
Abstract
Background and Aim:
For infants and small toddlers with congenital upper limb deficiencies, terminal devices mainly provide either cosmesis or functionality. We report a clinical note about fitting a child with a low-cost passive hand targeting both functionality and cosmesis.
Technique:
An elastomeric, alloy-wire-reinforced hand was fabricated using additive manufacturing to allow independent positioning of the digits. A clinical pilot in-home evaluation was conducted on a child with upper limb loss.
Discussion:
The fabricated hand met the functional requirements but required a cover for cosmesis due to a poor surface finish associated with the fabrication technique. The participant child was comfortable using the prosthesis for various tasks. The parents were satisfied with the hand’s function and cosmesis when covered with a cosmetic glove. This work demonstrated a new design and process that may in the future improve the utilization of prosthetic hands to promote early prosthesis use and a child’s development.
Clinical relevance
Early prosthesis use is important for infants and toddlers. Additive manufacturing may enable the fabrication of custom passive prosthetic hands that provide both cosmesis and functionality.
Keywords
Background and Aim
Children with congenital upper limb absence are born with one or two atypically formed or missing arm segments. For limbs terminating below the elbow, it is valuable to fit the first prosthesis as soon as the child begins to sit, that is, at the age of 3–7 months.1–4 Initially, a passive prosthesis is provided that supports various activities such as bi-handed object holding and weight bearing, while encouraging eye-hand coordination.5,6 As such, symmetrical muscular development is promoted and there will be less burden on the intact limb.
Currently, a number of options are available for the first prosthesis. Among them, TRS Inc. has a line of products that can be fit for children starting from the age of 4 months. Basic object holding is possible with these products that are durable and soft, but not cosmetically appealing. A prosthetic hand is available from Otto Bock for 6-month-olds, which replicates the anatomical hand more closely in terms of positioning and materials. Nevertheless, unilateral holding is rather difficult due to its relaxed, open-hand position. These existing gaps leave space for small-scale designs that integrate both high cosmesis and functional aspects.
The motivation for this project was a clinical case involving a prematurely born infant. The infant was an 18-month-old female client with a unilateral trans-radial amputation. She was using the Physiolino Babyhand (Otto Bock HealthCare GmbH, Duderstadt, Germany) for 7 weeks prior to this study. However, weighing only 17 lb, the child’s small physical size necessitated a compact hand that was functional for the child’s age and developmental stage and deemed cosmetically acceptable by the parents. Therefore, the goal of this study was to design, fabricate and test a functional and cosmetically acceptable hand prototype for this presented case; the goal of this report is to inform clinical care of infants and small toddlers with trans-radial congenital limb absence.
Technique
Decisions regarding the design’s size, functionality and appearance were informed by suitability to the identified client, who required a cosmetic prosthesis with greater functionality and a smaller size than is currently available. Hence, the design was restricted to sizes typical to children between 3 and 18 months of age and then customized in size to the client being treated. Materials were selected based on performance and cosmesis.
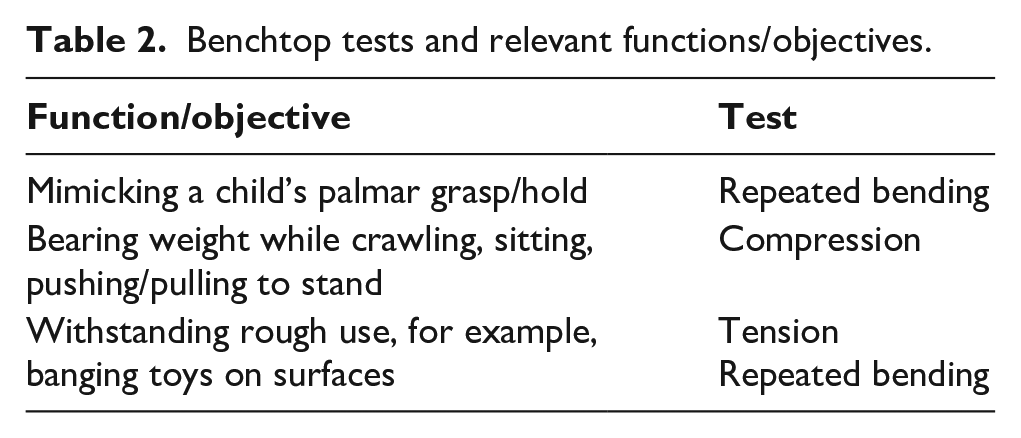
The prototype is a single-piece hand-shaped device with separated digits reinforced with a malleable metallic core (Figure 1). The hand was fabricated using additive manufacturing with a flexible material, providing a soft, fleshy texture but at the same time maintaining stiffness for weight-bearing activities. A three-dimensional (3D) printer (RepRapPro, London, United Kingdom) was modified by changing the extruder to direct drive to utilize an elastic material: FilaFlex® – flexible thermoplastic elastomers (TPE) (Recreus Industries S.L., Elda, Spain). While FilaFlex® UltraSoft is designated as a non-toxic material, it has not yet been approved for medical or nutritional use. Hence, for safety reasons and to improve the overall appearance, the hand was covered with a common polyvinyl chloride (PVC) cosmetic glove. The metallic core, made of 14-gauge stainless steel wire, allowed digits to be individually positioned and to retain their shape, enabling palmar and bilateral holding activities (Table 1). Each digit included notches to control the metallic core bend radius and locations, as shown in Figure 1. Benchtop testing of the prototype was done to ensure functionality, structural integrity and safety (Table 2).
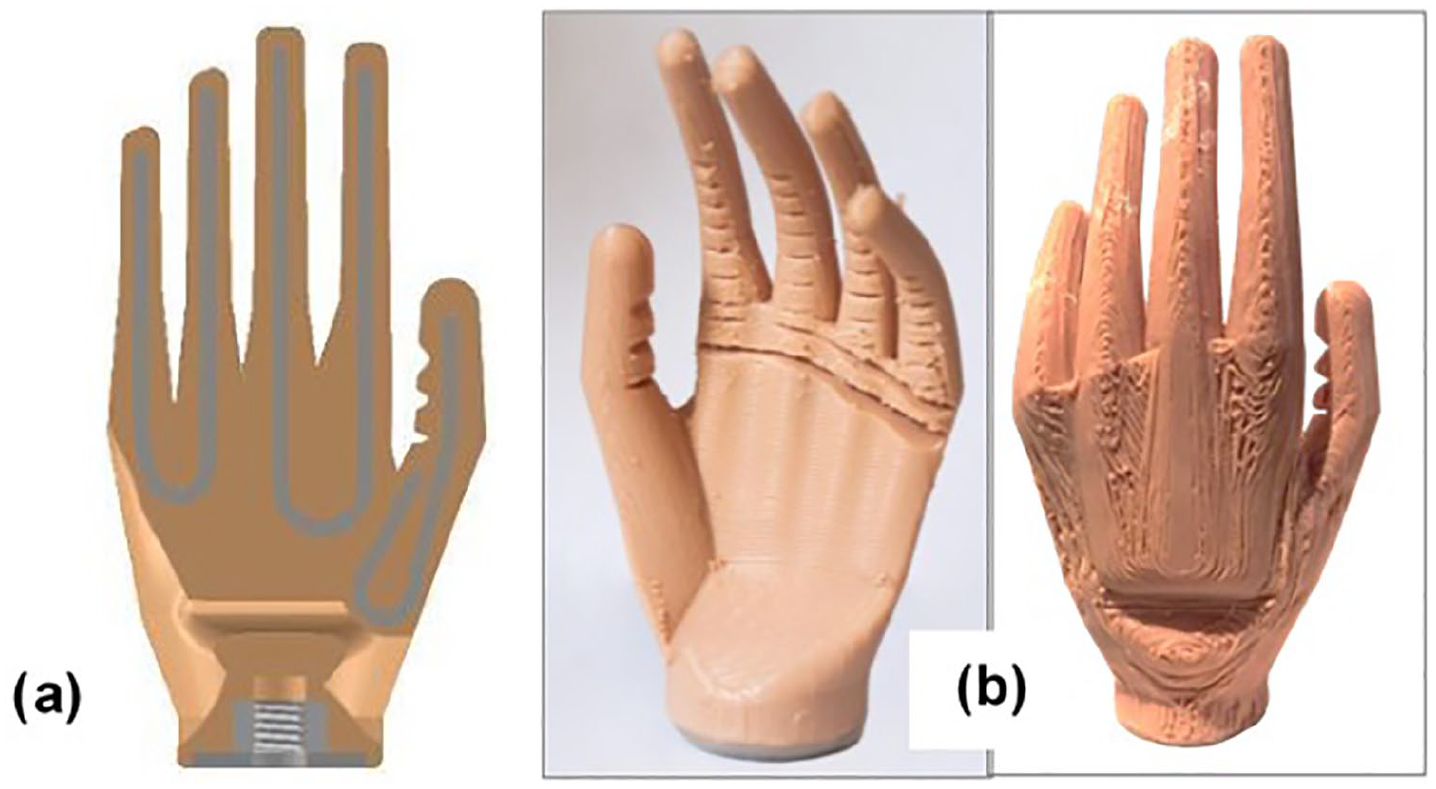
(a) Final CAD model with wire placements; (b) the final prototype hand.
Overall design specifications.
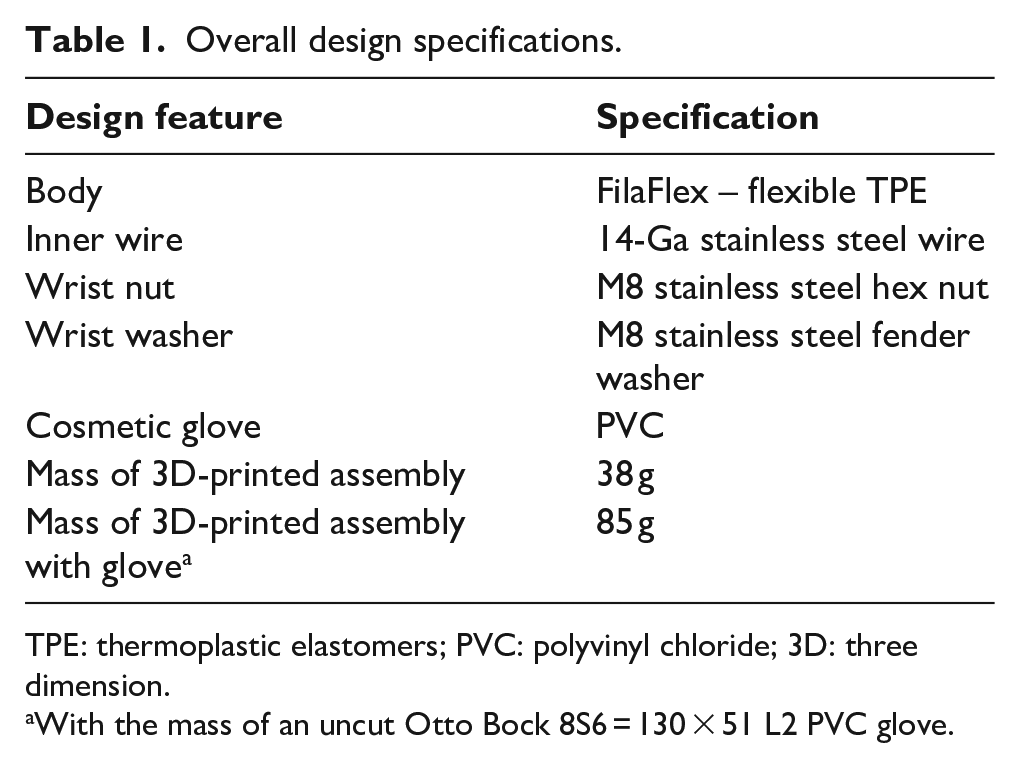
TPE: thermoplastic elastomers; PVC: polyvinyl chloride; 3D: three dimension.
With the mass of an uncut Otto Bock 8S6 = 130 × 51 L2 PVC glove.
Benchtop tests and relevant functions/objectives.
Ethics approval for this study was granted by the Holland Bloorview Research Ethics Board, and written consent was provided by the participant’s parents. The planned evaluation consisted of one controlled testing session at the clinic, and one take-home field evaluation. 7
At the on-site test session, the child was fitted with the prototype prosthetic hand by a certified prosthetist using her existing prosthetic socket. The child was encouraged to attempt a series of weight-bearing activities and to interact with toys. The parents were also asked to comment on the prototype’s appearance and texture, and to gauge the infant’s comfort while using the prosthesis. 8 Qualitative observations were recorded for the success of each attempted activity in a series of prescribed holding tasks.
Objects were secured into the prosthetic hand by the therapist and/or parents for unilateral and bilateral activities, as follows:
One toy held in prosthesis and waved around (unilateral);
Toy in prosthesis pulled out with natural hand (bilateral);
Container held in prosthesis while sound hand inserted beads (bilateral);
One toy held in both hands and squeezed/stretched (bilateral);
One toy held in each hand and banged together (bilateral);
Cart held with both hands and steered/lifted (bilateral).
As clinical experience suggests, what a child ‘does do’ in daily life (performance) and ‘can do’ in a clinical setting (capacity) may differ. 9 Thus, after the on-site session, the parents took the prosthesis home to observe and record its performance in everyday home-environment usage. The parents were asked to guide the child through the same set of activities as during the on-site session and to attempt any other activities at their discretion. The duration of the field trial was 1 week, and the child used the prosthetic hand for several hours per day based on the parents’ feedback.
Discussion
This work aimed to develop a prosthesis that is both functionally and aesthetically designed for small infants with congenital trans-radial amputations. This study represents a unique example of the application of elastomeric and flexible materials, and the fabrication of a composite-type structure using additive manufacturing. Similar structures are conventionally fabricated by moulding, which requires a high upfront investment for tools, and limits customizability (including size) to accommodate the growing child.
All of the unilateral and bilateral object-holding activities were performed successfully using toys of various shapes and sizes (Figure 2). The only difficulties observed were with objects that required a tight hold, such as smooth plates and thin rods due to bending resistance, possibly due to additional stiffness from the outer glove. Though the weight-bearing tasks (e.g. pulling/pushing to stand, crawling and leaning forward with both hands while sitting) were achieved with minimal difficulty, the child tended to not bear weight on the hand with the palm down. In addition to the above-planned activities, the following other activities were observed: clapping, giving high- and low-fives, repositioning prosthesis on her own (wrist rotation) and banging on a keyboard.

The child performing various tasks.
The child often behaved as if there was no prosthetic hand and aimed to make contact with objects at the terminal end of the residual limb instead. This may be an indication that the child had not ‘incorporated’ the prosthesis into her body-image, as she had only been using a prosthesis for 7 weeks prior to this study. It is not known if the child wore this initial prosthesis on a regular basis. Overall, the parents were pleased with the functionality of the device and found it to be an improvement over the child’s existing prosthesis. The child’s parents found it to be lifelike in overall appearance and texture when used with the glove on. However, there were concerns about the shape when held in a fist and the placement of the thumb. As for the bare 3D-printed hand, they suggested improvements regarding the surface texture (print quality) and thought the fingers were too thin, but recognized that the current device is intended to be used with an outer cosmetic glove.
There were some difficulties regarding fit. The prototype was manufactured to be compatible with the participant child’s existing prosthetic forearm socket. There was some difficulty with threading, as the socket bolt was too short for the wrist nut to thread all the way on, but the connection remained secure throughout the entire test session. To address this issue, a washer was inserted and the nut was shifted proximally to be flush with the washer.
The glove itself also presented some problems, as the glove was larger in certain areas than the inner body. This meant that the glove was loose, which resulted in kinking and twisting around the wrist and palm, and slippage in the fingers. Frequent repositioning of the device was therefore required.
Future work is needed to evaluate this technique in a larger group of subjects. While additional work is required to improve both the function and cosmesis of our initial design, and the related additive manufacturing processes, these early promising results provide the necessary basis for future development. Moreover, as additive manufacturing equipment and techniques continue to improve, so should the capabilities of producing customized prosthetic components. Further development of the 3D printing manufacturing process will enable multi-material printing, whereby a thin layer of flexible nylon could be printed to encase the wires within the flexible TPE to decrease the risk of puncture or tearing.
The wire material and structure could be further developed to improve the fingers’ ability to sustain more cycles of repeated bending. Alternatively, if bending durability is limited such that a new hand is needed before the user outgrows their prosthesis in size or capability, the hand could be replaced at regular intervals before the fingers are expected to fail, made possible by the low cost of materials and manufacturing.
The material and external appearance of the hand could also be further developed to achieve a design that does not require a cosmetic glove. This may require the printer parameters to be tuned more optimally to achieve a smoother, more cohesive surface than what was achievable with the team’s current manufacturing capabilities. Surface correction techniques could also be employed to smooth the surface post print.
A gloveless design would also enhance customizability, and reduce cost given that the glove accounted for over 90% of the total cost of the prototype. Testing to ensure all materials are food-safe would be required in a gloveless system. A final consideration for future work is the application of 3D scanning to achieve the aforementioned enhancement of the aesthetic appeal, through capturing the geometry of the user’s intact hand and to manufacture the prosthesis to match. A comparative evaluation involving other commercial hands such as the TRS should be conducted as part of future work.
Key Points
A rubbery prosthetic hand was fabricated using additive manufacturing.
Embedded malleable wires within a flexible material minimized manufacturing complexity, considering small hand sizes required for an infant hand.
Pilot trial results indicate that the design may meet the physical needs of infants and small toddlers.
Footnotes
Authors’ Note
Matthew Leineweber is also affiliated with Holland Bloorview Kids Rehabilitation Hospital.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was generously supported by the Centre for Leadership thanks to donors of the Holland Bloorview Foundation.