
Abstract
Background:
Children with lower limb prostheses cannot always keep up with their peers during active play. A pediatric crossover foot may be a promising prosthetic alternative for children engaging in high-intensity movements necessary for active play.
Objectives:
To compare children’s walking performance, running performance, experienced competence, and cosmesis using their prescribed prosthesis compared with the crossover foot.
Study Design:
Pretest-posttest study.
Methods:
Children with lower limb amputation or deficiency were recruited. Measurements were taken at baseline with the prescribed prosthesis and 6 weeks later with the crossover foot. Walking speed, energy cost of walking, anaerobic muscle power, stair climbing speed, ankle power, and cosmesis were evaluated.
Results:
Four children participated in the study. Two children had increased walking speed with the same energy cost, one child had decreased speed with increased energy cost, and one child had the same speed with decreased energy cost. Muscle power increased for three of the four children and ankle power increased for all children while using the crossover foot compared to the prescribed prosthesis. Two children reported knee pain or feeling excessive knee flexion when running with the crossover foot. One child reported negative feelings toward cosmesis of the crossover foot.
Conclusions:
This study suggests crossover foot may benefit active children by improving walking and running performance, and decreasing energy cost. However, knee pain reports or negative feelings toward the atypical design suggest the crossover foot may not be ideal for every child. Further research is needed to determine which pediatric users would benefit from this type of prosthetic foot.
Clinical relevance
Children with lower limb deficiencies are active prosthetic users who often switch between low- and high-intensity movements in their daily activities. Therefore, they might benefit from a crossover prosthetic design. The preliminary findings of this study suggest the crossover foot (XF) may be a promising foot for active children.
Keywords
Background
Prostheses are frequently used by children with lower limb amputation or deficiency (LLA or LLD, respectively). In the Netherlands, about 500–600 children (<18 years) use a lower limb prosthesis. 1 A prosthesis enables children to walk, run, climb stairs, cycle, play outdoors, and participate in sports. Most children with a prosthesis use it all day.2,3 Ideally, a prosthesis should facilitate children having a physically active life. Participation in active play is important for children’s physical and mental health. In children without amputation, cardiovascular disease and mortality are associated with reduced physical activity, and fitness has a positive impact on school performance and cognitive functioning.4,5
Parents report that children with LLA and LLD experience challenges keeping up with peers and experience barriers in active play due to problems with their mobility and the environment. 6 It is known that, in both adults and children, walking with a lower limb prosthesis requires more energy than walking with two sound legs.7,8 Furthermore, children with transtibial amputation are unable to actively produce ankle power and push-off is correspondingly decreased in the prosthetic leg.9,10 Sports requiring acceleration and endurance are therefore likely to be more difficult for children with lower limb prostheses than their peers.
Prosthetic feet available to children can be generally classified by the amount of energy they store and return. Conventional feet (CF), such as solid ankle cushioned heel (SACH) or multi-axial feet, store and return minimal energy. Energy-storing feet (ESF) store and release energy at push-off, noticeable mainly while running. 11 During normal walking, the differences between CF and ESF for walking speed and push off are minimal.12,13 Running-specific feet (RSF) are energy-storing feet with an extended keel (or “blade”) specifically designed for forward propulsion in running and jumping. A limitation of RSF is that they have no heel or footshell, and as such, they cannot be used with shoes. RSF are therefore often not suitable for all daily activities (e.g. heel-toe walking or walking backwards) due to the lack of stability in stance (i.e. a smaller contact surface and no heel). Crossover feet (XF), which are a hybrid of ESF and RSF, include an extended keel, heel, and foot shape. 14 As such, they may be an ideal design for children, who often need to switch between walking and running throughout their day.
Scientific studies of XF are rare in the pediatric population. In a prior case study (n = 1), a child used an XF, the Össur Cheetah Xplore Junior, and two ESF, the Össur Flex-Foot Junior and Össur Vari-Flex Junior. The child showed an increased horizontal propulsion force during walking and a decreased braking force during stair descent with the XF compared with the ESF. The XF performed between the ESF for the peak vertical loading response during stair descent. 15 One study (n = 7) of the adult version of the XF found an increase with the XF compared with ESF in mobility and endurance outcomes like the Timed Up and Go Test and the 6 Minute Walking Test (6MWT). 14 Also walking speed and step length of sound leg increased with the XF. In a larger study of adults with a transtibial amputation (n = 27), no significant differences in energy expenditure during walking were found when using the XF compared with the ESF, although there was a trend toward a reduced energy expenditure in participants who performed better on the 6MWT, had a higher step count and had a higher Medicare Functional Classification Level at baseline. 16 Also an increase in participants’ satisfaction was noted for walking, ascending stairs, running, and playing sports using the XF. 17 Although results of these studies suggest that the XF may be a promising foot for people with a transtibial amputation, and results could probably be translated to the pediatric population, additional evidence is needed to assess the potential benefits of XF relative to other feet in active children.
The aim of this study was to compare performance, comfort, and cosmesis of XF to CF or ESF (see Figure 1) regularly used by children with LLA or LLD. We hypothesized that the XF would increase walking speed; reduce the energy cost of walking; improve anaerobic performance during running, running up stairs, and running down stairs; and increase prosthetic ankle power during walking and running. We also hypothesized that children would rate cosmesis of the XF lower due to its unique design.
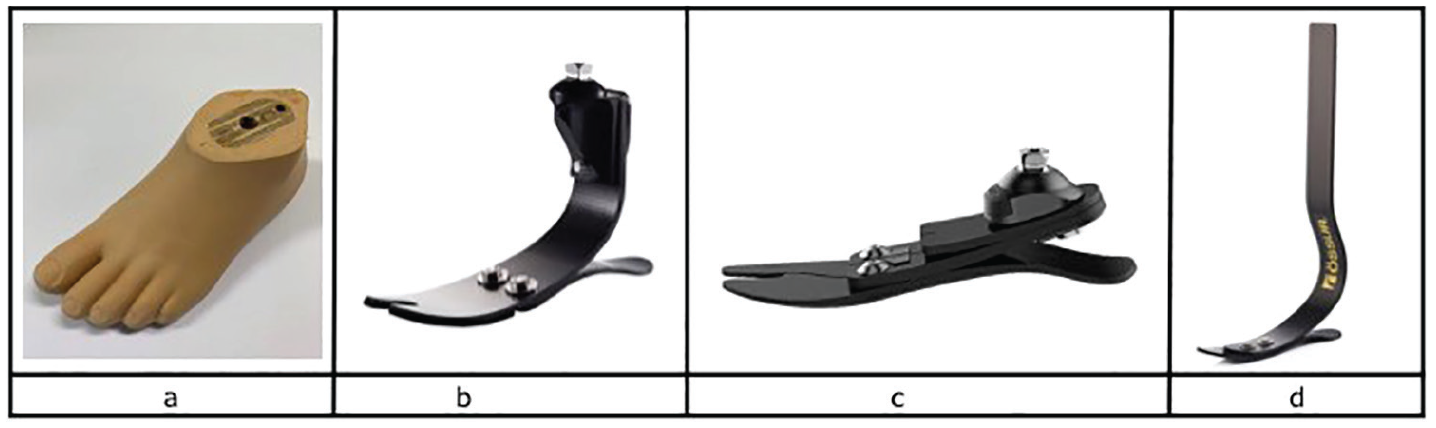
Pediatric feet used in this study: (a) SACH, conventional foot (CF); (b) Vari-Flex Junior, energy-storing foot (ESF); (c) Pro-Flex LP junior, energy-storing foot (ESF); (d) Cheetah Xplore Junior, crossover foot (XF).
Methods
Participants and inclusion
An exploratory pretest–posttest study was conducted with a convenience sample of four children due to limited resources. We aimed to include children of both sexes (i.e. two boys and two girls) and of different ages. Children with LLA or LLD of the distal lower limb were recruited from the outpatient pediatric rehabilitation clinic De Hoogstraat Rehabilitation in Utrecht, the Netherlands. Children were recruited from October to December 2016. Inclusion criteria were age between 8 and 18, use of a prosthesis for at least 1 year, classification as “community ambulator” according to the Hoffer classification, 18 and experience playing sports at a sports club at least once per week. The local ethical committee of De Hoogstraat Rehabilitation Center approved the study protocol. Written informed consent was obtained from the participants, or if the participant was <16 years old, the participant and both parents gave their written consent.
Research protocol
The research protocol consisted of a baseline evaluation with the child’s prescribed prosthesis (CF or ESF), and an evaluation after 6 weeks with the XF prosthesis (Cheetah Xplore Junior, Össur Europe BV, Eindhoven, the Netherlands), see Figure 1. At baseline, a certified prosthetist verified suspension and alignment of the prescribed prosthesis, using visual inspection and participant feedback. If needed, the prosthetist made adjustments for optimal fitting. Afterwards, the child was evaluated with the prescribed prosthesis. On the same day, the child was casted for a new socket because the XF requires direct lamination to the posterior socket. Each child returned within 1 week for fitting the XF prosthesis. Consistent with clinical practices, the prosthetist used visual inspection and participant feedback to determine alignment of the XF. The child was then asked to wear the XF prosthesis for 6 weeks. If necessary, adjustments were made to the socket after 2 weeks of wearing the XF. After 6 weeks (4 weeks after any necessary adjustments), the child was evaluated in the XF prosthesis. The same measurements were performed at baseline and at 6 weeks.
Instruments
A Cortex Metamax 3X (Samcon bvba, Melle, Belgium) was used to measure oxygen uptake (VO2), carbon dioxide production (VCO2), and respiratory exchange ratio (RER = VCO2/VO2). The system was calibrated prior to use, and metabolic stress software (Metasoft Studio) was used to process energetics data measured while the participants walked with their prostheses. A heart rate monitor (Polar Electro, Utrecht, The Netherlands) was used to measure heart rate.
Instrumented gait analysis was used to evaluate the children’s performance during walking and running. Motion capture was performed using eight Vicon T20s (Oxford Metrics, Oxford, UK) cameras. Ground reaction forces were measured with two AMTI Gen5 force plates (Advanced Mechanical Technology, Inc, Watertown, USA). Reflective markers were placed on participants according to Vicon’s Plug-In Gait lower body model. The ankle marker was placed on the prosthetic limb in the same location as the marker on the participant’s sound limb. Joint moments were derived from the collected kinetic and kinematic data.
Outcome measures
Walking speed and energy cost
Walking speed and energy cost during walking were assessed during 6 minutes of walking back and forth on a standardized 20-meter indoor track.19,20 Participants were instructed to walk at comfortable walking speed. Mean walking speed (m/s) was calculated over 6 min. A difference of 0.1 m/s was perceived as a clinically significant difference.21,22 Participants wore a heart rate monitor and calibrated Metamax system to continuously measure their heart rate and oxygen (O2) consumption during the test. Oxygen consumption was determined, after visual inspection of the data, when the mean VO2 reached a steady state in two of the last 4 minutes. Energy cost during walking was determined with the following formula: (4.960 × RER + 16.040) × VO2 (mL/kg/min). 23 A difference of 0.5 J/kg/m was used as a threshold for a clinically significant difference because the standard deviation of the Gross Energy Cost is 0.464 J/kg/m. 19
Anaerobic performance
Anaerobic performance was assessed using the Muscle Power Sprint Test (MPST).18,24 Participants completed six 15-meter runs with a standardized rest of 10 s between sprints. Mean and peak power were calculated using the following formula: Power = (body mass (with prosthesis) × (15 meter)) 2 /time 3 . The highest calculated power was defined as peak power. The average power over all six sprints was defined as mean power. Data of typically developing Dutch children were used as reference. 18 The minimal detectable change for typically developing children, 16.8 W, was used as the threshold for a clinically significant difference. 18
Stair performance
Stair climbing performance was assessed during the timed up and down stair test (TUDS). The TUDS (steps/s) assesses the functional mobility and balance by measuring the time required for the participant to go quickly up and down a 14-step staircase, divided by the number of risers in the stairs. 25 In this study, we modified the TUDS by using a 19-step staircase that was available for testing.
Ankle power and step length
Ankle (peak) power and step length were assessed using the motion analysis system. The Vicon Plug-in Gait lower body model was used to calculate these parameters. Each parameter was based on the average of three trials as participants walked or ran over a 10-meter, level, overground walkway.
Experienced competence and cosmesis
The experienced Competence and Cosmesis of prosthesis for Children with a Limb Deficiency (Co-Co ChiLD, see Supplement) is a survey developed for this study. It was adapted from the Bone Tumor (bt-DUX) questionnaire,26,27 an instrument developed to measure quality of life in children after surgery for a malignant bone tumor. We adjusted the bt-DUX so that it was applicable for children using lower limb prostheses by removing a question about the results of surgery, adding questions about running and cycling, and adding open-ended questions about the prosthesis. The final Co-Co ChiLD questionnaire consisted of 18 questions that span four domains (i.e. emotional, social, cosmetic, and functional); each scored using a 5-point ordinal scale. The questionnaire also included one question about the appearance of the prosthesis, and two open-ended questions about the advantages and disadvantages of the prosthesis.
Results
Four children, aged between 9 and 14 years, participated in the study. All participants had LLD, but two underwent a Syme’s amputation when they were younger (Table 1). Three children used a prosthesis with an ESF (i.e. two with an Össur Pro-Flex LP foot and one an Össur Vari-Flex Junior foot); one used a prosthesis with a CF (Otto Bock Benelux, Nieuwkuijk, The Netherlands). Results are summarized for each child (Tables 2 and 3 and Figure 2).
Patient characteristics.
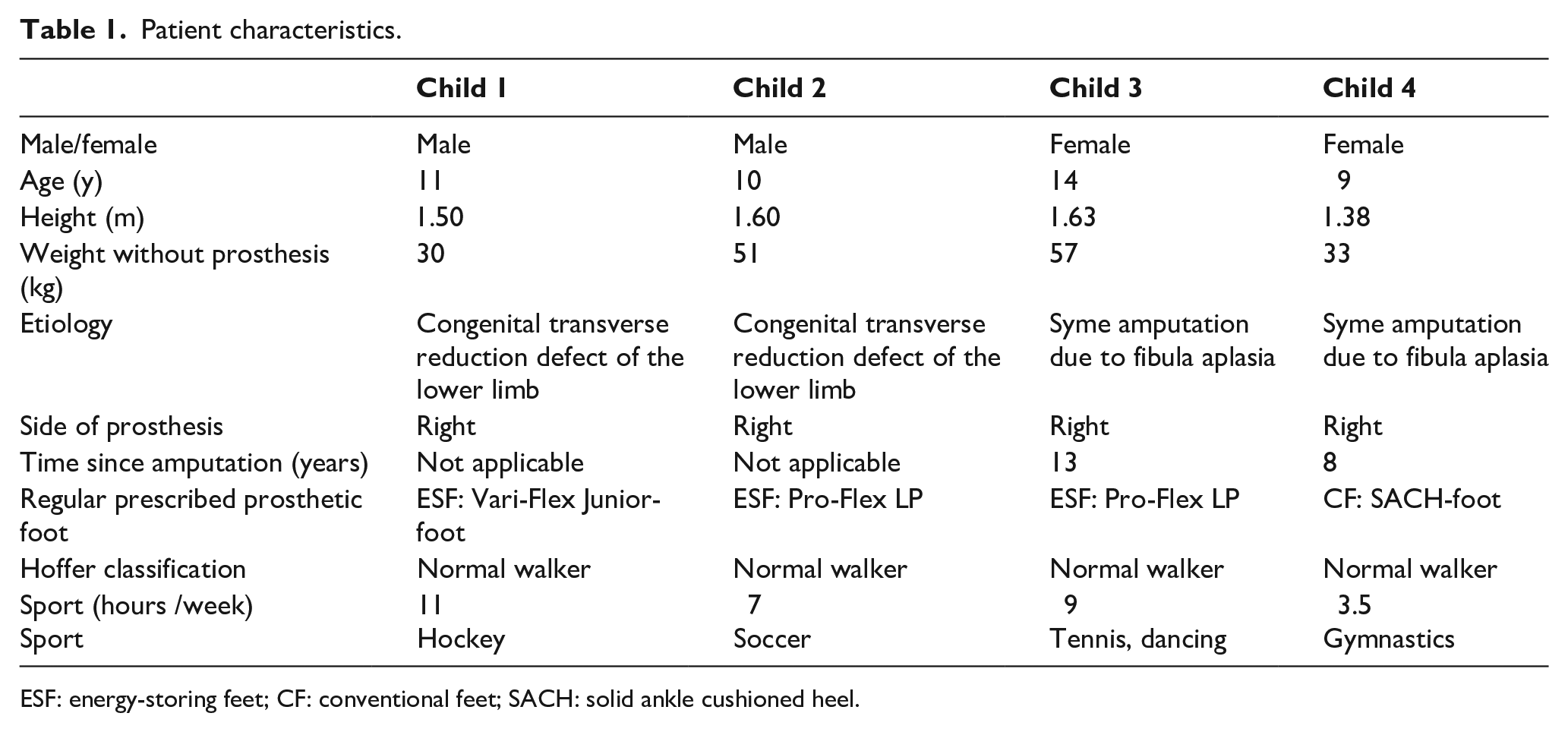
ESF: energy-storing feet; CF: conventional feet; SACH: solid ankle cushioned heel.
Results of gait analysis and functional tests.
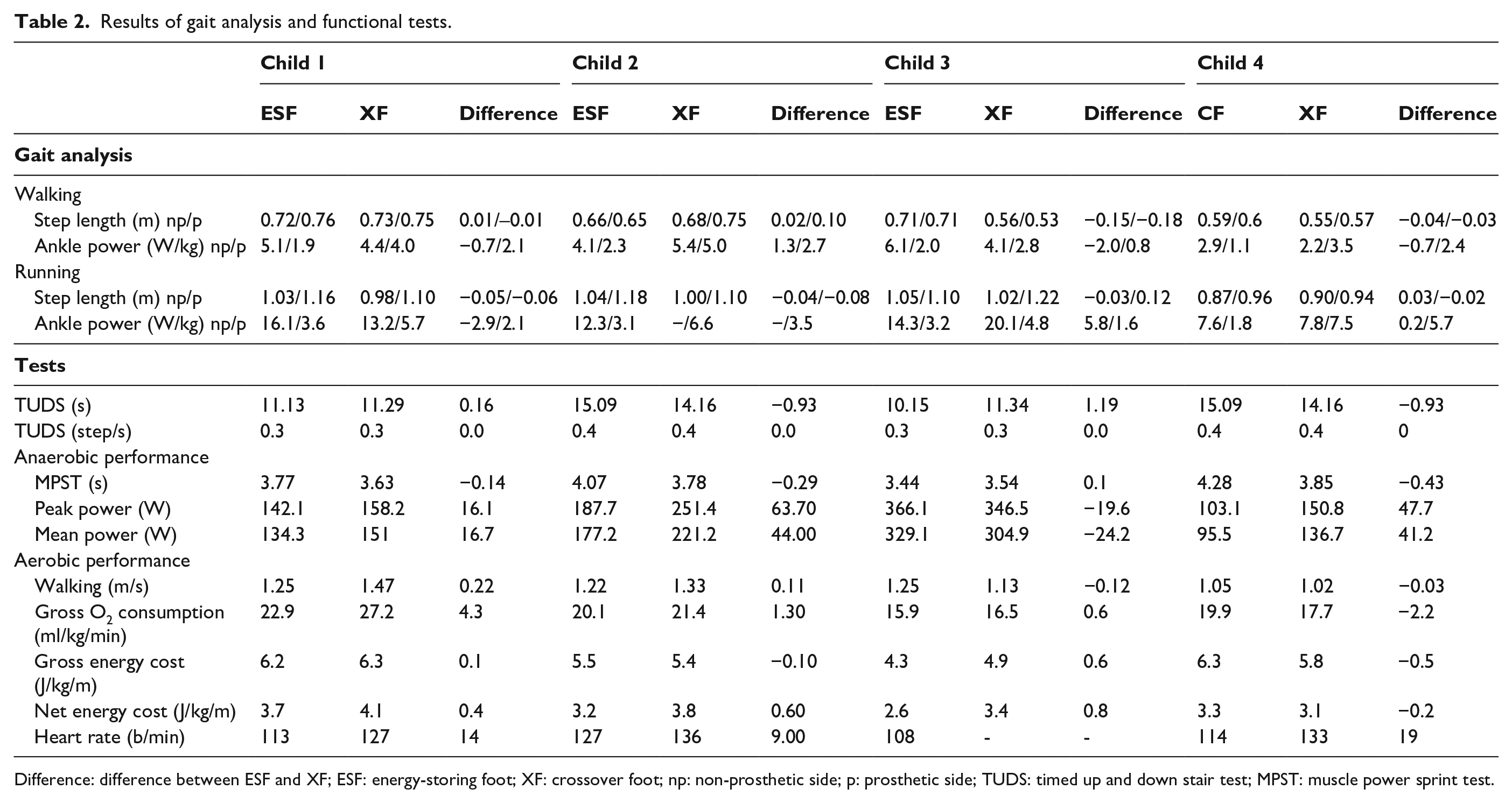
Difference: difference between ESF and XF; ESF: energy-storing foot; XF: crossover foot; np: non-prosthetic side; p: prosthetic side; TUDS: timed up and down stair test; MPST: muscle power sprint test.
Results of the Co-Co Child questionnaire.
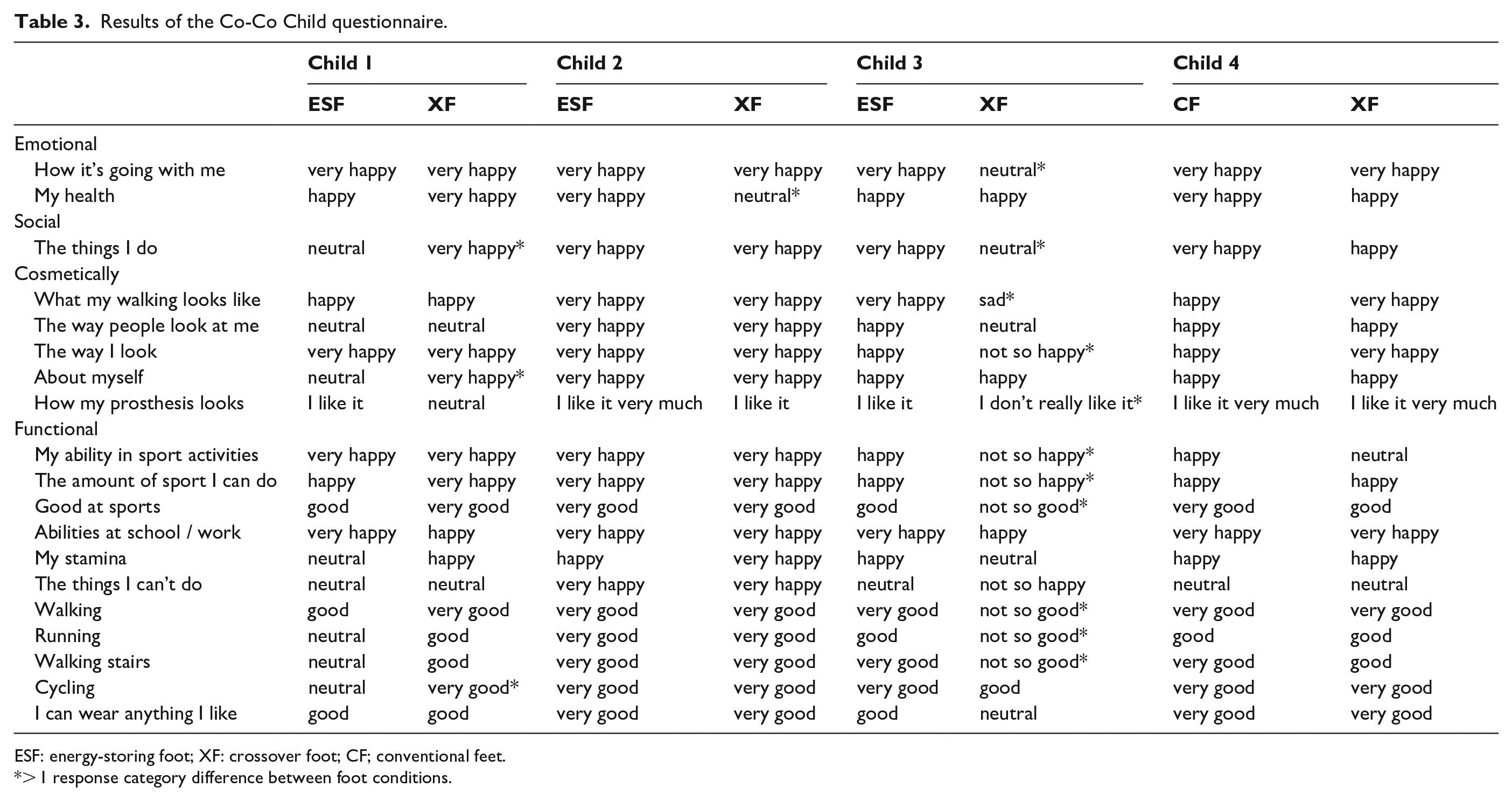
ESF: energy-storing foot; XF: crossover foot; CF; conventional feet.
> 1 response category difference between foot conditions.
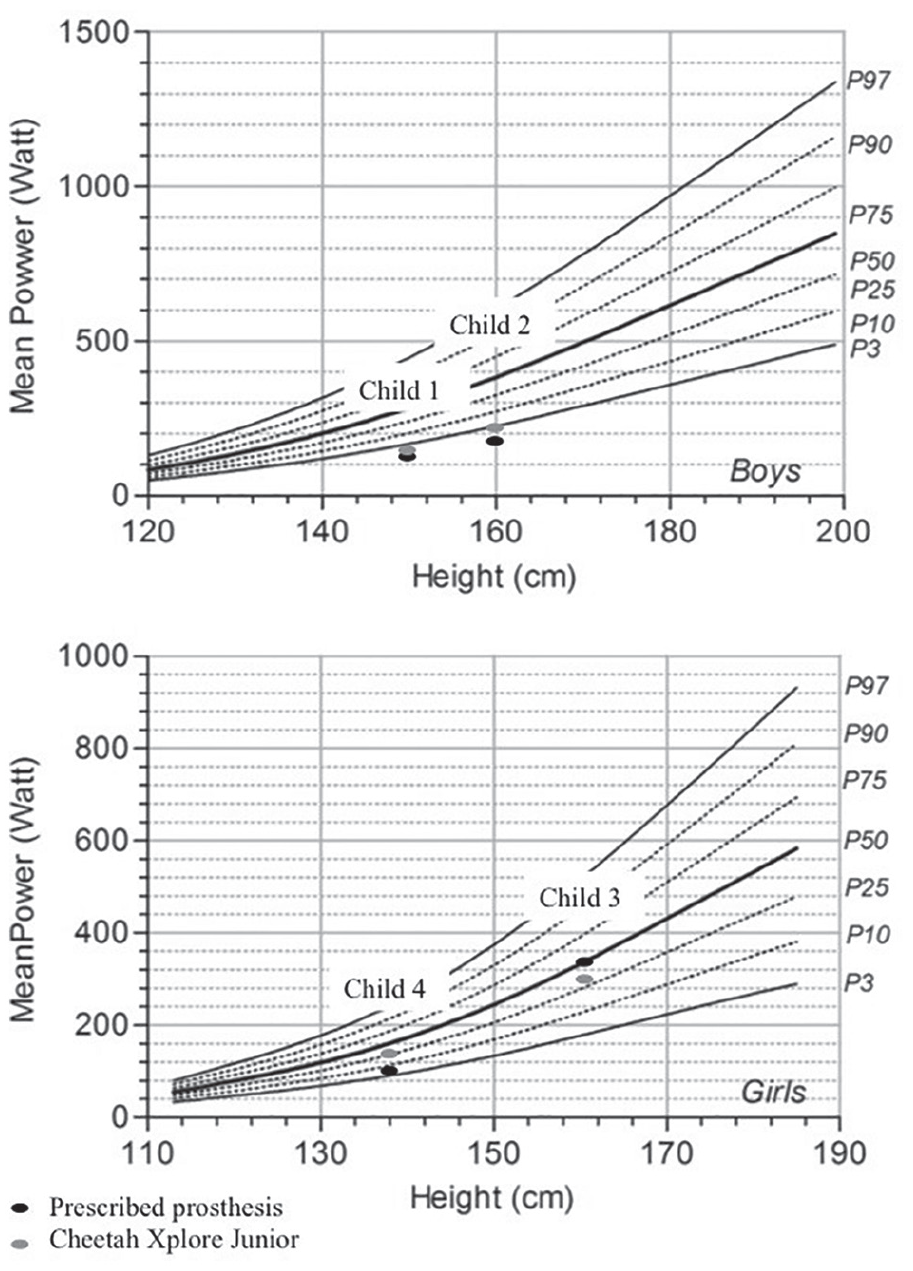
Mean power of the muscle power sprint test (MPST) of participants compared with reference values.
Child 1 exhibited faster walking speed with equivalent energy cost of walking, increased mean power on the MPST, and greater ankle power with the XF. TUDS time did not differ meaningfully between the two tested prostheses. The participant noted on the Co-Co ChiLD questionnaire that running was easier and faster with the XF. However, he also noted feeling excessive knee flexion when running with the XF at times.
Child 2 also showed faster walking speed with the same energy cost of walking, increased mean power on the MPST, and greater ankle power with the XF. TUDS time was similar with both prostheses. Co-Co ChiLD questionnaire responses suggested he expressed a clear preference for the XF regarding its cosmetic appearance and function.
Child 3 demonstrated slower walking speed and exhibited greater energy cost of walking with the XF. Ankle power was higher using the XF, but greater mean power on the MPST using the ESF. TUDS time was similar between prostheses. On the Co-Co ChiLD questionnaire, the participant noted she liked the cosmetic appearance of the ESF and did not like the appearance of the XF. She reported knee aches while walking and running using the XF. However, she reported good push-off with the XF.
Child 4 showed similar walking speed with both prostheses, but used less energy while walking with the XF. Her ankle power increased using the XF. She also demonstrated increased mean power on the MPST with the XF. TUDS time was similar between prostheses. Positive comments about the XF included running faster and walking the stairs more easily. Negative comments included that she could not use flip-flops using the XF and she disliked the way her pants looked when wearing it.
Discussion
In this explorative study, we assessed differences in children’s walking speed; energy cost of and ankle power during walking; anaerobic performance and prosthetic ankle power during running on level ground, running upstairs, and downstairs; and experienced competence and cosmesis while they wore a prosthesis with a XF relative to their prescribed prosthesis with a CF or ESF.
Two of the four children had a higher walking speed with the same energy consumption using the XF. One child had the same walking speed but used less energy. One child walked slower and had a higher energy consumption using the XF. The XF seems beneficial for either walking speed or the energy consumption in three of the four children. This outcome is comparable to two other (adult) studies which found an increase in walking speed with the XF 14 and a trend toward a reduced energy expenditure in participants who performed better on the performance-based outcomes. 16
As expected, most benefit from the XF was found in running. The mean power on the MPST improved in three of four children, indicating that they ran faster using the XF. Interestingly, the results of two children on the MPST were still lower compared with the typically developing children. In order to explain these differences, further research is required on sprinting capability of children with prostheses.
Also, the increase in ankle power with the XF was higher during running than during walking, as would be expected from the literature. 11 The increase of ankle power in this study ranged from +0.8–2.7 W/kg (+40%–218%) for walking and +1.6–5.7 W/kg (+50%–316%) for running, so all children had an increased ankle power >10% using the XF. However, we do not know the clinical implications of this increase. Therefore, we added other types of measurements such as anaerobic performance and energy cost of walking in order to evaluate the added value of the XF for children. A prosthesis with greater ankle power during running might help children with LLD to keep up with their peers. 6 Dutch children with LLD often participate in sports, but may not always participate in their preferred sport(s) because of prosthetic limitations. From clinical practice, we observed that children with lower limb prostheses often quit sports in which regular acceleration and endurance are required. The XF may be able to help children maintain their involvement in these types of sports.
Despite suggestions from other studies that dynamic prosthetic feet could have a greater benefit to people with transtibial amputation during stair ascent and descent,15,17,28 this was not reflected in the results of our study. Dynamic prosthetic feet are reported to store energy during stance and release it as the foot is unweighted, increasing forward acceleration of the leg and body. In stair ambulation, toe-off is less efficient in comparison with jogging, jumping or running due to decreased forward motion of the body over the foot during stance. This potentially restricts body weight from loading the energy-storing forefoot resulting in less advantage of the dynamic design. This might explain the similar performance observed between feet in our participants during stair climbing. This result is in accordance with findings from another study. 29 We think that each of the four children in our study have developed adequate coordination of muscle activity, due to their congenital deficit, to compensate for the functional deficit of an ankle joint on the prosthetic side. This might further explain their performance in stair climbing and the lack of benefit of the XF.
Interestingly, on the questionnaire, one of our participants reported excessive flexion of the knee while running with the XF, and another reported knee pain while walking and running. Other studies on the XF have not described this problem to date. The symptoms reported by our participants might be explained by the alignment of the XF foot. The XF is connected directly to the posterior socket, which places the prosthetic heel further behind the knee center in the sagittal plane, creating a larger knee flexion moment at heel strike. The XF design might require adjustments to decrease the knee flexion moment at heel strike.
Not all participants preferred the XF to their prescribed prosthesis. The appearance of the XF is different from conventional feet due to the J-shaped design, which makes it more difficult, for example, to wear tight jeans. We have included children of different ages and gender, as it is known that as children mature they become more aware of their appearance compared with others and that they might sometimes feel dissatisfied with their bodily appearance. 30 Co-Co ChiLD questionnaire results of Child 3 were generally more positive toward her ESF than the XF. Her walking and running performance test outcomes also decreased using the XF. It should be noted that this participant nearly exceeded the weight class for the XF, meaning that her weight might have hindered maximal energy return from the XF. These factors could have influenced the outcome of the tests and questionnaire. Regardless, this might imply that the XF is not suitable for everyone. Further studies are needed to determine which factors influence the preference for XF.
Limitations of study
A principal limitation to this study is the small sample size. Furthermore, this study included only children with LLD of the distal lower limb. As children with a more proximal amputation or LLD (like Proximal Focal Femur Dysplasia (PFFD)) have greater energetic demands, 31 results of this study may not apply to children with other levels of amputation (e.g. transfemoral amputation) or other types of LLD like PFFD. Additional research is required to determine whether children with other levels of amputation or other types of LLD would benefit from the use of an XF.
Another limitation is that some of the outcome measures used in this study have limited evidence of validity in children with LLD. The MPST has only been tested for validity to date in children with cerebral palsy (CP) and for typically developing 6- to 18-year-old Dutch children.18,24 The TUDS has been validated for children with CP and Down syndrome.25,32 Neither tests have previously been assessed for validity in children with LLD or LLA. Lacking a suitable alternative and given our positive clinical experiences using these tests, we chose to use these tests despite this limitation.
Furthermore, we used two different types of prosthetic feet with a different design. Placement of the markers (according to the “Plug-in Gait” model) had to be adapted for the use of a prosthetic foot and was based on visual inspection. We used the same location of the markers (placement on the foot shell/shoe) on the two types of prosthetic feet. The same footwear was used. Nevertheless, we know that the center of rotation position of prosthetic feet is not fixed. 33 Our results of ankle power measurements might be influenced by the marker position.
Finally, the fact that a new socket was needed in order to attach the XF to the socket might have caused differences in the fitting of the socket between the two types of prosthetic feet, although both sockets were made by the same, experienced prosthetist. It is not clear whether differences in socket fit between the XF and CF/ESF prostheses could have affected the study results.
Conclusions
The results of this pilot study suggest possible advantages of the XF to the prescribed prosthetic feet, particularly in anaerobic performance and energy cost during walking. However, physical complaints and negative feelings about the cosmetics imply that not all children would benefit from the XF used in this study. Thus, while the XF design offers a promise for active children, it may not be appropriate for all children. Additional work is needed to determine for which children the XF would be most appropriate. In future studies, outcome measures for agility, balance, and sidestepping could be included.
Supplemental Material
co-co_child_translated – Supplemental material for Effectiveness of a crossover prosthetic foot in active children with a congenital lower limb deficiency: an explorative study
Supplemental material, co-co_child_translated for Effectiveness of a crossover prosthetic foot in active children with a congenital lower limb deficiency: an explorative study by Floor Jacoba Marie-Georgette Verheul, Olaf Verschuren, Maremka Zwinkels, Mariska Herwegh, Anka Michielsen, Marieke de Haan and Iris van Wijk in Prosthetics and Orthotics International
Footnotes
Acknowledgements
The authors thank Össur Europe BV, Eindhoven, the Netherlands for providing prosthetic components and photos of the prosthetic feet for this study. They thank the children for participating in this study.
Author contributions
All authors contributed equally to the document and met the criteria of authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.