
Abstract
Background:
Few studies have explored the effects of exercise on gait performance in people with lower limb amputations.
Objectives:
To (1) summarize the effects of exercise programs on gait performance and (2) assess the overall quality of the evidence for adults ambulating with leg prostheses.
Study design:
Systematic review.
Methods:
Six databases were searched for one- and two-group studies published through June 2013 reporting effects of exercise on gait speed, a universal measure of performance in lower limb prosthetic users. The search adhered to a predetermined protocol following Cochrane Collaboration guidelines.
Results:
In all, 623 citations were reviewed and eight studies included. The quality level of the combined evidence was low with few randomized control trials and multiple sources of bias evident within the heterogeneous group of studies. The 11 exercise programs, including three control conditions, demonstrated small to large effect size improvements in self-selected gait speed. Use of exercise to improve gait speed was supported by low-quality level evidence, with low–moderate quality evidence to suggest that specific functional exercise programs were more effective than supervised walking.
Conclusion:
Using exercise to improve gait speed in people with lower limb amputation received a B grade recommendation. Future high-quality research is required.
Clinical relevance
Supervised walking, muscle strengthening, balance exercises, gait training, and functional training programs demonstrated small to large effect size gait performance improvements in people with lower limb amputation. Self-selected gait speed was the most consistent outcome measure. Exercise programs emphasizing resisted gait and functional training were more effective than supervised walking.
Background
Rehabilitation after lower limb amputation, once wound healing has been achieved, generally focuses on use of the prosthesis to restore walking ability. 1 A team approach after amputation may include initial prosthetic training with a prosthetist at the time of delivery and continued prosthetic training to optimize gait performance with a physiotherapist. 2 Physiotherapy includes varying degrees of emphasis, exercise, balance, gait, and functional training within an overall comprehensive plan of care. 1 However, no evidence-based best practice guideline for physiotherapy after lower limb amputation has been established, to the authors’ knowledge.
Physiotherapy in general and the specific exercise programs provided during rehabilitation vary with the rehabilitation settings and individual clinical presentations. For people after lower limb amputation, medical complications can delay readiness for prosthetic fitting 3 and prolong the rehabilitation process. 4 Delayed rehabilitation and the trend toward shorter hospital stays result in physiotherapy being conducted in a variety of settings including hospitals and rehabilitation centers but increasingly out-patient clinics and individual homes.5,6 In addition to the rehabilitation setting, other variables that influence the rehabilitation process include medical conditions and clinical characteristics such as age, amputation etiology, and amputation level. 2 Many of these variables, although beyond the control of the individual and clinician, can affect the rehabilitation process and outcome. Thus, modifiable variables such as the exercise program selected to optimize gait performance could have an important impact on the rehabilitation of the individual after lower limb amputation. 7
Clinicians have used a multitude of exercise approaches in amputation rehabilitation 8 as well as methods to assess gait performance, including kinetic, kinematic, functional, and self-report measures. 9 Perhaps, the simplest and most universal gait measure, gait speed has been suggested as a vital sign for screening physical performance. 10 Gait speed has demonstrated responsiveness to change in short bouts of rehabilitation 11 and strong correlation to gait indices that incorporate motion analysis measures of prosthetic gait deviations compared to the intact limb to differentiate gait performance abilities. 12 Beyond the ability to walk a short distance; 13 successful prosthesis use in a community setting requires sufficient ability to walk fast enough to cross a street or engage in other outdoor or functional activities that facilitate a return to vocational and recreational pursuits. 14
Few reports of specific exercise programs after lower limb amputation exist and no prior systematic reviews of specific exercise training programs to improve gait performance were identified. The purpose of this systematic review was to (1) summarize and assess the effects of exercise programs on prosthetic gait performance in people with lower limb amputations and (2) assess the overall quality of the combined evidence.
Methods
This systematic review adhered to a predetermined study protocol following the Cochrane Collaboration recommendations with the process reported per the PRISMA statement for reviews that evaluate healthcare interventions.15,16
Study inclusion and exclusion criteria
Inclusion criteria are as follows:
Experimental and quasi-experimental designs including one-group cohort and pre–post studies, and two-group case–control, and control trials.
Participants: prosthesis users at least 16 years of age with any unilateral or bilateral lower limb amputation level above the ankle, such as transtibial and transfemoral.
Intervention: experimental exposure conditions that emphasized exercise.
Outcomes: gait speed was the primary outcome measure. Other temporal, spatial, kinetic, and kinematic gait measures were noted.
Exclusion criteria are as follows:
Designs including case studies and case series with fewer than three subjects;
Participants who did not use prostheses and able-bodied individuals;
Interventions based on initiating prostheses or changing prosthetic components;
Outcome measures limited to those that could not be converted to gait speed;
Reporting not in English.
Search strategy
The following databases were searched to identify relevant systematic reviews and studies without language restrictions or time limits through June 2013: Cochrane, DARE, Ovid MEDLINE, PEDro, PubMed, and Web of Knowledge. The search strategy was based on Boolean combinations of the search terms “amputation,” “prostheses,” “muscle strength,” “exercise,” “postural balance,” “training,” “education,” “rehabilitation,” with “gait.” Other potential studies for inclusion were identified by hand searches of the reference lists of all included articles.
Study selection and data extraction
After duplicates were removed, two reviewers independently screened all citations and abstracts to identify studies potentially eligible for inclusion. The full texts of all potentially eligible studies were independently reviewed by four reviewers using a study eligibility form. Final study selection was based on consensus discussion. Data extraction for the included studies was facilitated by use of a customized data extraction checklist combined with the standard GATE-lite form for randomized control trials, adapted from the Graphic Appraisal Tool for Epidemiological studies, to ensure consistent documentation of relevant study data in PECOT format (Participants, Experimental condition, Comparison condition, Outcome, and Time) and potential bias risks in RAMBO format (Recruitment, Allocation, Maintenance, Blinding, and Objective outcomes). 17 Any disagreement regarding potential study eligibility, final inclusion, or the extracted data was resolved through consensus discussions and if necessary adjudication by an additional reviewer, although this was not required.
Study data summary and analysis
Study data including study design, sample size, experimental and comparison conditions, and gait outcome data were compiled and summarized. The primary outcome measure assessed was gait speed. Reported treatment effects on gait speed including mean differences with standard deviations and p-values were aggregated. Missing data, effect sizes, and percent changes were calculated when possible from data reported in the included studies. Secondary outcome measures were summarized, including kinematic data, multidimensional gait measures, and self-report outcomes. Study heterogeneity was expected and analyzed qualitatively.
Study quality assessment
Each study was assessed using the Cochrane Collaboration Risk of Bias tool for potential study bias in the domains of selection, performance, detection, attrition, reporting, and other bias. While quantitative assessment of study quality is common, the Cochrane Collaboration handbook explicitly discourages numeric rating of study quality due to the arbitrary weighting of scale items, the difficulty of distinguishing between incomplete reporting and study bias, and unreliable assessments of validity for numeric rating scales. 16 Risk of bias in each domain was assessed as high, low, or unclear (when reporting left unclear whether specific potential biases had been addressed). Each study was then potentially downgraded or double downgraded based on study biases. 16 Rating in this way allowed a level of evidence for each study to be assigned by consensus according to the 2001 Oxford Levels of Evidence chart for comparison to other studies rated. 18
Overall evidence quality assessment
The overall quality of the evidence was assessed using the Cochrane GRADE system 16 as high-, moderate-, low-, or very low-quality evidence based on the level of evidence of the combined studies and consideration of biases in five domains: study design, indirectness of the evidence, unexplained study heterogeneity or inconsistency, imprecise results, and probability of publication bias. 16
Results
The search strategy resulted in 623 article citations for potential inclusion after removing duplicates. As of June 2013, no systematic reviews regarding the effect of exercise on gait performance in people with lower limb amputations were identified. In all, 589 articles were excluded after review of the titles and abstracts and consideration of the inclusion and exclusion criteria. The full texts of the remaining 34 articles were reviewed with 26 additional studies excluded. Overall, 615 articles were excluded for reasons listed in the Systematic review flow chart (Figure 1). The eight included studies, the oldest from 1981, were conducted in North America, Sweden, Republic of Slovenia, Turkey, and Myanmar (Table 1). The studies varied in design, participants, experimental and comparison condition exposures, and outcomes described separately in short summary findings.
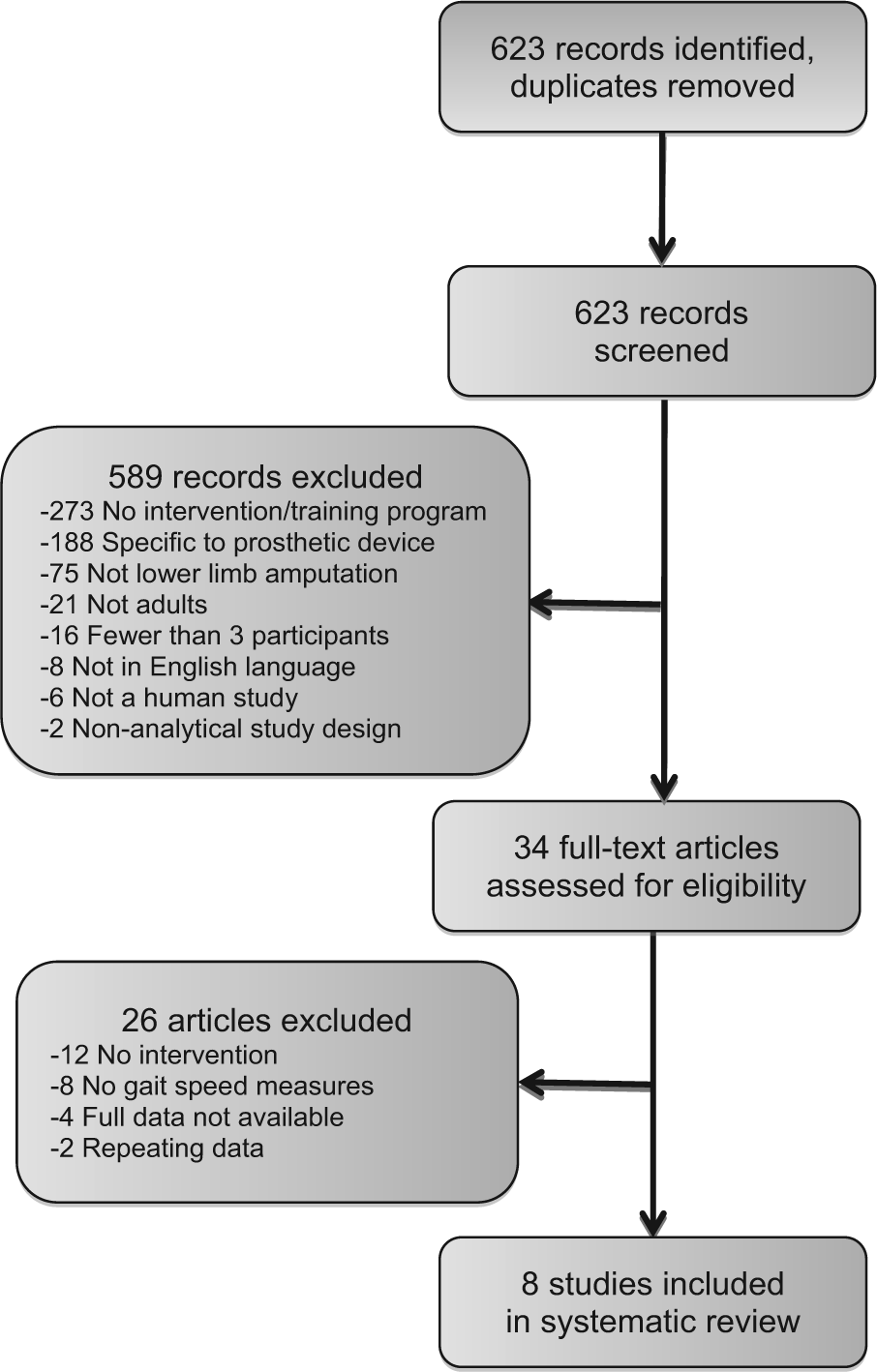
Systematic review flow chart.
Descriptive data for included studies.
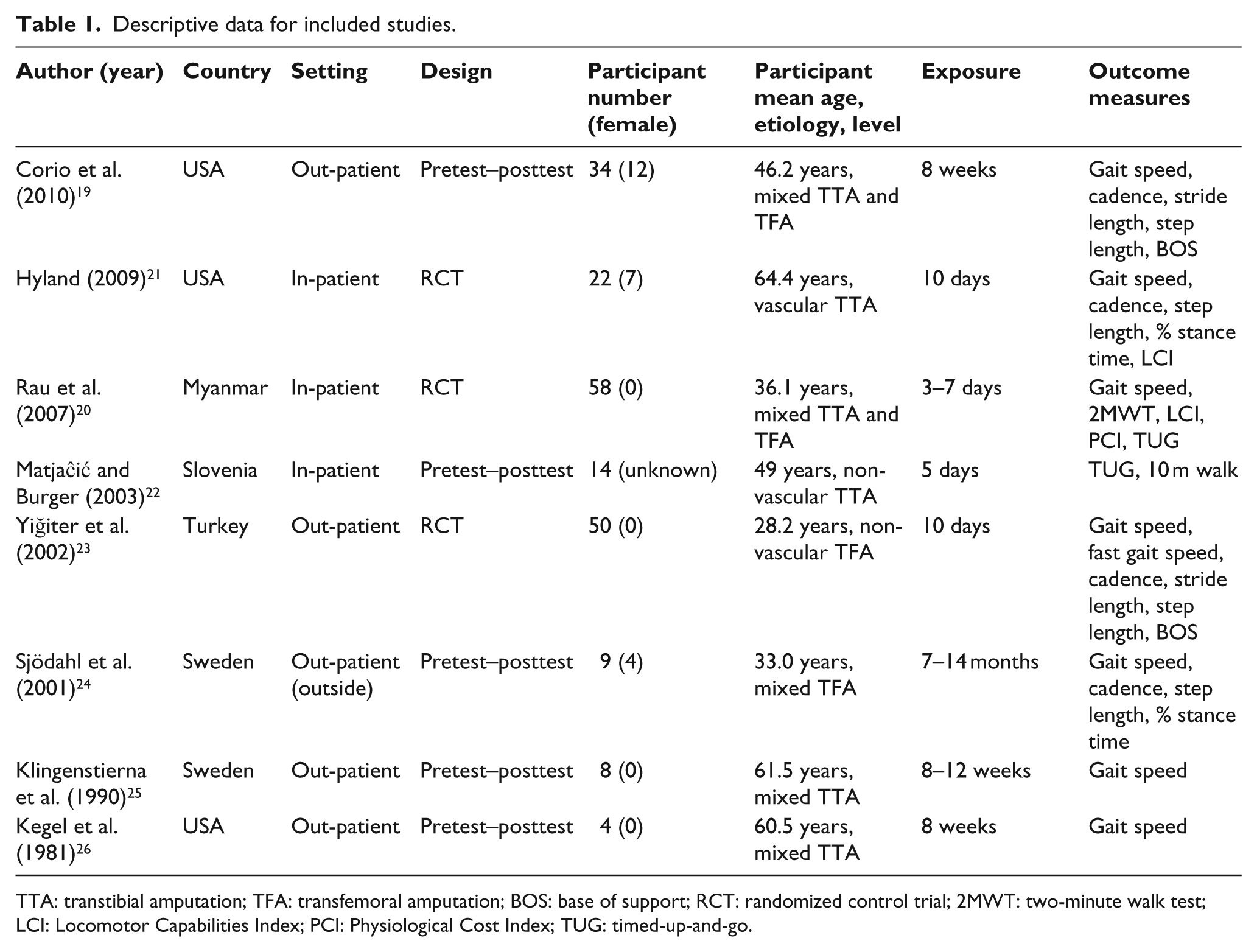
TTA: transtibial amputation; TFA: transfemoral amputation; BOS: base of support; RCT: randomized control trial; 2MWT: two-minute walk test; LCI: Locomotor Capabilities Index; PCI: Physiological Cost Index; TUG: timed-up-and-go.
Study design
Three studies were randomized control trials;20,21,23 five were pretest–posttest designs.19,22,24–26 All three randomized control trials used comparison groups that involved treatments that could potentially benefit gait performance and were not benign no-treatment, placebo, or sham conditions.
Participants
The included studies had a range of 4–58 participants, with a combined total of 199 participants. Participants varied with respect to age, amputation etiology and level, and years since amputation. In all, 23 were females and 162 were males (Table 1). Participant age averaged 25–50 years in five studies19,20,22 –24 and over 60 years in three studies.21,25,26 Amputation etiology19,25,26 and level19,20 were sometimes mixed within studies. Time since amputation averaged less than 1 year in two studies,21,23 2.5 years in one study, 25 and 7–11 years in the others.19,20,22,24,26
Exposure conditions
All experimental and comparison condition exposures included exercise programs. In the three randomized control trials, the comparison conditions primarily involved supervised walking20,21 with specific gait training used in one study. 23 The experimental conditions used different types of exercise that can be characterized as specific muscle strengthening exercises, balance training, part-to-whole gait training, and functional gait and activity training. Thus, there were five categories of exercise exposure:
Supervised walking. The primary treatment provided in two control groups20,21 was supervised walking, consisting of participants walking with and without physical and verbal cues. Non-standardized and inconsistently described cues were generally directed at correcting gait compensations.
Specific muscle strengthening. Three studies used different types of exercise programs aimed at developing specific muscle groups, not performed in standing. Biofeedback training was used during isometric exercises to facilitate strengthening in residual dorsiflexion and plantarflexion muscles. 26 Isokinetic training at different speeds was used to strengthen knee flexion and extension muscles. 25 And spinal stabilization exercise with an education program was employed to develop abdominal muscle strength and stability. 19
Balance training. While dynamic balance exercise is a staple of prosthetic training and was included in several studies in this review, one study used balance training for tasks specifically not involving gait. Computer-based activities involving cursor movement were controlled by weight shifting in the frontal and sagittal planes were performed during standing. 22
Gait training. Part-to-whole gait training exercise programs emphasized the development of specific parts of the gait cycle and then progression to practice of the whole gait cycle. 27 Specific weight shifting and dynamic balance activities required for different phases of gait or locomotor tasks, such as stairs, progressed to practice of the whole activity. This approach 28 was used with participants in the experimental group for at least 50% of the treatment time compared to participants in the comparison group who used this approach <10% of the time. 21 A similar approach was used in a two-group study with the comparison group training without resistance while the experimental group used the same exercises against the therapist’s manual resistance. 23
Functional training. Two studies employed functional exercise programs that were focused on coordination exercises and daily gait activities beyond walking and stair negotiation. The experimental condition of a randomized control trial employed seven exercises using boxes and ladders, obstacles and uneven ground, and other functional activities such as carrying water and simulated rice planting. 20 Another study employed functional training at various gait speeds focusing on rotatory movements performed exclusively outdoors to incorporate different terrains, natural obstacles, and the contextual stimuli of the environmental. This treatment condition also emphasized an emotional awareness in patient–therapist interactions during each session. 24
Other exposure condition variables
Regardless of the exercise category, a number of other factors summarized here could have affected the outcomes including treatment setting, duration, and compliance. Treatment settings included both in- and out-patient facilities. Five studies were conducted in out-patient settings,19,23 –26 with treatment held exclusively outside in one study. 24 Two studies were conducted at prosthetic clinics where participants stayed during the study.20,22 One study was conducted in hospital. 21 Treatment providers were physiotherapists in seven studies19–24,26 with two studies emphasizing home exercise.19,26 One study left the provider unspecified. 25 Treatment duration for the exercise programs ranged from 3 days 20 to 14 months 24 with as few as 219 and as many as 40 individual sessions 24 (Table 1). Individual sessions ranged from 30 23 to 90 min 24 with unspecified duration in three studies.21,25,26 Adherence to treatment was undefined in all studies. Two studies, however, did report completed sessions or weeks required due to variable adherence to the treatment schedule.24,25
Outcomes
Primary outcome measure
Self-selected gait speed was reported by all studies. Self-selected gait speed was reported in meters per second in six studies19,20,23–25 (Table 2). Significance values and standard deviations required for effect size calculation were not reported one study. 25 In the three randomized control trials, effect sizes for improvements in gait speed after the experimental versus the comparison conditions were small d = 0.40, 21 medium d = 0.64, 20 and large d = 1.38. 23 Self-selected gait speed was converted to meters per second for studies that provided time and distance data such as results for the 10-m walk test 22 and time to walk 30 m. 25 Units of measurement varied including gait speed at self-selected normal and fast paces, speed divided by limb length, and percent or normal speed reported.
Summary of within-group improvements in gait speed.
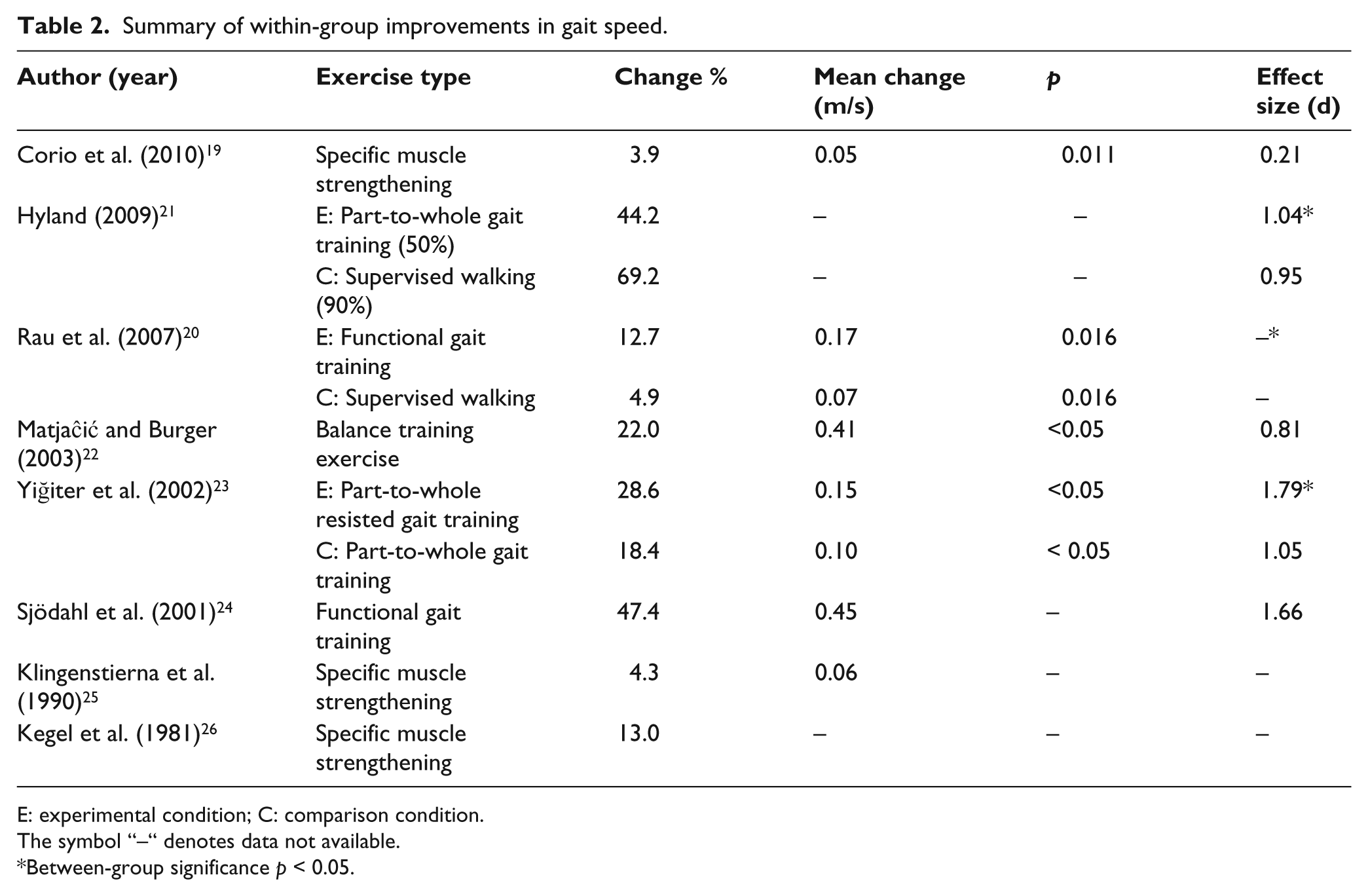
E: experimental condition; C: comparison condition.
The symbol “–“ denotes data not available.
Between-group significance p < 0.05.
Other gait measures were also reported. Fast paced gait, defined as a self-selected brisk walking speed, improved after treatment and was maintained at follow-up in a one-group study without significance testing. 24 One study reported gait speed lower limb length ratio without data necessary to convert the units to meters per second. Significant within-group increases were noted for both groups receiving gait training exercises 50% or 90% of the treatment time, with no difference between conditions. 21 One study reported a 13% average increase in gait speed without values for time or distance; thus, effect size could not be calculated. 26
Secondary outcome measures
Secondary outcome measures include kinematic data for gait performance and quality, multidimensional performance measures, and self-report outcomes (Table 1):
Kinematic data. Cadence measured in steps per minute was recorded in three studies.19,21,23 In one randomized control trial, cadence significantly increased within both exposure conditions with the between-group difference favoring the experimental part-to-whole gait training with resistance compared to no resistance. 23 No change was reported after treatment in the other two studies.19,21 Stride length was recorded by two studies with different designs.19,23 The pre–post test design study found a significant 3-cm increase after treatment. 19 The randomized control found no difference within or between groups. 23 Step length was reported by two studies with conflicting results: amputated side step length increased more in one 19 and sound side 23 step length increased more in the other. Base of support was recorded in two studies.19,23 One reported significantly decreased step widths after both experimental and comparison exercise treatments, with results favoring the resisted gait training exercise program. 23 The other reported no change. 19 Double limb support and single limb stance time showed no significant change after treatment. 21
Multidimensional performance measures. The timed-up-and-go (TUG) test combines functional walking and sit-to-stand transfer ability. 29 No significant between-group changes were reported. 20 The Physiological Cost Index (PCI) assesses cardiovascular system response to walking by comparing resting and post-walking heart rate. 30 The PCI showed a significant difference between-group improvements (p = 0.02) after functional training compared to supervised. 20
Self-report measures: the Locomotor Capabilities Index (LCI) score is a self-report assessment of 14 basic and advanced locomotor abilities each scored on a four-point ordinal scale. 31 No significant changes were noted after treatment.20,21
Time of assessment
Most studies reported assessing outcome data at a consistent time in the study, although three did not have consistent reassessment points.20,24,25 The only study to complete a follow-up assessment reported data similar to the post-treatment measurement. 24
Methodological study quality assessments
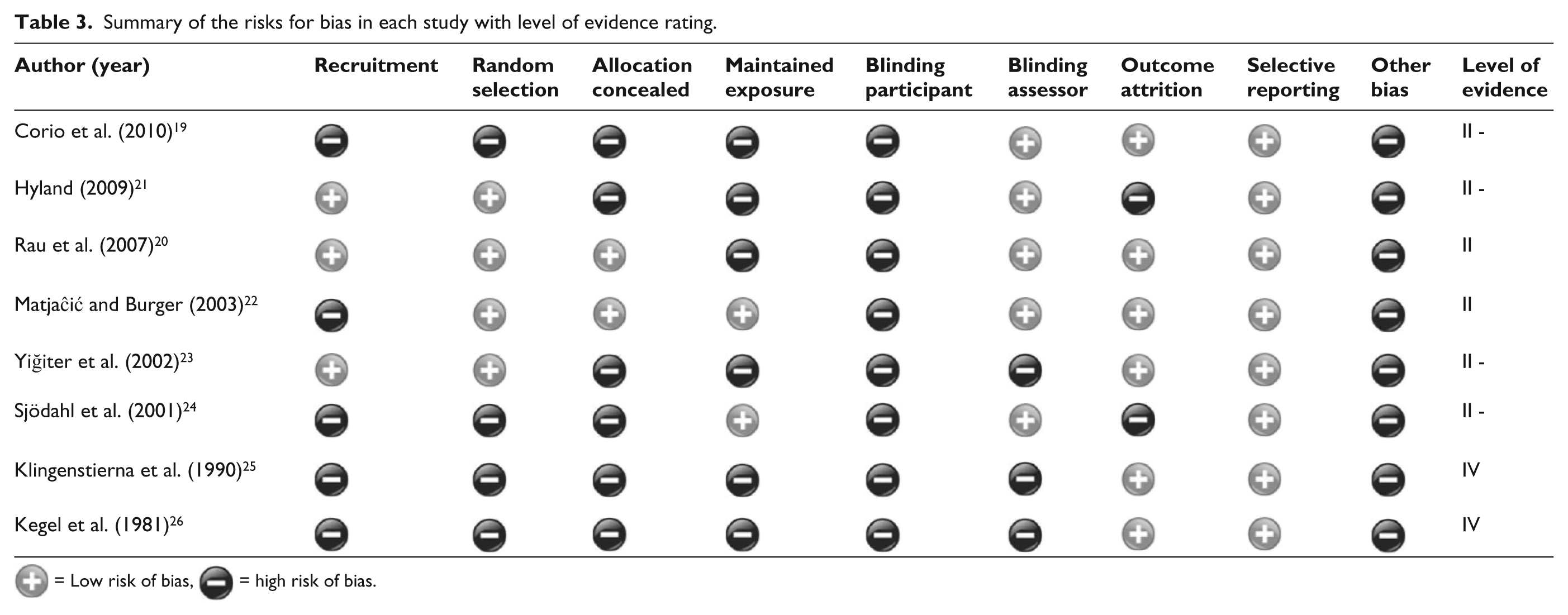
The results of the Cochrane Collaboration Risk of Bias assessment suggested that the combined studies had high risk of bias in the domains of Recruitment, Allocation, Maintenance, Blinding, Objective outcomes, and other bias (Table 3). Lack of control over which participants were recruited to participate and receive treatment was common in the included studies. Most did not describe how subjects were recruited, leaving the possibility of selection bias.19,20,22,23,25,26 The three control trials used randomized allocation to the treatment conditions,20,21,23 although only one reported allocation concealment. 20 Once allocated to an exposure condition, groups were maintained in the three randomized control trials. However, all participants in two studies received similar treatments suggesting potential maintenance bias. Therapist provided resistance was the difference in one study 23 while varying percent time receiving the part-to-whole gait training was the difference in the other. 21 Blinding was impossible for the participants and therapists in all studies. Two studies blinded the assessors.20,21 Incomplete outcome data pose a threat of bias. Two studies did not account for the attrition of subjects that dropped out after receiving treatment in their analysis.21,24 The other studies did not report whether dropouts had occurred.19 –24,26 All studies reported other potential study biases. A major source of potential bias comes from the small sample sizes, with several study samples with fewer than 10 subjects.24–26 Most studies included mostly non-vascular amputations,19,20,22–24 although vascular amputations make up the largest proportion of the overall population. 32 General activity level was uncontrolled for in all studies.
Summary of the risks for bias in each study with level of evidence rating.
 = Low risk of bias,
= Low risk of bias,  = high risk of bias.
= high risk of bias.
Levels of evidence
Of the three randomized control trials, one was downgraded to Level II due to lack of blinding, use of multiple testers, and different outcome time frames 20 and two were double downgraded to Level II - due to lack of blinding, 23 lack of intent-to-treat analysis, 21 sample sizes ≤50, and co-intervention between exposure conditions.21,23 Single group studies were Level II evidence. 22 Two were downgraded to Level II - due to sample heterogeneity 19 and lack of intent-to-treat analysis. 24 Two single-group studies with fewer than 10 subjects were classified as Level IV evidence.25,26
Overall quality of combined evidence
The overall quality of the combined evidence was low following the Cochrane GRADE system, 16 which corresponded to a B grade recommendation on the Oxford Levels of Evidence chart 18 in support of exercise programs. There was low–moderate quality evidence to support specific resisted part-to-whole or functional exercise gait training programs over unresisted gait training or supervised walking.20,23
Discussion
This is the first systematic review to examine the effect of exercise programs on gait performance in people with lower limb amputations. Of the eight studies that met the inclusion criteria, the only consistent measure of gait performance was self-selected gait speed. Overall, the strength of the combined evidence supporting exercise as a treatment to improve gait performance was low to moderate with a lack of Level I randomized control trial designs, a low number of combined participants, heterogeneity among sample populations and treatment conditions, and the presence of potential bias. The combined evidence suggests that a variety of different types of exercise can improve self-selected gait speed. All exercise programs led to increased gait speed with effect sizes ranging from small to large (Table 2). Study heterogeneity precluded meta-analysis.
Prosthetic function has been associated with a range of patient characteristics. The findings of this review were derived from studies including a wide variety of participants that varied in age, gender, amputation etiology, level, and prosthetic experience. Improvement in gait performance was seen throughout whether participants were in their third 23 or seventh decade21,25 and whether only men20,22,23,25,26 or men and women combined.19,21,24 No studies included only women. High within-group effect sizes for improved gait speed were observed for participants with non-vascular 22 or vascular etiologies.21,23 Participants improved whether they had transfemoral23,24 or transtibial amputations,21,22,25,26 whether first-time prosthesis users <6 months after surgery, 21 or experienced users nearly 10 years since surgery. 24 Heterogeneity within the population of people with lower limb amputations may limit the conclusions regarding any particular subset and pose a problem for researchers designing studies.
Little evidence consistently differentiated which type of exercise was most beneficial. All exercise types appeared effective in improving within-group gait speed, whether emphasizing supervised walking, specific muscle strengthening, balance training, part-to-whole gait training, or functional gait/activity training. This was true whether most exercise was performed as an unsupervised home exercise program,19,26 in focused daily treatments provided within a single week,20,22 or in regular sessions spanning months.24,25 The low-to-moderate level evidence from the three randomized control trials yielded medium to large effect sizes for improving gait speed with more demanding and functional exercise programs. Adding resistance to the part-to-whole gait training program made a difference, 23 for instance, as did adding specific gait exercise and functional training activities beyond supervised walking.20,21 No range-of-motion or flexibility exercises were included in these studies. All three randomized control trials used treatment durations that included 10 or fewer visits for a combined 3–5 h of out-patient treatment20,23 or approximately 10 h of in-patient care. 21
The number of total participants was too small to draw firm conclusions. However, the overall consistency in the results for this diverse group of studies spanning three continents with participants of varied age, amputation etiology and level, and prosthetic experience, who were treated in both in- and out-patient settings, suggest the findings of this review may have broad application. More high-quality research is needed to confirm these findings, determine which types of exercise are more effective than others, and explore the interaction between exercise type and different characteristics of people with lower limb amputation.
No other metric besides gait speed was used to assess gait performance in half of the studies. Gait symmetry, however, is a separate entity from gait speed and has been quantified using step length and stance time, which may vary depending on prosthetic user awareness, motivation, and ability. Two studies that measured step length19,23 reported conflicting results for increased step length on the amputated and sound limbs. No change was reported in single limb support time. 21 Increased speed can be achieved with increased step length of either limb. Gait symmetry may be best measured as a ratio of both step lengths. Such data were unavailable. Overall, data addressing gait symmetry were insufficient and too inconsistent for a synthesis of the results. More research should be performed to establish a standardized way of quantifying gait symmetry for future use in research.
Self-report measures and gait indices that combine various data may be useful but may require a more comprehensive approach to therapy to produce significant gains. Many tasks like the TUG require combinations of abilities and all volitional activities involve psychomotor performance not necessarily best assessed with time. Both supervised walking and functional exercise training improved TUG time with no significant difference between interventions, although the functional exercise training did significantly improve the PCI. 20 Overall, an exercise program emphasizing functional activities in real-life settings may be the best approach to increasing functional participation in life’s activities. 24 More research is needed to identify therapeutic exercise and activities that improve the multidimensional gait performance needed to facilitate a return to vocational and recreational pursuits.
Limitations
This systematic review of exercise programs to improve gait performance in people with limb loss was limited by potential bias resulting from heterogeneity of the study designs, participants, and exercise interventions. People with limb loss are a diverse population and the exercise protocols were in some cases complex, unclearly defined, and inconsistently maintained. The exercise programs were classified in this review to provide a descriptive sense of each program emphasis, although many programs had overlapping features. Although a variety of objective gait measures were noted, exclusion of studies that did not include gait speed as one of the outcome measures may have limited consideration of other gait performance measures, such as the use of walking aids. The lack of a consistent gait symmetry measure prevented synthesis of related data. Lack of long-term follow-up precluded any judgment as to the lasting benefit of any included exercise program. The effects of various prosthetic components or alignment parameters, surgical approaches or medical complications, and quality-of-life indices were beyond the scope of this review.
Conclusion
The available evidence provides a Grade B recommendation to support exercise programs that use a range of methods including supervised walking, specific muscle strengthening, balance training, part-to-whole gait training, and functional gait/activity training to improve gait performance for people with lower limb amputation. No consensus on a best approach to exercise emerged. As care has shifted out of in-patient training, the importance of exercise programs conducted in out-patient settings for people with lower limb amputations may increase. The lack of Level I randomized control trials identified in this review underscores the need for more and higher quality research into the clinical benefits of specific exercise programs in lower limb amputation rehabilitation.
Footnotes
Acknowledgements
The authors thank Dr Debra Krasinski for her guidance and support.
Author contribution
All authors have read and approved this article. Concept, design, analysis, and writing: CKW Data acquisition, analysis, and writing: JEE., JCE., and NJM.
Declaration of conflicting interests
The authors have no conflict of interest to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.