
Abstract
Background and Aim: Unlike sagittal plane prosthesis alignment, few studies have observed the effects of transverse plane alignment on gait and prosthesis behaviour. Changes in transverse plane rotation angle will rotate the points of loading on the prosthesis during stance and may alter its mechanical behaviour. This study observed the effects of increasing the external transverse plane rotation angle, or toe-out, on foot compression and effective lever arm of three commonly prescribed prosthetic feet.
Technique: The roll-over shape of a SACH, Flex and single-axis foot was measured at four external rotation angle conditions (0°, 5°, 7° and 12° relative to neutral). Differences in foot compression between conditions were measured as average distance between roll-over shapes.
Discussion: Increasing the transverse plane rotation angle did not affect foot compression. However, it did affect the effective lever arm, which was maximized with the 5° condition, although differences between conditions were small.
Increasing the transverse plane rotation angle of prosthetic feet by up to 12° beyond neutral has minimal effects on their mechanical behaviour in the plane of walking progression during weight-bearing.
Keywords
Background and Aim
Aligning transtibial prostheses is central to achieving stable, cosmetically acceptable and energy efficient amputee gait.1,2 The majority of alignment studies, both in-vivo 1 and in-silico,3,4 have investigated the effects of sagittal plane alignment on gait biomechanics. However, transverse plane alignment, in particular transverse plane rotation or toe-out, has received relatively little attention. Although prosthetists consider clinical transverse plane rotation to be acceptable within quite a large range of angles (12°), 2 standard clinical transverse plane rotation is commonly defined by aligning the foot’s medial border with the line of walking progression. This results in an external rotation angle (ERA) of approximately 7°, an angle measured between the line of walking progression and the foot axis (a line connecting the midpoint of the end of the heel to the point between the distal ends of the second and third toe). 5
Fridman et al. 6 reported an association between excessive external foot rotation of 18 to 36° beyond ‘optimal’ alignment and reduced stance time symmetry in unilateral transtibial amputees. Others reported that additional 6° external rotation beyond standard alignment increased maximum flexion and total work of the sound side knee 7 and hip 8 during early stance phase, which they believed was due to reduced energy generation during prosthetic side push-off. Additionally, despite changes to the centre of pressure progression during late stance phase 9 and medial-lateral forces under the prosthetic foot, 10 as well as reduced prosthetic side single support time,6-8 little change in prosthetic side joint dynamics were observed in unilateral transtibial amputees when ERA was increased to 6° beyond standard alignment.7.8
Despite the ability of lower-limb amputees to accommodate a range of transverse plane rotation angles, deviations from the standard alignment generates changes in gait parameters on both the prosthetic and sound sides. This is as expected, considering that transverse plane rotation determines the sagittal plane foot lever arm during the stance phase of able-bodied individuals, 11 and the same should theoretically apply to amputees. This may explain the reported gait changes following changes in transverse plane rotation. However, it is unclear why there is minimal change in prosthetic side joint dynamics, which may be due to compensatory mechanisms employed by the user or aspects of experimental protocol, such as non-standardization of prosthetic feet among subjects or selection of tested ERAs.7,8
Due to the inconclusive results of the above studies, information on changes to the mechanical behaviour of prosthetic feet (i.e. foot compression and lever arm) due to transverse plane rotation may provide additional insight, particularly for establishing guidelines for clinicians when aligning prostheses. Therefore, the purpose of this study was to measure the mechanical behaviour, independent of the amputee so as to eliminate confounding variables produced by compensatory gait mechanisms, of three commonly prescribed prosthetic feet during simulated stance phase at several ERAs. Based on previous studies of able-bodied individuals and prosthesis users, it was assumed that the effective lever arm will increase to a maximum at a certain ERA and decrease beyond that angle.
Technique
Three prosthetic feet were tested: a SACH foot (1S49, Otto Bock, Duderstadt, Germany), Flex foot (Assure, Össur, Reykjavik, Iceland) and single-axis foot (1H32, Otto Bock). The amputee-independent mechanical behaviour of each foot was characterized with the roll-over shape (ROS) model using a pylon-based local reference frame 12 (Figure 1), and measured at four ERAs: 0°, 5°, 7° and 12°, which are within the reported range of ERAs prescribed during clinical prosthesis alignment.2,5 Five ROS measurements were taken at each ERA using a motion capture system and a custom loading device (Figure 1).
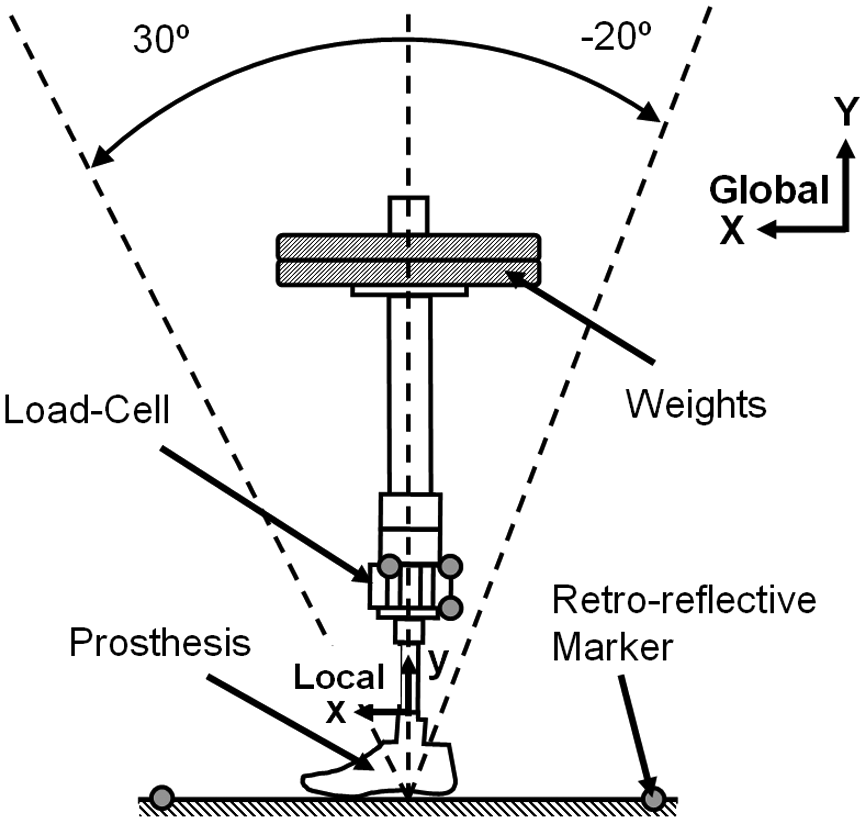
Schematic illustration of the custom loading device. A constant vertical load of 400 Newtons is applied via weights as the custom loading device operators slowly rotate the prosthetic foot within the sagittal plane (13±4°/second to minimize time-dependent effects on foot compression) through the approximate range of forward progression experienced by the tibia during normal gait (-20° to 30°). ROS was estimated by transforming the instantaneous centre of pressure (calculated from the force and moment data from a load-cell (JR3 Inc, Woodland, CA) and marker motion data (Vicon Ltd, Oxford, UK)) from the laboratory (global) reference frame to the prosthesis pylon-based (local) reference frame (origin at the centre of the distal end of the pylon with local x-axis and y-axis always aligned with the plane of simulated walking progression and longitudinal axis of the pylon, respectively). 12 Motion and kinetic data were sampled at 100 Hz and filtered using a Butterworth low-pass filter at 6 and 5 Hz cut-off frequency, respectively.
The prosthetic foot lever arm was determined from the ‘effective foot length ratio’ (EFLR), 13 defined as the ratio of the sagittal plane distance between the posterior end of the foot and the anterior end of the ROS relative to the total foot length. EFLR data normality was assessed with the Shapiro-Wilk test, and within-foot statistical differences were analyzed using a one-way ANOVA with Bonferroni adjustment for multiple comparisons (α=0.05) within SPSS version 13.0 (IBM, Armonk, NY).
Differences in foot compression were analyzed through a process of: 1) resampling each ROS to 100 points using a spline function in Matlab (Mathworks, Natick, MA); 2) calculating the average ROS for each ERA condition; and 3) calculating the distance between each corresponding point along two ROSs (d) and averaging over all 100 points. 14 Thus, the average distance (AveD) between two shapes S1 and S2 in the local reference frame (x-y) is calculated as follows:

and

where k is the number of ROS points, S1xi and S2xi are the x-coordinates of the ith point, and S1yi and S2yi are the y-coordinates of the ith point for shapes S1 and S2, respectively. ROSs are considered more identical (i.e. similar level of foot compression) as AveD approaches zero. Each successive ROS point corresponds approximately to a particular pylon angle as each ROS was estimated over the same range of pylon angles and at the same angular velocity. So each di is the distance between corresponding ROS points, which is not necessarily the shortest distance between the curves.
Discussion
Referring to Figure 2, no noticeable differences were observed in ROS geometry between ERA conditions for all feet and the maximum AveD between all conditions was 3, 3 and 2 millimetres for the SACH, Flex and single-axis foot, respectively. These differences are relatively small compared to the total foot compression under load (Figure 2a). Therefore, the foot’s normal, sagittal plane stiffness corresponding to the plantar surface points of loading during stance phase are similar across conditions. This indicates that the amount of energy absorption and return is not greatly affected by ERA, which is contrary to the suggestion that increased total work of the sound side knee and hip results from reduced energy generation during prosthetic side push-off.7,8
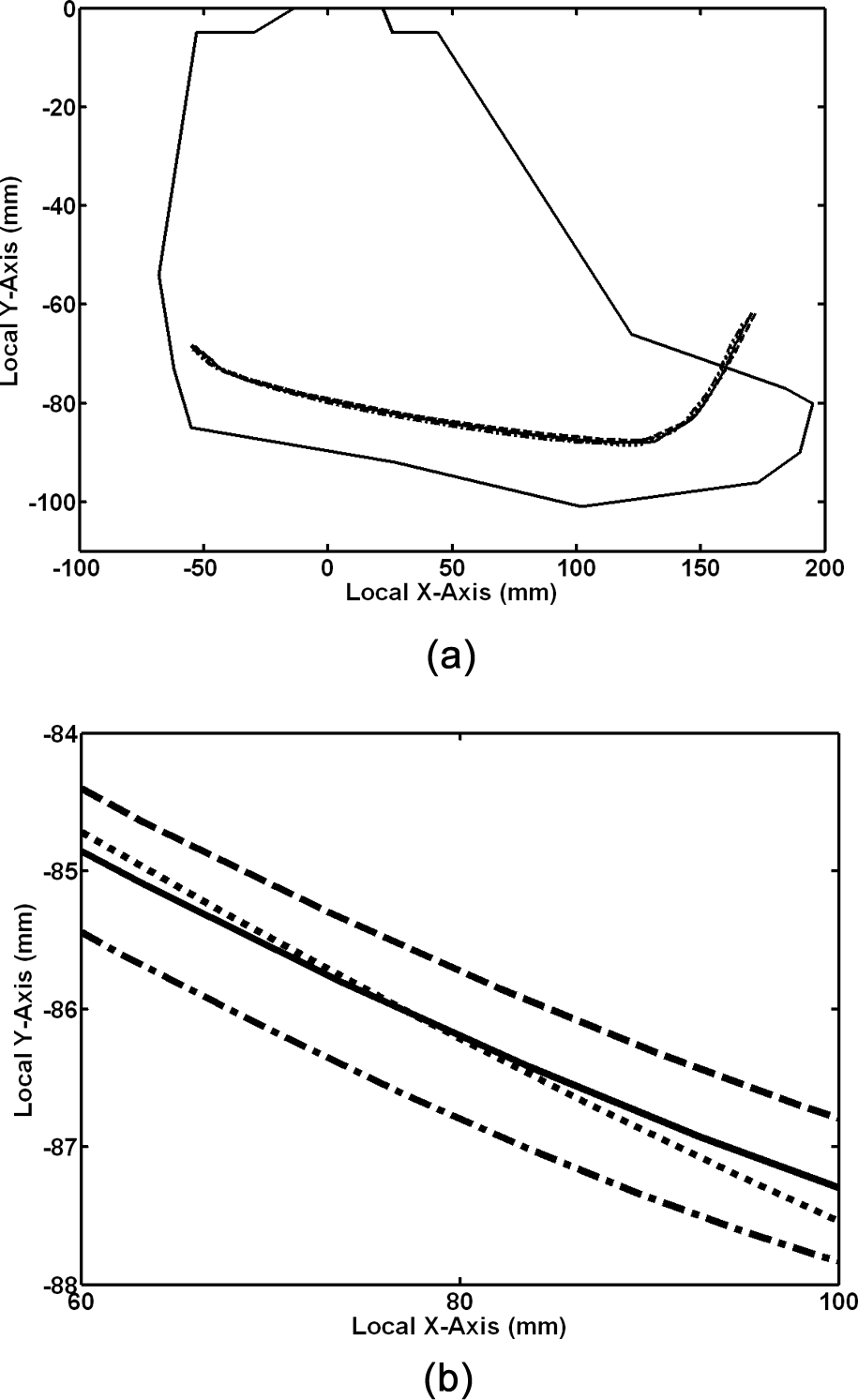
Average ROSs for the SACH foot (0° = solid line, 5° = dash line, 7° = dot line, 12° = dash-dot line), displayed with foot outline (a) and as a zoomed-in section representative of greatest deviation between ROSs (b).
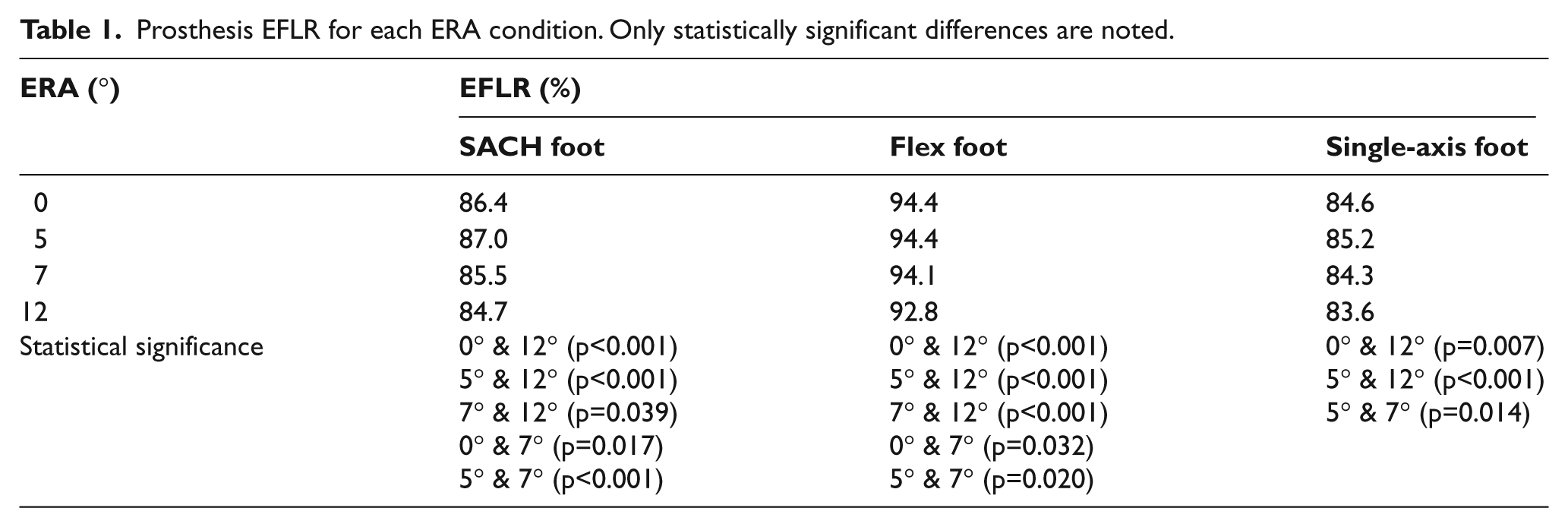
In support of our hypothesis, the EFLR of all feet increased due to increasing ERA, reaching a maximum EFLR at 5°, a reduced EFLR at 7° and a minimum at 12° (Table 1). As with able-bodied individuals, external rotation increases the lever arm by aligning the longitudinal axis of the big toe with the plane of walking progression, 11 whereby further external rotation subsequently decreases the lever arm. If the goal of prosthesis alignment is to achieve a maximum anterior lever arm, then the prosthetic foot should be rotated externally to approximately 5° from neutral. However, the greatest change observed in lever arm (i.e. difference between the 5° and 12° condition) was only 5 and 3 millimetres or 3 and 2% of the ROS length for the SACH and single-axis foot, respectively, indicating that ERA up to 12° had no profound effects on the lever arm and hence may have no clinical significance. This may be true in the sagittal plane, but changes in ERA may have clinical significance in the coronal plane as it could be linked to progressive knee osteoarthritis. For example, increasing the ERA decreases external knee adduction moments15-18 in non-amputee gait, thereby decreasing the load on the medial compartment of the knee and hence progression of medial knee osteoarthritis,19-21 but this will, in turn, increase the load on the lateral compartment. 16 Changing the prosthetic foot ERA may therefore also have implications for amputee gait and could be exploited as a way to minimize prosthetic side knee joint stress for amputees with progressive knee osteoarthritis. However, additional studies need to confirm that such relationships apply to amputee gait.
Prosthesis EFLR for each ERA condition. Only statistically significant differences are noted.
Presumably, the EFLR will continue to decrease with increased ERA beyond 12° and this might explain findings of previous studies. Hansen et al. 22 found a relationship between reduced prosthetic foot EFLR (from 82 to 62%) and reduced step length of the sound side, and believe this is a result of the shorter lever arms producing a ‘drop-off’ effect, meaning rapid prosthetic side unloading during late stance phase. This ‘drop-off’ effect would presumably reduce stance phase time of the prosthetic side, which was indeed observed in a previous study when the prosthetic foot was externally rotated 18° to 36° beyond the standard alignment. 6 In turn, an external rotation of 6° beyond standard alignment had no effect on prosthetic side stance time.7,8
The results from this study might explain why previous studies reported minimal change in prosthetic side joint dynamics,7,8 as there was minimal change in the mechanical behaviour of the three prosthetic feet during weight-bearing resulting from changes in ERA. Prosthetists may then be confident that external rotation up to 12° will not noticeably compromise foot function or profoundly affect prosthetic side dynamics. However, external foot rotation may still affect shear forces applied to the residuum, as an externally rotated foot might cause the socket to rotate externally during push-off, thus potentially causing discomfort and tissue damage, whereby this should be further investigated.
One limitation of this study is that only three prosthetic feet were tested, whereby a greater number of different designs would likely produce different results. However, the selection was felt to encompass designs of the most commonly used passive feet. Another limitation is that the chosen feet were, for safety of the custom loading device operators, loaded at only half the body weight of a typical male, which may explain why the EFLR values are greater than those published on similar feet. 13 However, this was considered appropriate, because the primary objective of this study was to compare within-foot differences of their mechanical behaviour. Additionally, the approximated linear force-displacement behaviour of prosthetic keels under quasi-static loads in previous mechanical characterization studies12,23-25 would indicate that the relationship between ERA and EFLR demonstrated in this study would hold for other effective loads.
Key Points
Changes in external rotation of the three prosthetic feet, which were tested within the range of typical ERAs:
did not noticeably change the overall compression and prosthetic foot lever arm;
increased the effective lever arm up to 5° of external rotation beyond neutral and decrease with further external rotation.
Footnotes
Acknowledgements
The authors wish to thank Colin Smith for his assistance in fabrication of components for the custom loading device.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors declare that there is no conflict of interest.