
Abstract
Background:
Conventional prosthetic devices fail to restore the function and characteristic movement quality of the upper limb. The DEKA Arm is a new, advanced prosthesis featuring a compound, powered wrist and multiple grip configurations.
Objectives:
The purpose of this study was to determine if the DEKA Arm improved the movement quality of upper limb prosthesis users compared to conventional prostheses.
Study design:
Case series.
Methods:
Three people with transradial amputation completed tasks of daily life with their conventional prosthesis and with the DEKA Arm. A total of 10 healthy controls completed the same tasks. The trajectory of the wrist joint center was analyzed to determine how different prostheses affected movement duration, speed, smoothness, and curvature compared to patients’ own intact limbs and controls.
Results:
Movement quality decreased with the DEKA Arm for two participants, and increased for the third. Prosthesis users made slower, less smooth, more curved movements with the prosthetic limb compared to the intact limb and controls, particularly when grasping and manipulating objects.
Conclusion:
The effects of one month of training with the DEKA Arm on movement quality varied with participants’ skill and experience with conventional prostheses. Future studies should examine changes in movement quality after long-term use of advanced prostheses.
Clinical relevance
Movement quality with the DEKA Arm may depend on the user’s previous experience with conventional prostheses. Quantitative analyses are needed to assess the efficacy of novel prosthetic devices and to better understand how to train people to use them effectively.
Keywords
Background
Reaching, grasping, and manipulating objects are required for a wide range of essential daily activities. In unimpaired individuals, reaching movements are characterized by several invariant qualities,1,2 including smooth, 3 straight hand trajectories with symmetrical velocity curves. 4 Reaching and grasping are tightly coupled so that the end of reaching is nearly simultaneous with grasping. 5 The characteristic straight trajectories and bell-shaped velocity curves can be replicated well by a model that maximizes movement smoothness. 2
People with upper limb amputation often use prosthetic devices designed to restore some degree of upper limb function. However, prosthesis users still take longer to complete movements using their prosthetic upper limb. 6 Grasping is more prolonged than reaching, resulting in uncoupling of reaching and grasping.6,7 Additionally, reaching movements of prosthesis users do not appear smooth. 7 When using upper limb prostheses, people require more discrete submovements to complete a task.8,9 Although prostheses may not need to completely restore natural upper limb movement patterns to provide functional capacity, 10 there are several reasons why it is important to restore “invariant” movement qualities. A greater number of submovements might make using a prosthetic arm more cognitively 11 and metabolically 12 demanding. This may also explain why many survey respondents report upper limb prosthesis use is too difficult or tiring. 13 Healthy, non-amputees exhibit a strong preference for synchronization of the arms during bilateral tasks. 14 Thus, poor movement quality of the prosthetic limb may also affect the intact limb during bilateral movements. Poor movement quality may contribute to the prolonged movement times and high rate of prosthesis rejection and abandonment among people with upper limb amputations. Quantitative analyses of prosthesis users are needed to better understand the impact of prosthesis use on movement quality. 15
Most currently available upper limb prostheses do not allow users to actively move their wrist. Thus, prosthesis users rely on compensatory movements. 16 Active wrist control may improve hand positioning and help to restore the characteristic movement qualities of the upper limb. 17 The DEKA Gen 3 arm (DEKA Research and Development Corporation) is a novel upper limb prosthesis recently approved by the Food and Drug Administration (FDA). The DEKA Arm provides active wrist flexion coupled with ulnar deviation, active wrist extension coupled with radial deviation, and active wrist rotation. 18 Due to the increased mechanical complexity and unique control approach of the DEKA Arm, significant training is required to become proficient with this device.19,20 Several studies have examined user’s perspectives on the DEKA Arm and compared dexterity and activity performance of the DEKA Arm with conventional prostheses.21–23 However, no study has examined whether and to what extent the DEKA Arm improves movement quality compared to other upper limb prostheses.
The purpose of this study was to determine if the DEKA Arm affected the quality of upper limb movements compared to conventional prostheses. Movement quality was quantified using speed, smoothness, and straightness of the wrist trajectory. If people learn to simultaneously control the additional degrees of freedom of the DEKA Arm to optimally position the hand, their movement quality should increase (e.g. faster, smoother, straighter movements) with the DEKA Arm compared to their conventional prosthesis. Conversely, if they are unable to learn to use the dual control or use a sequential control strategy, we expect their movement quality to decrease. We hypothesized that prosthesis users would make slower, less smooth, more curved movements when using their prosthetic limb compared to their intact limb and healthy control subjects.
Methods
Subjects
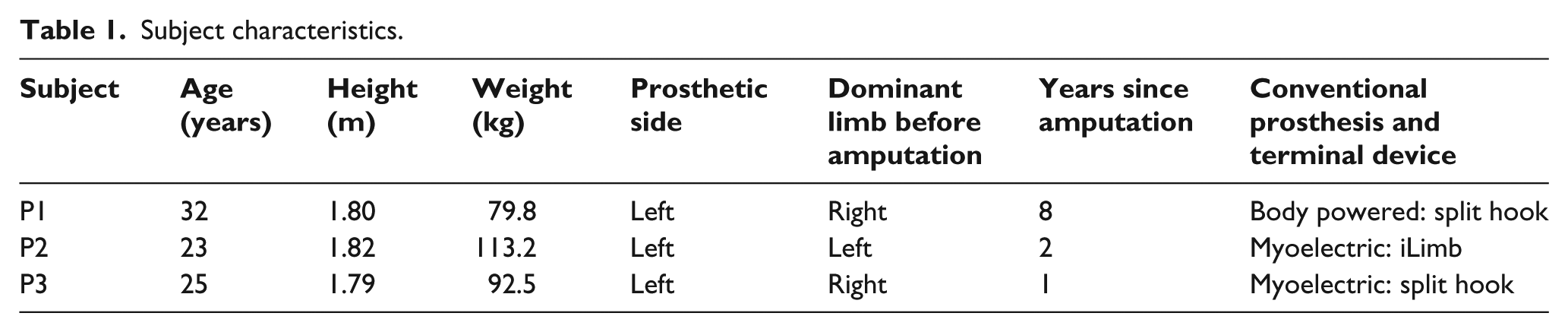
Three young adult males with traumatic, transradial amputation of the left limb (3 male; 26 ± 5.6 years) participated (Table 1). A total of 10 healthy right-handed (e.g. Edinburgh inventory ⩾ 9/10) 24 controls without amputation (6 male; 24.3 ± 5.2 years) also participated. All participants were screened for visual, and neurological impairments and other conditions or medications which could affect upper limb movement. Subjects gave written informed consent before participating in this institutionally approved study.
Subject characteristics.
The DEKA Gen 3 arm
The DEKA Gen 3 arm features six pre-programmed grip configurations and active wrist control. The compound wrist combines wrist flexion with ulnar deviation and wrist extension with radial deviation. 19 All devices used in this study used the same control scheme. Hand open/close was controlled via electrodes on the upper limb (myoelectric). An inertial measurement unit (IMU) on the left foot controlled wrist flexion–ulnar deviation/extension–radial deviation and pronation/supination. Participants could toggle through six grip patterns (fine pinch open, fine pinch closed, chuck grip, lateral pinch, power grip, and tool grip) to obtain their desired grip using an IMU on the right foot. The DEKA Arm was powered by an external rechargeable battery worn on a belt.
Experimental protocol
Prosthesis users completed a baseline data collection session wearing their clinically prescribed prosthesis. Each participant then received training with the DEKA Arm as part of the Veterans Affairs’ (VA) Home Study of an Advanced Upper Limb Prosthetic Device. Participants were provided with a DEKA Gen 3 arm (DEKA Research & Development, Manchester, NH). They were first set up and familiarized with the DEKA Arm controls and features using an interactive virtual reality software program. 25 Each participant then received 10 2-hour training sessions with the study therapist. Training proceeded from reinforcement of prosthetic control patterns of motions to simple grasp and release activities progressing to more complex functional tasks. The training protocol is described in detail elsewhere. 26 Participants were not allowed to use the DEKA arm outside the training sessions. Approximately 1 month later, participants returned to the lab for an identical, follow-up data collection session while wearing the DEKA Arm. Control subjects completed one data collection session.
Tasks
Participants performed a series of activities of daily living: moving a can from a shelf, moving a shoebox from a shelf, lifting a heavy box onto a table, applying deodorant (simulated), perineal care (simulated), and donning zippered pants. 27 For the purposes of this article, we examined three tasks representing specific types of movements. We selected the can (“CAN”), shoebox (“BOX”), and deodorant (“DEO”) tasks to represent unilateral reach and grasp, symmetric bilateral reach and grasp, and bilateral manipulation, respectively. A researcher read a description of each task and demonstrated the task for the subject. The CAN and bilateral BOX tasks required subjects to move objects from a high (1.48 m) shelf to a low (0.94 m) shelf with one (CAN: 15.5-ounce can) or both (BOX: empty shoebox) hands, respectively. Subjects stood facing the shelf with the hands resting at the sides. Subjects then reached up, grasped the object from the top shelf, and moved it to the low shelf. In the DEO task, subjects grasped a stick of deodorant with one hand, removed the cap with the opposite hand, and simulated applying deodorant to the contralateral axilla. Participants performed each task five times at a comfortable pace with the right/intact arm and the left/prosthetic arm.
Data analysis
Due to differences in the terminal devices used by the participants with amputation and between prosthetic and intact hands, the most distal common anatomical reference point was the wrist. Therefore, all analyses focused on the wrist. The three-dimensional position of reflective markers on the radial and ulnar styloids of control subjects or the approximate location of these landmarks on the prosthesis was collected at 120 Hz. Data were collected at two sites using optoelectric motion capture systems (Site 1: Motion Analysis Corp., Santa Rosa, CA; Site 2: Vicon, Oxford, UK). Accuracy of these systems is within 1 mm. Marker position data were filtered using a fourth-order low-pass Butterworth filter with a 6-Hz cut-off frequency. The wrist joint center was calculated as the midpoint between the markers using Visual 3D (C-Motion, Germantown, MA). Wrist velocity was calculated as vector sum of the derivative of the wrist joint center across all three planes of movement.
CAN and BOX trials were separated into phases to capture two separate aspects of movement: transport (reach) and object manipulation (grasp). A movement speed threshold of 5 cm/s was used to identify the beginning and end of each movement phase. For DEO trials, we analyzed uncapping the deodorant. When uncapping deodorant, the right and left wrist joint centers come close together, resulting in a local minimum in the distance between the wrist joint centers. The periods of uncapping the deodorant were identified by analyzing the relative movement speed when the distance between the wrist joint centers was near the minimum. A threshold of 10 cm/s of the relative speed of the wrist joint centers was used to identify the beginning and end of uncapping the deodorant. Start and stop times were also verified visually.
For CAN and BOX, the primary measures were the duration, peak speed, smoothness, and straightness of the reach phase and the duration and smoothness of the grasp phase. For DEO, the dependent measures were duration and smoothness while removing the cap. Non-dimensionalized integrated squared jerk was used to measure reaching smoothness. 28 Grasping smoothness was measured by summing the instances when wrist velocity crossed zero. This analysis provides the number of peaks in the speed profile and approximates the total number of “submovements.”29–31 To quantify reaching straightness, the index of curvature was calculated as the total length of the path traveled by the wrist divided by the length of a straight line between the movement start and end points, 31 where an index of 1 indicates a perfectly straight movement.
The mean and standard deviation of each variable was calculated for five trials of each subject. The magnitude of overall differences between prosthetic and intact limbs and controls was assessed using Cohen’s d as a measure of effect size.
Results
There were few consistent differences between the DEKA Arm and conventional prostheses. Participants 1 and 3 (P1, P3) made slower (Figure 1), less smooth (Figure 2) movements when using the DEKA Arm, while P2 made faster, smoother movements. P1 and P2 made straighter movements with the DEKA Arm (Figure 3), while P3 made more curved movements. P2 made fewer submovements during grasping when using the DEKA Arm (Figure 4), while P1 and P3 made more submovements. All participants exhibited slightly longer movement times (Table 2), with fewer submovements (Figure 5) during the deodorant task when using the DEKA Arm.
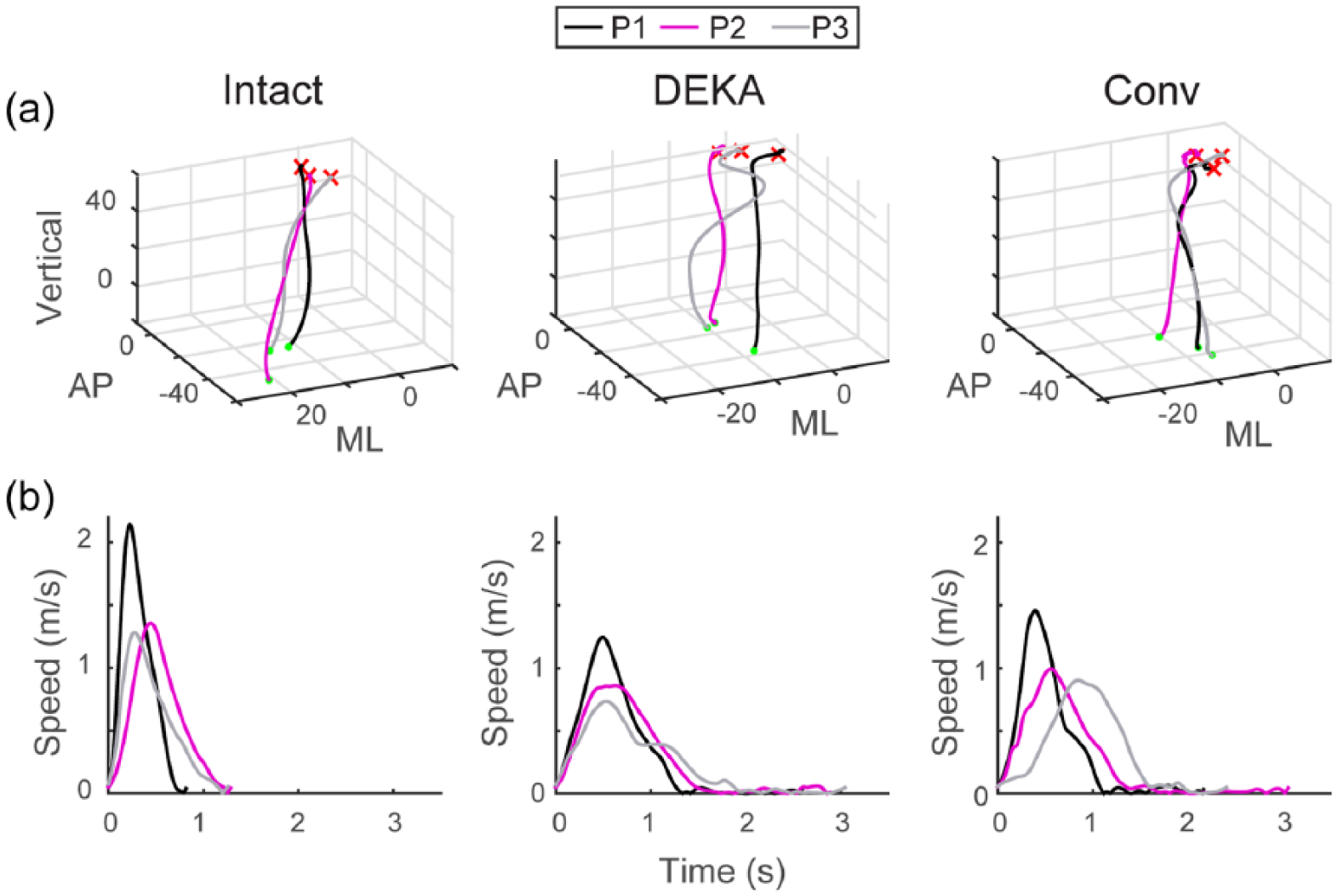
Reach trajectory and speed. Unilateral (CAN) reaches are shown for one representative trial of each participant with the intact arm, DEKA Arm, and conventional prosthesis (Conv): (a) three-dimensional (Anterior–posterior: AP, Mediolateral: ML, Vertical) reach trajectories are shown from the beginning (dot) to end (x) of the reach phase. Note that for intact, right arm reaches, the ML axis has been reversed to match the left arm reaches. (b) Movement speed profiles are shown from the beginning of the reach until the end of the grasp phase. A long tail in the velocity profile represents a prolonged grasping phase. Intact arm reaches have no tails, indicating tight coupling between reaching and grasping.
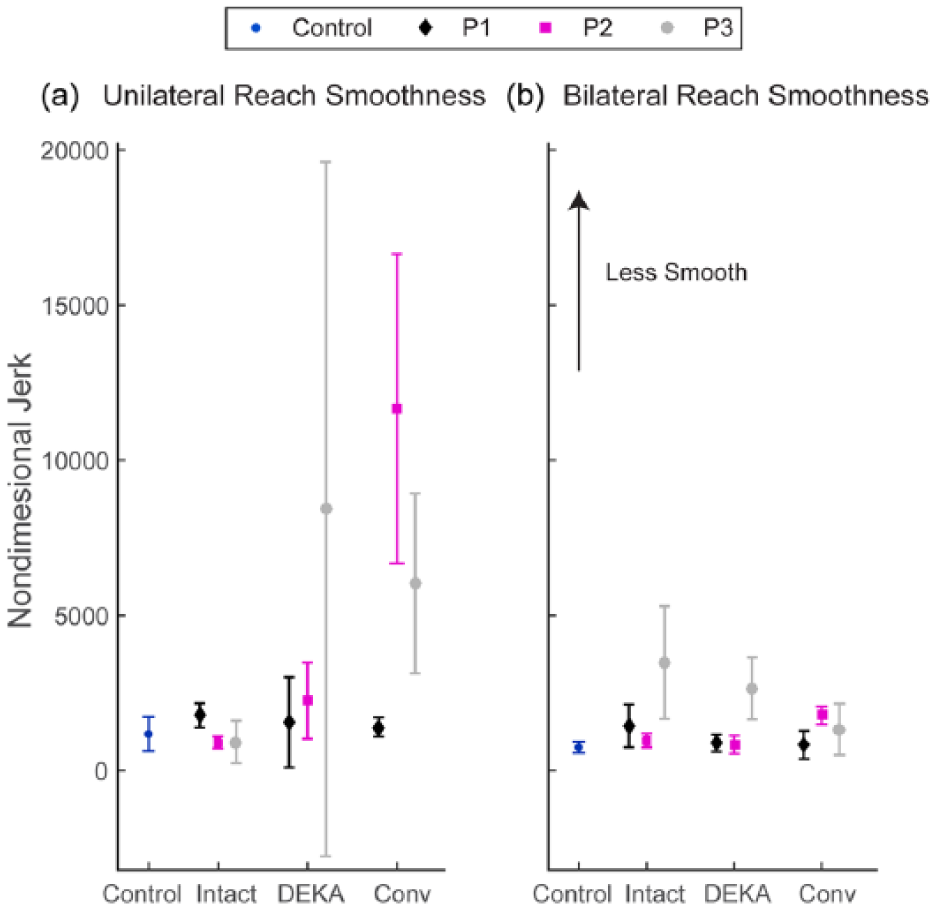
Average non-dimensional jerk during reaches to (a) CAN and (b) BOX for each prosthesis user and for healthy controls. Error bars represent the standard deviation.
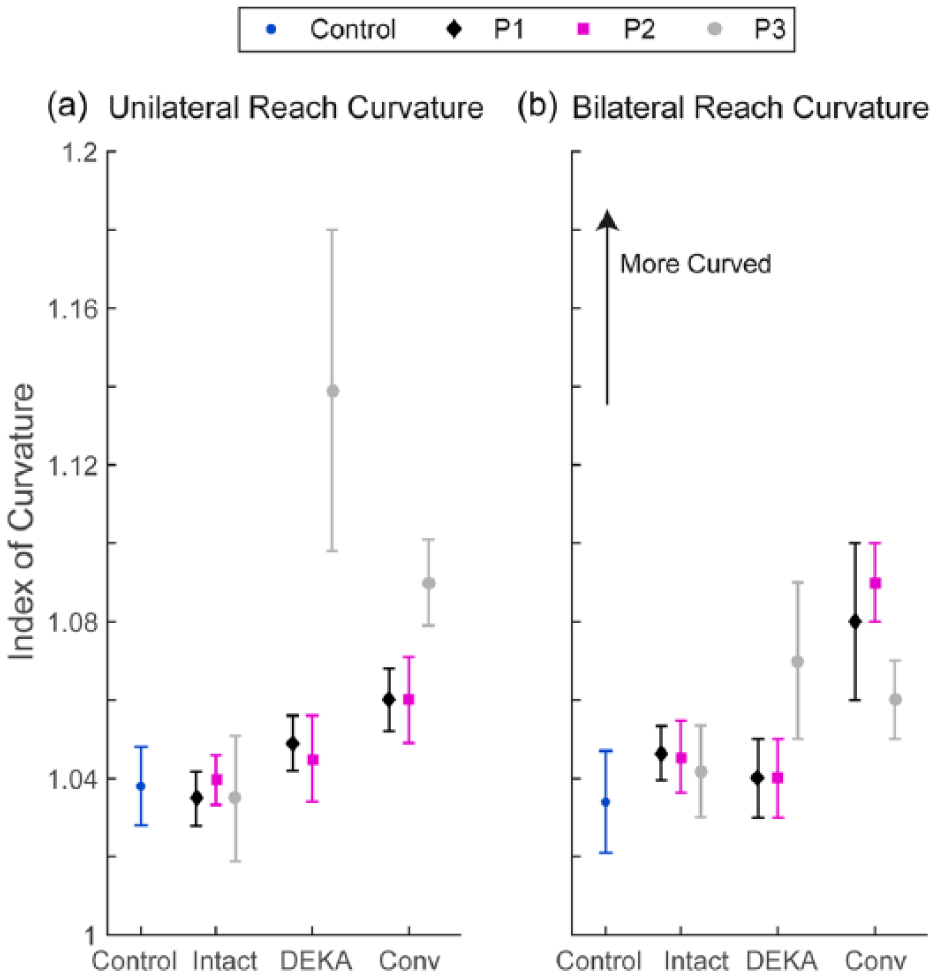
Average index of curvature during reaches to (a) CAN and (b) BOX for each prosthesis user and for healthy controls. Error bars represent the standard deviation.
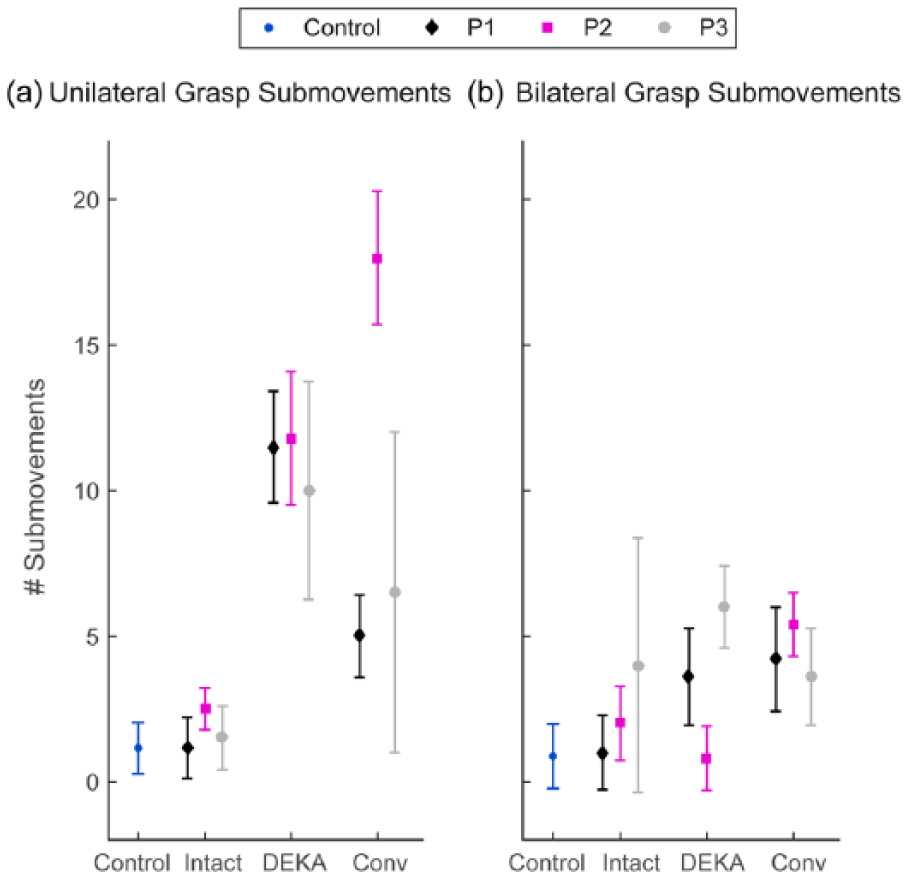
Average number of submovements during the grasping phase of the (a) CAN and (b) BOX tasks for each prosthesis user and for healthy controls. Error bars represent the standard deviation.
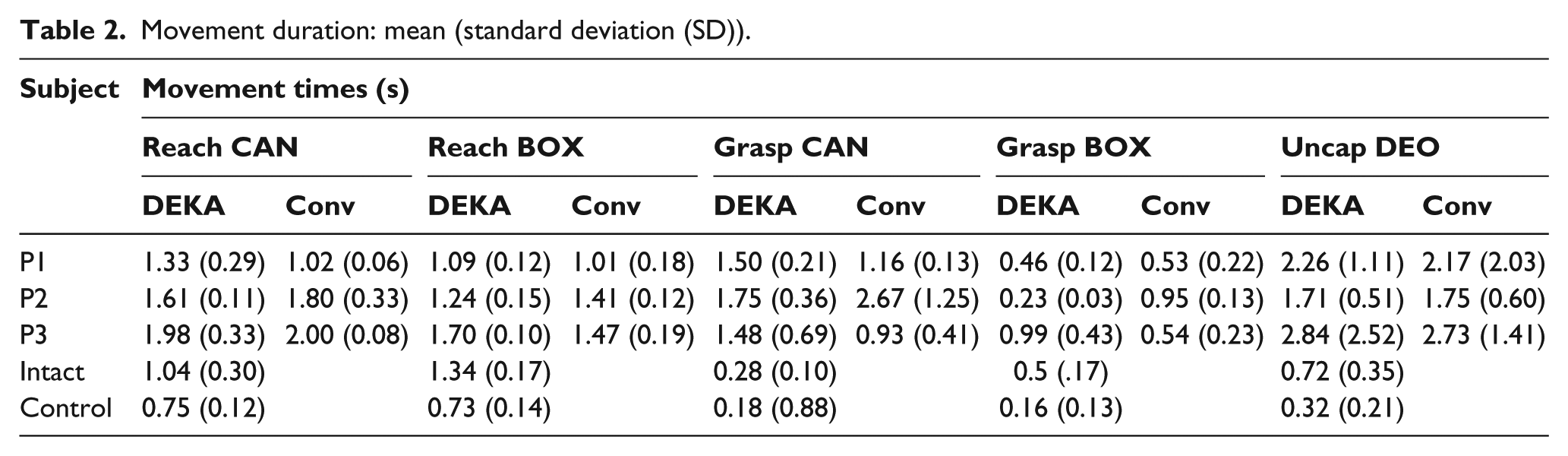
Movement duration: mean (standard deviation (SD)).
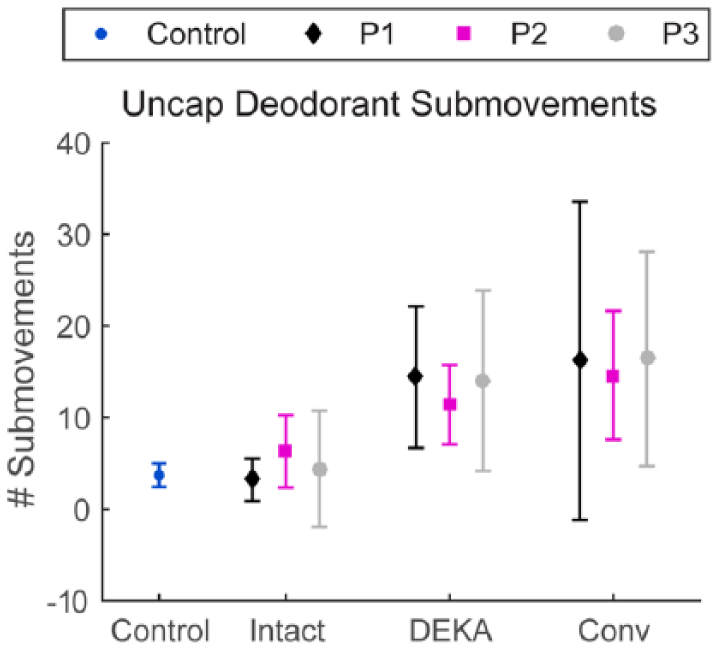
Average number of submovements during the uncapping phase of the DEO task for each prosthesis user and for healthy controls. Error bars represent the standard deviation.
Reaching
Overall, unilateral reaches with the prosthetic limb had longer duration, lower peak speed, decreased smoothness, and greater curvature compared to the intact limb (d > 1.20) and controls (d > 1.40). Intact limb reaches were longer, slower, slightly less smooth and more curved (d > 0.27) than control subjects.
During bilateral reaching, the prosthetic limb did not differ from the intact limb in duration or speed (d < 0.10). Prosthetic limb reaches were more smooth (d = 0.54), but more curved (d = 1.40) than the intact limb. Bilateral reaches were longer, slower, less smooth, and more curved compared to controls (d > 1.20).
Grasping and object manipulation
During the unilateral task, the grasp phase of the prosthetic limb was longer and had more submovements than the intact limb (d > 3.90) and controls (d > 4.20) (Figure 4(a)). During the bilateral task, the grasp phase of the prosthetic limb was longer and had more submovements compared to the intact limb (d > 0.35), and for both limbs the grasp phase was longer and had more submovements than that of controls (d > 1.0) (Figure 4(b)).
For DEO, performance depended upon which arm removed the cap. When the deodorant was uncapped with the intact arm, prosthesis users differed little from controls in task duration or submovements (d < 0.95). When the deodorant was uncapped with the prosthetic limb, participants took longer to remove the cap compared to the intact limb and controls (d > 3.75) (Table 2). Both arms made more submovements compared to uncapping with the intact limb (Prosthetic: d = 4.27; Intact: d = 3.15), and compared to controls (Prosthetic: d = 7.06; Intact: d = 4.06) (Figure 5).
Discussion
The purpose of this study was to determine whether an advanced prosthesis with active compound wrist control would improve the quality of upper limb movement compared to a conventional prosthesis. For participants 1 and 3, movement quality decreased and movement time increased during reach and grasp tasks when using the DEKA Arm. Participant 2 improved movement quality and decreased movement time when using the DEKA Arm. Prosthesis users completed each task slower than controls regardless of the prosthesis used. When using the prosthetic limb, participants’ movements were slower, less smooth, and more curved compared to intact limbs and controls.
The reach phase of the unilateral task took 50% longer with the prosthetic limb compared to controls (Table 2). When manipulating objects with the prosthetic limb, participants used five times more submovements and took five times longer to achieve each task (Figures 4 and 5). During grasping, participants held the arm suspended near the object while they made a series of small submovements to reposition the terminal device in order to complete the grasp. Thus, reaching and grasping were clearly uncoupled when using the prosthetic limb.
During bilateral tasks, participants maintained synchronous bilateral movement by slowing the movement of the intact limb, thus making intact limb movements more similar to prosthetic limbs and less like control subjects. People use the prosthetic limb primarily to stabilize objects and the intact limb to manipulate objects. The results of the DEO task demonstrate that when the roles of the hands are reversed, performance of both hands deteriorates significantly. Due to external constraints of the prosthetic limb and perhaps internal changes in the central nervous system, 32 the movement quality of prosthesis users’ intact limbs is affected during day to day tasks. Bilateral tasks are more problematic for unilateral prosthesis users, because the movement quality of the intact limb is limited by the prosthetic limb.
Most upper limb prostheses do not allow users to move the wrist. In unimpaired subjects, immobilization of the wrist results in compensatory movements 17 and decreased movement smoothness. 33 Similar effects occur in prosthesis users.9,16 Participants did operate the wrist of the DEKA Arm during the performed tasks, and they may have reduced the need for compensatory movements. For participants 1 and 3, who were accustomed to using split hook prostheses, the advanced controls of the DEKA Arm did not enable them to improve movement quality, and even resulted in slower movements. Participant 2 was accustomed to using an iLimb terminal device and was able to improve movement quality with the DEKA Arm. Notably, P2 exhibited the poorest movement quality with the conventional device (Figures 2 and 4).
Previous work suggests that subjects were able to adapt to operating the prosthetic wrist using foot controls. 19 However, it may have taken additional time to move the wrist sequentially in order to orient the prosthetic hand, particularly for P1 and P3 who typically used a split hook device. Due to the lack of tactile and proprioceptive feedback in the prosthetic limb, the orientation of the terminal device must be monitored by visual feedback. 9 Even with advanced wrist and hand devices, it may be difficult to position the hand to grasp objects because of limited sensory feedback in the prosthetic limb. Non-optimal hand postures may cause lower error tolerance during reach to grasp movements, resulting in slower movements with asymmetric velocity profiles.34,35 Furthermore, participants may have experienced some delays as they toggled through the available grasps in order to select the best grip pattern for the activity. The results observed for P2 may indicate that people who use a more advanced terminal device will adapt to the DEKA Arm features more quickly.
It is difficult to make comparisons because our participants used different types of conventional devices and had varying years of prosthetic experience. Although participants were trained in the laboratory with the DEKA Arm, they were still using their conventional prosthesis outside of the limited study activities. Therefore, they may not have been able to alter their established, unconscious, motor movement strategies to take advantage of the features of the DEKA Arm’s powered wrist. Clear differences were observed between participants, but differences between prostheses were less readily noted. This suggests that something about prosthesis use, perhaps more fundamental than the type of prosthesis, differed between participants. For example, P1, who had approximately 8 years of prosthetic experience, performed qualitatively and quantitatively more similar to control subjects than P2 or P3 regardless of the device used. Time since amputation, previous experience, hand dominance, and other factors are difficult to adjust for with this limited population. Some people will likely adapt their movement strategies to maximize the features of a new prosthesis more easily than others, and some will likely become proficient with the DEKA Arm more quickly than others. The individual factors that influence learning to use prostheses need further study.
A total of one month of training may not have been sufficient to improve movement quality with the DEKA Arm. The amount of training and experience needed to use the DEKA Arm’s control schemes are not well understood. 20 It is also possible that movement quality changed in ways that we did not measure. While we did not compare the results of functional tests here, future analyses will examine baseline and DEKA Arm functional test scores in a larger cohort of prosthesis users. Our results demonstrate that our measures of movement quality are closely correlated with movement duration which is a common outcome variable of functional tests. We chose metrics that detect changes in recovering stroke patients by analyzing wrist joint trajectories.30,31 A set of metrics for prosthesis users has not been established. To this end, analysis of the fingertip trajectories may provide additional information about the DEKA Arm and more detailed analysis of grasping in particular. Future studies should also include information that can be obtained from fingertip trajectories such as grip aperture. Quantifiable data regarding movement characteristics and patient outcomes is needed to determine whether novel devices improve quality of upper limb movement. Future research should examine how patients adapt to advanced prostheses with long-term use.
Conclusion
The results of this study demonstrate that prosthetic devices fail to restore natural upper limb movement and function, particularly during object manipulation. We found quantifiable differences between prosthesis users and controls in movement duration, speed, smoothness, and curvature. After 1 month of training with the DEKA Arm, one participant exhibited greater movement quality using the DEKA Arm, while two participants exhibited decreased movement quality. Further changes in movement quality may occur with more time and acclimation to a new device with more movement capabilities.
Footnotes
Acknowledgements
The views expressed herein are those of the authors and do not reflect the official policy or position of Brooke Army Medical Center, the US Army Medical Department, the US Army Office of the Surgeon General, the Department of the Army, Department of Defense, The US Department of Veterans Affairs, or the US Government.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Merit Research Award #A9226-R from the United States (US) Department for Veterans Affairs Rehabilitation Research and Development Service. D. Gates is supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number K12HD073945.