
Abstract
Background and objective:
Lower extremity amputee outcome measures assess basic mobility. The Comprehensive High-Level Activity Mobility Predictor was developed to assess high-level mobility. Validity evidence was collected in military men with traumatic lower extremity amputations. This study examines its validity in a broader population.
Study design:
Cross-sectional.
Methods:
Forty-five lower extremity amputees (Medicare Functional Classification Level K3 or K4) completed the 2-min walk test, Amputee Mobility Predictor with Prosthesis, and Comprehensive High-Level Activity Mobility Predictor.
Results:
The Comprehensive High-Level Activity Mobility Predictor correlated with the Amputee Mobility Predictor with Prosthesis (r = 0.77, p < 0.01) and the 2-min walk test (r = 0.65, p < 0.01). The Comprehensive High-Level Activity Mobility Predictor differentiated between K-levels, age groups, etiology of amputation, and amputation level (p < 0.005). No ceiling effect was observed (range: 2.5–29/40).
Conclusion:
This study provides convergent and discriminative validity evidence for Comprehensive High-Level Activity Mobility Predictor use in a more heterogeneous population than previously published, suggesting that clinicians should feel confident to use it as an outcome measure for individuals with amputations who are capable of more than level-ground walking.
Clinical relevance
Clinically, the Comprehensive High-Level Activity Mobility Predictor has validity evidence for use in a more heterogeneous population than originally demonstrated, including civilians, women, people over age 40 years, and non-traumatic etiologies. The Comprehensive High-Level Activity Mobility Predictor may be more useful than standard outcome measures for high-level mobility.
Background
A goal of rehabilitation for people with lower limb amputation is to optimize mobility. Commonly used physical mobility performance measures include the 10-m walk test, 6-min walk test (6MWT), 2-min walk test (2MWT), timed up and go test, and the L-test.1,2 These walking tests have demonstrated strong evidence for valid scores when applied to the amputee population.1–6 However, these tests have ceiling effects for higher functioning patients as they capture basic ambulatory skills. 7 Likewise, several amputee-specific self-report measures exist, but they are susceptible to recall bias and ceiling effects, which limit their utility for higher functioning amputees.1,8
To address this deficiency, the Comprehensive High-Level Activity Mobility Predictor (CHAMP) was developed and validated by Gailey et al.9,10 They demonstrated excellent interrater reliability (intraclass correlation coefficient (ICC) = 1.0) and test–retest reliability (ICC = 0.97). 9 They demonstrated convergent validity with very strong correlations for the 6MWT and Amputee Mobility Predictor with Prosthesis (AMPPro). 10 The CHAMP’s discriminative validity was demonstrated by its ability to separate participants by level of limb amputation based on the mean total CHAMP score. 10 The CHAMP is a performance-based outcome measure for high-level mobility consisting of four advanced physical tests: the single-limb stance test, the Edgren side step test (sidestepping between two cones placed 4 m apart, counting the number of 1 m intervals crossed in 10 s), T-test (time to complete a course moving forward, sidestepping, and backward in a T-shaped pattern), and Illinois agility test (time to complete a course with a prone to stand transfer, moving forward, and weaving in between cones). These tests assess balance, coordination, speed, power, and multidirectional agility. They are described in detail in the appendix of Gailey et al.’s development of the CHAMP. 9
In its development, the CHAMP was only administered to male military service-members less than 40 years of age with traumatic amputations. 9 However, many individuals with amputations are capable of mobility activities beyond level-ground walking. Therefore, having an outcome measure, such as the CHAMP, to assess these higher level mobility skills is important. Prior to using the CHAMP as an outcome measure in a more general population of individuals with amputations, additional evidence for its validity should be sought by analyzing its performance in a broader group of individuals.
In addition to being able to discriminate by level of amputation, it would be useful to know whether the CHAMP can differentiate between etiology of amputation, gender, age, and Medicare Functional Classification Level (MFCL) K-level.
The MFCL K-level system is used in amputation rehabilitation as a method of stratifying patients according to potential or current post-rehabilitation activity level and functioning. The K-level is assigned by the treating physician or prosthetist. People with lower limb amputation who are at higher level abilities are grouped into the K3 and K4 categories (K3: community ambulator able to traverse most environmental barriers; K4: exceeds basic ambulatory skills and can perform higher level activities).11,12
The objective of this study was to assess the convergent and discriminative validity of the CHAMP in a population that included women, individuals over 40 years of age, and those with amputation etiologies other than trauma. This will enable us to add to the evidence of validity demonstrated by Gailey et al.9,10 We hypothesize that the CHAMP will demonstrate evidence for convergent and discriminative validity in this broader population. We hypothesize that similar to Gailey et al.’s previous work, the CHAMP will demonstrate strong correlations with walking tests and be able to discriminate between limb amputation levels. We also hypothesize that the CHAMP will demonstrate the ability to discriminate between K-level groups, etiology, gender, and age.
Methods
This study was approved by The Ottawa Health Science Network research ethics board (approval number 20150711-01H).
Setting and participants
Participants were recruited from the outpatient amputation clinic at The Ottawa Hospital Rehabilitation Centre based on a chart review. To be included in the study, participants had to meet all of the following criteria: (a) 18–60 years old, (b) unilateral lower limb amputation, (c) use of a properly fitting prosthesis, and (d) MFCL K3 or K4 as determined by their treating Physiatrist based on the most recent clinic visit record. The goal of the CHAMP is to better assess higher level physical performance (i.e. beyond level-ground walking). This is consistent with K3- and K4-level performance. Therefore, only K3- and K4-level participants were included in our study.
Amputation levels included ankle disarticulation, transtibial, Van Nes rotationplasty, knee disarticulation, and transfemoral. Participants required sufficient literacy in either English or French to complete questionnaires. Participants who were unable to follow commands or provide informed consent due to cognitive impairment, as well as those unable to complete mobility tests due to a medical condition, were excluded.
Patients meeting inclusion criteria were mailed a letter informing them of the study. Two weeks later, they were contacted via telephone by the principal investigator to ensure that they met the inclusion/exclusion criteria and to determine their interest in participating. Willing participants were enrolled.
Protocol
Testing was carried out from January to June 2016. Recruiting and testing personnel (authors A.A. and Z.L.) were blinded to K-level. Informed written consent was obtained prior to testing. On the day of testing, age, sex, etiology of amputation, and amputation level were recorded.
Gailey et al. had participants first demonstrate a minimum level of functional ability prior to completing the CHAMP. His group defined this as an AMPPro score of ⩾37 and/or 6MWT of ⩾250 m. 9 The 2MWT is a strong predictor of distances ambulated in the 6MWT among people with lower limb amputation. 6 Therefore, we used the 2MWT and calculated an equivalent minimum standard of 97 meters using the predictive equation published by Reid et al., where 6MWT(meters) = 3.14(2MWT(meters)] – 54.5. 6 The AMPPro was administered according to the protocol outlined by Gailey et al. and the 2MWT was administered according to the protocol by Brooks et al.13,14
CHAMP testing was carried out according to the appendix protocol outlined by Gailey et al. 9 This sequentially consisted of one trial of the single-limb stance test, the Edgren side step test, t-test, and the Illinois agility test. Results of the four individual tests were converted into a score from 0 to 10 based on the pre-determined algorithm. 9 The total combined CHAMP score was obtained by adding the four results to produce a maximum score of 40, with higher scores indicating better performance.
A seated rest in between tests was given, during which the participants completed three previously validated self-report outcome measures: Locomotor Capabilities Index 5 (LCI-5), Houghton Scale, and Activities-Specific Balance Confidence (ABC) scale.8,15–20 The total time taken to complete the CHAMP was recorded. Gailey et al. established evidence for reliability. 9 Therefore, reliability was not assessed in this study.
Statistical analysis
Data were analyzed using SPSS Statistics for Windows, version 24. Descriptive statistics were calculated for each outcome measure. To assess for evidence of convergent validity for the CHAMP, its results were correlated with other outcome measures using Pearson’s correlation coefficients (r). Pearson’s level of correlation was interpreted as follows: very strong (r ⩾ 0.8), moderately strong (r = 0.79–0.6), fair (r = 0.59–0.3), and poor (r ⩽ 0.29). 21
Discriminative validity evidence was obtained by calculating the mean scores for the 2MWT, AMPPro, and CHAMP for each of the following groups: gender, amputation level, age, etiology, and K-level. For analysis, amputation level was split into two groups: “below knee”—those who used a prosthetic foot/ankle (ankle disarticulation, transtibial, and Van Nes rotationplasty) and “above knee”—those who used both a prosthetic foot/ankle and prosthetic knee (knee disarticulation and transfemoral). Age was categorized into two groups: 18–39 and 40–60 years. This split was chosen to represent an age group consistent with that previously used in Gailey’s study, in addition to an older group.9,10 Finally, etiology was grouped as follows: amputation in the context of chronic disease (peripheral vascular disease, diabetes) and amputation not associated with chronic disease (cancer, congenital, acute non-diabetic infection, and trauma). Independent t-tests were used to assess for differences between measures for these groups. For all statistical measures, a p level of <0.05 was considered significant.
Results
Based on chart review, 81 participants met inclusion criteria. Forty-five people enrolled. Reasons for not enrolling included the inability to contact the potential participant by telephone and the inability to schedule a time for testing due to other commitments of the potential participant. All participants were able to complete the entire protocol with no adverse events. No one used a gait aid. Table 1 describes the study population.
Study population and demographics.
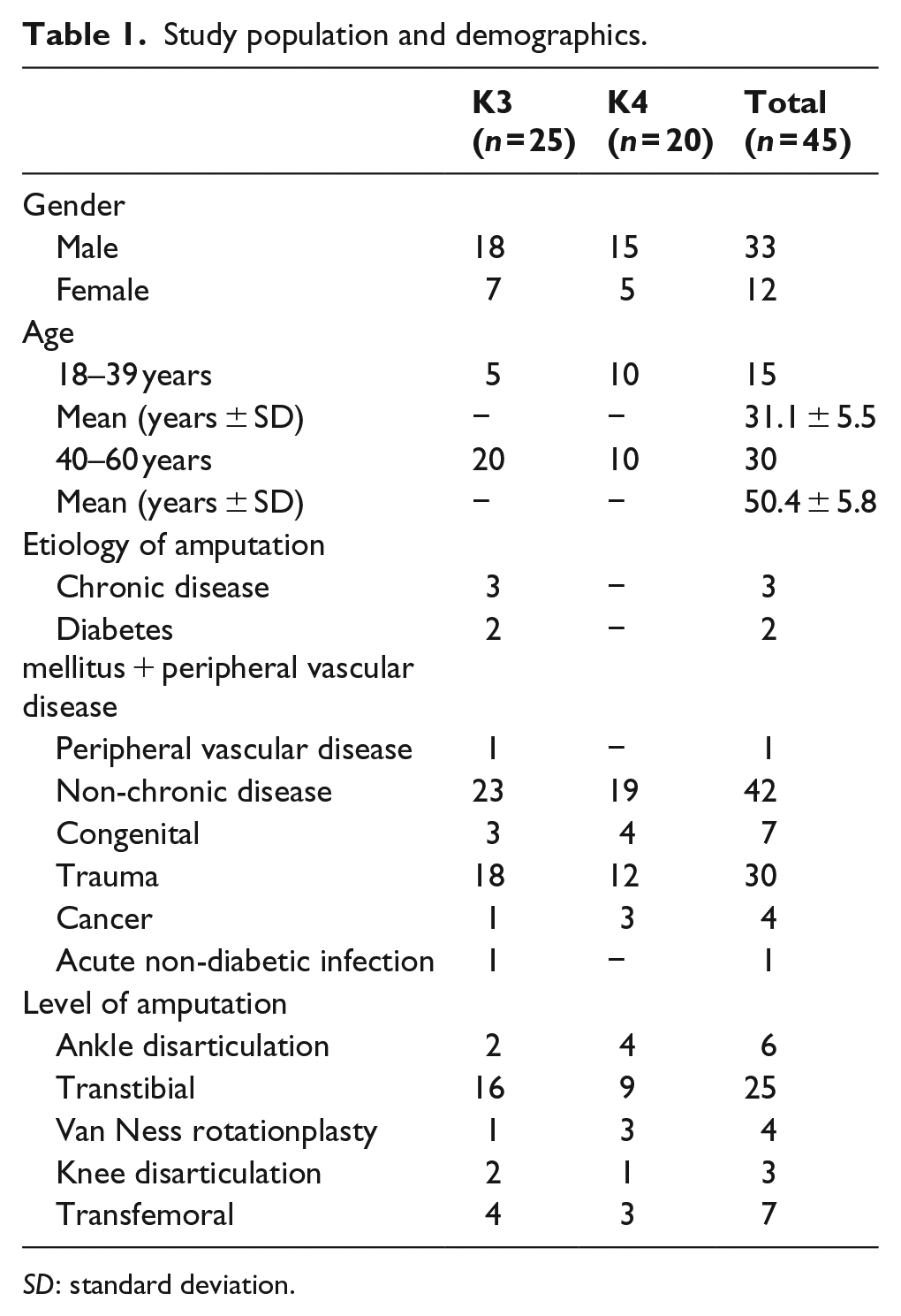
SD: standard deviation.
All participants scored >37 (range: 38–47/47) on the AMPPro and walked >97 m (range: 103–207 m) on the 2MWT to qualify to complete the CHAMP. All participants were able to complete the CHAMP protocol. Table 2 displays the descriptive statistics for each outcome measure.
Descriptive statistics for outcome measures.
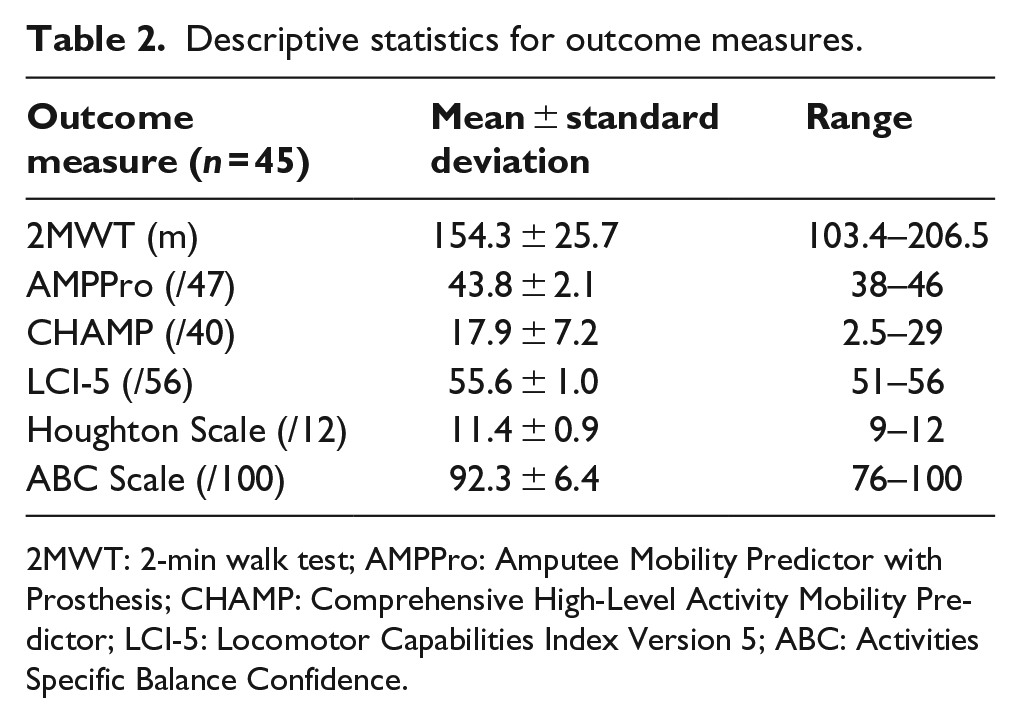
2MWT: 2-min walk test; AMPPro: Amputee Mobility Predictor with Prosthesis; CHAMP: Comprehensive High-Level Activity Mobility Predictor; LCI-5: Locomotor Capabilities Index Version 5; ABC: Activities Specific Balance Confidence.
Convergent validity
The CHAMP has a moderately strong correlation with both the AMPPro (r = 0.77, p < 0.01) and the 2MWT (r = 0.65, p < 0.01), demonstrating convergent validity. It was not correlated with the LCI-5 (r = –0.03, p = 0.85), Houghton scale (r = –0.09, p = 0.56), or ABC scale (r = 0.02, p = 0.90). This was also true for both the 2MWT and the AMPPro. The 2MWT and AMPPro had a fair correlation (r = 0.48, p < 0.01). The Houghton scale had fair correlations with both the LCI-5 (r = 0.42, p < 0.01) and the ABC scale (r = 0.33, p < 0.01). The LCI-5 and ABC scale were not correlated (r = 0.19, p = 0.22).
Discriminative validity
Table 3 details the CHAMP scores among the various subgroups. All groups have statistically significant differences (p < 0.05) with the exception of gender. The effect size for gender was 0.65, indicating a medium to large difference.
CHAMP score subgroups comparisons.
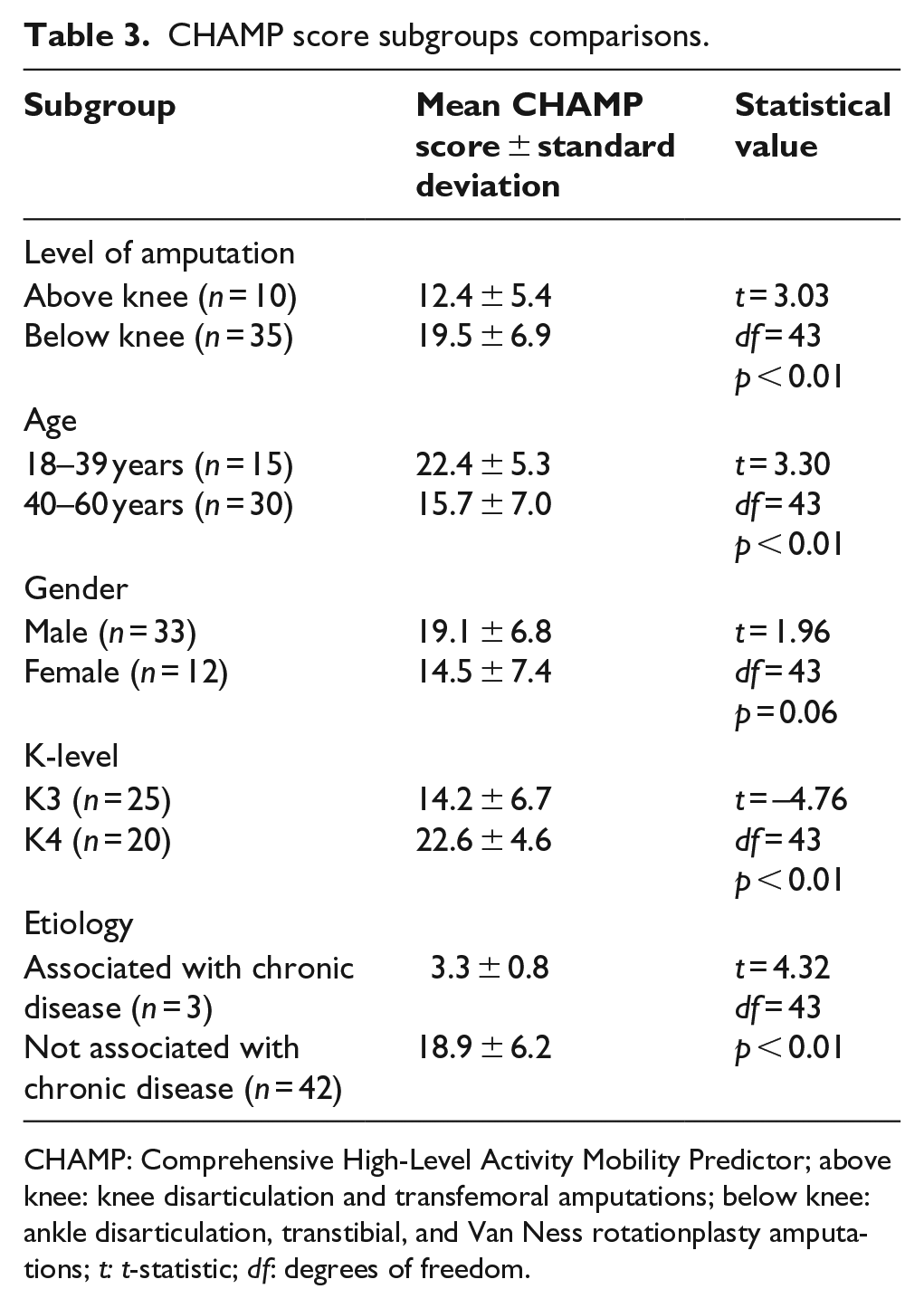
CHAMP: Comprehensive High-Level Activity Mobility Predictor; above knee: knee disarticulation and transfemoral amputations; below knee: ankle disarticulation, transtibial, and Van Nes rotationplasty amputations; t: t-statistic; df: degrees of freedom.
There were statistically significant differences (p < 0.05) on the 2MWT for gender, K-level, and etiology. There were statistically significant differences (p < 0.05) on the AMPPro for amputation level, K-level, and etiology. The Houghton scale, LCI-5, and ABC scale did not show any statistically significant differences between any subgroups.
CHAMP testing time
The average time to complete the CHAMP, including rests, was 9.3 ± 5.9 min.
Discussion
The objective of the study was to add to the literature demonstrating evidence of validity for use of the CHAMP as a physical mobility outcome measure for people with lower limb amputation. By recruiting a more heterogeneous participant group (i.e. including women, people over 40 years old, and those with amputation etiologies other than trauma), this study adds to the previously published literature supporting the use of the CHAMP as a valid outcome measure.9,10 CHAMP scores were strongly correlated with the 2MWT and AMPPro, demonstrating convergent validity in a more heterogeneous study population. The CHAMP also demonstrated discriminative validity with its ability to separate participants by age, amputation level, K-level, and etiology. Previous work had only demonstrated that the CHAMP could discriminate by limb amputation level. 10 Although the CHAMP did not statistically significantly differentiate between men and women, the effect size of 0.65 indicates a medium to large difference suggesting that the study was likely underpowered to detect this difference.
Interestingly, the self-report measures did not correlate with the CHAMP, 2MWT, or AMPPro. The self-report measures also did not detect any differences between the various subgroups (i.e. amputation level, age). We hypothesize that this was because of our higher performing study population (i.e. only K3 and K4 levels). This is consistent with a recent study that noted functional tests such as the 6MWT and AMPPro were able to distinguish between K3 and K4 groups but self-report measures, including the LCI-5, did not. 22 The Houghton, LCI-5, and ABC scales are known to be of lesser value for higher performing individuals because of significant ceiling effects.1,8 In a conservative approach, floor or ceiling effects are present when 15% or more of a group’s scores are at either extreme. 23 This study demonstrated ceiling effects with extremely high mean scores for all three measures, and score ranges clustered at the top end of each scale. With the ceiling effects, these outcome measures are not sensitive enough to differentiate among our subgroups.
It is interesting to consider whether the CHAMP provides more information than the other previously validated walking measures in terms of its ability to discriminate between various groups of individuals with amputations. Some evidence of this was seen in the ability of each of the three measures to discriminate between our five subgroups (age, level of amputation, K-level, etiology, and gender). The CHAMP was able to differentiate between four of the groups, whereas the AMPPro and 2MWT only differentiated between three of them. In particular, only the CHAMP could differentiate between age groups. Given the additional aspects of mobility that the CHAMP assesses, it is reasonable to hypothesize that it might be better at differentiating performance levels for individuals with lower limb amputation who have the capacity for higher level mobility. Future study is recommended to explore this.
This study has limitations. The small sample size meant that we had to group patients with different amputation levels into “below knee” and “above knee” categories. A larger sample size could determine whether or not the CHAMP is sensitive enough to find differences between individual amputation levels (e.g. ankle disarticulation vs transtibial). As well, there were only a very small number of individuals who had an amputation performed due to chronic disease who met the study’s inclusion criteria, so the conclusion that the CHAMP is capable of discriminating by etiology should be interpreted cautiously. However, realistically, many individuals with amputations secondary to chronic disease do not achieve high levels of ambulatory function and hence would not meet the performance standards necessary to use the CHAMP (i.e. minimum AMPPro and 6MWT).6,13 These individuals are likely relatively well served by our current measures of mobility. Finally, reliability of the CHAMP was not assessed in this study. Given that our study population was more extensive than Gailey et al.’s study, a wider range of physical abilities is expected and, therefore, reliability should be tested in future studies.
Conclusion
This study adds to the validity evidence for the use of the CHAMP. Everyone enrolled in the study was able to complete the CHAMP, which suggests that it is an appropriate outcome measure for people with lower limb amputation who are classified as K-level 3 or 4. No participant achieved a maximum CHAMP score in this study or that of Gailey et al., suggesting that the CHAMP has the potential to measure very high mobility performance.9,10 Future studies should include a larger sample size and track CHAMP scores over time for individuals going through rehabilitation to determine its responsiveness to change, which will add to the growing body of validity evidence for the CHAMP.
Footnotes
Acknowledgements
The authors wish to thank The Rehabilitation Centre physiotherapy department, the study participants, and Dr. Timothy Wood.
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Physicians’ Services Incorporated Foundation (grant number R15-280).