
Abstract
Background:
Strength deficits may play a central role in the severity of balance, mobility, and endurance impairments in lower limb prosthesis users. A body of literature detailing the scope and specifics of muscle weakness in lower limb prosthesis users is emerging, but has yet to be summarized. A synopsis of strength deficits, and their impact on functional abilities in lower limb prosthesis users, may inform rehabilitation and research needs.
Objectives:
Synthesize reported strength deficits in lower limb prosthesis users, and discuss possible causes, consequences, and solutions.
Study Design:
Scoping review.
Methods:
A search of biomedical databases was performed, and inclusion/exclusion criteria were applied to identify publications relevant to the purpose of the review.
Results:
In all, 377 publications were identified, of which 12 met the inclusion/exclusion criteria. When compared with the controls and the intact limb, the primary strength outcome, peak torque, was lower in transtibial residual limb knee flexors and extensors, as well as transfemoral residual limb hip muscles.
Conclusions:
The reviewed studies provide evidence of strength deficits in lower limb prosthesis users. These deficits appear to be consequential, as they may contribute to balance, mobility, and endurance impairments. Additional research exploring alternative strength metrics, clinical tests, and causal links to functional impairments is required.
Clinical relevance
Evidence of muscle weakness among lower limb prosthesis users, and its influence on balance, mobility, and endurance, suggests that greater clinical attention and scientific inquiry into physical conditioning of lower limb prosthesis users is merited and required.
Introduction
Lower limb amputation has a substantial effect on an individual’s functional ability,1–4 as evidenced by the 26%–62% of lower limb prosthesis users who regain the ability to walk outdoors. 1 Among the functional challenges faced by lower limb prosthesis users, increased metabolic demand,5–7 decreased balance ability,8–12 decreased walking speed,13,14 increased stumbles and falls,12,15–17 reduced activity level,18,19 and difficulty ambulating on hills, stairs, or uneven terrain20–22 are frequently cited. A wide variety of prosthetic interventions are available and have been used with varying degrees of success,23–32 to address these balance, mobility, and endurance challenges. Nonetheless, functional challenges persist following lower limb amputation.
In addition to prosthetic design, there is emerging evidence that preserving and/or restoring pre-amputation strength levels may be essential to mitigating or preventing gait and balance deficits associated with lower limb amputation. For example, when matched for age and fitness, unilateral transtibial prosthesis users walk with a metabolic cost equivalent to that of people without lower limb amputation.33,34 Furthermore, regardless of prosthetic foot function (i.e. powered or passive), when pre-limb loss muscle strength was maintained in a musculoskeletal model of a transtibial prosthesis user, the metabolic cost of walking was not significantly different post-amputation. 35 In addition to reduced metabolic cost, 36 stronger muscles also appear to be related to better balance,37,38 as well as greater mobility and endurance 39 among lower limb prosthesis users. These studies suggest that lower limb strength may be a key determinant of balance, mobility, and endurance in lower limb prosthesis users. A comprehensive understanding of strength deficits among lower limb prosthesis users, and any related consequences on balance, mobility, and endurance will be central to further advances in rehabilitation of lower limb prosthesis users.
The body of evidence detailing the scope and specifics of muscle weakness in lower limb prosthesis users has yet to be summarized. This scoping review aims to address this gap in the literature by thoroughly summarizing differences in strength between the residual and intact limbs of people with lower limb amputation, and with respect to unimpaired adults. A comprehensive review of strength deficits among lower limb prosthesis users is critical to providing physiological targets for engineers, surgeons, physical therapists, and prosthetists to develop and implement more effective prosthetic components, surgical procedures, and therapies. This review will also serve to identify gaps in the current body of knowledge from which future research questions can be developed. The objective of this scoping review was, therefore, to synthesize reported strength deficits among lower limb prosthesis users, and discuss their possible causes, consequences, and potential solutions.
Methods
Literature search
A search of the literature in March of 2018 was performed using two bibliographic databases: PubMed (1949 to March 2018), and the Cumulative Index to Nursing and Allied Health Literature Expanded Index (CINAHL; March 1981–March, 2018). Keywords based on the population of interest, “amputee,” and outcome of interest, “strength,” were used in the search across both databases. The syntax used in both PubMed and CINAHL was (“amputee” AND “strength). Additional manuscripts were identified by searching the references of the initially identified publications.
Inclusion and exclusion criteria
Inclusion and exclusion criteria were applied to identify publications relevant to the stated purpose of the review. Only those publications, written in, or translated into, English, and published in peer-reviewed journals were considered (i.e. no dissertations, conference proceedings, White Papers). Only studies that directly compared the strength of the residual, intact, and/or control leg hip and knee muscles were included. Studies whose objective was to evaluate the effectiveness of an exercise or resistance training program were excluded from the results, but considered for later discussion. Studies that did not report results based on the level of amputation or present data in a manner that allowed for its extraction according to level of amputation were also excluded. No exclusion criteria based on the etiology or level of amputation was applied.
Screening and review of publications
To select publications pertinent to the objective of the review, the inclusion and exclusion criteria were applied to the search results by two of the authors (A.H. and A.S.). After removing duplicate publications identified in both databases, each article was screened based on its title, and removed if unrelated to the objective of the review. The contents of the abstracts were then reviewed for details regarding the population of interest (i.e. people with lower limb amputation), and the outcome of interest (i.e. strength). All remaining publications were then reviewed, with their results binned into muscle group (i.e. knee extensors, hip flexors) and level of amputation (i.e. transtibial, transfemoral).
Results
Literature search
The search strategy yielded 377 citations across the two databases; 32 of these publications were selected based on their title and 2 additional publications were added after searching the references of these initial 32 papers. After review of the abstracts, 12 of the 34 publications were found to meet the inclusion and exclusion criteria established for this review. The included publications were found to span the years 1968–2018. Of the 12 publications included for review, nearly 70% were published on or prior to 2002, while nearly 50% were published prior to 2000.
Study demographics and outcomes
Study sample sizes ranged from 7 to 38. The level of amputation studied was predominantly transtibial (i.e. 9 of the 12 studies, and 74% of all study participants; Table 1). The etiology of limb loss across studies was mainly non-dysvascular (i.e. 60% of study subjects). Knee flexor and extensor strength was the most studied outcome among transtibial prosthesis users (i.e. eight studies), while hip strength was the primary outcome in studies involving transfemoral prosthesis users (i.e. three studies). Strength of the tested muscle groups was primarily quantified using peak isometric torque (i.e. eight studies), and to a lesser extent, peak isokinetic torque (i.e. five studies). Only 3 of the 12 studies included a control group of non-lower limb prosthesis users.43,49,47 In each of these studies, lower limb prosthesis users were matched to non-lower limb prosthesis user controls based on a combination of age, sex, height and/or body mass index. None of the studies matched for underlying comorbidities such as dysvascular disease.
Characteristics of studied samples.
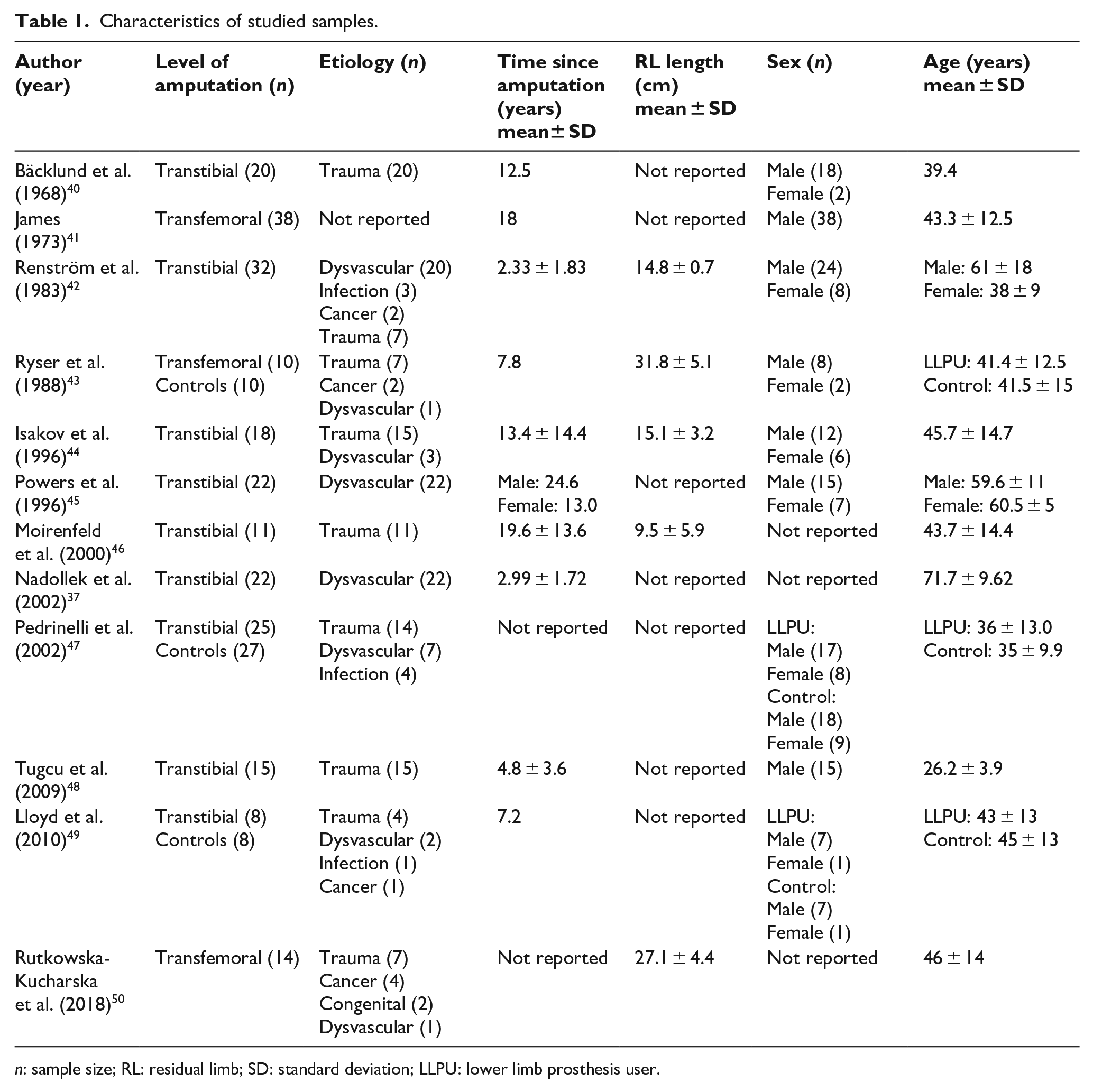
n: sample size; RL: residual limb; SD: standard deviation; LLPU: lower limb prosthesis user.
The reviewed studies offer evidence of strength deficits in people with lower limb amputation. Differences in isometric and isokinetic strength between the residual limb, intact limb, and controls are described below, and detailed in Tables 2 to 11. The percentage difference between legs is reported in the text, while study-specific torque values are provided in Tables 2, 3, 5, 6, and 9 for transtibial prosthesis users and Tables 4, 7, 8, 10, and 11 for transfemoral prosthesis users.
Summary of studies investigating knee flexor strength in unilateral transtibial prosthesis users.
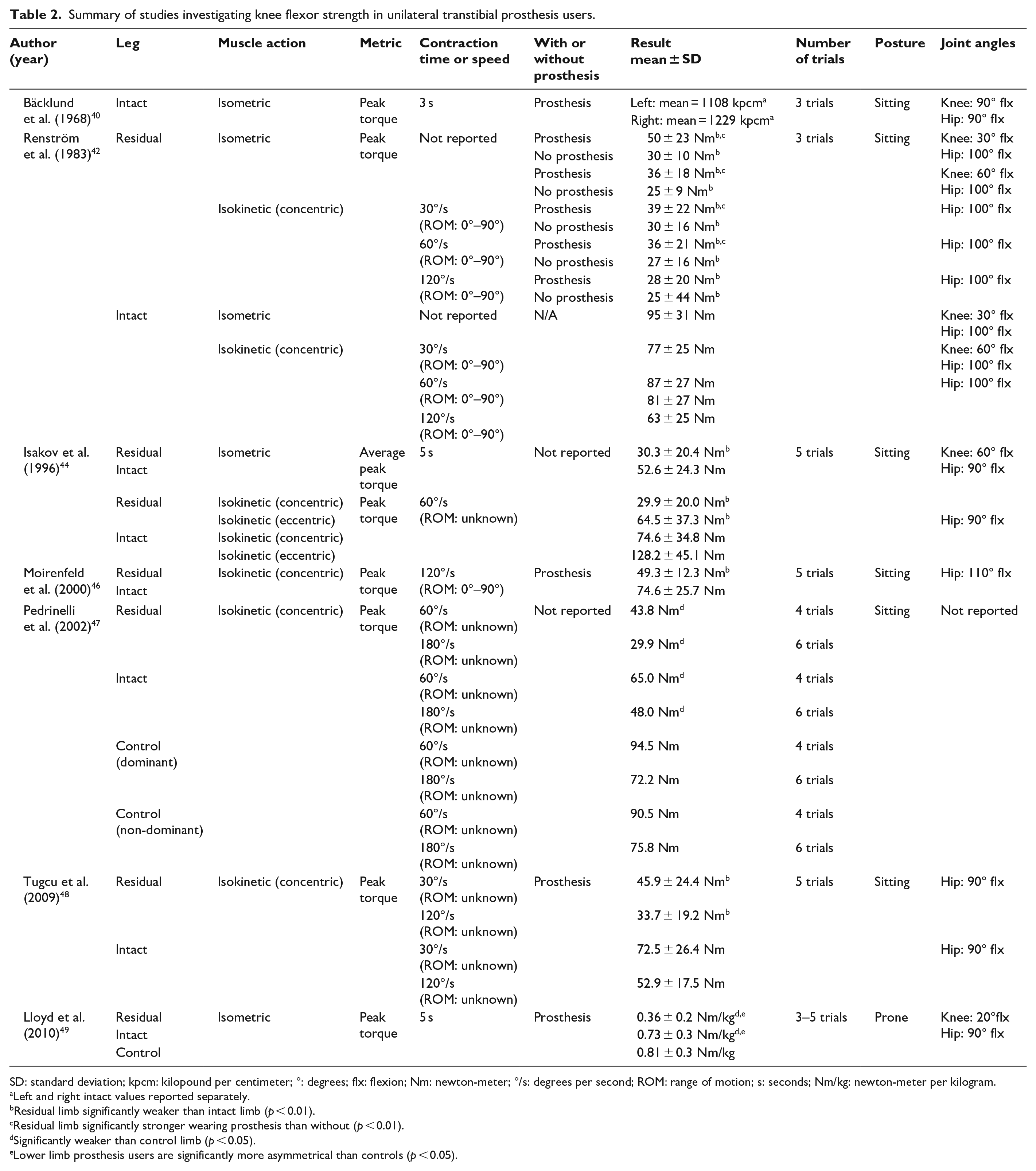
SD: standard deviation; kpcm: kilopound per centimeter; °: degrees; flx: flexion; Nm: newton-meter; °/s: degrees per second; ROM: range of motion; s: seconds; Nm/kg: newton-meter per kilogram.
Left and right intact values reported separately.
Residual limb significantly weaker than intact limb (p < 0.01).
Residual limb significantly stronger wearing prosthesis than without (p < 0.01).
Significantly weaker than control limb (p < 0.05).
Lower limb prosthesis users are significantly more asymmetrical than controls (p < 0.05).
Summary of studies investigating knee extensor strength in unilateral transtibial prosthesis users.
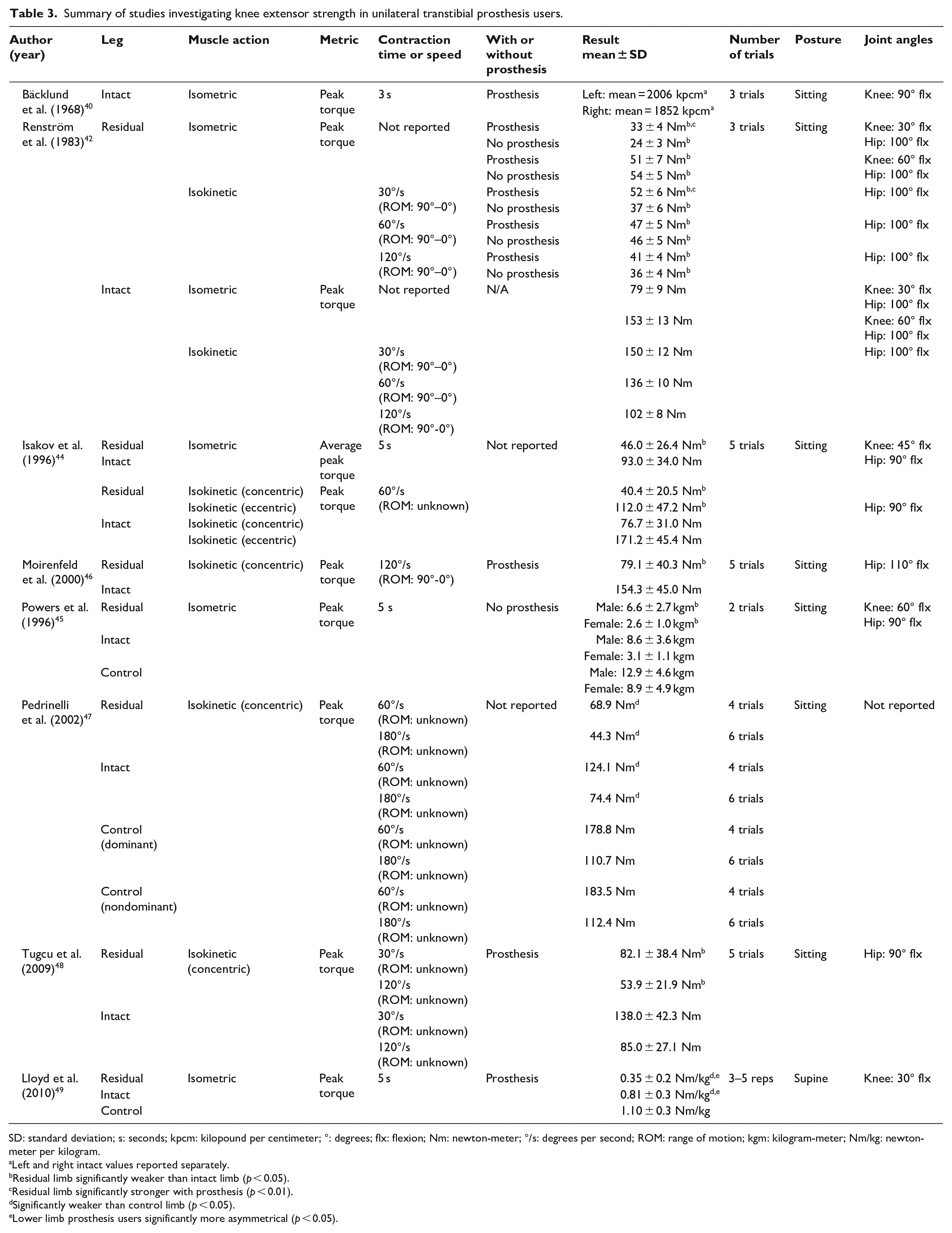
SD: standard deviation; s: seconds; kpcm: kilopound per centimeter; °: degrees; flx: flexion; Nm: newton-meter; °/s: degrees per second; ROM: range of motion; kgm: kilogram-meter; Nm/kg: newton-meter per kilogram.
Left and right intact values reported separately.
Residual limb significantly weaker than intact limb (p < 0.05).
Residual limb significantly stronger with prosthesis (p < 0.01).
Significantly weaker than control limb (p < 0.05).
Lower limb prosthesis users significantly more asymmetrical (p < 0.05).
Summary of studies investigating intact knee flexor and extensor strength in unilateral transfemoral prosthesis users.
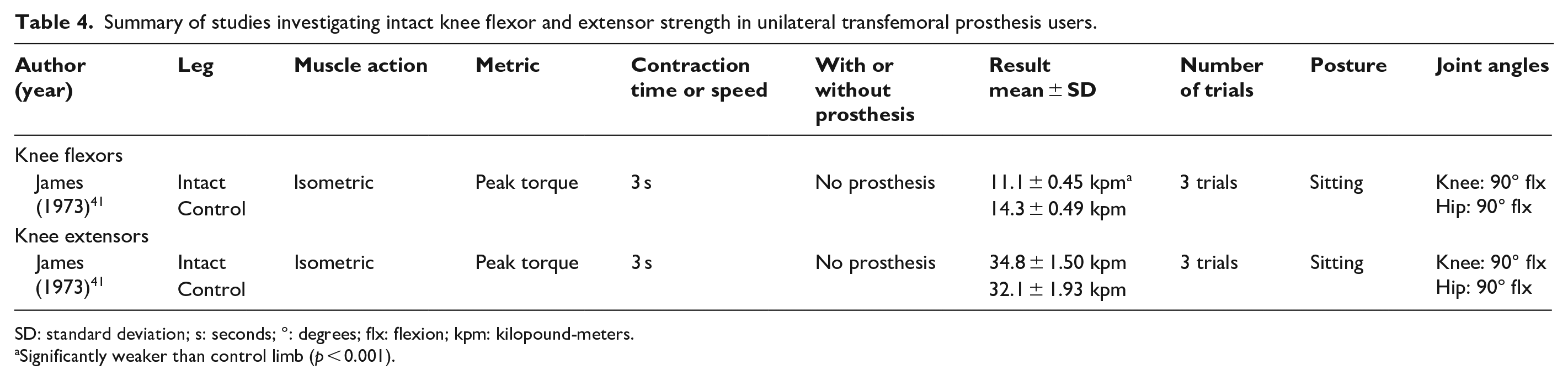
SD: standard deviation; s: seconds; °: degrees; flx: flexion; kpm: kilopound-meters.
Significantly weaker than control limb (p < 0.001).
Summary of studies investigating hip flexor strength in unilateral transtibial prosthesis users.
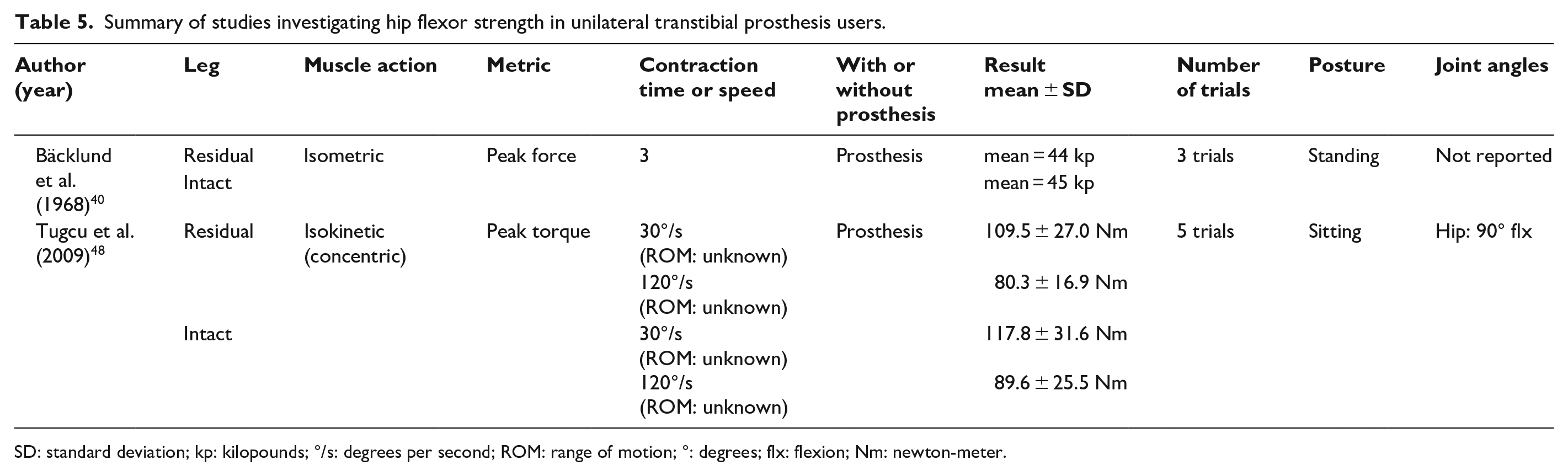
SD: standard deviation; kp: kilopounds; °/s: degrees per second; ROM: range of motion; °: degrees; flx: flexion; Nm: newton-meter.
Summary of studies investigating hip extensor strength in unilateral transtibial prosthesis users.
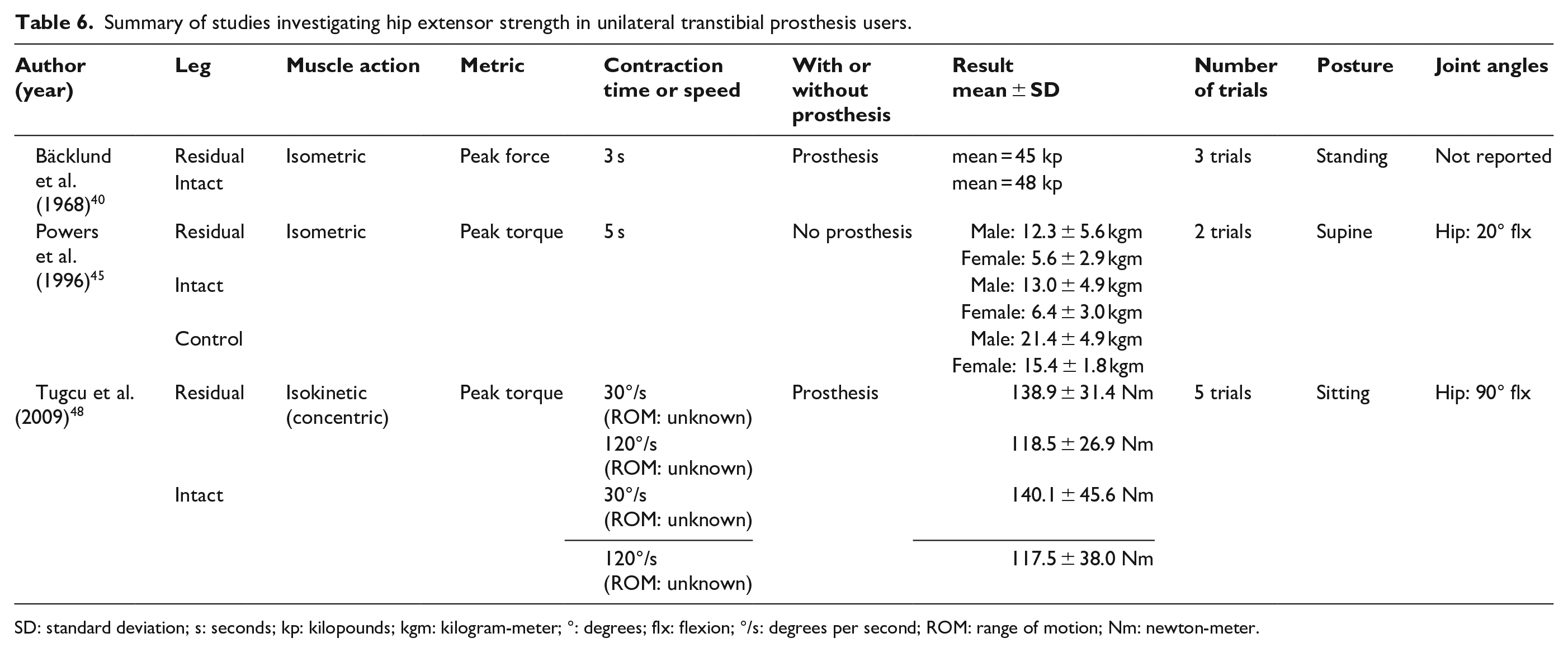
SD: standard deviation; s: seconds; kp: kilopounds; kgm: kilogram-meter; °: degrees; flx: flexion; °/s: degrees per second; ROM: range of motion; Nm: newton-meter.
Summary of studies investigating hip flexor strength in unilateral transfemoral prosthesis users.
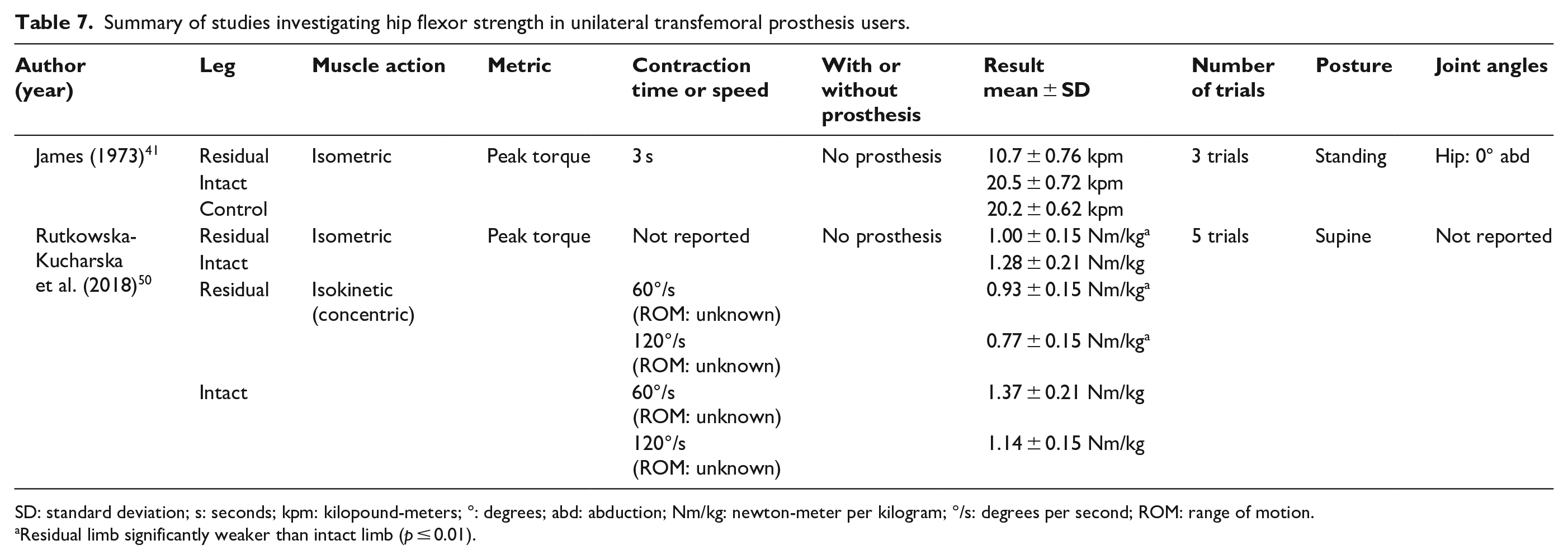
SD: standard deviation; s: seconds; kpm: kilopound-meters; °: degrees; abd: abduction; Nm/kg: newton-meter per kilogram; °/s: degrees per second; ROM: range of motion.
Residual limb significantly weaker than intact limb (p ≤ 0.01).
Summary of studies investigating hip extensor strength in unilateral transfemoral prosthesis users.
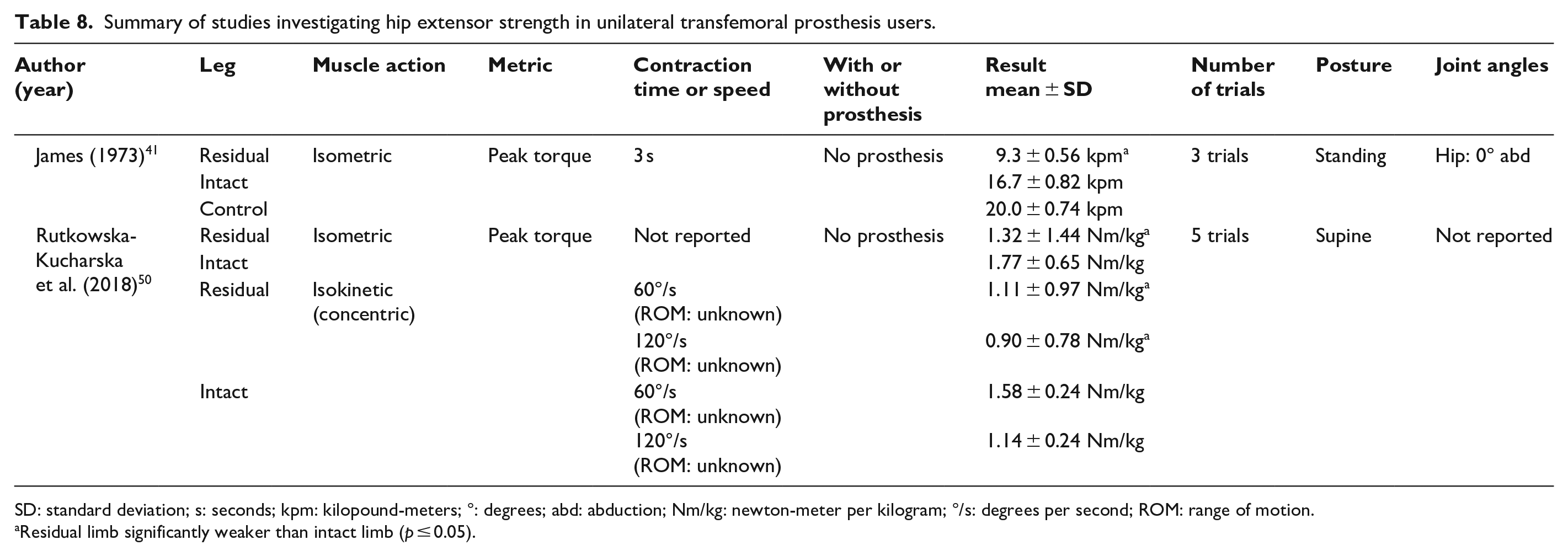
SD: standard deviation; s: seconds; kpm: kilopound-meters; °: degrees; abd: abduction; Nm/kg: newton-meter per kilogram; °/s: degrees per second; ROM: range of motion.
Residual limb significantly weaker than intact limb (p ≤ 0.05).
Summary of studies investigating hip abductor strength in unilateral transtibial prosthesis users.
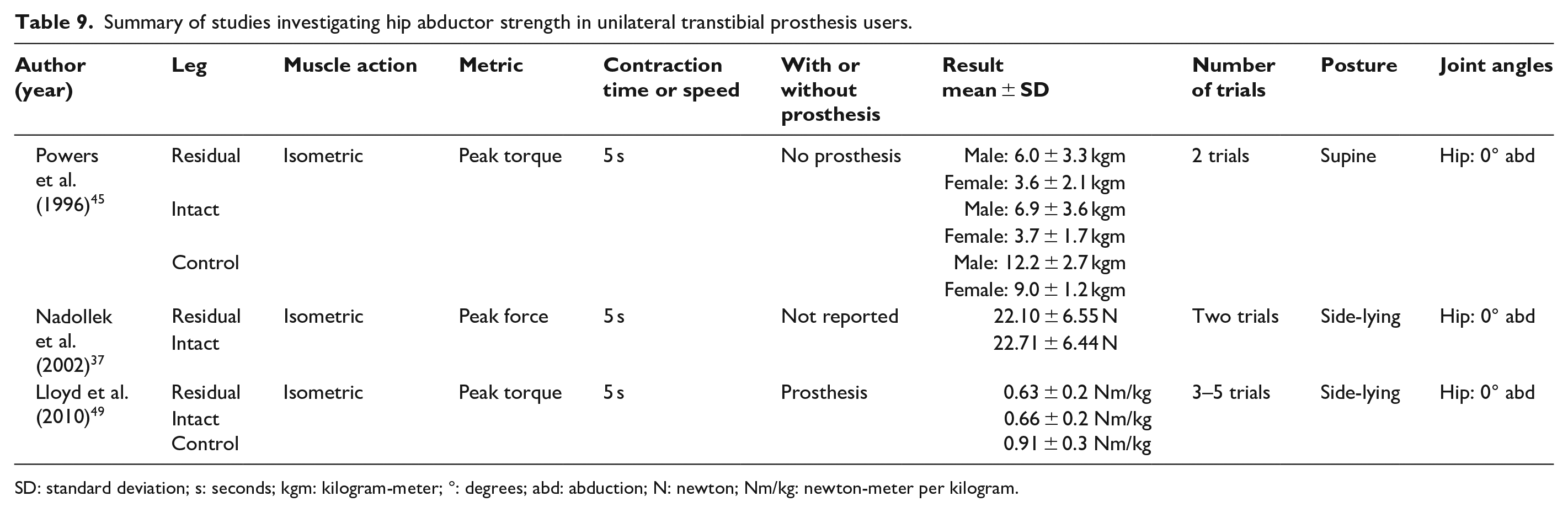
SD: standard deviation; s: seconds; kgm: kilogram-meter; °: degrees; abd: abduction; N: newton; Nm/kg: newton-meter per kilogram.
Summary of studies investigating hip abductor strength in unilateral transfemoral prosthesis users.
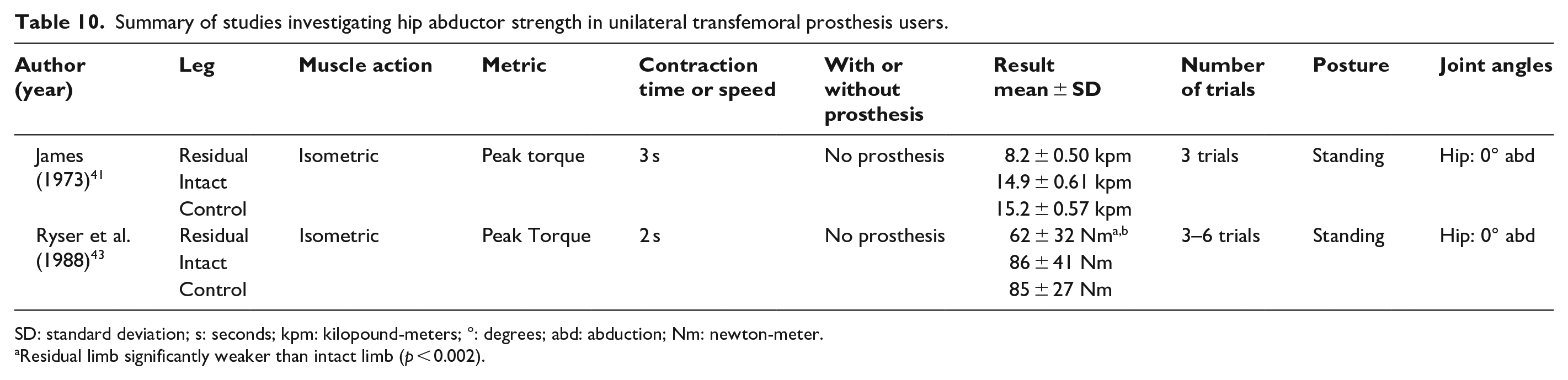
SD: standard deviation; s: seconds; kpm: kilopound-meters; °: degrees; abd: abduction; Nm: newton-meter.
Residual limb significantly weaker than intact limb (p < 0.002).
Summary of studies investigating hip adductor strength in unilateral transfemoral prosthesis users.

SD: standard deviation; s: seconds; kpm: kilopound-meters; °: degrees; abd: abduction; Nm: newton-meter
Residual limb significantly weaker than intact limb (p < 0.001).
Knee flexion and extension strength
There is evidence that across muscle actions (i.e. isometric37,40,41,43,45,49,50 and isokinetic42,44,46–48), test postures (i.e. seated,40,42,44–48 supine, 49 and prone 49 ) knee joint angles (i.e. 20°–90°40,42,44,45,49) and angular velocities (i.e. 30–180 °/s42,44,46–48), knee flexion and extension strength in the residual limb of unilateral transtibial prosthesis users are significantly lower than that of their intact leg or controls (Tables 2 and 3). There is less agreement, however, regarding deficits in knee flexion and extension strength in the intact limb of unilateral transtibial (Tables 2 and 3) and transfemoral prosthesis users (Table 4) compared with controls.
Residual versus intact limb
Seven studies (n = 8–32) compared knee flexion and/or extension strength between the residual and intact limb of unilateral transtibial prosthesis users42,45–49 (Tables 2 and 3). Peak isometric knee extension torque was reported to be between 57% and 70% lower in the residual limb than the intact limb.42,44,45,49 Three of those studies found this deficit to be statistically significant,42,44,45 while the fourth did not perform direct statistical comparisons. 49 Three of those same studies42,44,49 also reported that peak isometric knee flexion torque was significantly lower in the residual versus the intact limb of transtibial prosthesis users (i.e. 42%–68%). In addition to deficits in isometric knee strength, five studies found that across a range of angular velocities (i.e. 30–180°/s), peak concentric isokinetic knee flexion and extension torque were significantly lower in the residual limb than the intact limb of unilateral transtibial prosthesis users (flexion: 33%–60%, extension: 40%–75%).42,44,46,47 One study found peak eccentric isokinetic knee flexion and extension torque to be 50% and 35% lower, respectively, in the residual limb than the intact limb of unilateral transtibial prosthesis users. 44
Residual limb versus controls
Three studies (n = 8–25) compared residual limb knee flexion and/or extension strength with that of controls (Table 2).45,47,49 In each study, peak isometric knee flexion and extension torque was lower in the residual limb of unilateral transtibial prosthesis users compared with controls (i.e. flexion: 56% lower; extension: 49%–70% lower).45,49 Peak concentric isokinetic knee flexion and extension torque in the residual limb of unilateral transtibial prosthesis users was also significantly lower (i.e. flexion: 60%–62% lower; extension: 53%–60% lower) compared with controls (Tables 2 and 3). 47 Eccentric strength of residual limb knee muscles has yet to be assessed or compared with controls.
Intact limb versus controls
Six studies (n = 8–38) compared knee flexion and extension strength between the intact limb of people with unilateral lower limb amputation and controls.40,41,44,45,47,49 While there was a general consensus for strength deficits in the residual limb, findings were more variable when comparing the intact limb with controls. Bäcklund et al. 40 reported no marked difference between the intact limb of unilateral transtibial prosthesis users and controls in peak isometric knee flexion and extension force. The capacity of the intact limb to generate peak isometric knee flexion torque equivalent to that of controls was confirmed by a second study. 49 That same study however, 49 and one other, 45 found peak isometric knee extension torque generated by the intact limb of transtibial prosthesis users to be 26%–64% lower than that of controls.45,49 Regardless of angular velocity (i.e. 60°/s and 180°/s), peak concentric isokinetic knee flexion and extension torque was reported to be significantly lower in the intact limb of transtibial prosthesis users compared with controls (i.e. 23%-34% lower). 47 Eccentric strength of the intact limb knee muscles has yet to be compared with controls.
Hip strength
There is evidence that across muscle actions (i.e. isometric37,40,41,43,45,49,50 and isokinetic48,50), test postures (i.e. seated, 48 standing,40,41,43 supine,45,50 side-lying,37,49 and prone 51 ), hip joint angles (i.e. 0° of abduction,37,41,43,45,49 20° and 90° of flexion45,48), and angular velocities (i.e. 30–120°/s48,50), hip strength of transtibial prosthesis users does not differ significantly between their residual and intact limb, or with respect to control subjects (Tables 5, 6, and 9). In contrast, residual limb hip strength among unilateral transfemoral prosthesis users is significantly lower than in their intact limb (Tables 7, 8, 10, and 11). To date, there is limited data characterizing differences in hip flexion, extension, or adduction strength between transfemoral prosthesis users and controls, or in hip abduction strength among transtibial prosthesis users.
Hip flexion and extension
Residual versus intact limb
Three studies (n = 15–22) have compared hip flexion and/or extension strength between the residual and intact limb of transtibial prosthesis users (Tables 5 and 6).40,45,48 Two studies (n = 14 and 38) have done the same among transfemoral prosthesis users (Tables 7 and 8).41,50 Regardless of muscle action (i.e. isometric or isokinetic), peak hip flexion and extension torque or force were not significantly different between the residual and intact limb of transtibial prosthesis users (i.e. 0%–12% lower) (Tables 5 and 6).40,48 In contrast, among transfemoral prosthesis users, peak isometric and isokinetic hip flexion and extension torque were substantially lower in the residual versus intact limb.41,50 Peak residual limb isometric and isokinetic hip extension torque was between 25%–43% and 21%–30% lower than the intact limb, respectively,41,50 while residual limb peak isometric and isokinetic hip flexion torque was between 22%–47% and 36% lower than the intact limb, respectively.41,50
Residual and intact limb versus controls
There is some disagreement as to whether hip extension strength differs between transtibial prosthesis users and controls. Bäcklund et al. 40 reported that neither residual nor intact limb peak isometric hip extension force differed between transtibial prosthesis users and controls (i.e. residual limb: 2% lower; intact limb: 4% higher). 40 In contrast, Powers et al. 45 reported much larger deficits in peak isometric hip extension torque in the residual limb (41%–64% lower) and intact limb (i.e. 39%–58% lower) compared with controls. 45 Differences in hip flexion strength between transtibial prosthesis users and controls have not been assessed. There is also limited data concerning differences in hip flexion and extension strength between transfemoral prosthesis users and controls. In a single study of 38 unilateral transfemoral prosthesis users, peak isometric hip extension and flexion torque were 5% and 20% higher in the intact limb than controls. 41 Residual limb values were 47% and 53% lower than controls. 41
Hip adduction and abduction
Residual versus intact limb
Three studies (n = 8–22) have tested hip abduction strength among transtibial prosthesis users (Table 9),37,45,49 while two (n = 10–38) have examined hip abduction strength among transfemoral prosthesis users (Table 10).41,43 Hip adduction strength, however, has only been evaluated in a single study of transfemoral prosthesis users (Table 11). 41 Among unilateral transtibial prosthesis users, peak isometric hip abduction torque was not significantly lower in their residual versus intact limb (i.e. 3%–13% lower).37,45,49 In contrast, among transfemoral prosthesis users, peak isometric hip abduction torque was significantly lower in their residual versus intact limb (i.e. 33%–46% lower).41,43 Data to support similar differences in hip adduction strength among lower limb prosthesis users are limited to a single study of transfemoral prosthesis users that found residual limb peak isometric hip adduction torque to be significantly lower than in the intact limb (i.e. 47% lower). 41
Residual and intact limb versus controls
Regardless of amputation level, and despite sizable differences in magnitude, neither residual nor intact limb hip adduction nor abduction strength differed significantly with respect to controls (Tables 9 to 11). Peak isometric hip abduction torque in the residual and intact limbs of unilateral transtibial prosthesis users were lower (i.e. 31%–60% and 27%–59%, respectively), but not significantly different from controls.45,49 Similarly, neither residual nor intact limb peak isometric hip abduction torque of transfemoral prosthesis users differed significantly from controls (residual limb: 29% lower, intact limb: 1%–20% lower).43,45 Peak isometric hip adduction torque in the residual limb of transfemoral prosthesis users is the lone exception, being significantly lower compared with controls (i.e. 68% lower). 41
Additional strength measures
Beyond peak torque, other measures have been used, albeit sparingly, to characterize strength deficits in lower limb prosthesis users. Pedrinelli et al. 47 reported that among transtibial prosthesis users, the isokinetic work performed by residual limb knee flexors and extensors was substantially lower than that generated by their intact limb (i.e. extensors: 42%–46%, flexors: 25%–34% lower). Similarly, residual and intact limb knee flexion and extension work were lower than that of controls (i.e. residual limb extensors: 61%–63% lower, residual limb flexors: 57%–60% lower; intact limb extensors: 31%–36%, and intact limb flexors: 33%–46% lower). Similar differences were reported for joint power (i.e. the rate of doing work). 47 Moirenfeld et al. 46 used the percentage difference in total work between the last 10 and the first 10 repetitions to evaluate muscular endurance. Among a sample of 11 traumatic transtibial prosthesis users, residual limb knee flexors had significantly greater endurance than intact limb knee flexors (i.e. 23% more fatigue resistant), while knee extensor endurance did not differ between the residual and intact limb. 46 Differences in fatigue resistance between lower limb prosthesis users and controls remain untested.
Discussion
The objective of this scoping review was to synthesize reported strength deficits in lower limb prosthesis users, discuss their potential causes, consequences, and possible solutions, while highlighting gaps and suggesting future research directions. Among transtibial prosthesis users, muscle weakness appears to be the most prominent among residual limb knee flexors and extensors when compared with the intact limb or controls. Muscle weakness among transfemoral prosthesis users is the most prominent in the hip of their residual limb with respect to the intact limb. These between-limb differences exceeded a 10% bilateral deficit cited as the norm for controls, 52 and frequently exceeded a 20% threshold often cited as abnormal in other patient populations. 53 Below, we discuss the potential explanations, interpretations, and consequences of the reported strength deficits, and whether strength deficits in people with lower limb amputation are modifiable.
Amputation-, demographic-, and activity-related factors may contribute to muscle weakness in lower limb prosthesis users
Strength deficits among people with lower limb amputation appear related to several amputation, demographic, and activity-related factors. Among amputation-related factors, a shorter residual limb, dysvascular etiology, and certain aspects of the amputation procedure have been associated with reduced residual limb strength in lower limb prosthesis users. Peak isokinetic torque and maximal average isometric torque are significantly lower in people with transtibial amputation when the residual limb is shorter than 15.1 cm. 54 Similarly, hip strength on the amputated side is positively correlated to the length of the residual limb among transfemoral prosthesis users. 41 Specifically, peak extension and abduction torque weakly correlated to residual limb length (r = 0.41 and 0.44, respectively), while flexion and adduction torque moderately correlated to limb length (r = 0.50 and 0.60, respectively). 41 The higher correlations between residual limb length and hip adduction and flexion torque might be expected, as hip flexor and adductor muscles are both transected during transfemoral amputation.
The impact of a shorter residual limb on muscle strength may be offset by properly tensioning the muscles transected during an amputation. 55 Using a musculoskeletal simulation, Ranz et al. 55 found that preserving muscle tension following transfemoral amputation had the single greatest impact on a muscle’s force-generating capacity, to the point that femur length had little effect. Other features of transfemoral amputation, including muscle wrap orientation, has less impact on the force-generating capacity of residual hip muscles. 55 Disruption of the insertion of the iliotibial band during transfemoral amputation may also contribute to hip abductor weakness in people with transfemoral amputation. 43 The tensor fascia lata is believed to assist in hip abduction through its insertion in the iliotibial band.56,57 Thus, if the iliotibial band is not appropriately anchored following transfemoral amputation, the potential contribution of this muscle is reduced.
Time since amputation does not appear to play a substantial role in lower extremity weakness among lower limb prosthesis users. Isakov et al. 44 found no significant difference in isometric or isokinetic knee flexion or extension strength between transtibial prosthesis users less than or greater than 7 years post-amputation. The main effects of amputation on muscle strength may therefore occur in the years immediately following surgery. 44 Similarly, Croisier et al. 58 found that variation in time since amputation did not affect peak isokinetic hip torque among transtibial prosthesis users, and Pedrinelli et al. 47 reported that time since amputation was not a significant factor related to knee strength.
A single study directly compared lower extremity strength of dysvascular and non-dysvascular lower limb prosthesis users. Renström et al. 42 found that isometric and isokinetic strengths in the intact and residual limb were significantly lower in people with transtibial amputation due to peripheral vascular disease and diabetes than traumatic causes. The results of this study suggest that when interpreting strength values among dysvascular lower limb prosthesis users, we are looking at not only the impact of amputation, but also that of the underlying disease. A direct assessment of the impact of amputation alone on strength could be accomplished by limiting study samples to traumatic lower limb prosthesis users, as was done in 3 of the 12 studies.40,46,48 Alternatively, selecting controls who are also dysvascular would control for the impact of the disease. This was not done, however, in any of the studies that included dysvascular lower limb prosthesis users. The current body of literature may therefore be skewed toward greater strength deficits when the cause of amputation is dysvascular.
Demographic-related factors
Strength in lower limb prosthesis users appears related to age and sex. In people with transtibial amputation, isometric, as well as isokinetic knee flexion and extension strength decreased with increasing age both with and without a prosthesis. 42 Hip abductor strength has also been reported to negatively correlate with age (i.e. r = −0.539). 37 In a conflicting result, Pedrinelli et al. 47 found that age was not a significant factor related to isokinetic knee flexion or extension torque among transtibial prosthesis users. However, the subjects in that study were younger than those in the other two studies (see Table 1), with subjects ranging from 12 to 59 years of age with a mean age of 35.9 years. 47
Powers et al. 45 measured the isometric hip, knee, and ankle strength of female and male transtibial lower limb prosthesis users. Although direct statistical comparisons were not made, female prosthesis users had consistently lower strength than males (Table 2). 45 Women also demonstrated a larger difference between the residual and intact limb than men (i.e. 60% vs 23%). 45 Similarly, Renström et al. 42 found that residual limb isokinetic knee extension strength was lower among female transtibial prosthesis users than males (i.e. 45% lower).
Activity-related factors
Decreased activity prior to and after amputation may also contribute to weakness in the lower limbs. In a study of isometric and isokinetic strength in transfemoral prosthesis users, the etiology of weak residual limb hip abductors was believed to be deconditioning due to decreased use before and following amputation. 43 This disuse may be due to a decrease in ambulation and activity in general. Among transtibial prosthesis users, greater hip abductor strength is positively correlated with greater time spent wearing the prosthesis per day (r = 0.576). 37
Strength deficits among lower limb prosthesis users are consequential
There is evidence that lower muscular strength among lower limb prosthesis users contributes to mobility and health impairments. Specifically, changes in gait,37,40,42,45 reductions in energy efficiency 35 and walking endurance, 59 altered joint loading,37,50 as well as increased risk of knee osteoarthritis and low-back pain have been linked to deficits in lower extremity strength among lower limb prosthesis users.49,60
The strength of residual limb muscles appears critical to several aspects of mobility among lower limb prosthesis users. First, both preferred (r = 0.50–0.61)37,45 and fast (r = 0.30–0.72)42,45 walking speeds of transtibial prosthesis users are positively correlated to peak isometric hip extension, 45 hip abduction, 37 as well as knee flexion and extension torque in the residual limb. 42 Second, decreases in walking speed associated with a loss of residual limb strength appear to be attributable to shorter step and stride lengths, which in turn decrease with peak residual limb knee flexor (r = 0.46–0.52) 42 and extensor (r = 0.53–0.71) torque, 42 as well as hip abductor torque (r = 0.63). 37 In addition to walking speed, deficits in muscle strength also appear to impact walking endurance among transtibial and transfemoral prosthesis users. Among a host of variables (i.e. demographics, time since amputation, etiology, and level), residual limb hip extensor strength, followed by hip abductor strength, were the greatest predictors of walking endurance (i.e. 6-min-walk test distance) among lower limb prosthesis users (i.e. r = 0.69, 0.66 respectively). 59 Further, transtibial prosthesis users who were unable to walk 1 km had lower residual limb peak hip extension force than non-amputee controls. 40
Reductions in walking speed among lower limb prosthesis users have historically been attributed to an increased metabolic cost of locomotion. 61 The extent to which this increase is caused by lower muscular strength is controversial. 47 Recent evidence, however, suggests this may be the case. In a musculoskeletal simulation of walking, when pre-limb loss muscle strength was maintained, metabolic cost did not increase above pre-limb loss cost. 35 In addition, when matched for age and fitness, transtibial prosthesis users tend to walk with a metabolic cost that is equivalent to that of controls.33,34 Together, these results imply that strength, and specifically residual limb strength, plays a major role in offsetting increases in metabolic cost typically associated with lower limb amputation.
Lower limb prosthesis users are at risk for loading asymmetries between their intact and residual limbs that can introduce secondary disabilities. Increased loading of the intact limb is positively correlated with asymmetries in hip extensor strength among transfemoral prosthesis users, 50 and hip abductor strength among transtibial prosthesis users. 37 Several asymmetric loading patterns observed among transtibial prosthesis users 62 have been linked to degenerative changes in the knee (i.e. knee adduction moment load rate and maximum vertical ground reaction force load rate). 60 Asymmetries in peak isometric knee flexor and extensor torque (i.e. lower residual limb values) are correlated with these load rate variables (r = 0.64–0.71). 49 The loss of muscular strength among lower limb prosthesis users may therefore not only limit gait performance, but also introduce loading patterns that increase susceptibility to degenerative joint disease.
Strength deficits in lower limb prosthesis users appear to be modifiable
Given their consequences, it is essential to know whether, to what extent, and through what methods, strength deficits in lower limb prosthesis users may be best resolved. A variety of resistance and exercise training programs have shown promise in resolving strength deficits in transtibial38,51,63–65 and transfemoral prosthesis users.36,38,51,66 Increases in muscle size, muscle strength, and/or functional performance have been reported across training programs. This suggests that strength deficits, and their consequences, are amenable to modification among lower limb prosthesis users.
A variety of frequencies, intensities, durations, and types of training have been studied. Exercise types have included isometric 64 and isokinetic 65 strength training, as well as general exercise (i.e. cycling, weight lifting circuit, and walking).36,38,51,66 Training duration has varied between 8 and 12 weeks, frequency from twice a day 64 to two or three times a week,38,65 while the intensity of training has also fluctuated between studies (e.g. 25 contractions, 64 2 sets of 10 repetitions, 65 3 sets of 10 repetition max). 36 Interestingly, four studies implemented training programs that were in part or in whole performed at home,38,51,64,66 suggesting that barriers to facilities and access to equipment can be overcome. Study samples, while small (n = 4–17), included both transtibial (n = 21) and transfemoral prosthesis users (n = 41), varied amputation etiology (i.e. dysvascular and non-dysvascular), as well as average age (37.5–67.8 years) and time since amputation (2.5–19 years).36,38,51,63–66 This suggests that a number of key demographic and amputation-related characteristics may not pose as limiting of factors in addressing strength deficits among lower limb prosthesis users. Further research is required to identify barriers and facilitators to exercise among lower limb prosthesis users.
All training programs, regardless of frequency, intensity, time, or type of training were effective in reducing strength deficits and/or their functional consequences. Evidence of changes in muscle structure and size varied. While no changes in fiber composition were reported, 65 the mean cross-sectional area of residual limb knee extensor muscle fibers increased. 65 This, however, did not translate to an overall increase in size (i.e. thigh circumference) or cross-sectional area of the knee extensors. 65 In contrast, Kegel et al. 64 reported an increase in the cross-sectional area of the gastrocnemius muscle of the residual limb among transtibial prosthesis users following isometric strength training. Strength, largely measured via peak torque, increased in both residual and intact limb muscles between 11% and 22%.36,51,65,66 These strength gains translated to improvements in mobility (i.e. walking speed, Timed Up and Go performance),36,38 walking endurance (i.e. 2-min-walk test distance, walking distance),36,65 balance (i.e. reduction in falls, improved balance confidence),36,38 and gait (i.e. reduced asymmetry and increased propulsion).38,66 Despite these initial successes addressing strength deficits in lower limb prosthesis users, a number of needs remain. Namely, there are no specific recommendations for strength training of lower limb prosthesis users (i.e. which muscles, which deficits, timing post-amputation), 36 sample sizes were small, and more focused comparisons of specific training regiments are required.
Gaps and directions for future research
There is limited data characterizing differences in hip strength among lower limb prosthesis users and controls. With the importance of hip muscle function in lower limb prosthesis users,67–69 additional research is warranted.
Functional strength measures and assessments have, to date, been limited in large part to non-fatiguing conditions and measures of maximum voluntary strength. Important functional aspects of strength including the rate of force development, which is essential to balance,70–72 and muscular endurance, which is crucial to mobility46,73 have been overlooked. Additional research exploring these and other measures of strength, and their relationship to clinical strength tests (e.g. 5-times Sit to Stand) is necessary to advance our understanding of how amputation affects strength, and to identify or develop quick, simple, inexpensive, and valid clinical tests of strength tailored to lower limb prosthesis users. There was considerable variation in the methods used among the reviewed studies to test muscle strength in lower limb prosthesis users. Such variation makes it difficult to compare between studies. As such, working toward a common set of recommended methods would increase the consistency of reporting and facilitate greater comparisons between studies.
Muscle weakness has been associated with a number of functional challenges among lower limb prosthesis users including gait abnormalities,74,75 secondary degenerative disorders (e.g. joint degeneration), 76 increased metabolic cost of gait,35,39 and balance confidence. 36 Causal links, however, between muscle function and balance, mobility, or endurance among lower limb prosthesis users remain poorly understood. 1 Additional research is therefore needed to address this gap and help identify those muscles most closely associated with these functional challenges.
Conclusion
The reviewed studies provide evidence of strength deficits in lower limb prosthesis users. These deficits appear to be consequential, contributing to balance, mobility, and endurance impairments. Fortunately, preliminary studies have found these deficits to be modifiable, responding to an assortment of physical conditioning training programs. Additional research exploring alternative strength metrics, clinical tests, training program parameters, surgical procedures, and causal links to functional impairments is required.
Footnotes
Author contribution
The study concept and design were created by A.H. and A.S., acquisition of data was done by A.H., analysis and interpretation of data was carried out by A.H., S.D., and A.S., drafting of the manuscript was done by A.H., critical revision of the manuscript of important intellectual content was taken care of by S.D. and A.S., and study supervision was conducted by A.S.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Department of Defense under Award No. W81XWH1910507. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Department of Defense.