
Abstract
Background: Few published reports exist regarding the control of the human/prosthesis interface in persons with unilateral transtibial amputation.
Objective: To investigate strategies employed by prosthetic users in controlling the human/prosthesis interface to highlight challenges associated with either the amputation or the design of the prosthesis.
Study Design: Randomized controlled trial.
Methods: Cycling was used as the locomotor task to allow for better control of task mechanics compared to walking. A group of nine cyclists with intact limbs were compared to eight cyclists with transtibial amputation (CTA) during a simulated cycling time trial. The CTA group pedaled with a stiff and flexible prosthetic foot. Reaction forces between the foot and the pedal were measured using an instrumented pedal system. The force effectiveness (FE) ratio was used as the measure of task performance. The FE ratio is the force component normal to the bicycle crank arm divided by the resultant force for both limbs and is commonly used to analyze pedaling technique.
Results: The CTA group was equally as effective at applying forces as the intact group.
Conclusions: These data suggest that individuals with lower limb loss are able to compensate for their amputation to utilize a similar pedaling technique for locomotor performance. As global strategies, e.g. force effectiveness, appear similar between groups future research should focus on local strategies, e.g. individual joint kinematics and kinetics.
Keywords
Clinical relevance
Research involving local strategies, e.g. individual joint kinematics and kinetics and their relationship to net output of the human/prosthesis system, will enhance our understanding of this system while allowing for better clinical application of the research.
Background
Individuals with a unilateral transtibial amputation have lost the structure of the ankle joint and the muscles and connective tissues controlling the joint. In addition, sensory input from the joint and surrounding tissues has also been lost. These individuals must now adapt to structural and physiological changes related to the amputation and interact with their environment via a prosthetic limb on one side and via an intact limb on the other. 1 Changes that occur after amputation include: the sound limb becomes the dominate limb for locomotion2-6; atrophy of the residual limb with possible hypertrophy of the sound limb 7 ; and alterations in movement strategies.1,4,5
All of these changes are interrelated and will affect the person’s ability to generate and effectively direct forces to interact with their environment. It remains unclear how these distinct, yet integrated, changes relate to the control of task performance. The purpose of this study was to investigate the pedaling technique employed by transtibial amputees during a cycling task to establish a foundation for future research in motor control as well as a potential improvement in prosthetic design.
The cycling task was chosen because it requires effective integration of human neuromuscular control and bicycle systems thus providing a unique environment for the investigation of motor control. 8 Cycling is a rhythmic task similar to gait and one that includes upper body support by the saddle minimizing the need to stabilize the torso during propulsion. The cycling task also provides a well controlled mechanical environment allowing for easy manipulation of the imposed load and cadence to the human system. While there are usually four or five points of contact between the rider and the bicycle that set the rider position, the foot/pedal interface is a very important mechanical connection and one where the cyclist needs to appropriately apply forces to the crank for propulsion. Development of these ‘pedal forces’, their magnitude and direction, represents the end result of the physiological and mechanical integration of the rider and the bicycle and provides a basic outcome measure in the use of the cycling task in motor control.
Force effectiveness (FE) is the ratio between the force component orthogonal to the crank and the resultant force applied to the pedal. This calculation (FE) has been reported previously and has been used to assess a cyclist’s pedaling technique. 9 In this current investigation FE calculations were used to provide insight into compensation techniques used by the rider with an acquired amputation. Additionally, alterations in prosthetic foot stiffness, i.e. changes that alter the ability of the prosthesis to absorb and return energy during the power and recovery phase, were used to perturb the human/prosthesis/bicycle interface. Force effectiveness provides a ‘global’ measure of how the motor system is able to utilize and coordinate both limbs together to perform a cycling task.
Our hypotheses argue that the: total FE (combination of both limbs) will be greater in the intact group than the cyclists with transtibial amputation (CTA) group; and stiff aluminum foot (STIFF) condition will demonstrate greater force effectiveness than the flexible carbon fiber dynamic response prosthetic foot (FLEX) condition.
Methods
Subjects and protocol
A control group of nine intact cyclists (eight males and one female; average age 30.4 +/- 13.4 yrs, height 1.81 +/- 0.06 m, and mass 74.0 +/- 6.6 kg) and eight CTA subjects (six males and two females; average age 36.4 +/- 10.4 yrs, height 1.75 +/- 0.07 m, and mass 78.7.1 +/- 10.8 kg) participated in the study. Inclusion criteria for both groups were that subjects had to ride a bicycle at least once a month and be between 18 and 65 years of age. Inclusion criteria for the CTA group required each to have acquired a unilateral transtibial amputation at least one year prior to this investigation, with the cause of amputation being traumatic or tumor. Exclusion criteria for both groups included cardiovascular or pulmonary pathologies, muscle paralysis and open skin sores on the lower limbs. Among the eight members of this group, seven amputations were a result of trauma and one a result of cancer.
Additional data were collected on two cyclists with transfemoral amputation (CTFA) (average age 22.5 +/- 2.1 yrs, height 1.81 +/- 0.01 m, and mass 73.5 +/- 0.7 kg) and one cyclist with bilateral transtibial amputation (38 yrs, 1.74 m, 91.8 kg). These subjects all had amputation secondary to trauma. These three additional cyclists do not provide a large enough group for statistical analysis but, provide information on how other amputees may perform this task. Informed consent was obtained from all subjects before the beginning of data collection. The study protocol and informed consent forms were approved by the Institutional Review Board for the Georgia Institute of Technology. Cycling experience was at the recreational level for seven subjects in the CTA group and six subjects in the intact group. One cyclist in the CTA group was a Paralympic medalist and three cyclists in the intact group had competed in amateur races.
General methods
Each subject rode their personal conventional road bicycle mounted in a stationary trainer with a calibrated centripetal resistance unit (1-UP USA Inc., Platteville WI). The bicycle was adapted with dual piezoelectric element force pedals as well as the capability to monitor crank/pedal angular displacement using gear driven continuous turn potentiometers. 10 The crank arm length was set to 172 mm. Pedal/rider interface was either through a Look (Look Cycle USA, San Jose, CA.) or Shimano SPD (Shimano inc., Osaka, Japan) type pedal system adapted to fit the piezoelectric element force pedals. 11 The subjects all had experience using one of these pedal systems and subjects were allowed to choose between either pedal/rider interface systems as both measurement systems offered identical mechanical constraints to secure the subject’s foot to the pedal. This allowed the subject to use a pedal system that they were used to while not influencing the mechanical constraints of the task. Force data were recorded at 300 Hz and subsequently smoothed using a simple three-point moving average. 10 Time of each cycle was normalized to 100 data points using a least squares fit and five complete pedal cycles from each trial were averaged together for analysis. Zero position was defined as top dead center of the right crank.
All prosthetic modifications were performed by a certified prosthetist. The subject’s personal prosthesis was modified by replacing the pylon and foot section with an aluminum pylon with a stiff aluminum foot (STIFF) section or a flexible carbon fiber dynamic response prosthetic foot (Vari-flex, Ossur, Reykjavik, Iceland) (FLEX) (Figure 1). Prosthetic feet may be ordered in different stiffness categories set by the manufacturer and based on the mass and height of the user. The FLEX feet used in this study were the lowest category allowed by the manufacturer for each subject’s weight and height class. Alignment of the modified prosthesis was identical to each subject’s personal prosthesis. The cycling cleat was placed in the center of the foot in the frontal plane and aligned with the subject’s first metatarsal head on their sound limb in the sagittal plane for both feet. The three additional cyclists (two transfemoral (TF) and one bilateral transtibial) only cycled with the STIFF foot condition. The two TF cyclists pedaled with the prosthesis they typically used for cycling. This included an undamped (e.g. free-swinging) single axis knee joint. The only modification made to their prosthesis was to adapt the STIFF foot to their existing cycling prosthesis.

Cycling prosthesis used. The stiff aluminum foot is on the left and the flexible carbon fiber foot is on the right with the linear potentiometer mounted to measure foot deflection. The linear potentiometer was used in the complimentary article (Childers et al., in press). The prosthesis retained the subjects’ prosthetic socket but replaced the shank and foot section with a stiff aluminum piece to maintain consistency across subjects. The alignment of the cycling cleat relative to the socket was maintained across both foot conditions, the prostheses pictured here are representative of the prosthetic design used. Subject normally used a carbon fiber dynamic response type foot of similar design to the feet used in this study.
The subject retained their prosthetic socket and prosthetic suspension to minimize the confounding effect of the motor system having to adjust to a new prosthesis. Five of the unilateral transtibial subjects used a pin-type suspension. The rest of the subjects (three unilateral transtibial, both CFTA, and the bilateral transtibial subject) all used a suction suspension. The influence of prosthetic suspension on movement between the residuum and the prosthesis during cycling is minimal. 12
The order of presentation of prosthetic feet was randomized. Immediately following a five-minute warm-up period, each subject performed a six-minute time trial (TT). Each subject was asked to maintain a pace they considered ‘hard’ yet capable of maintaining for the entire trial. This relative load condition was used to replicate the cycling task in a laboratory setting. 13 In addition, the simulated TT defines the task goal to the subject as maintenance of crank output over the TT. Keeping the subject focused on the goal of pacing the TT minimizes the subject’s ability to consciously modify their cycling technique. Using a simulated TT indirectly controls for the subject deliberately changing their pedaling technique and provides a better ‘window’ into the ‘natural’ technique employed by the motor system.
A heart rate monitor was worn during all trials and the rate was recorded once during the final minute of each TT condition. Task difficulty was defined as the per cent of the subject’s maximum age-predicted heart rate, i.e. 220 – age of the subject. 14
The centripetal resistance unit in the stationary trainer increased load as a square of the rpm. This allowed the subject to vary the load by shifting to a different gear and/or by varying their cadence. Each subject, however, was asked to maintain a constant rear wheel speed and gear selection once they defined their TT condition. Subjects were provided feedback on rear wheel speed and cadence via a Cyclecomputer (Sigma-Elektro GmbH, Neustadt, GER) with actual power output calculated from the forces measured by the piezoelectric element force pedals.
The force effectiveness ratio 9 was calculated in this study as the total effectiveness of both limbs combined and was interpreted as the overall quality of the cyclist’s pedaling stroke. 15 Our subjects pedaled at different power output and cadences. Because group means for our data may be affected by the different power outputs and cadences chosen by our subjects, a formula was produced to correct our measured total force effectiveness based on data presented by Patterson and Moreno. 16 This formula is presented below:
FEcor = Corrected Force Effectiveness
FEMeas = Measured Fource Effectiveness
CADAvg = Average Cadence for the group
CADMeas = Measured Cadence for the Subject
PowerAvg = Average Power for the group
PowerMeas = Measured Power for the Subject
Statistical analysis
Task difficulty, torque and cadence as well as the total FE ratios were compared using a one-way ANOVA with three levels (intact group, STIFF foot CTA group, FLEX foot CTA group). When significant F-values were calculated, a Tukey post-hoc was used to determine significance between particular groups. A Pearson’s correlation was used to relate the uncorrected FE ratio to pedal torque, cadence and power. Significance was defined as a p-value ≤ 0.05 for all statistical analyses. Statistical analysis was not performed on data for the two CTFA and one bilateral CTA due to low sample size.
Results
There were no statistically significant differences between cyclists with unilateral transtibial amputation (CTA) and intact groups regarding per cent maximum heart rate maintained during data collection indicating that the difficulty of the task was matched to the individual capabilities of the subjects in each group (Figure 2).
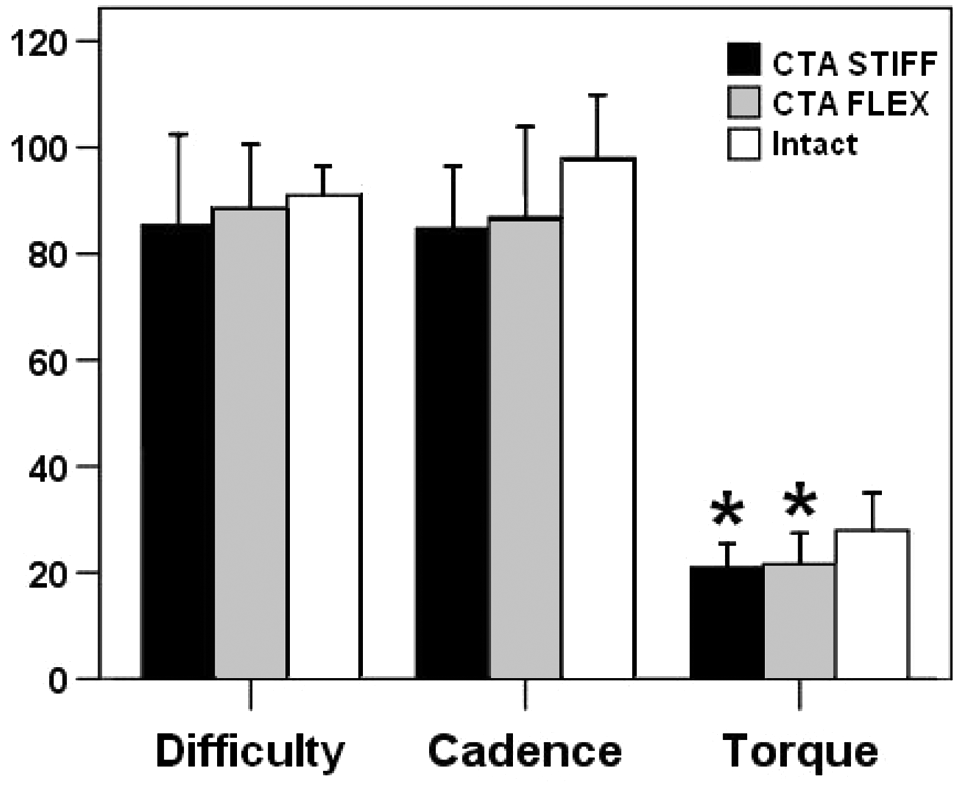
Group means for task difficulty expressed as a percentage of the subjects maximum heart rate, Cadence in rev/min and Torque in Nm ± SD. The cyclists with transtibial amputation (CTA) cycling with the stiff foot (black bars), the CTA cycling with the flexible foot (grey bars) and the intact group (white bars). * indicates significant difference from the intact group.
Total FE and corrected total FE results for the STIFF and FLEX conditions within the CTA and the intact group showed no significant differences (Figure 3). Generally, the corrected means increased for the CTA (STIFF and FLEX) and decreased for the intact group with lower standard deviations calculated for the corrected dataset.
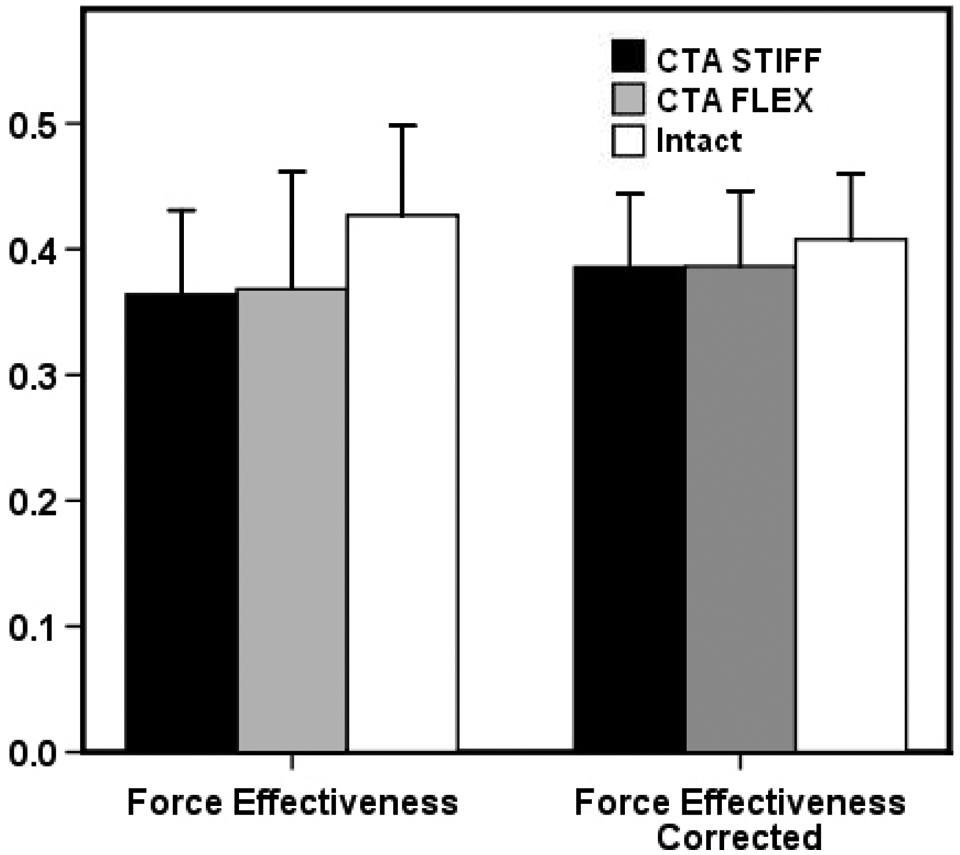
Force effectiveness ratio combining both limbs and averaged over the pedal stroke. The cyclists with transtibial amputation (CTA) cycling with the stiff foot (black bars), the CTA cycling with the flexible foot (grey bars) and the intact group (white bars).
The uncorrected FE ratio was significantly correlated with pedal torque (R = 0.80) and power (R = 0.72) but not significantly correlated with cadence (R = 0.18).
The two CTFAs pedaled with a force effectiveness of 0.43 ± 0.02 and a corrected FE ratio of 0.44 ± 0.02. The FE ratio for the one bilateral transtibial amputee was 0.31 and 0.44 for the uncorrected and corrected, respectfully.
Discussion
The major finding of this research is that the global strategy used to control cycling under the conditions employed in this investigation. The FE ratio was not affected by an altered musculoskeletal system related to the amputation nor by the mechanical properties of the prosthesis. This finding is supported by the fact that there were no statistical significant differences between the intact and CTA group or between prosthetic feet for the calculation of force effectiveness. The FE ratios for the two CTFA and one bilateral CTA provide additional support for this conclusion because these cyclists demonstrated a similar pedaling technique despite having additional joints amputated. These cyclists maintained a similar global strategy despite having asymmetries in output between limbs.4–6 Thus, the motor system of a CTA was able to coordinate asymmetric output between the sound and amputated limbs in conjunction with a prosthesis to achieve the same overall pedaling FE.
Force effectiveness was used as the primary outcome measure in this investigation to compare different pedaling techniques between the amputated and sound limb and between the CTA group and the intact group. This variable was defined previously by Lafortune and Cavanagh 9 and used as a method to quantify a rider’s pedaling technique. This measure is related to the orientation of the forces generated at the foot/pedal interface and, as a result, influenced by inertial, gravitational and muscular components. 6 Furthermore, the constraints imposed by the bicycle on the cyclist also affect the direction of force application and thus FE. 17 The primary focus of this investigation was to evaluate the technique used by cyclists that have acquired a unilateral transtibial amputation. In this context, the inertial and gravitational components, as well as the constraints of the bicycle (e.g. the position of the rider), did not change between experimental conditions leaving the muscular component as the primary cause for changes observed in FE. This variable has been shown to distinguish between different pedaling techniques 18 and therefore seems appropriate for use in this study.
A simulated TT was used to challenge the subject’s motor system while keeping the exercise submaximal. This design allowed flexibility in load and cadence selection to better match the different physical abilities of these subjects. The findings of Patterson and Moreno 16 suggest that variability in force production at the pedal would be minimized when the subject is performing close to their maximal ability and at their preferred cadence. Sanderson 15 also suggested increasing pedaling resistance as a method to challenge the subject’s motor system. Therefore, it was important to select a load that would challenge the motor system while not fatiguing the individual. This was the rationale behind using a submaximal TT at approximately 85% maximum predicted heart rate. The simulated TT, in effect, normalized the mechanical environment to each individual subject’s physical ability. 13 The correction factors derived from Patterson and Moreno 16 did provide a method to normalize across load and cadence and account for those effects.
These results are also supported by unpublished data from Murray and Kram 19 showing no difference in muscular efficiency between three cyclists with amputation and matched intact controls. The positive relationship between muscular efficiency and load has been established.20,21 Mornieux 21 also showed a correlation between muscular efficiency and FE as well as FE and crank power. The FE ratio in this dataset was significantly correlated with crank power and torque. Collectively, these results suggest that the total FE ratio is dependent on load and not on an altered musculoskeletal system or the design of the prosthesis.
These data suggest that mechanical effectiveness is related to load thus not dependant on whether the person has an amputation because the mechanical coupling of the bicycle allows the sound limb to compensate for the amputated limb so the whole system can maintain a given output. Given this scenario it is also important to recognize that variables that represent the global output of a system (total FE, metabolic cost) are not necessarily the best outcome measures to understand movement strategies in individuals with amputation. Instead, these individuals are able to utilize compensation strategies within limbs, e.g. altered coordination across joints. Motor strategies within limbs would not be reflected in an outcome measure investigating whole system performance. This research highlights the motor system’s ability to maintain whole system performance, e.g. global strategy, even when a significant portion of the neuromuscular system has been altered, e.g. transtibial amputation. This means using variables that describe whole system performance (FE ratio, metabolic cost, some functional outcome measures) may not be able to discern differences between persons with an amputation and intact individuals. Thus, measurement of more local variables, e.g. individual joint kinematics and kinetics, may be more appropriate for future research in motor control of persons with an amputation. Future research may then concentrate on the relationship between these more local variables and the net output of the system.
In conclusion, these data suggest that individuals with lower limb loss are able to compensate for an altered musculoskeletal system and the mechanical properties of the prosthetic device and utilize a similar pedaling technique for task performance. As global strategies appear similar between groups, future research should focus on local strategies used within each of the intact and affected limbs.
Footnotes
Acknowledgements
The authors gratefully acknowledge the incredible support from the students, faculty and staff of the School of Applied Physiology as well as the subjects that participated in these research studies. We would also like to thank Ossur Corp., Prosthetic Design Inc., Outback Bicycles and Serotta Bicycles for their donation of prosthetic components and bicycle equipment.
Conflict of interest
The authors report no conflicts of interest.
Funding
Ossur Corp. and Prosthetic Design Inc. donated prosthetic components including the Vari-flex prosthetic feet used. Outback Bicycles and Serotta Bicycles donated miscellaneous bicycle components. Limited monetary support provided internally by the School of Applied Physiology.