
Abstract
Purpose:
Worldwide advances in microsurgery have made salvaging of amputated hand via replantation and revascularization common procedures. The present study examines the outcome of these procedures in a tertiary hospital in Malaysia.
Methods:
Patients with hand amputation who underwent replantation or revascularization from 2005 to 2012 were identified and reviewed for patient characteristics, amputation characteristics and survival rates. Successfully treated patients were interviewed to assess the functional outcome using Quick Disability of the Arm, Shoulder and Hand (Quick-DASH) questionnaire and Michigan Hand Outcome Questionnaire (MHQ). Statistical analysis was performed to evaluate outcome and elicit predictive factors.
Results:
Fifty-five patients were enrolled: 37 (67.3%) underwent replantation and 18 (32.7%) underwent revascularization. The overall success rate of 78% (n = 43) was within the range of previously reported data (61.6% to 96.0%). Ischaemic time <6 h provided significantly better survival rates (p < 0.05). Functional outcomes were successfully assessed in 34 patients (79%), at a mean follow-up of 40 months (range 11–93 months). The overall Quick-DASH and MHQ scores were 42.82 ± 23.69 and 60.94 ± 12.82, respectively. No previous reports of functional outcome were available for comparison. Both Quick-DASH (p = 0.001) and MHQ scores (p < 0.001) were significantly higher for finger injuries, followed by thumb, wrist and palm injuries.
Conclusion:
Ischaemic time and level of injury are important predictors of success rate of replantation and revascularization of amputated upper limb appendages.
Brief introduction
Among the different types of hand injuries, traumatic amputations are catastrophic events that occur primarily as a result of high-energy trauma in young healthy individuals. For the majority, these injuries are life-changing events that result in multiple surgeries, lengthy hospitalization, absent from work, financial and psychological disturbance. 1 –4 Since the first successful limb replantation was reported by Ronald Malt in 1964, 5 replantation and revascularization of the post-traumatic limb amputation facilitated surgeons to preserve the quality of life of amputees. Advances in microsurgery in recent years have made the salvation of amputated hand via replantation and revascularization as commonly performed procedures in medical centres throughout the world. This expanding knowledge and technology, along with surgeons’ growing experience, has allowed success rates to reach 80–90%. 6 –9
Following the high survival rate of replanted and revascularized post-traumatic hand amputation, recent emphasis has now shifted to functional recovery of the restored part rather than mere survival only. Although the functional outcome of replanted hands will never equal to that of the normal healthy counterpart, the aim of surgery is to produce major functional, cosmetic and psychological improvements in these patients. 9 At present, there is limited literature on the functional outcome of replanted and revascularized amputations of the upper limb. A systematic review of the outcomes of distal digital replantation by Sebastin and Chung 10 concluded that there are no studies with truly sufficient data on functional outcome available at present. Hand-specific outcome instruments such as the Michigan Hand Outcome Questionnaire (MHQ) 11 and the Disability of the Arm, Shoulder and Hand (DASH) 12 questionnaire are patient-reported outcome measures that can be utilized as direct assessment of patients’ overall hand function and symptoms following replantation and revascularizations and provide further insight as to whether the intervention was successful or not. The MHQ measures outcomes in symptoms, function, aesthetics and satisfaction and has also been reported as one of the dominant outcomes questionnaires in hand surgery. 13 As for the outcome of surgery, both the MHQ and DASH have been reported to measure the outcome of surgery, 14 with good reliability and validity in a variety of arm disorders. 12,15 –18 An abbreviated version of the DASH questionnaire, the Quick-DASH, has been tested to have similar precision in upper extremity disorders. 19
In relation to outcomes, the analysis of predictive factors will be able to provide insight into improving existing algorithms for hand amputations. This is because not all persons who have experienced amputation will benefit from, or are deemed suitable candidates for replantation. The decision to replant a severed part is influenced by many factors. Variables such as the type and level of injury have been recognized as factors that may influence the morbidity and functional outcome of replanted parts. 20 However, information relating to outcomes of amputations in association with patient demographics and injury characteristics remains unclear. Indications for replantation and revascularization must follow careful and objective patient selection to optimize functional results and maximize therapeutic benefits.
The only published data available to suggest the level of service provided in Malaysia is from a 6-year report by Razana et al. in 1998, 21 which described an overall success rate of 65.6%, however, there was no data on functional outcomes. With this in mind, the objective of this article is to (1) evaluate the surgical and functional outcomes of replantation and revascularization of post-traumatic amputations conducted over 8 years, and (2) investigate the factors that may influence the final outcomes of both procedures conducted. These findings will enable effective patient selection prior to procedures and promote continuing improvement in clinical services offered by centres in Malaysia.
Materials and methods
In this retrospective cross-sectional study, patients who underwent replantation and revascularization procedures from 1 January 2005, to 31 December 2012, were identified from operation theatre books and listed in a single database management system. Patients were enrolled based on predetermined inclusion and exclusion criteria as outlined in Table 1.
Inclusion and exclusion criteria.

After successfully tracing patient medical records, information regarding patient characteristics (sex, race, age, co-morbidities (diabetes mellitus and hypertension)), concomitant medication (antidiabetic (gliclazide and metformin) and antihypertensives (calcium channel blockers and angiotensin converting enzyme inhibitors), smoking and alcohol consumption), amputation characteristics (level, type and mechanism of injury and time to surgery) and surgical outcomes were extracted for the purpose of analysis. Individuals with successful surgical outcomes were contacted via phone for interview. Using two hand functional scores, Quick-DASH 12 and MHQ, 11 patients’ functional outcome from the date of injury to October 2013 was determined in either English or Malay language, as preferred by the patients. Data collection was concluded by 1 October 2013. Statistical analysis to evaluate surgical outcome and factors that may influence these outcomes was performed using SPSS version 20. Numerical variables were described as mean ± standard deviation (±1 SD) and categorical variables were described as frequency and percentage. χ 2 test was used to determine the association between two categorical variables. Independent sample t test was used to detect the mean difference in two groups, and one-way analysis of variance (ANOVA) was used for mean comparison of more than two groups. All statistical evaluations were set at 5% level of significance. This cross-sectional study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (www.strobe-statement.org).
Informed consent
The study was approved by the institutional medical ethics committee. All patients enrolled provided informed consent to participate in the study.
Results
Study characteristics
A total of 55 patients (Table 2) who received either replantation or revascularization of the upper limb amputation from the study period 1 January 2005, to 31 December 2012, were identified from the operation theatre record books after applying strict inclusion and exclusion criteria. Of the 55 patients, 43 (78%) were successfully operated (i.e. graft survived) and 12 (22%) failed surgery (i.e. graft failed). The successfully operated patients were interviewed over telephone to assess the functional outcome of surgery using MHQ and Quick-DASH questionnaire. A total of 34 (79%) (Table 3) out of 43 patients were successfully interviewed, while the remaining 9 patients were not contactable by telephone. The mean follow-up for functional outcome assessment was 40 months (median 35 months, range 11–93 months). Of the 34 patients interviewed, only 16 patients (47.1%) had adjusted the way they use or did not use their injured hand/part.
Correlation between variable factors and surgical outcome (n = 55a).
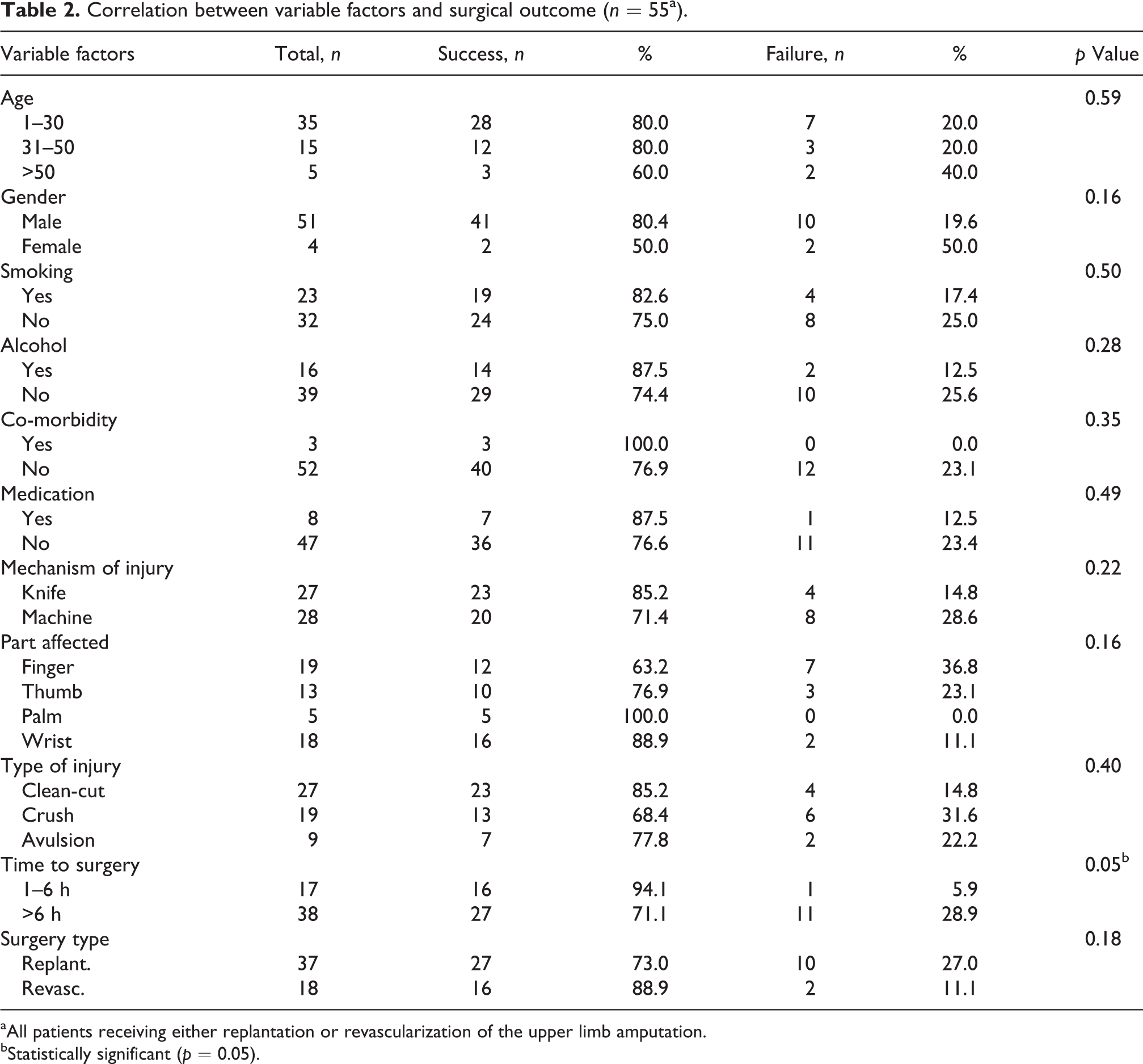
aAll patients receiving either replantation or revascularization of the upper limb amputation.
bStatistically significant (p = 0.05).
Correlation between variable factors and Quick-DASH scores (n = 34a).

Quick-DASH: Quick Disability of the Arm, Shoulder and Hand.
aPatients who were successfully interviewed.
bStatistically significant (p < 0.05).
Patient population characteristics
Majority of patients were aged <30 years (63.6%) and male (92.7%). By ethnicity, more than half were Indians (53.3%), followed by Chinese (20.0%), Malay (16.7%) and other racial groups (10.0%). Majority of patients did not smoke (58.2%) and did not consume alcohol (70.9%). A small number (6%) had co-morbidities such as hypertension and diabetes, and 14.5% were found to be using medication for various health reasons at the time of presentation. With regard to the cause of injury, more than half were due to machine cut (50.9%), while the remaining were due to assault by attackers using sharp objects (49.1%). Clean-cut injury (49.1%) was the most common one, followed by crush injury (34.5%) and avulsion injury (16.4%). The parts of hand mostly affected (i.e. level of injury) were the fingers (34.5%), followed by wrist (32.7%), thumb (23.6%) and palm (9.1%). The majority of injuries were operated after 6 h (69.1%). A total of 37 patients (67.3%) underwent replantation and 18 patients (32.7%) underwent revascularization.
Surgical outcome and relationship to variable factors
On the whole, the procedures were successful in 43 (78.2%) of 55 cases. Only 12 cases were considered failure (21.8%). Replantation was successful in 27 (73%) of 37 patients, while revascularization was successful in 16 (88.9%) of 18 patients. Statistical analysis performed suggested that with regard to the surgical outcome, ischaemic time (i.e. time to surgery) was the only significant factor affecting the success rate, where patients operated within 6 h had significantly better survival rate than those operated after 6 h (94.1% vs. 71.1%; p = 0.05). Success rate analysis according to variable factors is outlined in Table 2.
Functional outcome and relationship to variable factors
Quick-DASH questionnaire
The Quick-DASH assesses the severity of symptoms and difficulty in completing specific tasks and is scaled from 0 to 100, where higher scores indicate more severe disability. 11 The mean Quick-DASH score for all 34 respondents was 42.82 ± 23.69. ANOVA demonstrated no significant difference for most tested variables, except for affected part (i.e. level of injury). For the level of injury, finger amputations (26.33 ± 21.17) and thumb amputations (30.13 ± 19.50) were observed to result in significantly better Quick-DASH scores compared to wrist amputations (56.25 ± 15.48) and palm amputations (60.20 ± 24.02; p = 0.001), reflecting better functional status for patients with distal amputations. Statistical analysis for gender with functional questionnaires was not possible, as of the 34 successfully interviewed patients, only 1 was female. Analysis of Quick-DASH scores in relation to variable factors is outlined in Table 3.
MHQ
The MHQ evaluates six domains that assess patients’ general hand function. Total score ranges from 0 to 100, with higher scores indicating better hand function. 14 Overall, the MHQ score for treated patients was 60.94 ± 12.82. The mean scores for each domain were the overall hand function is 52.79 ± 15.23, activities of daily living 67.03 ± 17.01, pain 64.26 ± 28.31, work performance 60.44 ± 19.24, aesthetics 56.23 ± 10.56 and patient satisfaction 59.00 ± 12.82. ANOVA demonstrated no significant difference for most tested variables, except for affected part (i.e. level of injury) and medication. Those with finger injuries (72.00 ± 9.14) had significantly (p < 0.001) higher MHQ mean score, followed by thumb injuries (67.62 ± 9.26), wrist injuries (52.75 ± 9.24) and lastly palm injuries (50.00 ± 9.46). Patients on no medication also had significantly better MHQ score than those on medication (62.73 ± 12.38 vs. 47.50 ± 7.33; p = 0.02). Analysis of MHQ scores in relation to variable factors is outlined in Table 4.
Correlation between variable factors and MHQ scores (n = 34a).

MHQ: Michigan Hand Outcome Questionnaire.
aPatients who were successfully interviewed.
bStatistically significant (p < 0.05).
Discussion
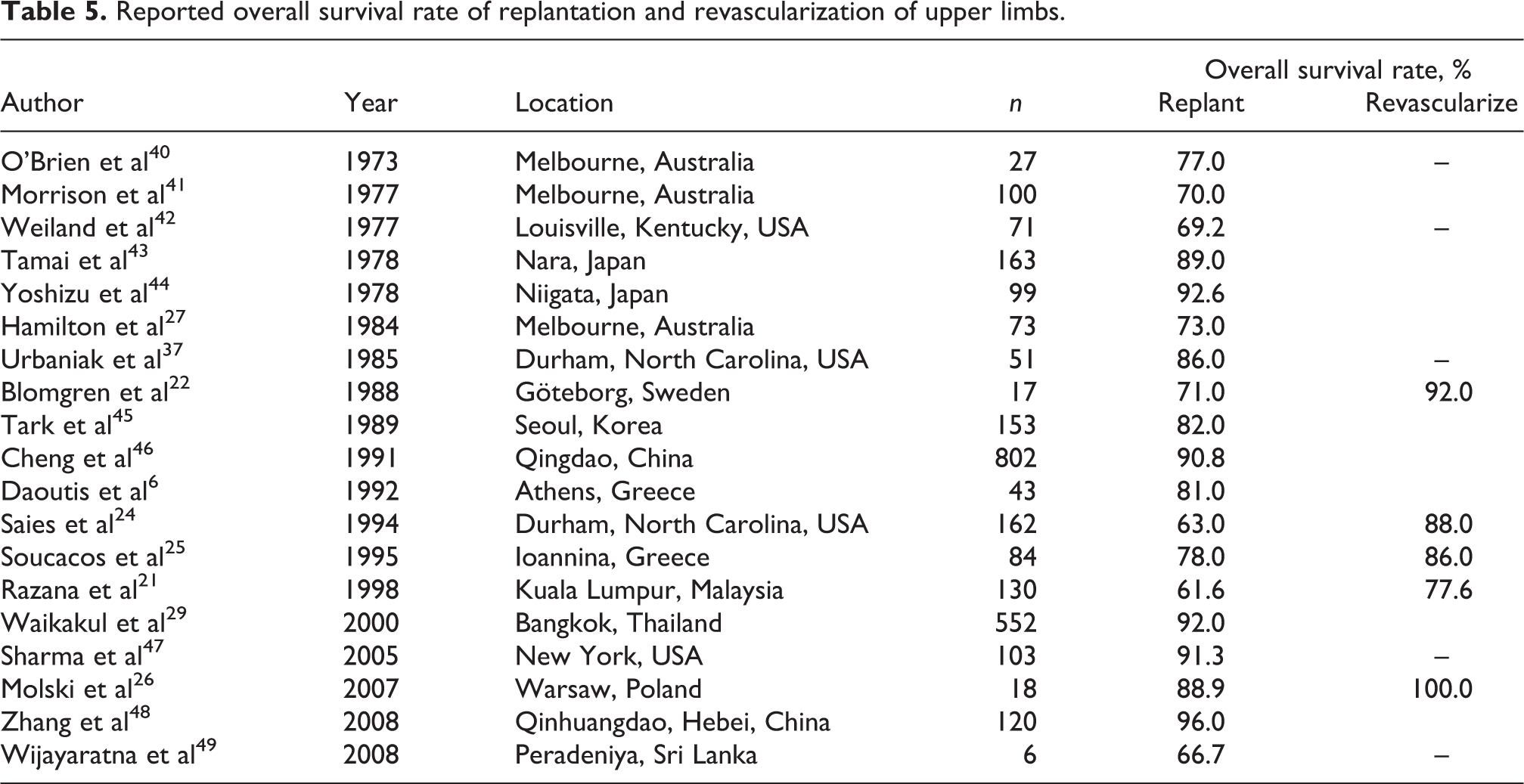
Previously published data by various clinical centres worldwide that provided replantation and revascularization services had reported success rates ranging from 61.6% to 96.0% (Table 5). This retrospective cross-sectional study thus demonstrated that the tertiary hospital studied is up to par with the international standards, achieving an overall survival rate of 78.2%, which is an improvement when compared to the 65.6% success rate reported by Razana et al. 21 in 1998, suggesting a growing experience and improving level of clinical services for managing post-traumatic amputations in Malaysia. The present research however was unable to demonstrate any clear relationship between majority of the tested factors with surgical and functional outcomes. The lack of significant relationship may be due to the low number of subjects enrolled in this study. However, this study noted a significant difference in surgical outcome by ischaemic time and significant functional outcome by different level of injury.
Reported overall survival rate of replantation and revascularization of upper limbs.
The rate of survival of amputated part was observed to be higher following revascularization than after replantation, although this difference did not reach significance. This observation was also reported by many authors. 21 –26 For example, Saies et al. 24 and Hamilton et al. 27 reported a significantly lower rate of acute complications and failure in revascularized patients when compared to replanted patients. In general, viability rates for revascularization are better than those for replantation because adequate venous drainage often remains intact in revascularized amputations. 25
In this study, analysis of patient demographic factors (age, sex, co-morbidities, smoking and alcohol consumption) and factors related to amputation (level and type of injury) showed no significant influence in the overall survival rate. However, significantly better survival rates were observed in patients who were operated within 6 h compared to those who were operated after 6 h. This was also noted by Dec 28 in his meta-analysis involving 1299 patients and 1803 digit replantations, which reported a significant difference between digits salvaged in less than 12 h (i.e. short) and those salvaged after 12 h (i.e. long), with more likelihood of survival in short ischaemia time (odds ratio 2.08). Waikakul et al. 29 studied the results of 1018 digital replantations and argued that while ischaemia remains a key factor in determining the success of replantation, warm ischaemia is tolerated for longer as digits lack muscle, and consequently prolonged ischaemia has been observed to only slightly lessen the survival rate. On the other hand, Chim et al. 30 reported that the survival and ultimate functional recovery were not compromised by prolonged ischaemia. However, it is important to limit ischaemia time to avoid severe post-operative complications such as cardiac or renal failure. 31
Although the present study did not demonstrate this, most authors report that the type of injury is the most important predictive variable. 6,10,28,29,32 Dec 28 reported that clean-cut replanted digits are 5.17 times more likely to be replanted successfully compared to crush and avulsion injuries. Sebastin and Chung 10 observed a similar correlation in their systematic review involving 2273 distal replantations. This could be attributed to the fact that clean-cut injuries involve minimal trauma to surrounding soft tissues, bone, tendons and nerves, whereas crush and avulsion injuries cause widespread damage with large zone of injury. In clean-cut injuries, most vessels could be anastomosed directly without tension and good patency was usually observed, but crushed and avulsed digits have extensive structural damage. 25,29
In addition, smoking and extremes of age are factors reported to significantly affect survival rates. Dec 28 reported that replanted digits of non-smokers are 11.8 times more likely to survive compared to those of smokers, and Waikakul et al. 29 found a statistical correlation between smoking and failure rate. This is due to the vasoconstrictive effect of nicotine, which affects the vascular supply to the replanted digits. As for replantation surgery in children, Saies et al. 24 and Waikakul et al. 29 observed a significantly higher survival rate in children who were aged <13 years, but Beris et al. 32 and Soucacos 33 reported lower survival rate for children. The success rates in children tend to be lower due to the fact that children with amputations had higher technical difficulty due to smaller vessels and greater degree of vasospasm 34 ; however, children benefit from better recuperative ability. Elderly patients on the other hand often have greater number of co-morbidities and higher rate of complications 31 and higher prevalence of arteriosclerosis that can preclude functional patency in small vessels after anastomosis, leading to poorer outcomes. 23,33
The overall Quick-DASH and MHQ scores observed in this study indicated the least satisfactory outcome. Further analysis of MHQ revealed a pain score within the worst half of the scoring spectrum of the pain domain, suggesting that the patients were having significant pain that may have impacted the overall functional outcome. In relation to this, subjective factors such as pain and depression have been reported to have greater influences when disability is measured with respect to hand functions. 35 This finding indicates a need to address the psychosocial issues when managing patients. A comparison with the available literature was difficult due to the scarcity of literature reporting functional outcomes for hand replantation and revascularization. For Quick-DASH score, Haas et al. 36 observed an overall score of 11.3 for 34 replanted thumbs, while no published report currently exists for the comparison of MHQ score. The lack of literature was noted by Sebastin and Chung 10 in their systematic review, which concluded that there are no studies with truly sufficient data about functional outcome. It is important to address this issue in future studies, because although patent vascular anastomoses will often guarantee survivability of replanted parts, functional utility determines patients’ ability to use the replanted part for activities of everyday life and ultimately concludes whether an intervention was successful or not.
The current study found that part of the hand affected (i.e. level of injury) to be the only significant factor affecting the post-operative functional status of patients. A significant difference was seen in Quick-DASH results of different amputated parts, with finger injuries having the best score, followed by thumb injuries, wrist injuries and lastly palm injuries. A similar pattern was also observed with MHQ results, consistent with the findings reported by many authors 23,24,29,33,37,38 who concluded better functional results for amputations distal to the insertion of flexor digitorum superficialis compared to proximal injuries. Also, many authors agree that amputation in ‘no man’s land’ (zone II, Chen’s classification) had the worst functional outcome, due to the complexity of multiple pulleys and complex interweaving of tendons. 24,29,37,39
In this study, age was not a significant predictor, but other authors have reported age to affect the functional outcome after replantation and revascularization. Beris et al. 32 and Soucacos 33 observed that although replanted fingers in children have a lower survival rate than adults, their functional results are uniformly superior. Children have better recuperative ability compared to adults and demonstrate faster nerve recovery. 33 In contrast, poor nerve regeneration, joint stiffness, strength and coordination pose problems for good functional outcome in the elderly. 33
The relatively small sample size is one of the limitations of this study. In future, a more robust study that is prospective in nature and encompassing data from multiple medical centres should be conducted to provide a more meaningful research outcome. Another limitation is that this study involved a heterogeneous group of patient population with varying demographic and injury characteristics and that surgeons of various expertise and background experience conducted the surgery.
Conclusion
In order to achieve maximum survival rate and functional status, there is a need to consider ischaemic time and level of injury in replantation and revascularization of amputated upper limb appendages. This study found that demographic factors (age, sex, co-morbidities, smoking and alcohol consumption) and type of injury did not significantly influence the overall survival rate.
Footnotes
Acknowledgement
The authors would like to thank Gemma Humm for contributing to the project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.