
Abstract
Background:
Usable myoelectric control relies on secure and intimate contact at all times between the electrode, the socket and the residual limb. At present, there is little post-fitting socket adjustment available to prosthetists with respect to electrode contact security or alignment. Failure to provide secure electrode contact could result in the development of motion artefacts, poor prehensor response and subsequent prosthesis non-usage.
Objectives:
To establish the effect of alteration to electrode contract security and alignment on prosthesis functionality using a bespoke electrode housing unit.
Study design:
This study investigated the effect of electrode contact security and alignment on upper limb myoelectric prosthesis functionality.
Methods:
Four different electrode housing arrangements were assessed within prosthetic sockets fitted to six transradial prosthesis subjects using the Southampton Hand Assessment Procedure, which is a reliable and validated prosthesis functionality assessment tool.
Results:
Significantly higher functionality scores were achieved with the bespoke housing unit compared to when using conventional electrode housings.
Conclusion:
Myoelectric prosthesis functionality is closely linked to electrode contact security and to electrode alignment with respect to the residual limb. Both of these factors can be improved locally using an adjustable electrode housing unit.
Clinical relevance
Provision of an electrode housing system that enables adjustments to be made to electrode orientation can improve prosthesis functionality, particularly in cases where tight-fitting sockets are not possible, and/or where the prosthetist may be inexperienced with regard to myoelectric prosthesis fitting.
Background
Upper limb myoelectric prostheses are controlled by myoelectric signals produced by muscles that remain within the residual limb. These signals are acquired via dry surface electrodes housed within the inner walls of the prosthetic interface, or ‘socket’. The conventional solution to create a semi-rigid mounting for myoelectric electrodes by all the major manufacturers is to fix them into position using stiff rubber locating rods within fixed housings created during the socket manufacturing process.
Although the literature related to this specific area is limited, a review has suggested that adult rates of rejection of myoelectric prostheses are over 20%; with rates of non-use being of a similar order. 1 The reasons for rejection and/or non-use are varied, but prosthesis users are consistently requesting improvements in prosthesis functionality. 2 Interestingly, 68% of those with upper limb absence who do not use a prosthesis would reconsider this decision if technological improvements were made to prostheses at a reasonable cost. Although it is widely believed anecdotally that inconsistent response and unwanted activation of the myoelectric device may be apportioned to the production of motion artefacts within the myoelectric acquisition process,3–6 research within this area is also limited.
It is generally accepted that effective signal acquisition depends upon the electrodes being securely attached to the skin’s surface, and also placed along the long axis of the target muscle fibres.7,8 In addition, maintaining the electrode positioned along the long axis of the muscle fibre has been shown to maximise the acquired signal strength since the signal acquired will comprise the summative voltage of all the fibres that are detected by the electrode.3,7 Misalignment of the electrodes can also increase the chance of cross-talk, where muscle fibres from muscles other than the target muscle may be transduced and hence affect the operation of the prehensor. 8
Anecdotal evidence suggests that standard clinical practice is to place the long axis of the electrodes on an area parallel to the long axis of the residuum with maximum signal strength; this can be ‘trial and error’, particularly in paediatric cases. 9 Providing an electrode site that will produce a clear, usable signal on the positive plaster model is also challenging, particularly for clinicians inexperienced in fitting myoelectric prostheses. Indeed, clinicians report that many myoelectric control problems emanate from a lack of electrode placement consistency over the appropriate sites.10,11
Given the importance of appropriate location, plus a secure electrode–skin interface and appropriate alignment of electrodes relative to the muscle, it is surprising that current designs of myoelectric electrode application allow for little or no adjustment of the location or orientation with respect to the anatomy once the electrode is fitted into its housing within the prosthetic socket. The electrodes used in most myoelectric prostheses are dry, differential electrodes fixed within the walls of the socket into specifically manufactured housings using semi-rigid locating rods. Consequently, they do not allow for adjustment of skin–electrode contact security pressure. The housings enable the electrodes to be conveniently inserted and removed, but do not allow for adjustment of electrode orientation relative to the anatomy.
In this study, an adjustable electrode housing was used to examine the relationships between electrode and skin contact security and variations in electrode alignment with prosthesis functionality. This was achieved using myoelectric sockets adapted with a newly designed and novel electrode housing device, which was able to offer three different alignment orientations with respect to the residual limb while attached to the socket. It also enabled contact security between the electrode and the skin to be adjusted. The functionality available from the electrodes located within this housing unit was contrasted with the respective functionality available from electrodes located in standard housings. A validated, reliable functionality assessment procedure, the Southampton Hand Assessment Procedure (SHAP), was used to perform the functionality assessments. 12
Methods
Prior to the commencement of the study, ethical approval was received from the appropriate UK National Health Service Central Office for Research Ethics Committees (NHS COREC) and the University of Salford Ethical Committee. Six transradial prosthesis users with experience of using myoelectric control were recruited for this study. Volunteer subjects were required to be experienced in using a myoelectric prosthesis, be aged over 18 years with transradial limb absence from any relevant cause and have acceptable cognitive ability to be included in the study. All volunteer subjects signed a consent form after reading a subject information sheet.
A self-suspending transradial myoelectric socket was manufactured for each volunteer transradial prosthesis user; the specific type being selected in accordance with the corresponding residual limb length (Table 1). The electrode sites used within their existing prosthesis were determined as being the most suitable for myoelectric signal acquisition and hence were also used within this study.
Subject information and residual limb length, plus socket type provided.
A bespoke endoskeletal prosthesis was also manufactured, which allowed each socket for each patient to be interchanged and assessed with the same componentry. A plastic tubular unit was also manufactured into the distal aspect of the socket. This unit enabled the insertion of an aluminium tube, which in turn was connected to a screw-fastening wrist unit. An RSL Steeper ‘Select MYA775’ myoelectric hand was then attached to the wrist unit. The aluminium tubes were manufactured to suit the specific length needed in accordance with each subject’s anthropometric measurements.
Each myoelectric socket, for each separate subject, could therefore be fitted with the same components as their peers, thereby limiting the effects on the results of design factors not directly associated with the socket. As described in detail below, the socket was designed to accommodate a removable electrode housing unit. Two types of electrode housing units were used in the study, one a clinical standard, with a fixed electrode housing position (see Figure 1), and one the bespoke experimental (see Figure 2) unit that enabled the electrode to be secured within three distinct orientation positions about an axis approximately normal to the skin surface.
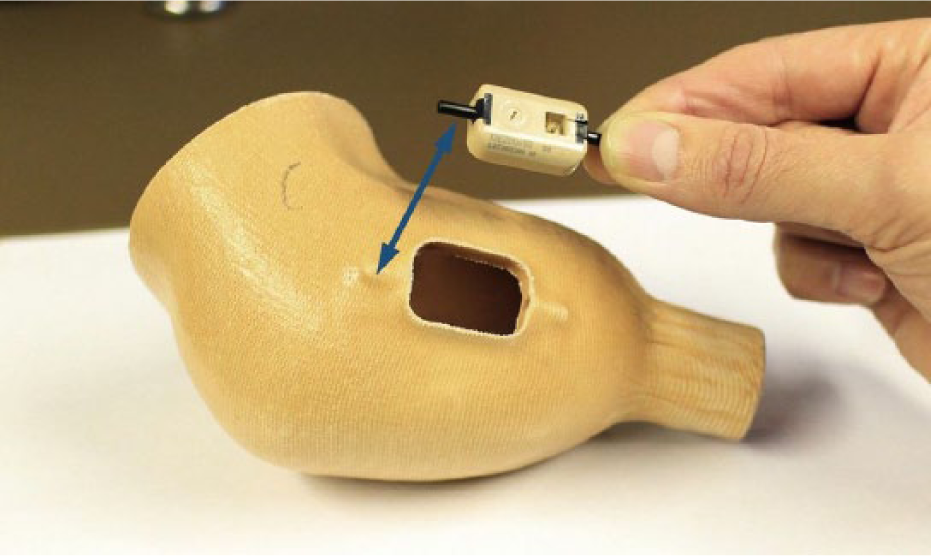
The standard housing arrangement; the semi-rigid rods slot into the holes created at each end of the socket aperture.
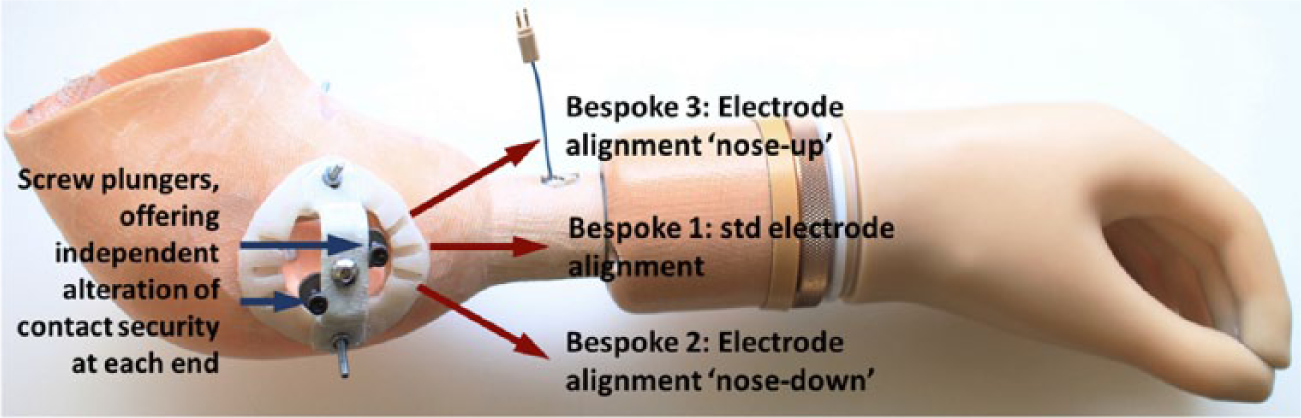
The bespoke prosthesis incorporating the electrode housing unit with three different alignment positions, and screw plungers to adjust contact security.
The bespoke electrode housing unit comprised two plungers mounted on a laminated plastic plate, which were positioned equidistant from a central pivot point on the plate. This central pivot point allowed rotational adjustment to alter the orientation of the electrode beneath it. The two screw plungers facilitated adjustment of the contact security of the electrode across the surface of the skin. The screw plungers therefore enabled the most intimate yet comfortable electrode contact perceived by the prosthesis user to be obtained (the users themselves were able to adjust the unit).
The electrode alignment position providing the clearest, most usable signal for each subject and for each site was determined following a standard clinical assessment undertaken by an experienced prosthetist. The orientation of the electrode relative to the socket selected by the experienced prosthetist was measured using a hand-held goniometer. The angle was measured between the upper edge of the electrode housing and a line drawn joining the medial or lateral epicondyle (depending on which electrode site was being examined) to the distal end of the ulna. The standard electrode housing unit was located in this orientation.
The bespoke housing unit was also designed to be attached to the same position to allow the electrode to be moved from its central axis to provide two other electrode orientations. As a means of estimating a realistic range of electrode–limb orientations to explore, we carried out a preliminary study. A group of 26 inexperienced student prosthetists were recruited onto the study and asked to orientate each electrode in what they considered to be orientation. Two alternative electrode orientations selected as the test positions for this study represented the maximum alignment difference between that determined by the experienced prosthetist, and that determined by the student prosthetists.
A functionality assessment for the bespoke prosthesis for each alignment position was then undertaken using the SHAP, which has been used in a number of previous upper limb prosthesis studies.13–15 The SHAP provides a functionality index score of between 0 and 100; 0 = no hand function, 95 or over = unimpaired hand function.12,14
During the main testing periods, three separate SHAP assessments were carried out for each electrode arrangement, by each subject (see Figure 3). A mean score was then calculated from these three trials.

Subject ‘B’ undertaking part of the SHAP using the bespoke prosthesis and housing unit.
The functionality assessment had to be conducted using the standard electrode housings first, since these would have to be completely removed to allow for the fitting of the bespoke housing unit. However, each subject was provided with at least 20 min of trial fitting and practice prior to the actual initial assessment with the standard housings. Following this, the bespoke housing unit was fitted, and the assessment orders for each electrode position within this unit were randomised, that is, for subject A, the assessment orders were position 1, then position 2 and then position 3 (1, 2, 3); then 2, 3, 1 and then 3, 1, 2. For subject B, the orders were 2, 3, 1; 3, 1, 2; 1, 2, 3 and so on, varying again in order for each subject.
The SHAP functionality scores were obtained for the following test conditions:
A prosthetic socket with the standard electrode housing with the electrode positioned in the perceived optimal alignment via standard clinical assessment (std).
The same socket with the bespoke electrode housing unit attached and with the electrode again in optimal alignment but adjusted using the plungers to improve the perceived contact security experienced between the skin and the electrode surface (bespoke 1: Figure 2).
The same socket with the bespoke electrode housing unit with the electrode rotated along its longitudinal axis by 25° with the distal aspect of the electrode in a ‘nose down’ position with respect to the standard alignment position and again adjusted for perceived contact security (bespoke 2).
The same socket with the bespoke electrode housing unit with the electrode rotated along its longitudinal axis by 25° with the distal aspect of the electrode in a ‘nose up’ position with respect to the standard alignment position and again adjusted for perceived contact security (bespoke 3).
Each designated electrode position was identical for each electrode site, that is, both electrodes were 25° ‘nose down’ in this designated position.
A Friedman’s repeated measures assessment, with post-hoc analysis was performed to assess for significant differences within the data, because the data is non-parametric and this assessment is also suitable for repeated, small samples and related variables.
The hypothesis was that the provision of a bespoke housing unit which would facilitate more precise adjustment to electrode orientation and perceived electrode contact with the skin in an upper limb myoelectric prosthesis would result in improved functionality index scores for prosthesis users when performing pre-determined tasks.
Results
The mean SHAP functionality index scores for each assessment using each test condition are represented in Figure 4 and Table 2.
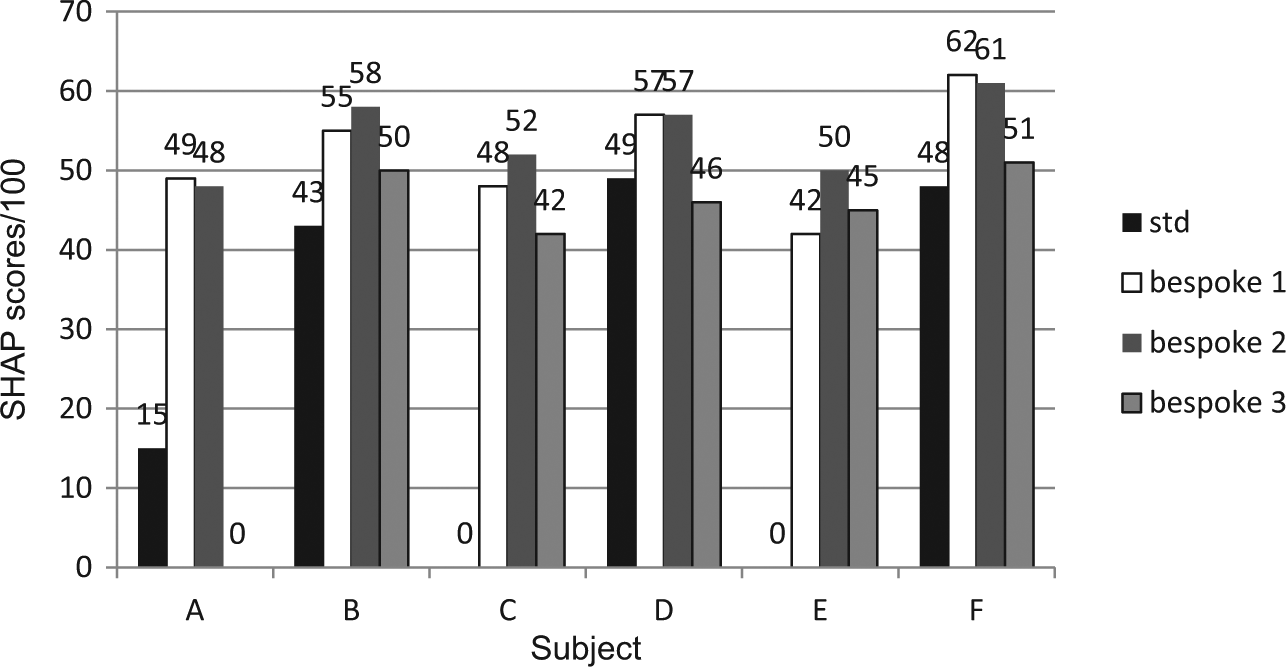
Mean functionality scores from each SHAP assessment with respective electrode alignment positions for subjects A–F.
Mean SHAP functionality index scores.
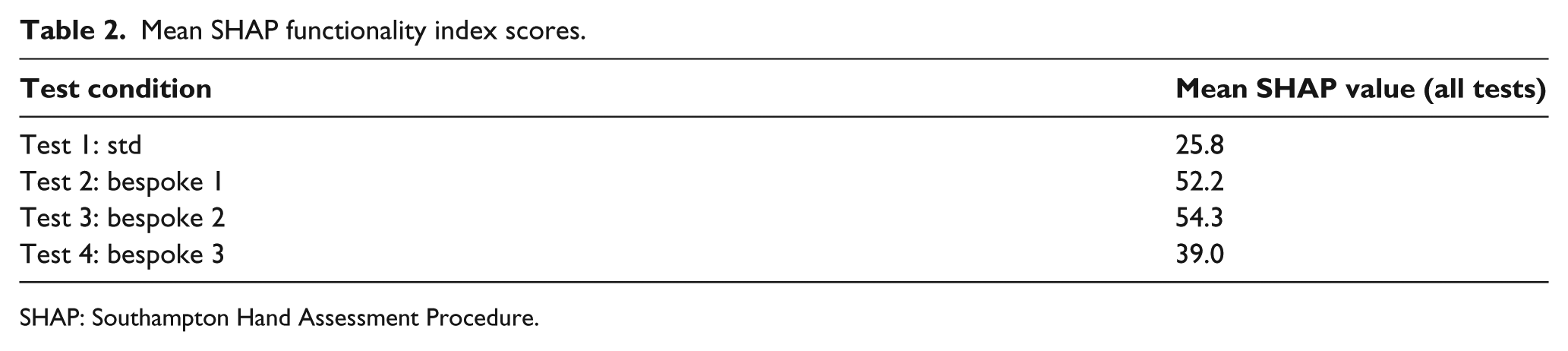
SHAP: Southampton Hand Assessment Procedure.
Please note that subject A acquired a functionality index score of ‘0’ using the ‘bespoke 3’ test condition. Subjects C and E acquired scores of ‘0’ using the ‘Std’ test condition.
Further definitions of the electrode housing positions are as follows:
std. Alignment assessed by an experienced prosthetist, within standard housing;
Bespoke 1. Alignment assessed by an experienced prosthetist, within bespoke electrode housing unit;
Bespoke 2. Alignment within bespoke electrode housing unit rotated 25° ‘nose down’ with respect to alignment assessed by an experienced prosthetist;
Bespoke 3. Alignment within bespoke electrode housing unit rotated 25° ‘nose up’ with respect to alignment assessed by an experienced prosthetist.
The maximum SHAP score when using the bespoke housing (where contact security could be adjusted) compared to the standard housing was significantly increased in all subjects by an average of 88%, where all scores were included (Table 2). Where scores of ‘0’ were excluded, this was still an increase of 32%.
Friedman’s repeated-measures analysis showed a statistically significant difference in prosthesis functionality when using the different housing conditions at p < 0.001, χ2(3) = 35.107. A post hoc Wilcoxon signed-rank test also found a significant difference between the functionality achieved using the standard housing and ‘bespoke 1’ and ‘bespoke 2’, respectively, at p < 0.001. Use of the bespoke 2 housing and ‘bespoke 3’ housing also proved to be functionally significant at p < 0.001. Use of the bespoke 1 housing, when compared to the ‘bespoke 2’ housing and ‘bespoke 3’ housings, respectively, was not significant at p = 0.035. Additionally, functionality achieved via the use of the standard housing when compared to the use of the ‘bespoke 3’ housing was not significant at p = 0.060.
The maximum average increase between the standard housing and the other test conditions was shown by subject E, who had the shortest residual limb among the subject group. The results (Figure 4) showed clear variations between functionality when comparing the standard and bespoke housing units. For user subjects C and E, the standard housing proved unusable. The use of this standard housing also resulted in a poor functionality score for user subject A. Overall, the standard housing produced functionality scores which were the lowest recorded for five out of the six users.
Discussion
Standard electrode housings rely on the prosthetist carefully contouring the appropriate electrode site area onto the positive plaster model. Although anecdotal evidence suggests that washers and/or elastic bands may subsequently be used on the outer surface of electrodes to enhance contact security in conjunction with standard housings, these do not provide the intermittent adjustments delivered by the bespoke housing unit used here. Additionally, standard methods do little to ensure effective contact across the surface of the electrode particularly if the electrode is able to move.
The functionality variations within this study demonstrate that a system that enables electrode alignment adjustment post-casting would be beneficial. Functionality score variations between the different test positions within the bespoke housing unit were generally smaller than contrasting scores achieved using the standard housing. Nevertheless, there were significant differences between the score for ‘bespoke 3’ and the scores for ‘bespoke 1’ and ‘bespoke 2’, respectively. Electrodes rotated 25° in a ‘nose up’ position with respect to the standard position (‘bespoke 3’) produced a significantly larger reduction in prosthesis functionality than electrodes rotated 25° in the relative ‘nose down’ position (‘bespoke 2’). This is despite the fact that the electrode contact security could be adjusted using the bespoke housing mechanism in all these cases. For subject A, electrodes housed within ‘bespoke 3’ proved unusable.
It is therefore important to recognise these factors when determining electrode alignment, particularly as they can lead to a significant change in the resultant functionality of the prosthesis. The aim of this study was not to pinpoint ‘optimal’ electrode alignment but to provide an assessment of the effect of alignment variations that may realistically occur using a pool of inexperienced prosthetists. Although electrode alignment has previously been shown to have a more significant effect on signal strength than contact pressure in a generic context, 7 this study used practical manipulation assessment to show that both factors can have a significant effect on prosthesis functionality. The adjustable bespoke unit used within this study mirrors the evident adjustability of other types of prosthesis control. For example, in lower limb prostheses, control is achieved through alignment of components after initial fitting.
It should be noted that there are some limitations to this study. The study involved a relatively small number of subjects. The myoelectric equipment used was functional, but not the latest design, and no glove was used. The assessment had to be performed first using the standard electrode housing because this housing was permanently removed to allow for the fitting of the bespoke housing unit. The assessment order, and the effect of practice learning using the SHAP, could also have skewed the results. Repeating with a revised assessment order, as well as repeating with a different assessment battery, such as Box and Block, could improve our understanding of the results and their significance.
In addition, congenital users have musculature which is less well-developed than that of traditional amputees, potentially leading to a reduction in signal usability. Taffler and Kyberd 16 demonstrated that electrode orientation in congenital subjects was less critical than those with normally developed muscles (i.e. amputees). This may make the differences between the electrode orientations less pronounced in the cases of those with congenital absences, compared with the amputees. With these factors in mind, further investigations are planned along with variations in equipment and cosmesis.
Conclusion
The use of an adjustable housing unit which provided the facility to provide alignment and contact security variations demonstrated significant variances and improvements in prosthesis functionality compared to the commonly accepted clinical standard, albeit with investigative limitations. The number of alignment variations was also limited and the unit itself was fixed which restricted the capacity of the system to provide more clinical fitting refinements. Nevertheless, the unit was still able to improve myoelectric prosthesis functionality, which may be recorded when even limited alignment alterations and contact security arrangement are provided.
As the clinical profile of the upper limb prosthetist changes, 17 with fewer specialist upper limb prosthetists available, and the capabilities of prostheses improve, providing adjustable devices may offer improved results to future wearers of myoelectric prostheses.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.