
Abstract
Background:
The relationship between gait speed and prosthetic potential (K-level classifications) and function has not been explored among people transitioning from hospital rehabilitation to the community.
Objectives:
To examine gait speed at discharge from inpatient rehabilitation among people prescribed a prosthetic leg after unilateral lower limb amputation, and associations between gait speed, prosthetic potential and functional ability.
Study design:
Cohort.
Methods:
Gait speed (10-m walk test), K-level (Amputee Mobility Predictor) and Functional Independence Measure motor were compared for 110 people (mean (standard deviation) age: 63 (13) years, 77% male, 71% transtibial amputation, 70% dysvascular causes).
Results:
Median (interquartile range) gait speed and Functional Independence Measure motor were 0.52 (0.37–0.67) m/s and 84 (81, 85), respectively. Median (IQR) gait speed scores for each K-level were as follows: K1 = 0.17 (0.15–0.19) m/s, K2 = 0.38 (0.25–0.54) m/s, K3 = 0.63 (0.50–0.71) m/s and K4 = 1.06 (0.95–1.18) m/s. Median (IQR) FIM-Motor scores for each K-level were as follows: K1 = 82 (69–84), K2 = 83 (79–84), K3 = 85 (83–87) and K4 = 87 (86–89). Faster gait speed was associated with higher K-level, higher FIM-Motor, being younger, male and having transtibial amputation with nonvascular aetiology.
Conclusion:
Gait speed was faster among each higher K-level classification. However, gait speeds observed across all K-levels were slower than healthy populations, consistent with values indicating high risk of morbidity and mortality.
Clinical relevance
Factors associated with faster gait speed are useful for clinical teams considering walking potential of people with lower limb prostheses and those seeking to refine prosthetic rehabilitation programmes.
Background
The loss of a lower limb has been shown to negatively impact a person’s quality of life 1 and is associated with a deterioration in function and residential status. 2 In addition to the personal consequences of lower limb amputation, a significant social and financial burden is placed on the person, community and healthcare system. 3 It is anticipated that this burden will continue to rise due to increasing population prevalence of risk factors for amputation such as diabetes 4 and ageing populations. 5
Prosthetic walking potential of people with lower limb amputation was originally described by the Medicare Functional Classification Level. 6 This classification system consists of five levels, referred to as ‘K-levels’. 7 K-levels range from 0 to 4, where K0 refers to a person who does not have the ability or potential to use a prosthesis for transfers or walking and K4 refers to a person with the ability or potential to exceed basic ambulation skills, exhibiting high impact, stress or energy levels. Since its development, the K-level system has directed distribution of government funding to people with lower limb amputation in countries such as the United States and Australia.8,9 K-levels have also been adopted world-wide by prosthetic companies to guide the prescription and use of prosthetic components.
Determining a person’s K-level remained a subjective process until the Amputee Mobility Predictor (AMPPRO) assessment tool was developed. 7 The AMPPRO assessment has evidence supporting its validity and reliability in providing an objective method to determine a person’s K-level and requires approximately 10–15 min to complete. 7 It is expected that an individual assigned a higher K-level would be able to walk faster, consistent with requirements to complete functional tasks that are mobility dependent, while a lower K-level is expected to be associated with slower walking. Consequently, a timed walking test (such as the timed 10-m walk test) may be a time-efficient, practical alternative to the AMPPRO as an indicator of a person’s K-level. Timed walking tests are used frequently in clinical settings to assess the gait of people with lower limb amputations; however, the relationship between K-level and gait speed has not yet been examined.
Gait speed derived from walking tests is an indicator of walking ability 10 that has evidence supporting its reliability and validity. 11 Gait speed is also a known predictor of community mobility in other populations including stroke, 12 Parkinson’s disease 13 and frail older adults. 14 Gait speed appears to be a suitable measure for people who walk with lower limb prostheses and has been used in the amputation population to explore energy cost 15 and prosthetic weight. 16 However, its relationship with functional status in the amputation population has not yet been explored. It would be useful to examine whether walking speed could be an indicator of potential for community walking with a prosthesis (K2/3), as compared to household prosthetic users (K1).
This study focused on gait speed and K-levels at an important point in the rehabilitation process where people were coming to the completion of their inpatient hospital rehabilitation and were about to transition home to the community with a lower limb prosthesis. This is a pivotal time for patients as they depart from access to full-time care and potential for high levels of support with their daily activities in the hospital as they transition to continue their recovery in their own home and surrounding community. However, prior to this study it was unknown whether people with lower limb amputation, who were being discharged from hospital rehabilitation, walked at speeds that have been associated with successful functional ambulation in the community among the other aforementioned clinical populations.13,14 The aim of this study was to assess gait speed at discharge from hospital rehabilitation across K-levels and whether this gait speed would likely be sufficient for patients to walk and function in the community at the point of transitioning from the hospital to the community.
Methods
Design
This is a cohort investigation.
Setting and participants
The setting was an inpatient rehabilitation unit at an Australian tertiary hospital. The study included consecutive patients who met the study eligibility criteria. Patients were eligible if they were admitted to the hospital rehabilitation unit after a new unilateral major lower limb amputation (transtibial or transfemoral amputation, knee or hip disarticulation) and prescribed an interim lower limb prosthesis for gait which they were utilising to walk during a clinical assessment immediately prior to their discharge from inpatient hospital rehabilitation. Patients were excluded if amputation was not their reason for admission, or if they were not able to walk with a lower limb prosthesis at their discharge assessment. Local hospital and university institutional human research ethics committees approved this study.
Procedures
The Geriatric and Rehabilitation Unit at the participating hospital has a custom-designed database to prospectively record demographic and clinical information during patient admissions. This information is recorded at admission to this unit by clinicians in the treating multidisciplinary team. Admission data include aetiology, cognition (measured using the Modified Mini-Mental State Examination (MMSE)), 17 gender, age, amputation level, comorbidities and whether the patient used an indoor mobility aid prior to this admission. Prior to discharge from this unit, information from routine discharge assessments is also recorded by clinicians including walking outcome measures (gait speed and AMPPRO/K-level scores) and Functional Independence Measure (FIM) scores. Records in the database were examined by the lead investigator (HB) to confirm participant eligibility and any missing information (e.g. information about pre-amputation indoor mobility aid use) was retrieved from written medical records. Transtibial prosthetic design was most commonly a thermoplastic Patella Tendon Bearing socket, pelite liner, suprapatellar cuff or suspension sleeve and Solid Ankle Cushioned Heel (SACH) or single-axis foot. Transfemoral prosthetic design was most commonly a thermoplastic quadrilateral socket, rigid pelvic belt or suction suspension, 3R49 Safety Knee or 3R40 Lock knee with a SACH or single-axis foot.
Outcomes
The primary outcome measure was gait speed, derived from a 10-m walk test 18 where the patient was permitted to use his or her usual walking aid and instructed to walk at a safe and comfortable pace (i.e. a self-selected velocity). This test was conducted by a physiotherapist in accordance with a standardised protocol 18 where participants walked a total of 12 m indoors on a flat surface with the middle 10 m timed to allow for acceleration and deceleration. Two secondary measures were recorded: (1) K-level (0–4), determined by the AMPPRO conducted by a physiotherapist, 7 and (2) functional ability according to the FIM 19 motor subscore (FIM-Motor) completed with input from members of the multidisciplinary team. Each of the 13 FIM-Motor items reports the level of independence achieved with specific functional tasks (including personal care, walking and bed mobility tasks). Functional independence for each task is scored on a seven-point scale from total dependence (score of 1) to complete independence (score of 7) such that the FIM-Motor yields a subscore out of 91.
Analysis
Descriptive statistics were used to describe the characteristics of the sample at admission and discharge from inpatient hospital rehabilitation. Median and interquartile ranges were used to describe gait speed and FIM-Motor for each of the ordinal K-levels (K1–4), which were not normally distributed. Spearman’s correlation coefficient was used as an indicator of the strength of the association between K-level, gait speed and FIM-Motor. To examine which characteristics (potential explanatory variables) were associated with faster gait speed (outcome variable), generalised linear models were prepared. Explanatory variables included in the model were K-level, aetiology, MMSE, discharge FIM-Motor, gender, age, amputation level, comorbidities that were present in >15% of the sample and whether the person used an indoor mobility aid prior to this amputation. Huber–White sandwich variance estimates were used to account for potential heteroscedasticity. 20 The alpha value was set at 0.05 and all analyses were performed using Stata/MP v13 (StataCorp LP, College Station, TX, USA).
Results
A total of 335 individuals were admitted to the participating hospital rehabilitation unit with a new lower limb amputation and screened for eligibility. A total of 110 patients underwent a unilateral amputation resulting in a prosthetic leg prescription and fulfilled the study criteria. Of those who were not included in this study, 76 were prescribed a prosthesis but 10 were bilateral amputees, 63 were not walking with their prosthesis at discharge from inpatient rehabilitation and 3 had missing data which means that it was not possible to determine whether they were walking with the prosthesis at their discharge assessment. Of them, 15 people died during the study and the remaining 149 people were not prescribed a prosthesis and mobilised in a wheelchair.
Characteristics of the eligible sample are described in Table 1. The mean (standard deviation) age was 63 (13) years, 77% were male and 70% had an amputation for dysvascular causes. Transtibial amputation level composed 71% of the group and 58% walked unaided indoors prior to their amputation. Median (interquartile range (IQR)) MMSE for the group was 30 (26.5–30) and the total MMSE range was 24–30. Median (IQR) FIM-Motor on admission for the sample was 74 (69–78).
Characteristics of people with lower limb amputation (n = 110) who were prescribed a prosthesis during hospital rehabilitation.
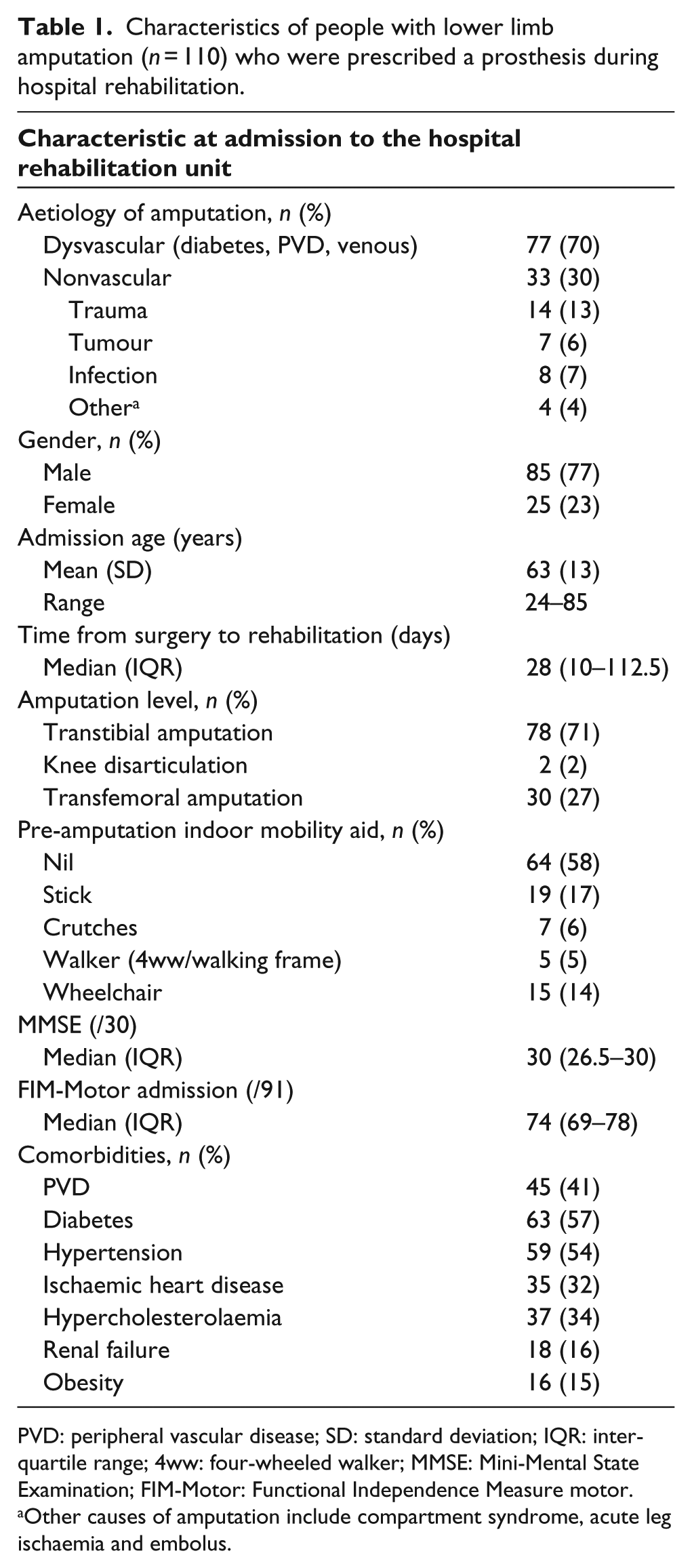
PVD: peripheral vascular disease; SD: standard deviation; IQR: interquartile range; 4ww: four-wheeled walker; MMSE: Mini-Mental State Examination; FIM-Motor: Functional Independence Measure motor.
Other causes of amputation include compartment syndrome, acute leg ischaemia and embolus.
Outcomes of people with lower limb amputation at hospital discharge
The outcomes of people with lower limb amputation at their discharge assessment are presented in Table 2. Median (IQR) length of stay was 59 (23–83) days. In this sample, the number of people in each K-level was as follows: K1, n = 6; K2, n = 43; K3, n = 54; and K4, n = 7, and 68% (n = 75) walked with a walking stick(s) at discharge from inpatient rehabilitation.
Discharge outcomes of people with lower limb amputation who were prescribed a prosthesis.
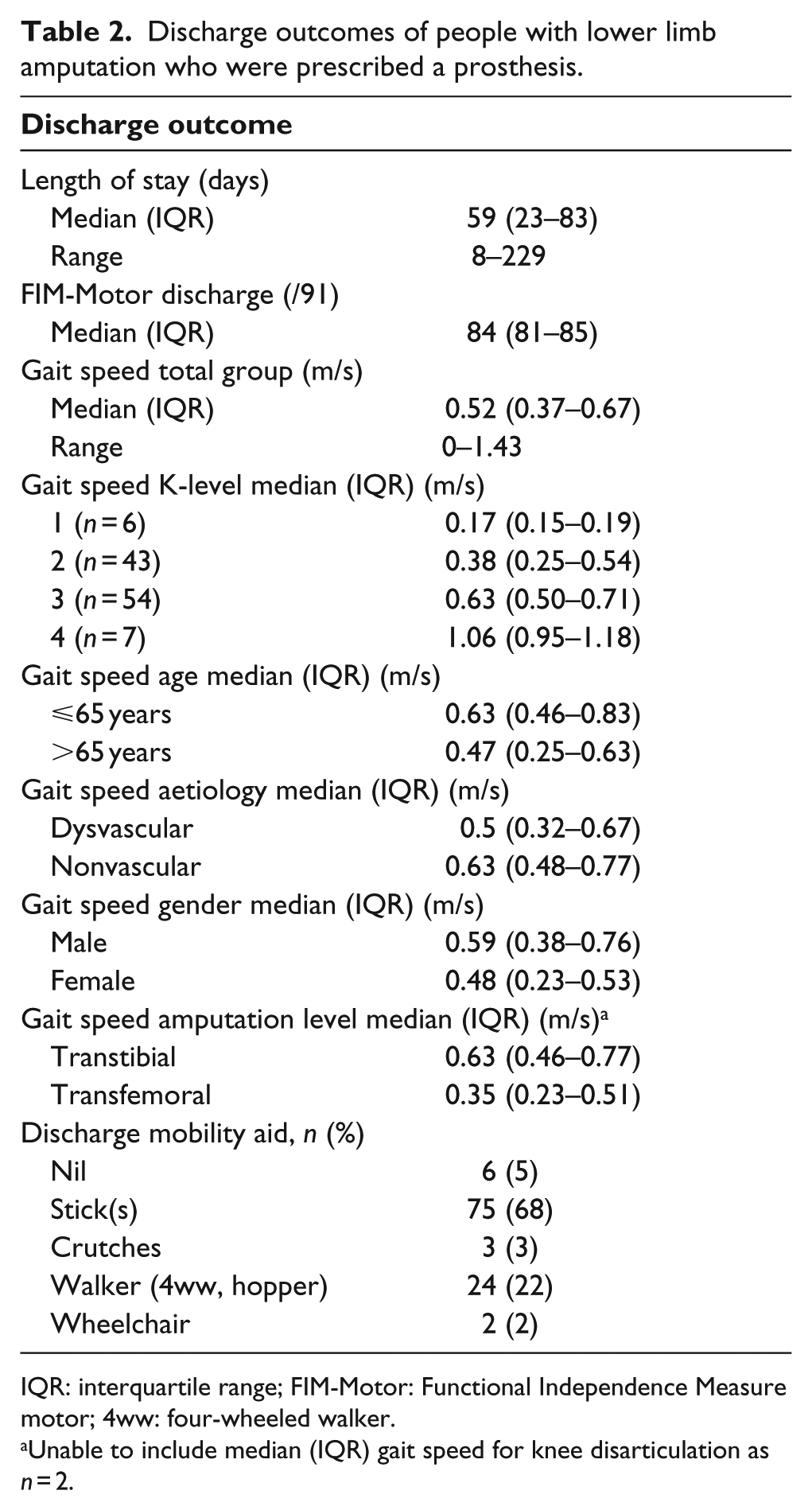
IQR: interquartile range; FIM-Motor: Functional Independence Measure motor; 4ww: four-wheeled walker.
Unable to include median (IQR) gait speed for knee disarticulation as n = 2.
Discharge gait speed and FIM-Motor by K-level
Median (IQR) gait speeds and FIM-Motor scores for each K-level, as well as for other subsamples of patients, are listed in Figures 1 and 2. In summary, median (IQR) gait speed for each K-level was as follows: K1 = 0.17 (0.15–0.19) m/s; K2 = 0.38 (0.25–0.54) m/s; K3 = 0.63 (0.50–0.71) m/s and K4 = 1.06 (0.95–1.18) m/s. Median (IQR) gait speed for people with transtibial amputation was 0.63 (0.46–0.77) m/s and for those with transfemoral amputation was 0.35 (0.23–0.51) m/s (Table 2). Median gait speed for people with dysvascular amputations was 0.5 (0.32–0.67) m/s and for nonvascular aetiology it was 0.63 (0.48–0.77) m/s. Median (IQR) FIM-Motor scores for each K-level were as follows: K1 = 82 (69–84), K2 = 83 (79–84), K3 = 85 (83–87) and K4 = 87 (86–89). Positive correlations were observed between K-level and discharge gait speed (rho = 0.64, p < 0.001) and between discharge gait speed and FIM-Motor (rho = 0.36, p < 0.001).
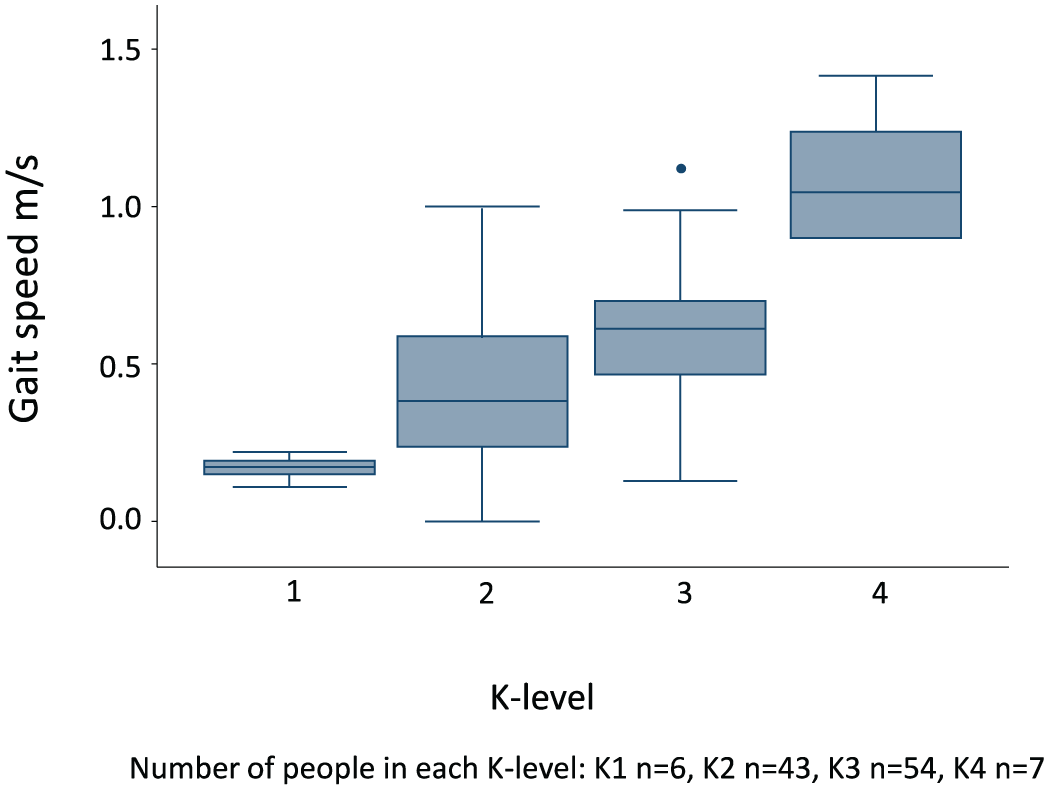
Gait speed by K-level.
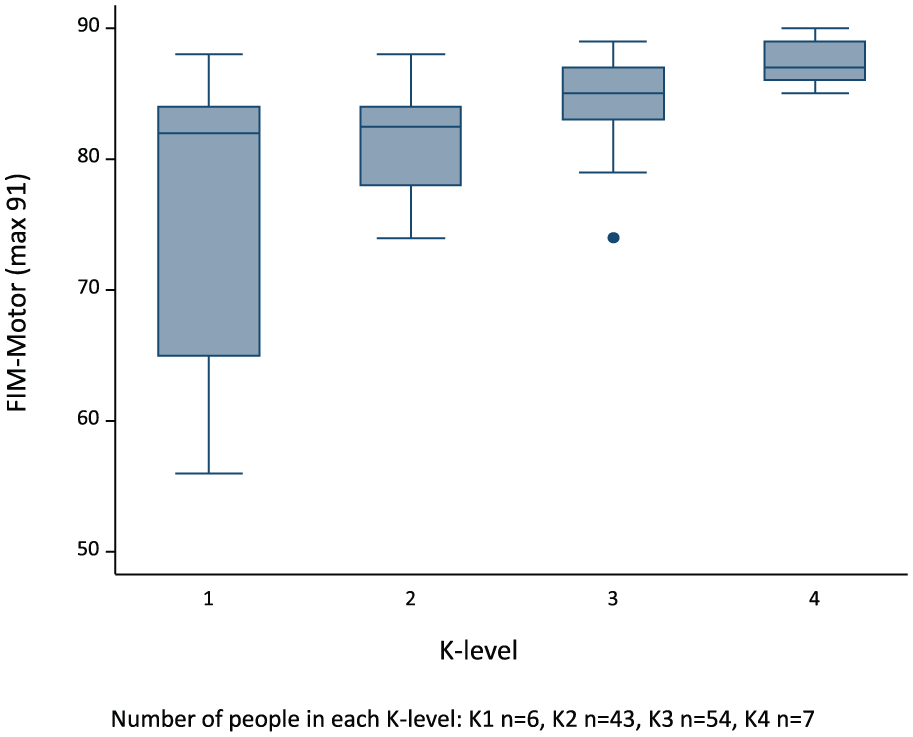
FIM-Motor by K-level.
Characteristics associated with discharge gait speed
Table 3 reports a generalised linear model examining the characteristics associated with discharge gait speed. In summary, faster gait speed was associated with higher K-level, higher discharge FIM-Motor scores (coeff = 0.07, p = 0.04), being younger (coeff = 0.04, p = 0.03), male (coeff = 0.16, p < 0.001) and having a transtibial amputation with a nonvascular aetiology (i.e. trauma, tumour, infection). MMSE (p = 0.65), pre-amputation indoor mobility aid (p = 0.34) and comorbidities present were not associated with discharge gait speed.
Summary of coefficients (and 95% confidence intervals) and p-values from the generalised linear model examining characteristics associated with discharge gait speed (model Wald Chi2(21) = 467, p < 0.001).
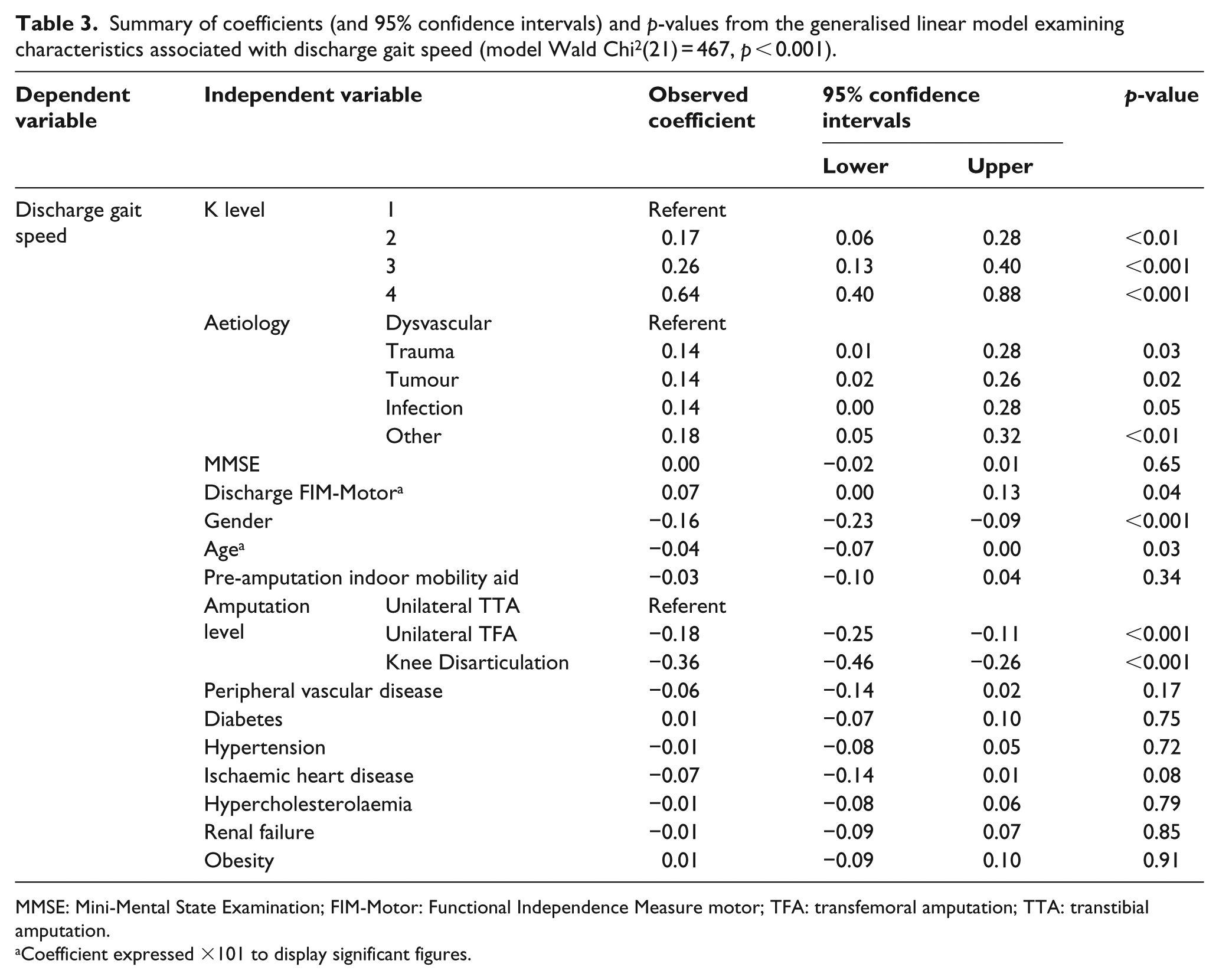
MMSE: Mini-Mental State Examination; FIM-Motor: Functional Independence Measure motor; TFA: transfemoral amputation; TTA: transtibial amputation.
Coefficient expressed ×101 to display significant figures.
Discussion
This study was the first to quantify gait speed for people with a unilateral lower limb amputation according to K-level and confirmed that K-level is related to gait speed. People with lower limb amputation with higher K-levels were found to have faster gait speeds, compared to those with lower K-levels. However, even those classified as having the greatest functioning potential (i.e. K4) had discharge gait speeds consistent with a high risk of mortality. 21 Aetiology, discharge functional ability (FIM-Motor), gender, age and amputation level were also associated with discharge gait speed. Cognition, pre-amputation indoor mobility aid and comorbidities were not associated with discharge gait speed.
People with lower limb amputations have been reported to have slower gait speeds than healthy people.11,22–25 In able-bodied populations, slower gait speed has been associated with poorer health and functioning and increased hospital visits. 26 People with gait speeds of at least 1.36 m/s have been found to have a lower risk of mortality. 21 However, in this study, gait speeds across all K-levels were consistently slower than 1.36 m/s, suggesting high risk of morbidity and mortality. The slow gait speeds observed in our study may indicate that hospital rehabilitation programmes should address factors contributing to slow gait speeds in people with lower limb amputation, such as pain, impaired weight bearing through prosthesis 27 and use of walking aids. 28 It is plausible that interventions to address these factors will ultimately improve gait speed and reduce the risk of mortality and morbidity. 29
Gait speeds of more than 0.8 m/s have been associated with being able to successfully walk in the community following stroke 12 and post-orthopaedic injury. 30 However, the extent to which people with lower limb amputation being discharged from hospital rehabilitation are able to walk at speeds associated with successful ambulation in the community is unknown. The relationship between gait speed and community mobility in people following lower limb amputation has received relatively little attention. However, in our study, more than three quarters of the K3 group ( ‘typical of the community ambulator who has the ability to traverse most environmental barriers’ 6 ) walked slower than 0.8 m/s and this may have implications for returning to work and leisure activities in the post-hospitalisation period. 31 The K4 group ( ‘has the ability or potential for prosthetic ambulation that exceeds basic ambulation skills, exhibiting high impact, stress, or energy levels’ 6 ) exhibited gait speeds that suggest successful community mobility is possible at the point of being discharged from hospital rehabilitation, although the proportion of patients in this group was low. Gait speed could be useful for goal setting and specific gait speed training may also be considered for inclusion in prosthetic rehabilitation programmes. Further follow-up studies are required to determine if people with lower limb amputation reach their prescribed potential (i.e. K-level), as K-level is a measure of potential, not the actual function.
In the context of this study, the FIM had some limitations as a measure of functional independence. The FIM comprises ratings of independence completing functional tasks that are not necessarily dependent on gait ability after amputation (e.g. dressing), and people in this study received functional task training during their rehabilitation to promote independence at discharge regardless of K-level. Nonetheless, it was interesting to note that a weak but significant correlation between K-level and FIM still existed, although the clinical importance of this is uncertain.
It is difficult to compare walking ability of our study sample with other lower limb amputation populations due to the diversity of measures used in the literature 32 and the absence of a gold standard assessment of gait in this population. Gait speed has been measured by timed 10-m walk test,11,27 2-min walk test, 25 on a treadmill, 23 3.6-m walkway, 33 8-m path, 22 12-m gait path, 32 20-m walkway 28 and along walkways of unspecified length. 24 Differences in methodology have also been noted in the use of walking aids where some studies22,27,28 permitted the use of usual walking aids, while other studies excluded people who required use of a walking aid. 33 Further research in the amputee rehabilitation setting is required to determine the best practice for walking tests, which would enable more informative comparisons of outcomes from rehabilitation programmes and models of care.
The Amputee Mobility Predictor tool was designed to assist with the prescription of a person’s K-level and takes between 10 and 15 minutes to complete. 7 Gait speed, more specifically the timed 10-m walk test, 18 has the potential to be a quicker alternative objective test to the Amputee Mobility Predictor.
An interesting finding from our study was that there were high FIM-Motor scores observed at discharge across the four K-levels. The investigators considered whether this may be due to a measurement-related ceiling effect in using the FIM with this clinical population. The presence of high FIM scores at the admission assessment among some patients lends some weight to this interpretation. 34 However, perhaps the greater contribution to consistency in FIM-Motor score at the discharge assessment across K-levels was owing to the pragmatic requirements for safe discharge from hospital being satisfied once people achieve these levels of functional independence. 35 At the participating facility, once people are sufficiently independent (regardless of K-level), they are typically discharged from hospital to continue rehabilitation as an outpatient. It is possible that gait speed and function may continue to improve among those patients undergoing outpatient rehabilitation; however, that was beyond the scope of this study.
This study identified a range of factors that are likely to influence amputee gait speed including aetiology, age, gender and amputation level. These findings were generally consistent with an earlier systematic review that reported predictors of good walking ability following lower limb amputation. 36 However, in contrast to findings from previous studies, 36 patient cognition, comorbidities and pre-amputation indoor mobility aid were not found to be associated with gait speed in our study. This may be explained, at least in part, by the nature of the sample in our study where moderate or severe cognitive impairments were not prevalent; in addition, patients who used a wheelchair for ambulation were not included in this study. There has been an inconsistency in prior studies regarding the inclusion 37 or exclusion 38 of people who used a wheelchair for ambulation. Findings from this study may not be able to be extrapolated to populations with higher prevalence of cognitive impairments or clinical samples with dissimilar functional abilities. Nonetheless, determining predictive factors of walking ability among similar clinical populations following amputation may help direct rehabilitation programmes and aid in goal setting and identification of individuals who might be able to walk in the community.
Study limitations
Data for this study were sourced from a database of prospectively recorded routine clinical assessments where clinicians completed a minimum dataset for all patients on admission and discharge from rehabilitation. Thus, data relied upon the accuracy and completeness of the documentation by the multidisciplinary team. Unfortunately, within the constraints of this study, there were no feasible processes to verify the accuracy of measurements taken and recorded. However, assessments were completed by appropriately qualified clinical staff and we are not aware of any reason to suspect inaccuracy in the data. In addition, missing data were retrieved from medical records to ensure the completeness of the dataset where possible. Another limitation of this study was that only people with unilateral lower amputation were examined, as the AMPPRO was not initially designed for people with bilateral lower limb amputation. Therefore, our findings may not be generalisable to patients with bilateral lower limb amputations. Prosthetic design (socket, knees, feet, suspension systems) is known to influence gait speed, 39 but this relationship was not able to be explored in this study.
Conclusion
Gait speed was considerably faster among each higher K-level classification at the point of discharge from hospital rehabilitation for people with lower limb amputation. However, gait speeds observed across all K-levels were typically slower than minimum thresholds associated with functional community ambulation; in contrast, they were consistent with values indicating high risk of morbidity and mortality. A range of personal and clinical factors associated with gait speed were identified in this study that may be useful for those seeking to refine rehabilitation programmes that incorporate gait speed training during hospital rehabilitation for people with unilateral amputations. Further research is required to investigate changes in gait speed characteristics after discharge from hospital and which rehabilitation-related factors may favourably influence outcomes achieved in the post-hospital discharge period. Further research is also warranted to better understand the impact of other factors that may influence the transition from hospital to returning to live in, and engage with, the community after hospital rehabilitation following lower limb amputations.
Footnotes
Acknowledgements
HB was primarily responsible for this research project and manuscript development. PV made contributions to the research project. SK, SM and AM were involved in the research project and manuscript development.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Institutional Human Research Ethics Committees approved this research (HREC/10/QPAH/68 and UQ 2013000338).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by Health Practitioner Grant (Grant/Award No. 2011/12) and ISPO ANMS Research Grant (Grant/Award No. 2013).