
Abstract
Background: Little research has been done on the robustness of prosthetic feet prescribed to military personnel, and manufacturers are not required to test their products prior to sale. This is problematic because the prosthetic feet used by active individuals are subjected to loading conditions not seen in normal gait.
Objectives: To evaluate whether commercially available heavy-duty prosthetic feet intended for use by military personnel meet ISO 10328 standards.
Study Design: Bench testing of heavy-duty prosthetic feet using ISO 10328 standards.
Methods: Prosthetic feet from three different manufacturers were tested according to ISO 10328 standards, using a testing frame fitted with axial load and displacement transducers. Pass/fail information was recorded as well as the stiffness and creep of each foot before and after cyclic testing.
Results: All feet passed the ISO 10328 standards at the highest loading level, and some significant differences were found within a given model of prosthesis when comparing stiffness and creep before and after cyclic testing.
Conclusions: This study demonstrated that manufacturers of heavy-duty prosthetic feet adhere to the voluntary ISO 10328 standards. However, these standards may be insufficient because the tests simulate only idealized gait. Further development of the standards may be necessary to reproduce the circumstances that occur during extreme usage to ensure that prosthetic feet do not fail.
Clinical relevance
This study contributes to the understanding of the mechanical behaviour of prosthetics prescribed to active individuals, such as active-duty military service members and paralympic athletes. The results of this study suggest that while existing prosthetic feet may meet the requirements of ISO standards, the tests may not accurately reflect in vivo loading conditions.
Introduction
The incidence of lower-limb amputation has risen in recent years due to the increase in dysvascular disease and the conflicts in Iraq and Afganistan. 1 Traumatic injuries that led to major limb amputation (at or above the wrist or ankle) associated with Operation Iraqi Freedom and Operation Enduring Freedom totalled 1100 by the end of 2009. 2 Individuals receiving amputations due to combat-related injuries are most frequently young and active adults who were in good health prior to their injury. The military states that wounded service members may be returned to active duty if they are making satisfactory rehabilitation progress and if they or their units can manage their medical needs. 3 Approximately 24% of amputees in the current conflicts are returning to active duty, which is a substantial increase over the 7% who returned in Vietnam.4,5 Even if military personnel do not return to active duty, their relative youth and active-duty training implies that they are likely to return to and maintain an active lifestyle. This is feasible, in part, because of recent advances in the quality of treatment and the introduction of more sophisticated prosthetic technology for different activities.6,7 As these technologies advance, allowing users to place more rigorous demands on them, it is crucial to ensure that they are robust and reliable.
Ensuring the quality of prosthetic feet is extremely important under the circumstances of combat-related operations, where service members perform highly strenuous activities that load the prostheses in unusual ways. These unique loading conditions may be attributed to equipment weight, adverse environmental conditions and strenuous gait cycles, such as side-stepping, cutting, twisting and moving over uneven terrain. 1 When loading changes dramatically, such as when a service member performs the abovementioned activities, the performance of the prosthetic foot may not be adequate. Furthermore, actual combat operations involve potentially loading the prosthesis beyond its original design criteria. This scenario could cause catastrophic failure of the prosthesis, placing the life of the service member and others at risk, which underscores the need to ensure high quality prostheses. To accommodate the unusual loading conditions on prosthetic components, active duty service members often have several limbs that have been prescribed for different expected load levels. While this is a feasible solution, it has several obvious drawbacks: it adds additional cargo weight, it is inconvenient for a soldier to have to frequently change the limb, and changing the limb may not be possible when conditions change spontaneously.
The US Food and Drug Administration (FDA), as with all medical devices, provides approval for the sale of prostheses. Prosthetic devices, including prosthetic feet, are Class-1 medical devices requiring only a pre-market notification (510(k)) prior to sale in the US. The FDA does not require structural or performance test reports to be filed for the 510(k), although testing protocols (described below) have been developed. In addition to these testing protocols, the American Orthotic and Prosthetic Association has published advice on design characteristics that should be met for different Center for Medicare and Medicaid Services (CMS) reimbursement codes. 8
This current regulatory mechanism for prostheses has potential shortcomings. Most importantly, because ISO testing is not required for a 510(k) or for reimbursement from CMS, the onus to maintain high-quality products is on the manufacturers. This has proven problematic with other medical devices, most specifically wheelchairs. Several comparison studies performed by independent researchers have demonstrated that wheelchairs frequently do not meet voluntary standards.9-12 Results of these wheelchair comparison studies are one reason the CMS and the Department of Veterans Affairs began requiring the inclusion of test results when applying for a reimbursement code.
ISO 10328:2006 and ISO 22675:2006 include protocols to test the performance and durability of lower-limb prostheses.13,14 For prosthetic feet, ISO 10328 prescribes the following tests in the order presented: static proof test, ultimate strength test, cyclic test, and a final static proof test. Tests can be performed at three different loading levels (P3, P4 and P5) where P5 is the highest loading level and meant for prosthetic components prescribed for heavier individuals. 13 A more in-depth description of these loading levels is presented in the methods section.
A possible solution to the shortcomings in the regulatory mechanisms for prosthetic feet would be for the FDA or CMS to require each product to pass ISO tests before they can be sold or reimbursed in the US. However, this is unlikely to occur without an impetus, such as reported evidence of failure in the field or through independent ISO testing, which is not currently the case. Geil et al. (2001) conducted cyclic testing on 11 prosthetic feet and recommended classifications based on stiffness and hysteresis. 15 Another study by Zeller 16 investigated the stiffness properties of prosthetic feet under various cross-slope conditions, and reported significant differences in stiffness among feet of the same brand. The only study we have identified that reported ISO 10328 results was by Jensen and Treichl 17 , which tested 21 prosthetic feet commercially available in developing countries. None of the feet passed the standards, reportedly due to the fact that they were made of substandard materials such as rubber, polyurethane and ethyl-vinyl acetate. Jensen also reported a significant relationship between internal architecture, quality of material and failure. 17
With a goal similar to Jensen and colleagues, we performed this study to better understand the performance and robustness, according to the ISO 10328 testing standards, of commercially available prosthetic feet commonly prescribed to injured service members who wish to return to active duty or maintain an active lifestyle. We hypothesized that not all of these feet would pass the ISO 10328 standards at the highest loading level due to shortcomings in engineering or materials, as found by Jensen. Furthermore, we sought to identify whether the performance of these devices (e.g. stiffness and dampening) changed as a result of these tests. We also hypothesized that the prostheses would show a reduction in stiffness and an increase in creep due to the cyclic portion of the ISO 10328 standards. As with the Jensen study 17 and several others related to wheelchair durability,9-12 the outcomes may have an important impact on product selection, design and regulation.
Methods
Prosthetic feet from three different manufacturers were obtained for testing to the ISO 10328 protocol. The feet selected were three Sierras from Freedom Innovations, three Re-Flex VSPs from Ossur and three Pathfinder IIs from Ohio Willow Wood, resulting in a total sample size of nine. These particular models were selected because they are the ones most commonly prescribed to wounded service members by the Veteran Health Administration and the Armed Forces Amputee Patient Care Program, based on suggestions from clinicians at Military Treatment Facilities (MTFs). The prostheses and their important characteristics can be seen in Figure 1 and Table 1.

The three feet investigated in this study: Sierra (left), Re-flex VSP (middle), and Pathfinder II (right).
Important characteristics of tested prostheses.

To ensure that regular production feet were obtained for the study, vendors were not informed that the prosthetic components would be tested. Each foot was inspected and photographed prior to testing to ensure that no visible defects were present that could affect results. The feet were tested in a randomized order to minimize testing bias. While the Re-flex VSP and Pathfinder II both possess shock-absorbing components, the stiffness of the shock-absorbing unit on Pathfinder II feet can be altered by a clinician to properly adjust the prosthetic for a given patient. The Pathfinder II feet were tested with their shock-absorbing unit pressure set to 40 psi, which is the manufacturer’s pressure setting.
A jig was fabricated to hold the feet according to specifications found in ISO 10328, which can be seen in Figure 2. The jig was constructed so that the longitudinal axis of the foot was 7° off axis (a ‘toe out’ position), the forefoot loading platen angle was 20° from the vertical, and the heel loading platen angle was 15° from the vertical.

Prosthetic foot in jig constructed to ISO 10328 specifications.
All testing was performed with a testing frame (858 Bionix II, MTS Corporation, Eden Prairie, MN) with hydraulically actuated pistons fitted with axial load cells, linear variable displacement transducers (LVDT), and low friction platens applying force and displacement to the prosthesis. The loading surface of the platens and the prosthetic feet were made low-friction by adding Teflon sheets and Teflon tape, respectively, resulting in a friction coefficient of approximately 0.05.
In order to simulate the variety of loading conditions prosthetic feet may experience, the ISO 10328 testing protocol is divided into four sequential sections: an initial static proof test, an ultimate strength test, a cyclic test and a final static proof test. These tests can be performed at three increasing loading levels: P3, P4 and P5. According to Annex B of the ISO 10328 standards, the loading levels are based on locomotion data collected from amputees. 13 The P3 and P4 loading levels are based on data collected from prosthesis users whose body mass was approximately 60 kg and 80 kg, respectively. The P5 loading level is based on data collected from users with a body mass exceeding 100 kg. 13 To simulate the most extreme usage, the P5 loading level was used for all tests.
Before the series of tests, the foot was loaded into the jig and the low-friction platens set to a zero displacement position, determined by the point at which the platens made initial contact with the heel or forefoot portion of the prosthesis.
The first test performed was the static proof test, which simulates a sustained load of double the body weight of a 100 kg individual. This test entails sequentially loading the heel and then the forefoot of the prosthesis to 2240 N at a rate of 175 N/sec, and maintaining that force for 30 seconds before ramp-down. The ramp-down was programmed so as to allow the platens to back off to the zero displacement position in displacement control over a ten second period.
The next portion of the standard was the static ultimate test, so named not because it is a test to failure, but because it simulates an acute prosthesis overload of four times the body weight of a 100 kg user. This test consists of loading the heel and forefoot sequentially to 4480 N at a rate of 175 N/sec with no hold period. Once again, after reaching the maximum load of 4480 N, the platen immediately backs off in displacement control to the zero displacement position over a ten second period.
Next, the cyclic test was performed on the foot, which involved sinusoidally loading the heel and forefoot alternately between 50 and 1330 N at a frequency 1 Hz. Lastly, after 2,000,000 cycles, the ISO 10328 standard prescribes a final static proof test identical to the initial static proof test.
The models were visually inspected by the author after each test and at regular scheduled intervals during the cyclic test, to look for any damage (i.e. fractures or cracks) visible to the naked eye on the surface of the prosthesis. Visual inspection was used because a prosthesis user or a clinician in the field would be limited to this type of inspection. If there was no visible damage during or after the battery of testing, the foot was considered to have passed the ISO 10328 standard. During all tests, force and displacement data were collected from each platen’s load cell and LVDT for further analysis. From this data, stiffness and creep information was obtained using Matlab (version R2009b). Stiffness was obtained by finding a linear best-fit approximation of the slope of the force-displacement curve during the loading portion of the initial and final static proof test. Creep was calculated by finding the difference between the first and last displacement values during the initial and final static proof tests.
To investigate whether a given model foot suffered internal or non-visible damage during the cyclic test, a two repeated measures ANOVA with a Tukey post-hoc test were used to determine any differences in stiffness or creep between initial and final static proof tests. A non-parametric Kruskal-Wallis test was used to determine whether the prosthetic feet models were affected differently by the cyclic portion of the standard, by comparing stiffness and creep experienced during the final static proof test. All statistical analyses were done with SPSS (version 16) with a significance level of 0.05.18,19
Results
All feet were considered to have passed the ISO 10328 standard at the P5 loading level because no visible damage was detected on the prostheses during or after each section of testing. To further differentiate the behaviour and robustness of the feet, force and displacement data from the initial and final static proof tests were analysed to ascertain the stiffness and creep experienced by each section of the prosthesis (forefoot and heel). Table 2 summarizes the means and standard deviations (SD) of this data:
Summary of stiffness and creep data from initial and final static proof tests.
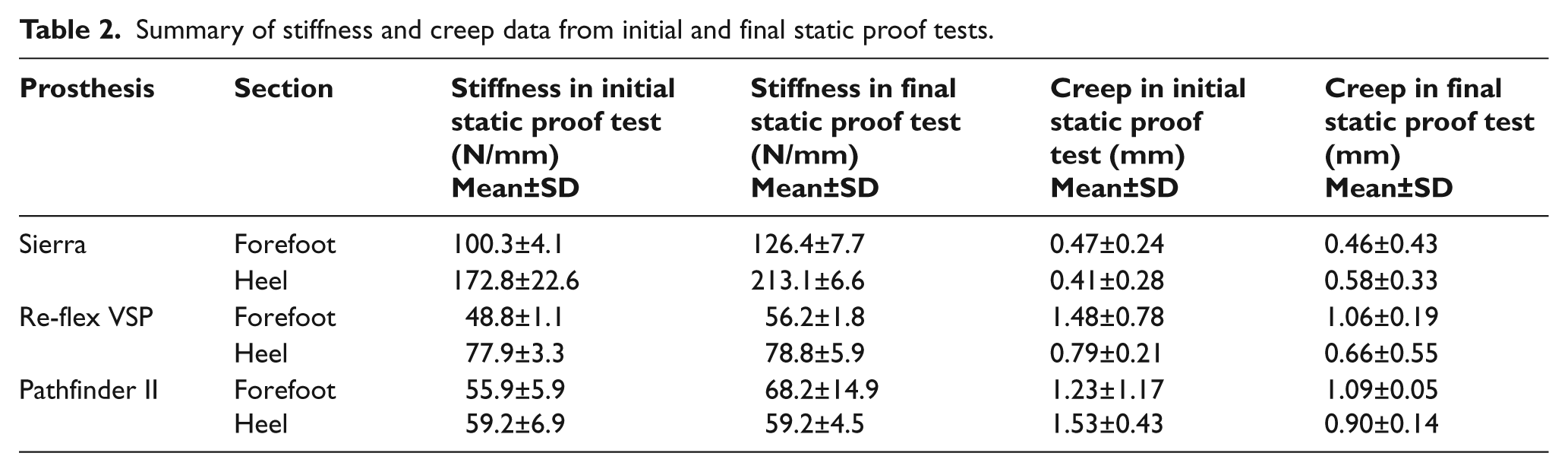
Table 3 summarizes the results of the repeated measures ANOVA test with a Tukey post-hoc test.
Summary of repeated measures ANOVA comparing stiffness and creep between initial and final static proof tests for a given model of prosthesis.
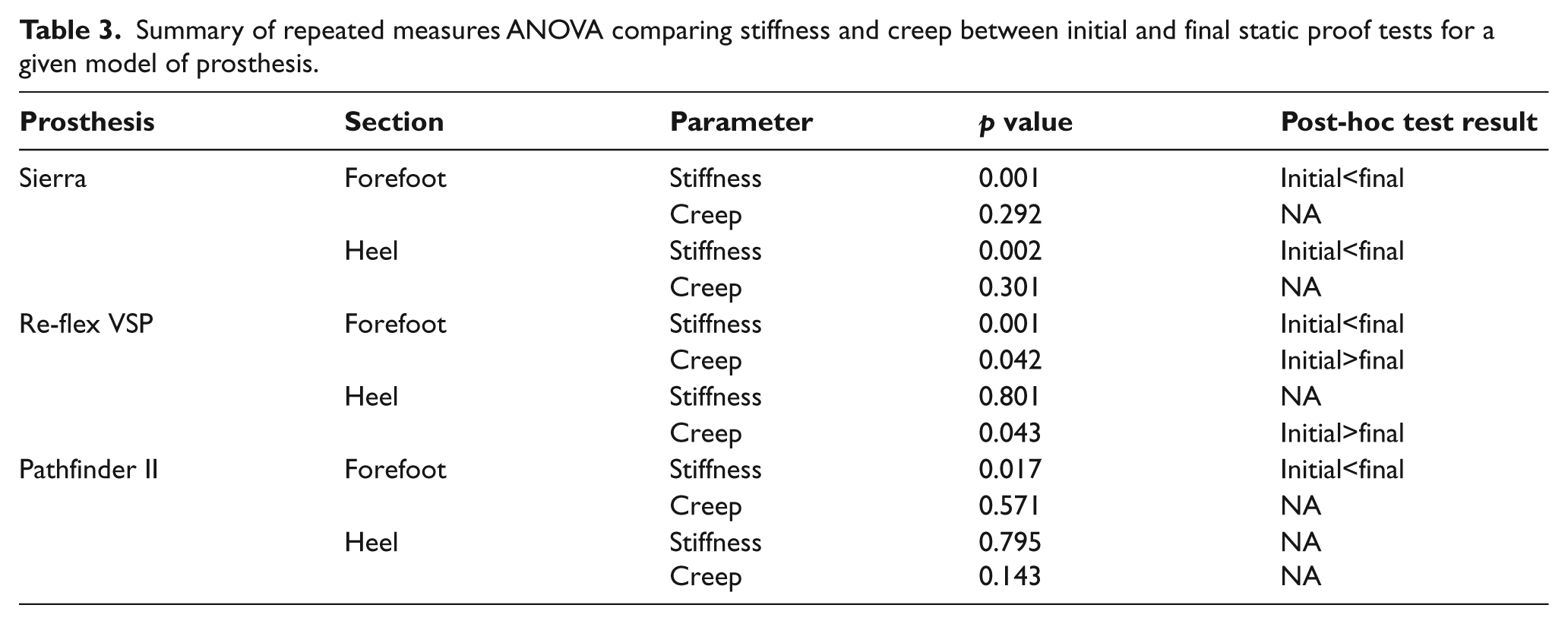
Finally, the Kruskal-Wallis result indicated no differences in stiffness (p=0.393) or creep (p=0.193) among the three models of prosthetic feet during the final static proof test.
Discussion
All heavy-duty prosthetic feet tested passed the ISO 10328 standards at the P5 loading level. This result contradicts our major hypothesis and suggests that the particular models tested and their manufacturers adhere to the voluntary ISO standards. Lower-rated prosthetic components may perform differently, as Jensen and colleagues17,20 found for low-cost prosthetic feet, such as those available in low-income countries. While this study focused on high-cost prostheses intended for use by military service members and other active individuals, further study is necessary to determine whether lower-cost feet available in the US meet the ISO 10328 standards.
Usually, materials exposed to fatigue tests, such as the cyclic test prescribed by the ISO 10328 standards, experience a reduction in modulus and an increase in creep. 21 Since the modulus of the prosthetic feet could not be determined by the test methods used in this study, stiffness was used as an analogue for the modulus. After the repeated loading experienced by each prosthesis during the cyclic test, we expected a decrease in stiffness from the initial to the final static proof test, and an increase in creep because of internal damage propagation. As shown by the repeated measures ANOVA test of this data, in many cases the exact opposite occurred. This may be due to cycle-dependent hardening, which some materials experience during fatigue tests, especially those tested at stresses well below the yield stress of the material. 21 Since these prosthetic feet are composed of several different materials and the testing was purely structural, we cannot be sure which component or components experienced this hardening.
Even though the Kruskal-Wallis test showed no significant differences in stiffness or creep during the final static proof test, a potential interpretation of the data in Table 2 may be that the Sierra feet are the most robust, because the trends indicate higher stiffness and lower creep compared to the other models tested. However, the Reflex VSP and Pathfinder II possess shock-absorbing components while the Sierra does not. This key difference could affect stiffness and creep results, since feet with shock-absorbing capability are designed to deform much more under load and to dissipate this energy during gait, providing a smoother step than a foot without shock absorption. Further investigation should be done to differentiate the effectiveness and robustness of shock-absorbing versus non-shock-absorbing prosthetic feet.
It is important to note a few limitations of this study. First, only three feet from each manufacturer were tested, resulting in a sample size of nine. Due to the length of the cyclic testing (over three weeks), it is extremely time-consuming to test additional feet to reach a more powered sample size. Also, calculating stress and measuring strain during the tests would paint a more vivid picture of how the prosthesis materials react to the loading conditions in the ISO 10328 standards.
An important limitation in applying the ISO 10328 standards to evaluate the robustness of prostheses used by active individuals is that these standards only address durability under the loading conditions of an idealized gait. These conditions may not be representative of actual performance during use. Current tests are uni-axial, simulating the gait cycle during fatigue testing, and acute overloading during proof and ultimate strength testing. The prosthetic feet used by active military personnel with lower limb amputations can be exposed to many different loading conditions, such as those caused by moving over uneven terrain, donning and doffing heavy equipment, or side-stepping maneuvers. Lateral and torsional loads that may occur when performing these activities are not applied to the foot during testing. 22 Consequently, failure modes that may occur during these maneuvers are not addressed during ISO testing, and thus design deficiencies would be unknown prior to commercialization. Failure of these components under critical circumstances in combat could lead to additional injuries and could potentially be fatal. With this in mind, it may be necessary to include tests that apply torsion and bending in addition to uni-axial loading. Moreover, standards to determine the true robustness of prosthetic feet should include destructive testing, such as tests to simulate sudden impact and torsion to failure, which would be expected for a soldier during combat. Additionally, the ISO 10328 standards are performed at room temperature, whereas the prosthetic feet of service members could experience extremes of heat, cold and humidity. Jensen and Heim 23 subjected prosthetic feet to various forms of environmental exposure (moisture, UV), which had a negative impact on durability. Similar results may occur if heavy-duty prosthetic feet were exposed to extreme environmental conditions.
The results of this study offer several directions for future work. More in-depth evaluation of the performance of prosthetic components in the laboratory and field is critical, in order to observe how they fail, the frequency of failure, and the conditions under which they fail. As in the wheelchair sector,24-27 such real-world reports are valuable to help determine the scope of the problems and how best to address them. A recent survey of 2213 wheelchair users found that 44.8% of respondents reported maintenance issues with their devices within the previous six months. 28 Similar failure reports for prostheses are needed to develop multi-axial testing protocols so that testing can more accurately simulate real-world conditions. This work will likely require more laboratory testing, such as static and cyclic tests to failure, user and clinician surveys, and in-lab gait studies to measure the ground reaction force of manoeuvres under which the prosthetic components fail.
Conclusion
This goal of this study was to determine whether the prosthetic feet commonly used by active duty military service members meet ISO 10328 standards. The findings showed that, even though these are voluntary standards in the US, all prostheses tested passed the standard. Further study in the laboratory and the field is necessary to develop standards for prosthetic feet to accurately address the needs of military personnel and other active prosthesis users, and to demonstrate definitive differences in the robustness of prosthetic feet.
Footnotes
Funding
This study was funded by the Telemedicine and Advanced Technology Research Center under contract number W81XWH-07-1-0716.
Conflict of interest
The authors report no conflicts of interest. The contents of this paper do not represent the views of the Department of Veterans Affairs or the United States Government.