the collection of quantitative data through physical assessments and self-report questionnaires. Published outcomes include evidence of improved hip range of motion and sitting comfort when wearing prostheses, 14 improved general and specific health-related quality of life (HRQL), 5 improved hip extension and less pelvic tilt during gait 15 and a high functional level in terms of temporal gait characteristics. 16 These quantitative studies provided strong evidence of the prosthetic and biomechanical benefits of an osseointegrated fixation as well as improved HRQL as reported by questionnaires, but might only partially capture the patient’s experience of what it means to live with an OI-prosthesis compared to a socket-suspended prosthesis (S-prosthesis). Research methodology that captures patients’ experiences has been sought among patients using prosthetic and orthotic devices. 2,17 One methodology that enables researchers to explore the realm of lived experience is phenomenological methodology. Phenomenological methods have been recommended as an appropriate research paradigm for physical therapy research. 18
The aim of the current study was to increase our knowledge about the experience of living with an osseointegrated prosthetic limb, compared to a socket suspended prosthesis through the use of a qualitative phenomenological research method.
Methods
Participants
Participants were recruited by means of purposive sampling. Inclusion criteria were:
unilateral upper or lower limb amputation having been treated with OI-prostheses at least three years ago currently using the OI-prosthesis.
Individuals not living in Sweden or not able to communicate in Swedish were excluded. The sample included 13 participants (7 males, 6 females) of whom 10 had a transfemoral amputation and three an upper limb amputation (2 transhumeral, 1 transradial). The amputation had been performed between the age of 14 and 45 due to trauma (n = 6), tumour (n = 5) or infection (n = 2). All had used conventional socket prostheses before OI-treatment (1–42 years of experience of S-prostheses). The OI-treatment was performed during the years 1992 to 2005 and at the time of the interview the participants had used their OI-prosthesis for 3 to 15 years. All interviews were performed during 2009 and at this time the participants were aged between 37 and 67 years. Informed consent was obtained prior to participation and the study was approved by the Regional Ethical Review Board in Gothenburg.
Procedure
An audio-taped in-depth interview, lasting between one and two hours, was performed at a location chosen by the patient. Five patients were interviewed at home and the others in a room provided by the researcher. All interviews were performed by the first author, who had no prior relationship to the participants and no clinical experience of working with amputee rehabilitation. Open-ended questions were used in order to stimulate detailed accounts of the participants’ experience. The guiding question was ‘How do you experience living with your osseointegrated prosthesis compared to your earlier prostheses suspended with sockets?’. Prior to the taped interview the participant was asked to speak briefly about the amputation itself and was thereafter told that the aim of the interview was to focus on the OI-prosthesis.
Data analysis
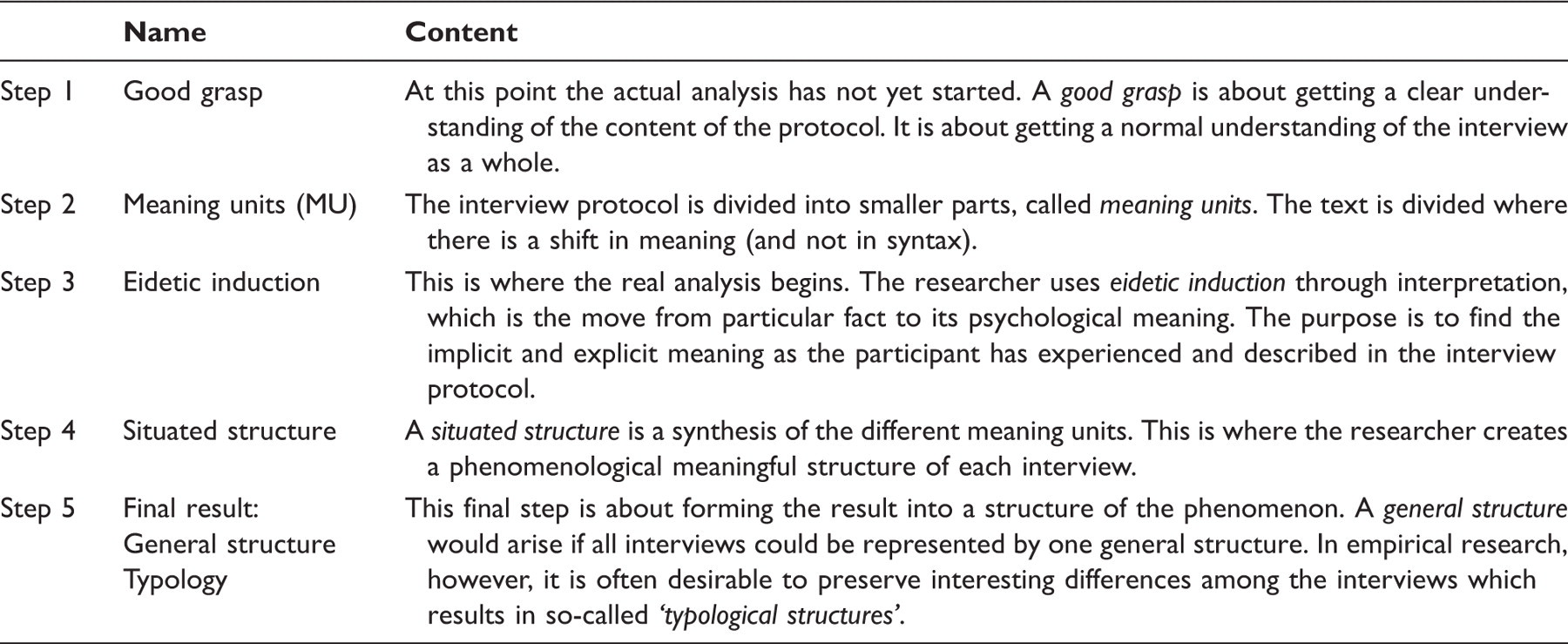
An example of the five analytic steps of the empirical phenomenological psychological (EPP) method. 19
Results
General characteristics
All participants in the present study described living with an OI-prosthesis as a revolutionary change in their lives as amputees. All of them described radical functional changes, such as being able to trust the fit and suspension of the prosthesis, being able to sit comfortably and not needing to spend time and mental energy being concerned with a socket. All these factors were experienced as contributing to an improvement in quality of life. These changes meant that the participants were less frustrated and could be more engaged in their life and social interactions rather than focusing on a scrambling socket chafing their skin or aching and pinching. Although living with the OI-prosthesis meant increased function and freedom, it also gave rise to some caution, due to a fear of losing this much improved function and freedom. For instance, they described a fear of falling that could cause a fracture of the skeleton and/or implant and a fear of getting infections at the skin-implant interface. Finally, living with the OI-prosthesis had a profound existential impact on their lives, in the sense that the new possibilities opened up by the prosthesis began a process of self-development. This process is described in terms of a gradual change in their identity from considering oneself as being disabled to having an identity as a healthy person.
In addition to the general characteristics described above, there were differences in the findings according to the degree by which the prosthesis had been incorporated into the persons’ lived body, their psychosocial environment and their sense of self. We have chosen to present how these patients experienced their world and life with their OI-prostheses in terms of three typologies, ‘Practical prosthesis’, ‘Pretend limb ‘and ‘A part of me’.
Typology I: Practical prosthesis
This typology depicts a way of living with the OI-prosthesis which can be characterized as a practical, technical attitude which regards the prosthesis as a tool, with pros and cons. It was talked about in concrete, practical terms, like a thing rather than a part of the person’s body or self. Living with the OI-prosthesis had started a process of feeling more like a normal person, but the technical limitations were still seen as hindrances to being able to live a normal life. The participants experienced limitations at the level of the ‘tool’ rather than in the way in which they adapted to, and coped with, the prosthesis.
The participants in this typology took a rational view of their OI-prosthesis and did not consider it to be a part of their body. They refer to the OI-prosthesis as a thing, but nevertheless looked upon it as a far more positive experience than the S-prosthesis.
‘I can feel that it’s (OI-prosthesis) not as good as a healthy leg, but it’s far more normal than the old one (S-prosthesis) … This is perhaps 70% as compared to a real leg and a real leg being 100% and an old prosthesis is perhaps 25%.’ (I4, MU19)
Although these participants were able to spend more time and energy on fun things like walking, they still felt frustrated that the prosthesis itself, e.g. the knee unit, was not perfect. They described that they were more mobile and experienced themselves as being less disabled or dependent in certain respects, but at the same time they experienced technical limitations causing a certain degree of dependency.
‘When the prosthesis works completely so that I can open and close the prosthesis (OI-prosthetic hand), then it’s fantastic, I can sit and eat with a knife and a fork, I can take the glass with my hand and lift it up and drink with it if I need to. It’s often the left arm(healthy arm) that does the work, but you have a completely new mobility and complement to the left arm, when the prosthesis functions that well. So for me being without the prosthesis is like feeling handicapped.’ (I10, MU 12-14)
‘The disadvantage (with the OI-prosthesis) is that if you got stuck with the foot for instance which has happened a number of times, the leg is twitching (the fail-safe attachment device) and then you can’t turn it right unless you get to the prosthetic workshop and then you feel much more handicapped instead.’ (I4, MU4)
Typology II: Pretend limb
The participants within this typology felt that the OI-prosthesis had become almost part of the body, although it was still viewed as a ‘pretend limb’. There was a duality in feelings towards the OI-prosthesis which concerned the function, as well as the cosmetic, aspects. Described in more concrete terms, on the one hand the improved function had given greater degrees of freedom in actual range of motion, meaning that the patient could do things that they had not been able to do before, such as dancing or cycling. On the other hand, the protruding implant of the OI-prosthesis stands out more, for instance in a swimming pool.
The participants described how their perception of themselves had changed in relation to their bodily change. In this typology they could describe how the OI-prosthesis had gone from being a technical device to almost becoming part of their body.
‘No, it’s much more integrated than it was with this old prostheses – it becomes a part of you. I don’t know how to describe it since it’s not like I’m feeling my foot in any way and it’s still a prosthesis, and that I am very much aware of – especially when I am in a bad mood.’ (I1, MU28)
‘The prosthesis(OI-prosthesis) is a part of me since it works so well, and you don’t have to think that it’s a problem and that it should be hard and so forth … it’s more like a substitute, my “pretend leg”.’ (I2, MU54)
The OI-prosthesis had created new possibilities for a better life, starting a process regarding their feelings of self. For some, this process involved an identity crisis, leading to a reformulation of their identity. The improved function and mobility made it possible for them to be more the person they wanted to be, giving rise to improved self-confidence, but also raising doubts about who they really were.
‘There is something missing, one part of me is missing and I miss it physically in a way I haven’t done before, not after the accident either. And this happened after I got the prosthesis(OI-prosthesis) that is more me than ever, that makes me feel more whole as a person.’ (I3, MU6)
The participants in this typology had an ambivalent comprehension of how they were considered by people in their environment with or without the prosthesis. On the one hand, when not wearing the OI-prosthesis, the residual limb with the protruding screw became more prominent than before the treatment. On the other hand, when wearing the prosthesis, they could see an advantage in that they could get closer to another human being, without the feeling of a hard and cold socket.
‘Yes, but my God I have forgotten to say something that is really important. I can hug without people killing themselves on me. I can hug people and my children. It’s still not so convenient to sit on this side, but it works, compared to before when I was all hard. I couldn’t hug anybody, but now I can hug. I don’t know how much they have thought about it, but I have thought about it a lot.’ (I3, MU 24)
Typology III: A part of me
Within this typology the participants experienced the OI-prosthesis as an incorporated part of the body. There was a complete acceptance of, and trust in, the functionality of the technical solution. The OI-prosthesis had in different ways strengthened the feeling of being a ‘whole body’, which influenced their way of looking at, and experiencing, the world. One way in which the OI-prosthesis had strengthened the feeling of wholeness in strictly practical terms, was the actual anchorage to the skeleton. Another way was the fact that the residual limb is set free and enables touching of the skin. The integration of the OI-prosthesis into the body and sense of self had gone so far that the patient believed that they could be more the person that they were before the amputation.
The participants accepted the OI-prosthesis as a part of themselves and were surprised by how well the body and brain had accepted it and described that they actually forgot about it. They also described that the concrete bone-anchorage strengthened the feeling of being a whole human being.
‘I don’t think about having the prosthesis in that it doesn’t feel like a prosthesis. With this kind of technology you can’t feel it. I sit just as much on this leg as on the other leg and the scary thing was this week when I didn’t have my leg on, and when I suddenly stood up I felt I had on the prosthesis. It has come so far that the brain has also gradually begun to believe that I have a real leg … ’ (I5, MU27)
‘Yes, because it’s purely physical, there is a fixture properly anchored, femur is reinforced with marrow and bone from the pelvis, it’s anchored with material from my own body, with the only purpose to give me the possibility to walk. It’s very concrete. As opposed to a traditional prosthesis that is slipped on to the outside of the body. But here I can feel when I put the foot down, so that I can feel the shock throughout the body, not in an unpleasant way but I feel it and it gives me a positive experience of my body as a whole.’ (I12, MU38)
For the participants in this typology, the improved function is experienced as more central than the cosmetic feature. The gain in function is also described at an existential level, like what it does to a person to not have an entrapped body part and how it heals you as a person to feel your body.
‘One part of the body is trapped in this vacuum-packed socket, that’s the way it’s. To be let out of this entrapment, just to feel the sun towards the thigh or the air that surrounds the thigh instead of this heat and the sweating that is coming. It was like … it was my definition of freedom, that and to not have to think about the suspension’ (I5, MU46)
‘One could feel what one did inside the body in some way, I felt when I cut a tomato or an apple or a potato, when you cut you can feel the hollows within the apple, it’s felt inside the prosthesis, one can feel what one cuts in to. Just a simple thing like that. And it heals very much, it makes you very whole, even though you are not’ (I8, MU14)
Within this typology the OI-prosthesis is experienced as such an integrated part of the person that it is not noticed as before in relation to other people.
‘I don’t think that they actually think in the same way that I do actually have a prosthesis, actually but no … no one questions today if I can do this or that but everyone takes it for granted that I can do it … if we’re about to do something I never hear anyone asking “Do you think you can make it?”.’ (I6, MU44)
Furthermore, the participants described how this prosthesis made it possible to be more themselves and to take control of their lives.
‘The other prosthesis ruled my life, it was my master in a way, it’s inevitable … it affected my mood and my interest in doing things that I knew would demand an extra effort. You had to weigh the pros and cons and that’s all gone now. Now it’s actually me … I am in command and not the left leg(S-prosthesis) and that’s a big difference.’ (I5, MU33)
‘Yes, it was at a Christmas party with the children when I had been walking with this prosthesis for maybe six weeks, and my little boy fell and I could bend down exactly where he fell, almost squatting, grab him, lifted him, got hold of him and could stand up with him in my arms and comfort him, that I recall as a wonderful experience. I could manage the whole sequence without losing the prosthesis or falling or asking anyone else for help.’ (I12, MU14-15)
Discussion
This is the first study using a qualitative approach in order to learn more about what it is like to live with a bone-anchored artificial limb. The principal finding was that all participants described living with an OI-prosthesis as a revolutionary change in their lives as amputees. The novelty of these findings is that the meaning of that change went far beyond the functional improvements, incorporating existential implications in the concept of quality of life.
Radical functional improvements, such as being able to use the prosthesis more, the ease to attach it and being more active, were described by all participants and are in line with previously published results. 5,12,14 A recent study on patients with limb loss stated that about one third would consider the osseointegration treatment to obtain such improvements. 20 It was evident, however, that the functional changes had a deeper meaning than earlier studies had been able to capture. 5,12,14 In another previous qualitative study the skills most missed among lower limb amputees were walking, biking and driving a car. 21 Our participants described the joy of being able to perform these activities. Furthermore, they described what it meant to them in terms of feeling more independent and more like themselves, feeling like the person they were before the amputation. Other qualitative studies on patients with limb loss have reported on the importance of autonomy for subjective wellbeing 21,22 and the importance of having meaningful roles or activities for the satisfaction in life. 21,23
The revolutionary change of improved quality of life was a common theme in all interviews. Among patients with transfemoral OI-prostheses, improved HRQL, as measured by self-report questionnaires, has been reported. 5 Furthermore, positive and negative aspects of the osseointegration treatment have also been pointed out in an interview study, 12 aspects brought up in that study were; improved proprioception, being able to walk further and feeling less disabled. In the present study, the existential component of quality of life was elucidated as a further aspect of the osseointegrated limb.
Based on what the participants in the present study described, to live with an OI-prosthesis is to adapt to an additional transformed body image. Body image is defined as ‘the image of our own body. It refers to the body as a psychological experience, which includes our emotions and attitudes, developed through our experience toward our own body’. 24 The individual with limb loss has to adapt to three different images of their body: before the amputation, without wearing prosthesis and when wearing prosthesis. 22 Earlier studies have reported a highly negative correlation between body image disorder and prosthesis satisfaction, 25,26 a negative correlation between body image disorder and mobility 24 and a positive correlation between physical activity and body image. 27 In addition, amputees who perform regular physical activities have been found to have a more intact body image. 27 It is not yet known what these associations might be among patients with OI-prostheses. However, one might speculate that since the patients report using their OI-prosthesis more, and are more physically active, they might also develop a more positive body image. Another interesting speculation is if the first adaptation of the amputation has an influence on the later adaptation of transformed body image caused by the OI-prosthesis.
As illustrated in the three typologies, participants described their adjustment process in different ways. It has earlier been pointed out that adjustment to wearing a prosthesis can vary depending on demographic variables, such as age, gender and length of time with prosthesis. 28 It needs to be pointed out that in the current study the participants in the three typologies varied in terms of such demographic data.
An adjustment process in terms of body image and body schema was reflected in the various typologies. It has been shown that wearing an artificial limb helps the amputee to maintain a body schema similar to an intact leg. 25 However, the same authors stated that ‘although the amputee can see the prosthesis and sense the phantom limb he/she does not consider it as their own, being aware of its absence’. 25 In the present study, participants in Typology II and III described how the OI-prosthesis had become more or less integrated in their experience of their body. The same phenomenon has been reported among patients with edentulousness treated with osseointegrated implants. 29 Moreover, it has been found that an artificial limb may lead to a sense of independence and bodily ability because of what it enables them to do. This can be described as prosthetic embodiment. 27,28 Our findings indicate that a bone-anchored prosthesis contributes to this phenomenon.
The body plays an important role in social life. 22 In the eyes of others, the person with an amputation might appear disabled and stigmatized. 30 The importance of being treated as a person and not only being related to in terms of one’s disability has been reported among individuals with limb loss. 22,31 Within Typology III the participants described that people in their environment related to them as being a normal person, who can participate in daily life on equal terms. Moreover, they described themselves as less frustrated and more positive towards their surroundings. It has been found that the less trouble the patient experiences with the prosthesis, the fewer emotional problems will be exhibited and the better social interaction will be. 28 Even though we are in need of further studies, there is reason to believe that due to the perception of less trouble with the OI-prosthesis compared to the conventional prostheses, patients with OI-prostheses would experience less emotional problems.
One limitation of the current study is that we only included those who currently used their OI-prosthesis. There are some known complications related to the osseointegration treatment 12,13 and in a low number of cases the treatment has been unsuccessful and the implant has been removed. 6 We would like to emphasize that the majority of the 13 participants had experienced occasional complications and a few had even experienced severe complications. For the purpose of this study we included patients with a unilateral amputation living in Sweden. This means we cannot assure that other aspects of the phenomena might be present among patients with OI-prostheses with bilateral amputations or those from other cultures. Moreover, only three of the 13 participants had an upper extremity amputation. However, the choice of participants in the study reflects to a high degree the current population of patients treated with OI-prostheses. Finally, it is clear that those treated with osseointegration so far constitute a highly selected group of patients. One could speculate that this has influenced their experiences of the phenomenon ‘living with an OI-prosthesis’.
Conclusion
All participants with OI-prosthesis in the present study reported radical improvements in terms of functional restoration and prosthetic use. The most important finding is that the meaning of that change went beyond the functional improvements, incorporating existential implications in the concept of quality of life. The future challenge is to find ways to capture changes in body image due to osseointegration treatment and to better understand the process of adjustment to improve the individual support to each patient.
Footnotes
Acknowledgement
The authors would like to thank all patients willing to share their thoughts and experiences with us.
Funding
This research was funded by ALF grant from the Sahlgrenska University Hospital, Gothenburg, Sweden.
Conflict of interest
The authors report not conflicts of interest. The authors alone are responsible for the content and writing of the paper.