
Abstract
Background:
The clinical utility of measuring pressure at the prosthetic socket-residual limb interface is currently unknown.
Objectives:
This study aimed to identify whether measuring interface pressure during prosthetic design and fabrication results in closer agreement in pressure measurements between sockets made by different clinicians, and a reduction in pressure over areas of concern. It also investigated whether clinicians value knowing the interface pressure during the fabrication process.
Study design:
Mixed methods.
Methods:
Three prosthetists designed a complete prosthetic system for a transtibial residual limb surrogate. Standardised mechanical testing was performed on each prosthetic system to gain pressure measurements at four key anatomical locations. These measurements were provided to the clinicians, who subsequently modified their sockets as each saw fit. The pressure at each location was re-measured. Each prosthetist completed a survey that evaluated the usefulness of knowing interface pressures during the fabrication process.
Results:
Feedback and subsequent socket modifications saw a reduction in the pressure measurements at three of the four anatomical locations. Furthermore, the pressure measurements between prosthetists converged. All three prosthetists found value in the pressure measurement system and felt they would use it clinically.
Conclusions:
Results suggest that sensors measuring pressure at the socket-limb interface has clinical utility in the context of informing prosthetic socket design and fabrication. If the technology is used at the check socket stage, iterative designs with repeated measurements can result in increased consistency between clinicians for the same residual limb, and reductions in the magnitudes of pressures over specific anatomical landmarks.
Clinical relevance
This study provides new information on the value of pressure feedback to the prosthetic socket design process. It shows that with feedback, socket modifications can result in reduced limb pressures, and more consistent pressure distributions between prosthetists. It also justifies the use of pressure feedback in informing clinical decisions.
Keywords
Background
The design and fabrication of prosthetic sockets is a process requiring significant training and skill. Traditionally, the limb geometry is captured via plaster casting; a positive mould of the limb is created, modified and then used to fabricate the prosthetic socket. Although the use of computer assisted design (CAD) is emerging in this area, it is expensive, and cannot replace modifications made by hand in all instances. Therefore, clinics still rely on the clinical expertise of their staff in the design and manufacture of prosthetic sockets. 1 They also rely on the feedback of the person for whom the socket is designed in order to assess fit.2,3 A recent study has shown that of those fitted with a transtibial prosthesis, 59% will re-present with a problem associated with socket fit. 4 This indicates that socket fabrication to achieve good fit is a challenging task.
The interface between the residual limb and prosthetic socket of a person with an amputation is subject to complex, variable loading conditions.5–8 Furthermore, temperature and geometric fluctuations mean that this pressure distribution can vary even within the individual on a daily basis.9–11 People who have undergone a transtibial amputation may also experience altered sensation on the surface of their residual limb, meaning excess loading may not be detected through the usual pain mechanisms. 12 These factors must all be considered when clinicians are attempting to optimise socket fit.
Several sensors have been developed that can quantify the interface mechanics at the socket-limb interface.5,13–16 The application of various pressure sensors in this context has taken place over several decades. 16 As the range of custom designed and fabricated sensors increases, there is an increasing body of data available detailing the loading state at this interface. To date however, this data has not been used to inform socket modifications or design, but rather to quantify loading for a specific prosthesis or activity. This information is valuable in improving understanding of the interface mechanics of these prosthetic users. One potential avenue to extend this knowledge is to consider its use during the socket design phase. An increased understanding of when in the design and fabrication process this information is most useful and what type of information is of value may better inform the design of future iterations of these sensing technologies.
This study will use an off-the-shelf pressure measurement system to provide feedback to prosthetists during the design and fabrication of a socket. Socket design will be performed for a limb model to standardise testing conditions. This study will seek to identify whether pressure measurement feedback during the design process enables clinicians to design sockets with more consistent pressure measurements, and whether peak pressures can be reduced over anatomical features of interest. It will also qualitatively assess whether clinicians value the feedback and what further suggestions they have for methods of communicating interface measurements.
Methods
Participants
Three qualified prosthetists with different levels of experience were recruited from a private prosthetics and orthotics company in Redfern, Australia. Prosthetist 1 had 3 years of experience, prosthetist 2 had 2 years of experience and prosthetist 3 had 40 years of experience.
Each participant consented to participate prior to the study and ethical approval was granted by Human Ethics Office, UNSW, Sydney (HC180659).
Development of amputated limb model
An anatomically accurate residual limb model was manufactured for this study to ensure all clinicians fabricated sockets based on the same residual limb geometry and to enable mechanical testing. The tissues that make up a residual limb of a person with a transtibial amputation are far more complex than any materials that could be used to manufacture a residual limb surrogate. The purpose of the surrogate in this context is not to replace human testing, but rather to offer a means to perform repeated standardised testing. This also allows preliminary testing without risk to participant safety. The surrogate limb was designed to be ‘biofidelic’, which in this context means the extent to which it can mimic the anatomy and material characteristics of a transtibial residual limb. 17 Bone geometry was three-dimensionally (3D) printed from poly lactic acid (PLA) (FlashForge 3D printer, FlashForge, USA) (Figure 1(a)). The PLA was reinforced with 6-mm steel rod to increase strength during testing (Figure 1(b)). Soft tissue of the surrogate was created using ‘Banana Skin’ silicone (Barnes, Australia). This material is a two part off the shelf liquid silicone. It was chosen due to its representative material properties as well as curing time, and the fact that it does not shrink during curing. This enabled the outer geometry of the residual limb to be captured, which was the single most important aspect of the surrogate. A plaster cast of a residual limb was used as the geometry and was converted into a negative mould into which the silicone could be poured (Figure 1(c)). The bone was fixed in position inside the negative mould, and the silicone was poured around it, embedding the bone in the correct anatomical position (Figure 1(d)). The surrogate limb was then used as the basis for socket design and fabrication (Figure 1(e)).
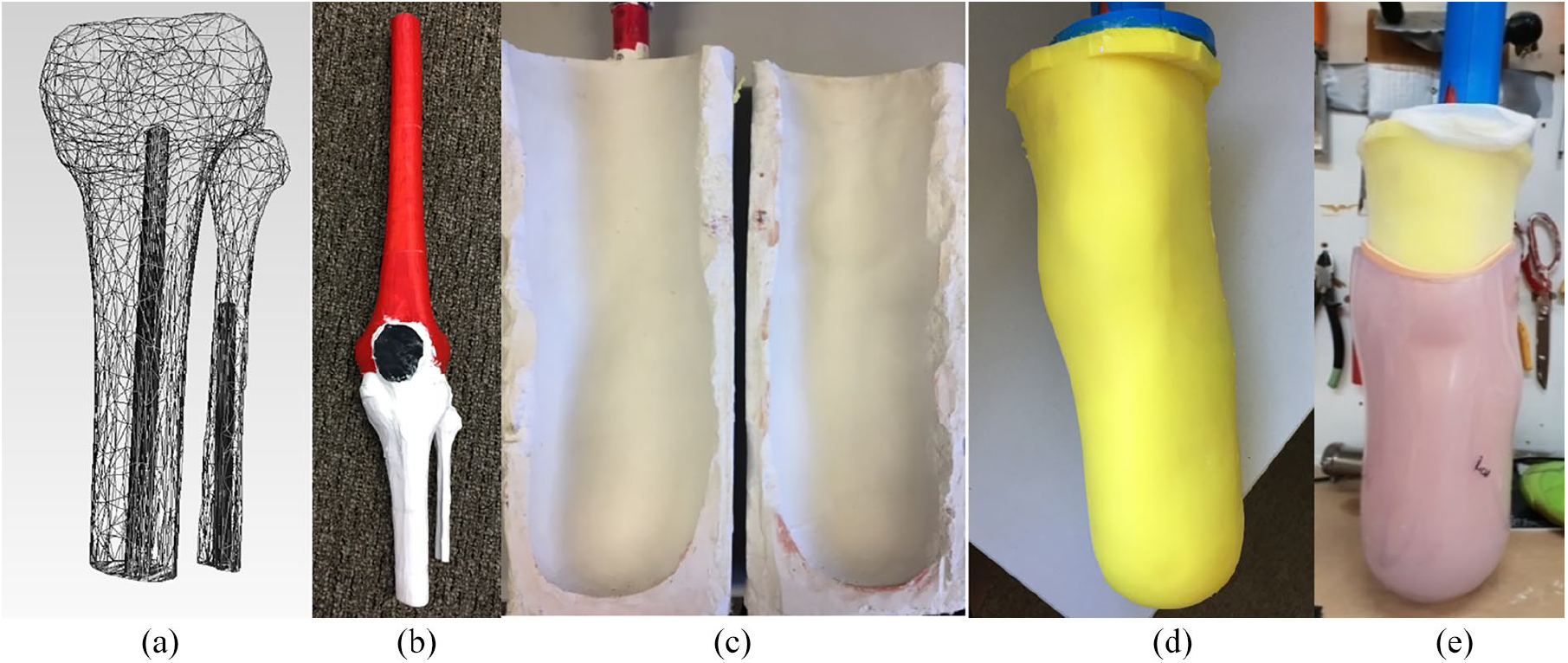
Fabrication of surrogate limb model: (a) computer model of bones with reinforcement channels for insertion of steel rod, (b) three-dimensionally printed skeleton, (c) plaster mould for silicone soft tissue, (d) surrogate limb with skeleton embedded, and (e) surrogate limb with preliminary socket.
Fabrication of initial sockets
Each prosthetist was provided with a positive plaster model of the aforementioned residual limb. They were instructed to design and create a ‘check socket’ based on this limb. All sockets were patella tendon bearing and used a knee sleeve suspension. The decision on socket and liner type was based on ease of manufacture and modification for the purpose of the study, however, this experimental set up is not limited to this configuration. They performed this task independently as if it were a part of their usual daily schedule. They were instructed to record what clinical decisions they made about loading and offloading, as well as any other specific modifications. Each prosthetist then aligned their socket on a standardised pylon and foot for testing.
Instrumentation of the socket
Collectively, the prosthetists were asked to identify four regions on the shank of the residual limb as regions of interest for this experiment. They selected the fibula head, the tibial crest, the popliteal muscle and the distal end of the limb. These regions were marked on all sockets. The minimum pressure that induces pain and maximum tolerable pain thresholds were identified for each of these regions based on the work done by Lee et al. 18 This information was provided to the prosthetists via a schematic (Figure 2). An off the shelf calibrated pressure sensor (SingleTact, USA) was placed at each of these locations. SingleTact are capacitive sensors. This type of sensor has several advantages over a resistive system including higher sensitivity, better accuracy and repeatability.16,19 They measure force applied normal to the surface of the sensor. The electronics exited the socket via a 4-mm drill hole adjacent to the sensing region Figure 3(c). Each socket was then attached to the residual limb model during testing.
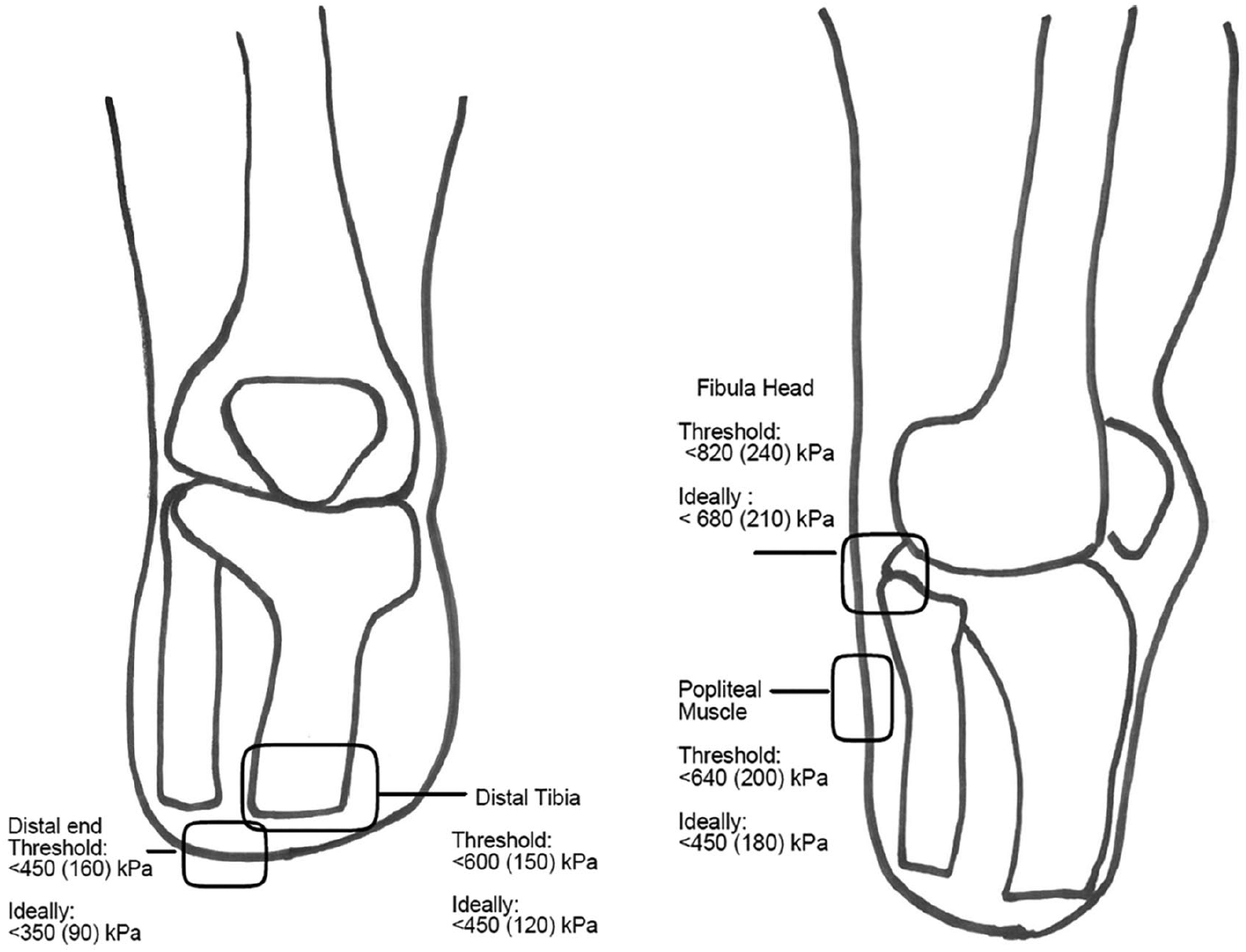
Schematic provided to prosthetists. Regions of interest were selected by the prosthetists. Minimum pressures for onset of pain and maximum tolerable pressures were included for each region. 18
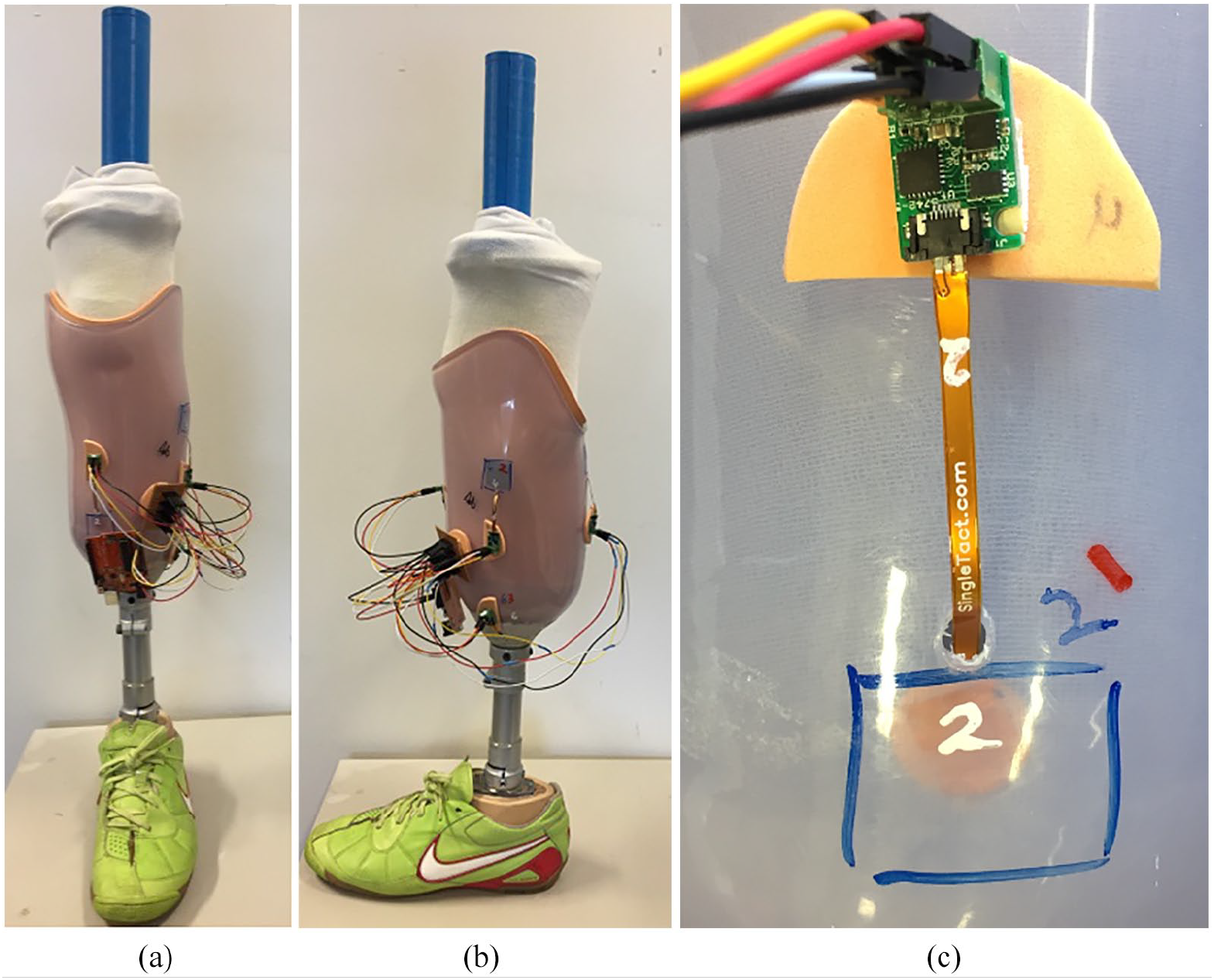
(a) Front and (b) side views of instrumentation of one of the sockets with the residual limb model in situ. (c) Close up of drill hole and sensor set up on the socket.
Testing
The limb model and socket were housed in a custom-built rig in an Instron 3369 (Instron, USA). As the limb model was designed with the knee in the extended position, two points in the gait cycle where this anatomical alignment occurs were identified for testing. One was in mid-stance where the ground reaction force was assumed to be vertical. The other was at initial contact where the model was offset from the load cell by 15° to mimic hip flexion. Force was applied to the foot at a rate of 10 mm/min, up to a maximum of 800 N. The 800 N was maintained for a period of 30 seconds (Figure 4). Pressure at each of the four anatomical locations was measured simultaneously during testing. Testing in each position was repeated five times for each socket. Pressure was defined as the force acting normal to the surface of interest divided by the cross-sectional area of the sensor.
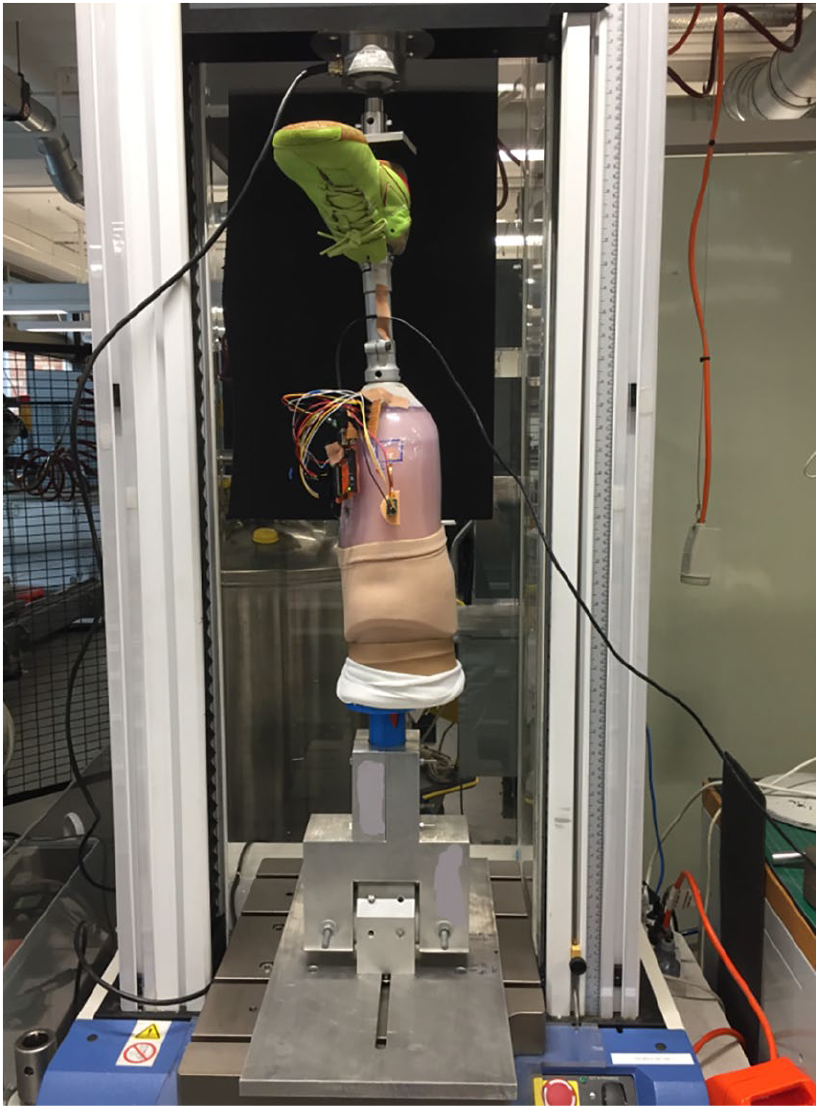
One of the sockets in the custom built rig during testing in the Instron.
Re-fabrication, re-testing and evaluation
The sensors returned a normal force in Newtons. This was converted to a pressure reading by dividing the output by the cross-sectional area of the sensor. Results from initial testing were then processed using MATLAB 2014b (Mathworks, USA). Each prosthetist was provided with feedback on the mean and standard deviation (SD) of the peak pressure occurring at each anatomical location at each position. They were also provided with the schematic outline in Figure 2.
The prosthetists were then asked to modify their socket in whatever way they felt was appropriate in order to modify loading if they felt that was indicated. They recorded the modifications that they made. Testing was then repeated using the same protocol and peak pressures were measured at each location. The mean and SD of the peak pressures for the second tests were provided to each of the prosthetists. After testing was completed and results had been provided to the prosthetists, they were each asked to complete a questionnaire detailing how useful they found the feedback process.
Results
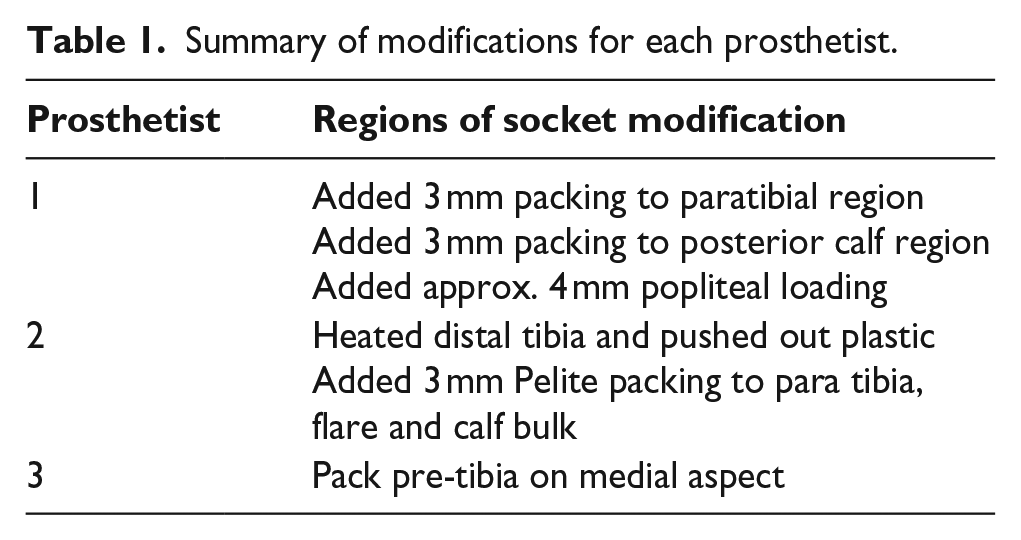
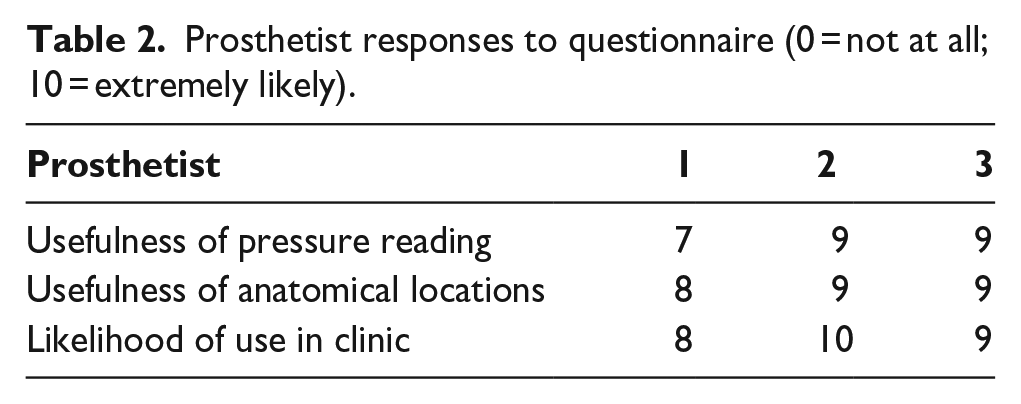
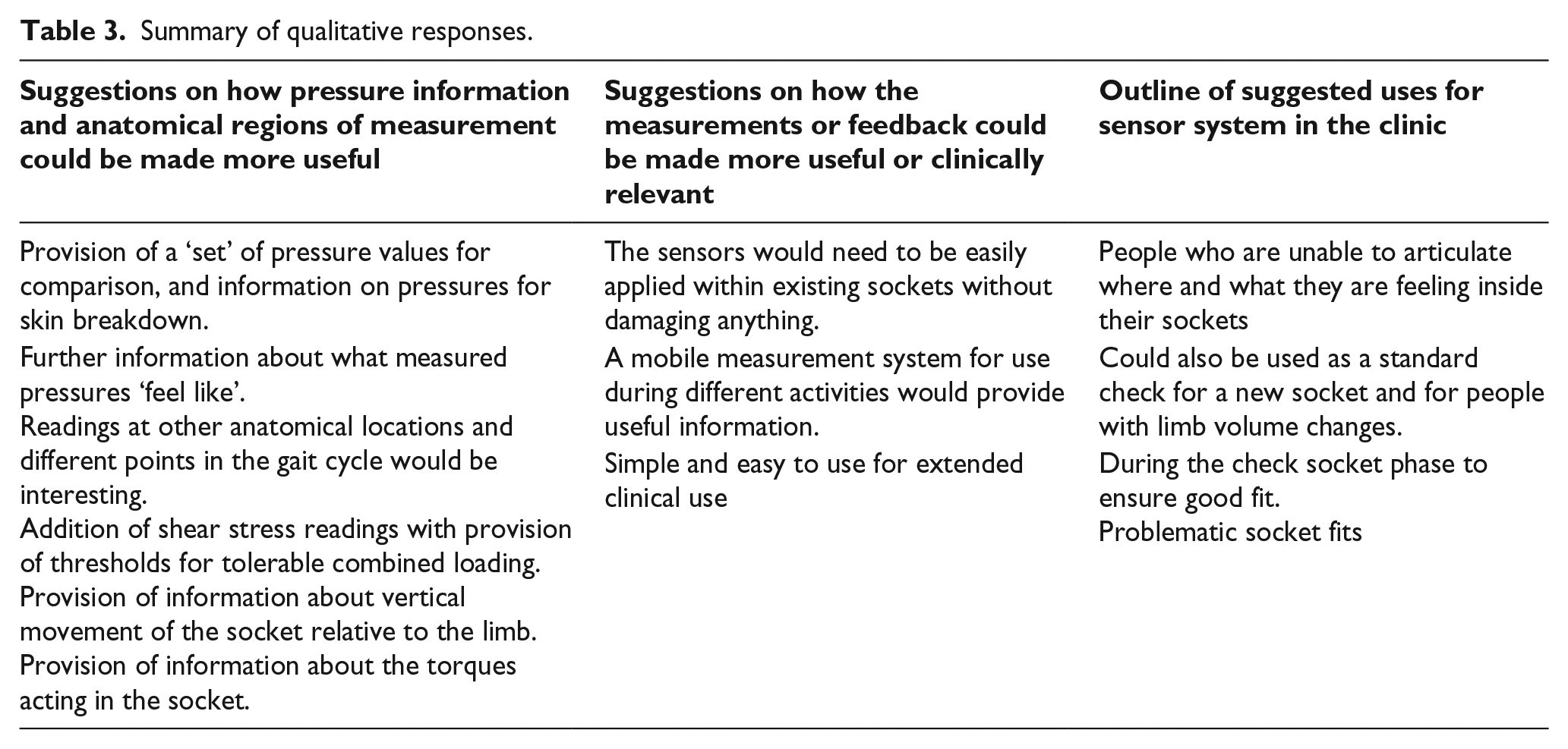
Table 1 summarises the modifications each prosthetist made when fabricating their second sockets. Pressure measurements at each of the regions of interest for the initial socket design and modified socket design at a position imitating mid-stance and heel strike are shown in Figure 5. Table 2 summarises the prosthetists’ responses to questions about likelihood of use and usefulness in the clinic. Qualitative feedback and suggestions for improvements to the system were also collected and have been summarised in Table 3.
Summary of modifications for each prosthetist.
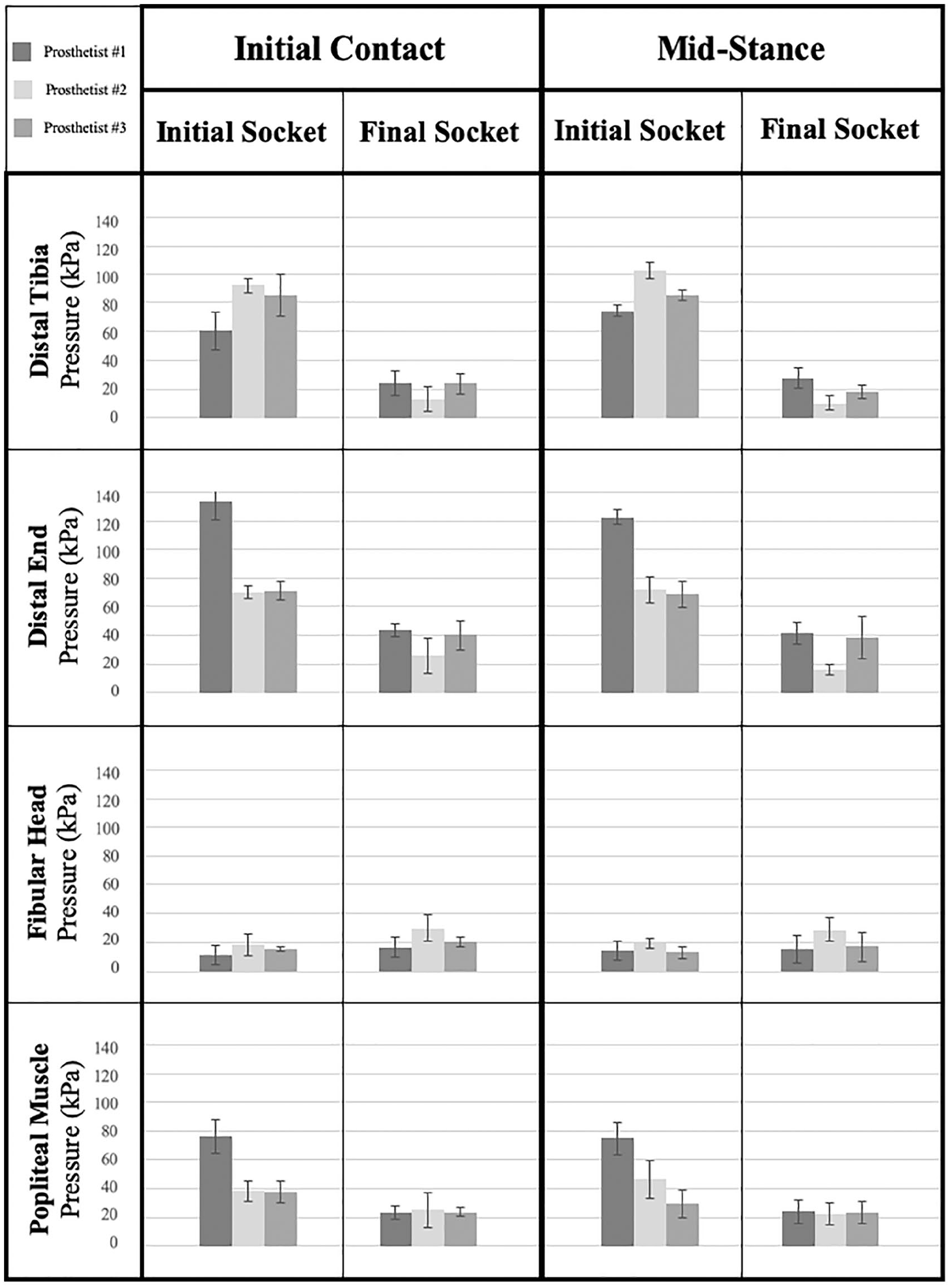
Mean pressure at each anatomical location during initial and final testing of each socket at mid-stance and initial contact. Error bars represent ±1 standard deviation.
Prosthetist responses to questionnaire (0 = not at all; 10 = extremely likely).
Summary of qualitative responses.
Discussion
Results from initial testing of each socket showed variation in magnitude as well as distribution of loading between sockets. This indicated that despite all sockets being designed for the same leg geometry, different clinicians develop different sockets. This inter-prosthetist variation is not something that has been investigated previously in the literature; however, the results from this study indicate that this may be a future avenue of investigation. Despite the variations, the pressure measurements in all regions of all sockets were well below the thresholds for in onset of pain that were provided to the clinicians.
Decisions about the modifications were made by each prosthetist individually, although each prosthetist was given access to the pressure measurements for all three sockets. All three made modifications to the paratibial region. Prosthetists 1 and 2 made additional further changes. Interestingly, despite all the designs being below the threshold pressure for the onset of pain, all the prosthetists decided to make some modifications in an attempt to further lower the pressures, or change the pressure distribution.
Post modification testing resulted in reductions in peak pressure at the distal tibia, end of the residual limb and at the popliteal muscle. This demonstrates that the methods employed by these clinicians to alleviate pressure over specific points are effective at these points. It also demonstrates the effectiveness of clinician specific modifications in altering pressures over these specific anatomical landmarks. Modifications resulted in an increase in the peak pressures at the fibula head, but not above the threshold pressures. This finding is interesting given that none of the prosthetists directly modified the region over the fibula head.
Modifications also resulted in convergence of pressures between prosthetists, shown by less variation in pressure measurements for all regions except the fibula head. Consistency between prosthetists has not been extensively investigated in the literature, however, a desire for reproducibility and consistency has been called for.20,21 This finding provides insight into a potential method to improve this constancy between prosthetists.
Results from this sensing system detected differences in loading between the sockets designed by each prosthetist, as well as before and after modifications on each socket. What these results do not determine is whether the changes in pressure between sockets are clinically meaningful. To date, there is no clearly established causal relationship between a particular pressure threshold and the onset of skin problems. 22 Although the data presented by Lee et al 18 established thresholds for pain, this does not necessary correlate with the pressure thresholds at which tissue damage may be occurring. There is evidence from one study 23 that skin breakdown may be occurring at much lower pressures that those outlined by Lee et al. 18 Simulated pressures in the range of 100kPa appear to correlate with skin breakdown in the participants examined by Cagle et al. Furthermore, parameters other than pressure have been identified in the literature that affect tissue health in in this population.24,25 In this context, it is important that clinicians have access to sensors that are capable of detecting changes in pressure at a range that is meaningful to detect potential damage. This is likely much lower than the pain thresholds that were used in this study. In other aspects of transtibial amputation research such as residual limb volume measurement, a 5% change deemed clinically significant.26,27 In the absence of further information, 5% is proposed as a starting point for a similar threshold of sensor accuracy. Based on the potential for significant injury to be occurring at pressures of 100 kPa, a clinically significant change in pressure, sensors should be able to detect a +/-5 kPa change.
There is a body of studies performed by Sanders et al demonstrating pressure outputs at or below approximately 300kPa, with most pressure data being below 200kPa.14,28,29 The range of these results are mirrored in studies by other researchers.6,30 This data agrees with the data presented in our study. These outputs are significantly less than the pain threshold values that were used in our study. Given the body of data, combined with the results presented here, it is recommended that future studies consider different threshold parameters to inform socket modifications. As a starting point, it may be useful to designate pressure over 100kPa as potentially harmful based on the recent finding of Cagle et al. 23 Furthermore, due to the potential contribution of cyclical loading, it may also be useful to consider a pressure range in addition to peak pressures. The need for shear stress measurements in this context to give clinicians a more complete picture of the loading state should not be forgotten.
Qualitative feedback was largely positive. Clinicians felt that the pressure feedback and the anatomical landmarks selected were very useful. They suggested that further information around ‘safe’ levels of pressure and also what certain pressures ‘felt like’ would add to the insights given by the feedback. This suggests that further information could have been supplied by the authors with regards to the current literature that has quantified tolerable pressures. It also highlights the need for further research to be undertaken in this space, as the body of literature is currently very small, and not generalizable over large cohorts of participants.
There was also some feedback suggesting investigation of other anatomical regions using similar methods. This is another possible avenue for future work. The prosthetists also expressed a desire for information pertaining to shear stress at the anatomical locations, as well as torque measurements in the sockets itself. This is something that has long been called for in the literature and continues to be the focus of ongoing research.14,30,31 There was also feedback calling for a mobile measurement system that could be used on human participants, which would enable pressure measurement over a range of functional activities in the clinic. This feedback also aligns with ongoing work in the literature that has identified the need for this sort of feedback in the clinical setting. 30 Another interesting element of the qualitative feedback was a request for the amount of vertical displacement that the socket underwent during loading. Vertical displacement of the prosthesis relative to the residual limb, also known as pistoning, can affect comfort and tissue health.32,33 The relationship between pistoning and acceptable comfort is currently poorly understood and warrants further investigation.
This study has several limitations. Firstly, the pressure measurements were taken at the surface between the Pe-Lite liner and check socket, not directly on the ‘soft tissue’ of the residual limb. This may mean that pressures are reduced by the cushioning effect of the Pe-Lite. This decision was made to overcome difficulties with the embedding holes in the socket and liner becoming misaligned during testing, which affected sensor output. This decision is reasonable in the context of this study, where the pressure readings themselves were less important than the ability for the setup to detect the changes in pressures that came with the modifications, as well as the differences in pressures between the different sockets made by each prosthetist. This aspect of the method may need to be modified if the system was to be used on human subjects and the pressure readings at the skin were important.Secondly, despite attempts to standardise placement of sensors between sockets, there may have been some variation in precise location between different sockets as well as between testing and retesting on each of the sockets. This may have affected pressure measurements. Thirdly, although the positioning of the surrogate limb in the machine mimics mid stance and heel strike to some degree, the lack of contraction of muscles within the socket may also have affected pressure readings. In addition to this, although the silicone used in the residual limb surrogate was selected to be representative of the material properties of a limb, it was not a perfect representation. This may have affected results. Future studies may find other products that are more ‘biofidelic’ in their nature. Finally, the sensors used in this study are subject to noise and results may contain some errors associated with that. Post processing of the data was also difficult due to this noise, and some corrections to the pressures provided to the prosthetists were needed during the study. The ongoing need for readily available reliable pressure sensors for this application has previously been highlighted in the literature, and this is echoed by the authors of this study.
Conclusions
This study has demonstrated the clinical utility of a pressure measurement system to provide feedback to prosthetists during the design and fabrication of prosthetic sockets. Quantitative results show a reduction in pressures and improved consistency between prosthetists after pressure feedback has been provided. Qualitative feedback was supportive of the system and called for improvements by adding shear measurements, and implementing a mobile system that can be used on human subjects.
Footnotes
Acknowledgements
The authors wish to acknowledge the assistance of Stephen O’Brien in the development of the sensor system used in the study.
Author contributions
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: International Society for Prosthetics and Orthotics provided financial support for this study in the form of 2017 Australian National Member Society Encouragement Research Grant. LA was supported by an Australian Government Research Training Program Scholarship as part of her doctoral studies. The facilities within the ARC Training Centre for Automated Manufacture of Advanced Composites (IC160100040), supported by the Commonwealth of Australia under the Australian Research Council’s Industrial Transformation Research Program.