
Abstract
Background and Aim:
Development of a passive suction version of the Northwestern University Flexible Sub-Ischial Vacuum socket would expand application of sub-ischial sockets to a larger proportion of persons with transfemoral amputation. While active vacuum suspension provides more positive coupling of the residual limb to the prosthetic socket, there are circumstances when use of active vacuum is not appropriate or feasible. Therefore, this technical note describes the technique modifications required to cast, fabricate, and fit a passive suction version of the Northwestern University Flexible Sub-Ischial Vacuum socket (i.e. the Northwestern University Flexible Sub-Ischial Suction socket).
Technique:
Most technique modifications stem from the use of an internal seal with the Northwestern University Flexible Sub-Ischial Suction socket and the need to account for the greater relative motion occurring between the residual limb and socket with passive suction compared to active vacuum suspension.
Discussion:
Between January 2015 and March 2018, 266 Northwestern University Flexible Sub-Ischial Suction sockets were fit successfully using the described technique modifications.
Clinical relevance
A passive suction version of the Northwestern University Flexible Sub-Ischial Vacuum socket—the Northwestern University Flexible Sub-Ischial Suction socket—broadens the application of sub-ischial sockets to a larger proportion of the population with transfemoral amputation.
Background and Aim
The Northwestern University Flexible Sub-Ischial Vacuum (NU-FlexSIV) socket was developed to provide a more comfortable socket, 1 given that socket discomfort is a leading complaint among transfemoral prosthesis users.2–4 The technique required to cast, fabricate and fit a NU-FlexSIV socket has been described in detail in previous publications.1,5 Initial unilateral amputee case studies of sockets fabricated using that technique suggest improved comfort in the NU-FlexSIV socket compared to the ischial containment socket, without a change in walking.6–8 For bilateral amputees, postural alignment and back pain may also improve with sub-ischial socket use. 9
While active vacuum suspension provides more positive coupling between the residual limb and socket, resulting in a healthier residual limb,10–12 there are circumstances when its use is not appropriate or feasible. For example, active vacuum requires the constant maintenance of total contact between the liner and residual limb to avoid forming blisters and/or sores. Hence, NU-FlexSIV socket contraindications are mostly related to issues with total contact. 1 While the NU-FlexSIV socket technique has been described,1,5 modifications to the technique are required if passive suction is to be used. Therefore, this technical note describes modifications of the previously published technique that are needed to cast, fabricate, and fit a passive suction version of the NU-FlexSIV socket (i.e. the Northwestern University Flexible Sub-Ischial Suction (NU-FlexSIS) socket). Understanding of the original NU-FlexSIV socket technique is necessary to appreciating the technique modifications described in this technical note.
Technique
The goals of the NU-FlexSIV and NU-FlexSIS sockets are the same, with both having proximal trim-lines that avoid pelvic contact and flexibility so that muscles can move comfortably within the socket. In addition, the technique for casting, fabricating, and fitting the NU-FlexSIS socket is similar to that described for the NU-FlexSIV socket 1 with a few modifications developed through clinical experimentation and summarized in Table 1.
Summary of differences in the NU-FlexSIV and NU-FlexSIS socket techniques.
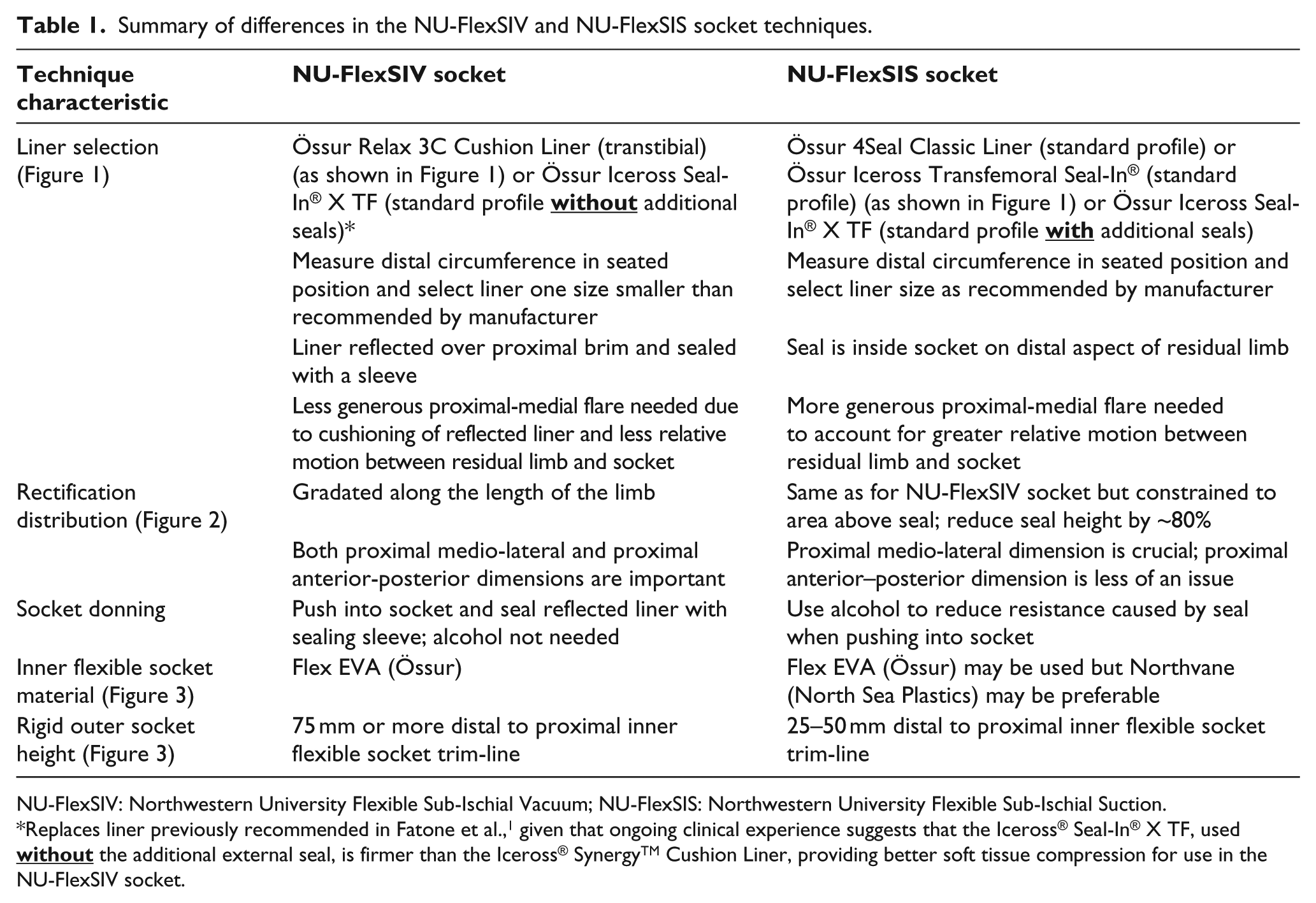
NU-FlexSIV: Northwestern University Flexible Sub-Ischial Vacuum; NU-FlexSIS: Northwestern University Flexible Sub-Ischial Suction.
Replaces liner previously recommended in Fatone et al.,
1
given that ongoing clinical experience suggests that the Iceross® Seal-In® X TF, used
Patient selection
The NU-FlexSIS socket is suitable for new amputees and those with residual limb volume fluctuation; where there are concerns with prosthesis users’ understanding of socket fit maintenance; for less active individuals where active vacuum is not necessary; where active vacuum is not tolerated; or where finances are an issue, given that active vacuum is more costly, and reimbursement is more challenging than for passive suction.
Liner selection
NU-FlexSIS socket contraindications include inability to don a seal-in liner or residual limbs <5 inches, where there is insufficient length for the seal to travel into the socket and flatten. Unlike the NU-FlexSIV socket, the NU-FlexSIS socket can be used where there exist significant muscle bunching and deep longitudinal invaginations.
Both sockets include a silicone liner along with flexible inner and rigid outer sockets. Liners preferred for use with both sockets have a full-length fabric matrix and cylindrical profile, both features that help pre-compress and minimize splaying of soft tissues. The Iceross® Seal-In® X TF, used without the additional external seal, works well for the NU-FlexSIV socket and, when used with the additional external seal, works well for the NU-FlexSIS socket; as do the Iceross® Transfemoral Seal-In® and 4Seal ClassicTM Liners (all liners from Össur, Reykjavik, Iceland). Since the seal can be located distally and internal to the NU-FlexSIS socket on all liners, it is unnecessary to reflect the liner over the proximal brim and seal with an external sleeve as in the NU-FlexSIV socket. 1 The internal seal reduces the chances of losing suction between the liner and limb, and the liner and socket, and the distal seal allows for socks to be used proximal to the seal when managing residual limb volume. To size liners for either socket, distal limb circumference is measured in the same sitting position used for casting. However, for the NU-FlexSIS socket, liners are sized as recommended by the manufacturer rather than a size smaller as for the NU-FlexSIV socket. 1
For both sockets, the impression is taken sitting with the residual limb flexed 90° and slightly abducted. 1 However, when casting with less-firm liners the proximal-medial negative mold has a more generous radius and may extend slightly more proximally (Figure 1). For the NU-FlexSIS socket, it is important to capture this more generous proximal-medial flare in the mold because passive suction allows more relative motion between the liner-clad residual limb and socket. When this happens, the more generous radius, which will be transferred from the negative impression to the proximal-medial trim-line of the NU-FlexSIS socket, will ensure the socket is comfortable in the perineum. While reflecting the liner over the proximal brim of the NU-FlexSIS socket is not necessary for sealing purposes, it could still be used to improve comfort in the perineal area, as a reflected liner will further cushion contact between the perineum and inner flexible socket.
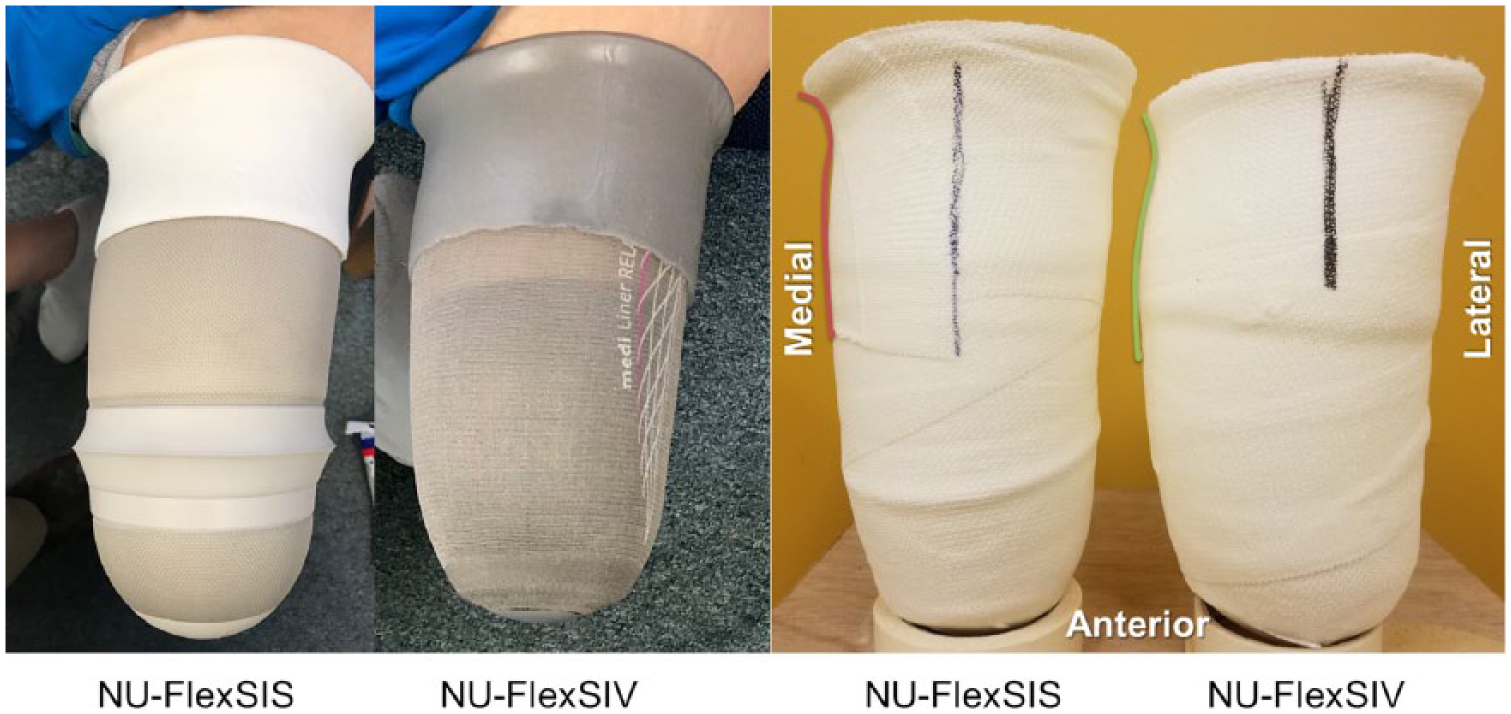
Comparison of proximal-medial flare created when casting the same residual limb for a NU-FlexSIS socket with Iceross Transfemoral Seal-In® Liner (Össur, Reykjavik, Iceland) and a NU-FlexSIV socket with Relax 3C Cushion Liner (Össur). Resulting negative molds are also shown with colored lines emphasizing differences in proximal-medial flare.
Rectification distribution
For both sockets, positive model rectification requires only plaster removal.1,5 While the same clinical algorithm 1 is used for both sockets, the rectification maps in Figure 2 (produced using the procedure described in Fatone et al. 5 ) compare rectifications for the NU-FlexSIS and NU-FlexSIV sockets for the same residual limb. While rectifications are similar, the boomerang outline highlights that the posterior rectification terminates proximal to the seal and that the proximal-lateral rectification is slightly deeper for the NU-FlexSIS socket.
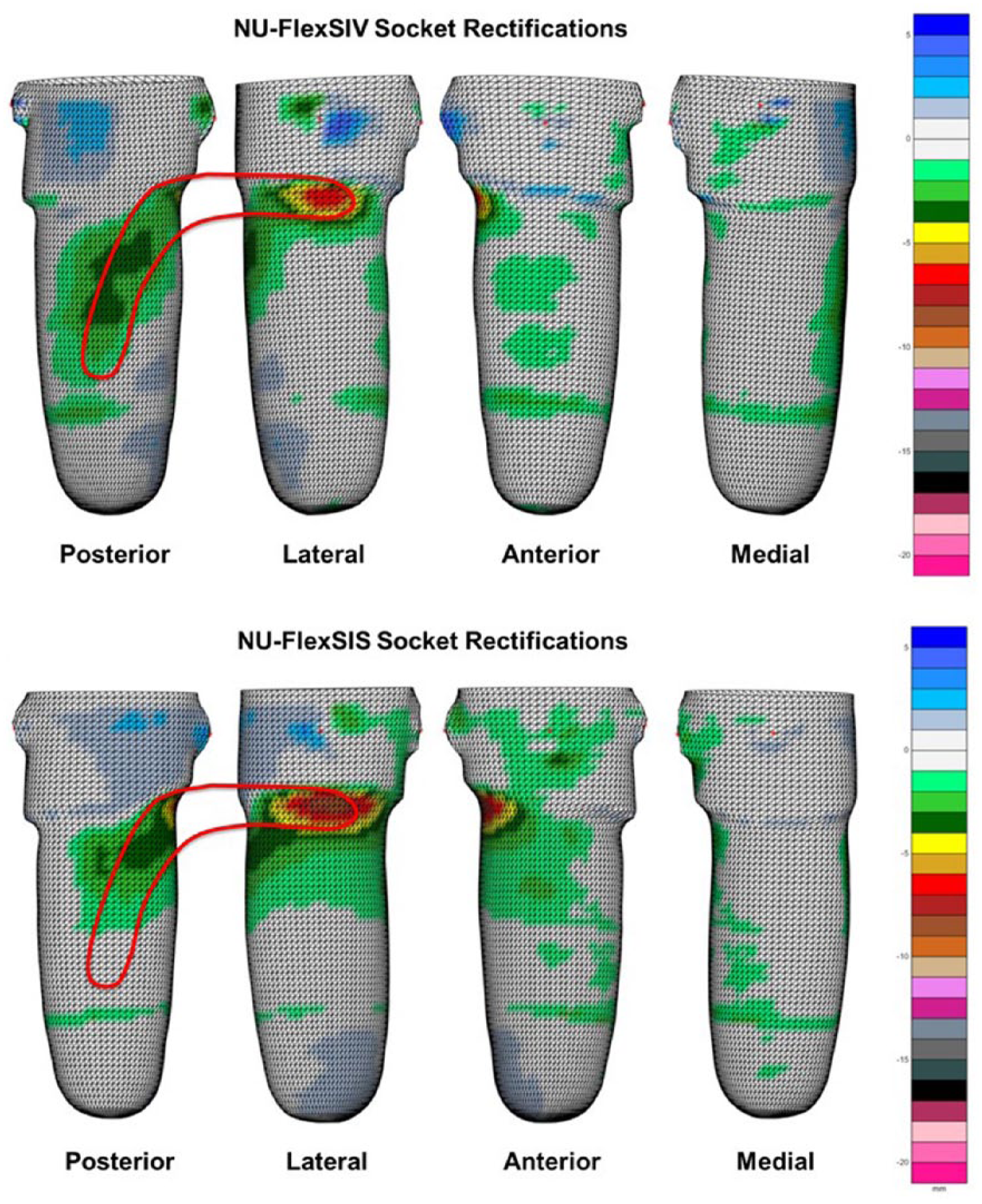
Comparison of rectification maps for the same residual limb when rectified for the NU-FlexSIS and NU-FlexSIV sockets. Color-coded scale indicates amount of plaster removed. The boomerang outline highlights that the posterior rectification terminates more proximally and that the proximal-lateral modification is slightly deeper in the NU-FlexSIS socket than the NU-FlexSIV socket.
While both the proximal medio-lateral and anterior-posterior dimensions are equally important in the NU-FlexSIV socket, the former is of primary importance in the NU-FlexSIS socket, explaining the slightly more aggressive proximal-lateral rectification shown in Figure 2. The proximal anterior-posterior dimension is less critical, given that the distal, internal seal will not allow air to enter anteriorly between the liner and residual limb when seated. This is a more challenging issue when the seal is located at the proximal socket brim.
On the positive model, the liner’s internal seal can be perceived as a plaster ridge that should be reduced in height ~80%, so it does not become overly compressed in the finished socket. No modifications are made distal to the seal to ensure that the residual limb is able to achieve total distal end contact despite any friction from the seal when the limb is pushed into the socket.
Socket donning
A diagnostic NU-FlexSIS socket is fabricated with a one-way valve on the distal, anterior-medial aspect to expel air when the liner-clad residual limb is pushed into the socket. If more than modest resistance occurs during donning, rubbing alcohol applied to the seal can reduce friction. As for the NU-FlexSIV socket, 1 static fitting of the NU-FlexSIS check socket confirms appropriate volume reductions and total distal end contact. In the NU-FlexSIS socket, the proximal-medial trim-line should be generously flared to accommodate the greater relative motion expected between the residual limb and socket. Initial check socket trim-lines may be too high, contacting the ischial ramus or tuberosity: this can be relieved by flaring and trimming to gradually lower the proximal trim-lines. It is important to keep as much of the residual limb within the socket as possible to maximize tissue containment and compression.
Neither socket requires specific alignment other than what is needed for prosthetic knee function or to accommodate muscular contractures. 1 Dynamic check socket fitting is successful if a liner-only fit is achieved; there is only slight resistance seating the limb into the socket upon standing; and the lateral-proximal trim-line is secure to the residual limb in standing and during walking. While weight-bearing, the user should feel a general tightness without any specific pressure points, especially on the distal end. There should be minimal or no contact with the pelvis during weight-bearing or with hip motion. While it is good to resolve issues of contact between the proximal trim-lines of the rigid check socket and pelvis, it is possible for minor issues to resolve by transitioning to the flexible inner socket. Unlike the NU-FlexSIV socket, 1 rigid check sockets can be used with passive suction for extended evaluation periods as liner breakdown is less likely when not reflected over the proximal brim.
Troubleshooting of socket fit is similar in both sockets. 1 For example, when distal end contact is not achieved, the proximal trim-line should be checked to ensure that it does not contact the pelvis and prevent the limb from seating fully into the socket. If proximal-lateral gapping occurs, pad the proximal-medial socket wall to pull the lateral socket wall tightly against the residual limb.
Inner flexible socket material
The inner flexible socket for the NU-FlexSIS socket can be fabricated from Flex EVA (ethyl vinyl acetate, Össur) as recommended for the NU-FlexSIV socket; however, a less-firm thermoplastic such as Northvane (North Sea Plastics, Glasgow, Scotland) may be preferable for the NU-FlexSIS socket as the socket trim-lines will be more forgiving of relative motion. This may be particularly necessary where the proximal-medial residual limb is very sensitive.
Rigid outer socket height
Rigid socket trim-lines need to be higher when a less-firm thermoplastic is used for the inner flexible socket (Figure 3). Hence, the NU-FlexSIS rigid socket trim-lines are typically 25–50 mm below that of the flexible inner socket. Posteriorly, the rigid socket trim-line can be lowered in a “U” shape to allow the flexible inner socket to splay more easily when sitting (Figure 4).
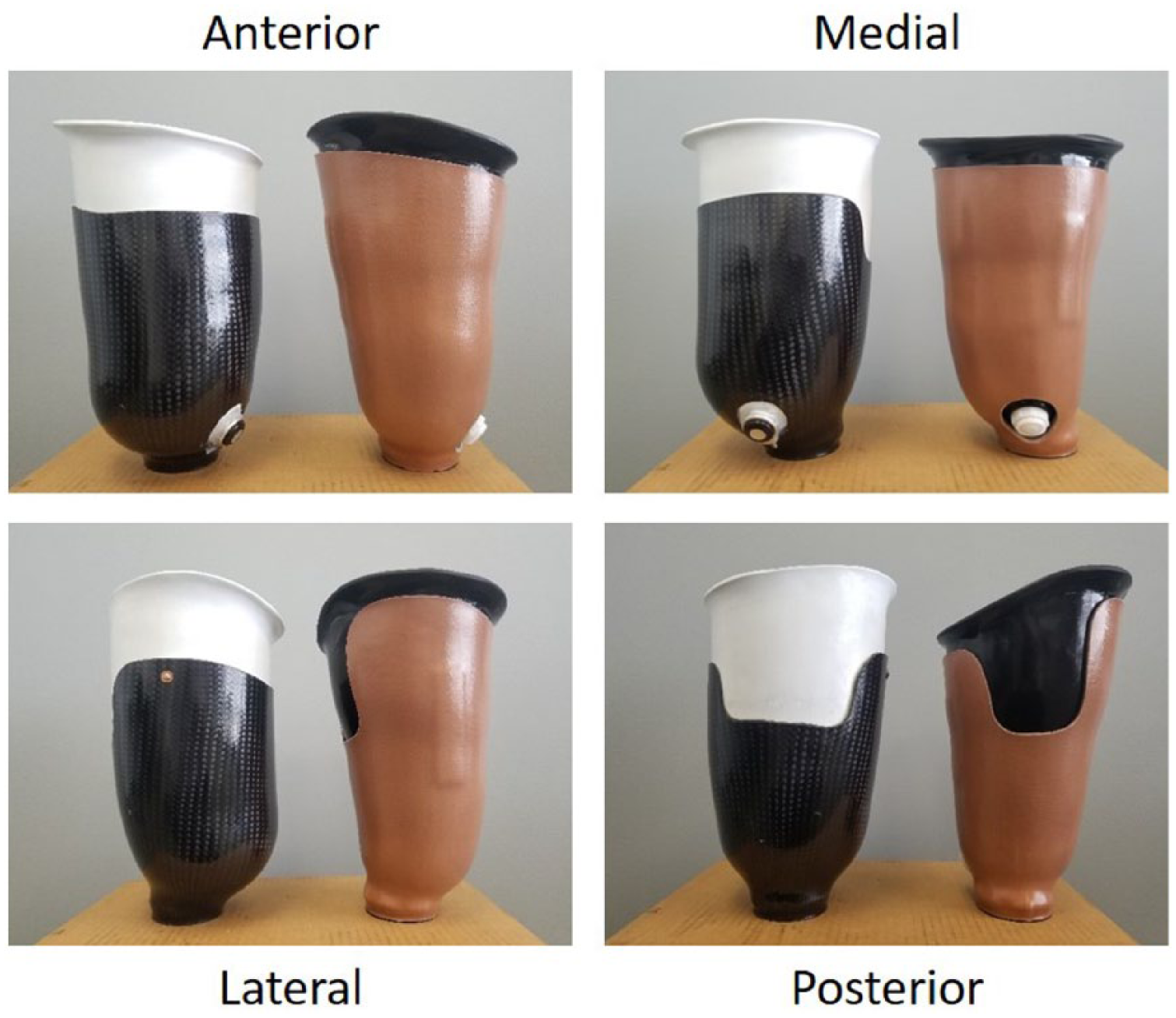
Comparison of rigid socket trim-lines for NU-FlexSIV socket with an inner flexible socket made from Flex EVA (Össur, Reykjavik, Iceland) (left) and NU-FlexSIS socket with an inner flexible socket made from Northvane (North Sea Plastics, Glasgow, Scotland) (right).
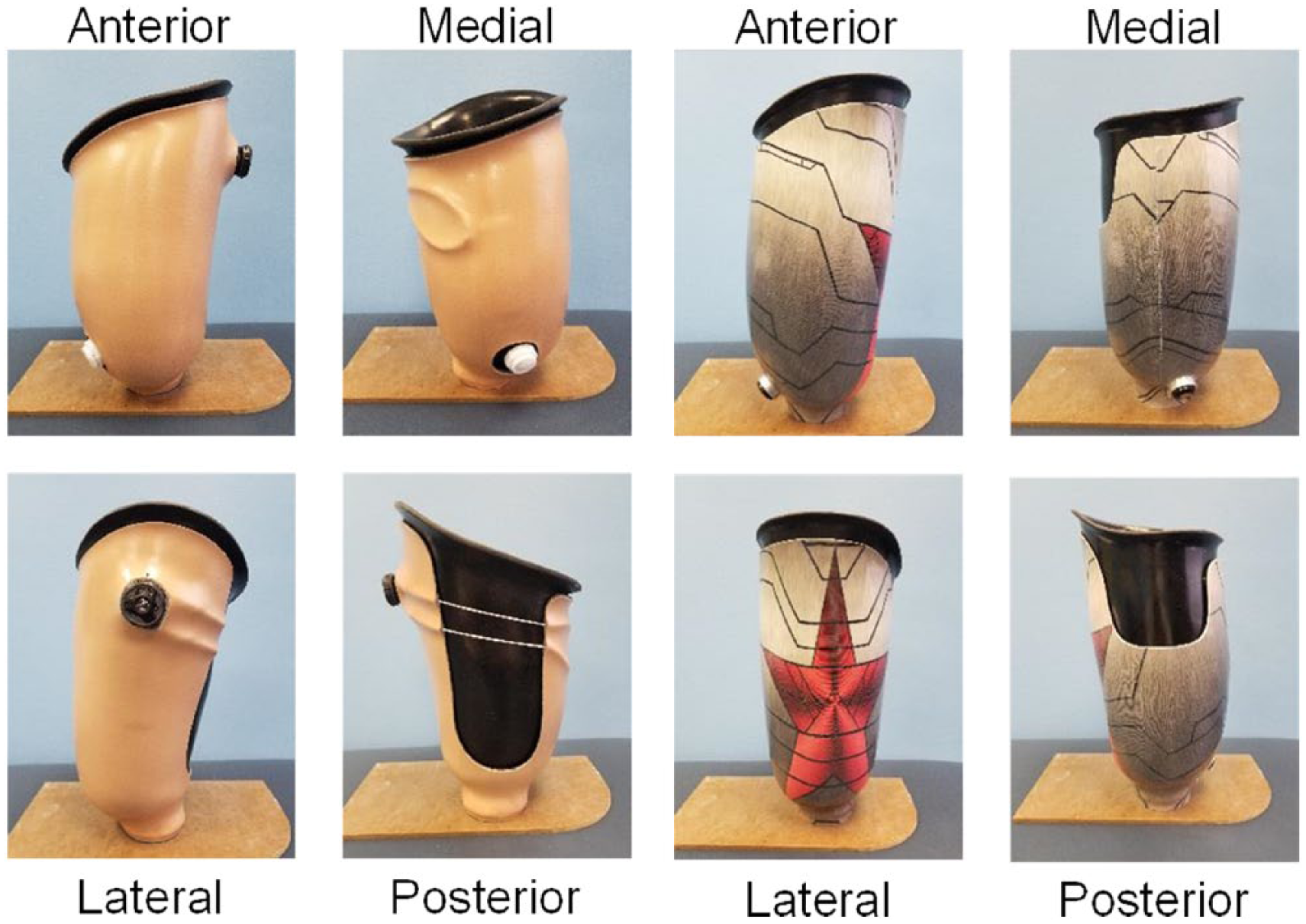
Examples of different configurations of the rigid outer socket that may be used for the NU-FlexSIS socket.
Discussion
The purpose of this technical note was to describe the technique modifications needed to cast, fabricate, and fit a passive suction version of the NU-FlexSIV socket. Given previous reports that active vacuum suspension results in less relative motion between the socket and residual limb, 10 we expected greater relative motion with the NU-FlexSIS socket. Hence, most of the technique modifications stem from the need to account for this greater relative motion and the use of an internal seal with the NU-FlexSIS socket. This greater relative motion must be accounted for by more generous flaring and flexibility of the medial proximal socket trim-line or the wearer will likely complain of proximal socket discomfort in the perineum. The internal seal negates the need to rectify the mold distal to the seal and reduces issues with loss of suspension when anterior gapping occurs in sitting but potentially places greater tension on the limb during socket donning. Additionally, while the NU-FlexSIS socket is observed to work well in 266 fittings, transverse plane prosthesis rotation is occasionally greater in the passive suction version than the active vacuum version, given the difference in suspension forces.
The development of a passive suction version of the NU-FlexSIV socket expands the application of sub-ischial sockets. It provides an option that is easier to manage in new amputees, for those in whom volume is likely to fluctuate, where limbs are insensate, and for lower activity users who may not benefit from added vacuum. This is reflected in the types of patients with successful clinical fittings of the NU-FlexSIS socket by the first author in his clinical practice: 38% to new amputees, 55% to individuals with dysvascular amputation, and 29% to limited community ambulators (i.e. those classified as having a Medicare Functional Classification level of K2 13 ). Finally, where necessary, a suction version also allows the prosthetist to create reliefs in the socket over problematic areas of the residual limb; whereas, reliefs should be avoided when using vacuum suspension where reliefs in the socket disrupt total contact between the limb and socket and may cause blistering.
While our experiences teaching these technique modifications over the past year suggest that it is possible to achieve a successful initial socket fitting with positive feedback from the prosthesis user, further evaluation of the NU-FlexSIS socket is needed to substantiate the outcomes observed during clinical practice and when teaching the technique, particularly in less active individuals. Pre-liminary evaluation of the NU-FlexSIV socket has been primarily targeted at higher functioning individuals.8,14 However, individuals who are less active may also benefit from a socket that is more comfortable. In particular, improving sitting comfort, may lead to increased prosthesis wear, and if the prosthesis is being worn, bouts of walking and step counts may also increase.
Key Points
Development of a passive suction version of the NU-FlexSIV socket expands application of more comfortable sub-ischial sockets to a larger proportion of persons with transfemoral amputation.
While the NU-FlexSIV socket technique has been described, modifications of the technique are needed if passive suction is to be used.
Most of the technique modifications for the NU-FlexSIS socket stem from the use of an internal seal and the need to account for greater relative motion between the residual limb and socket.
While the NU-FlexSIS socket is observed to work well in 266 fittings, occasionally prosthesis rotation in the transverse plane can be greater in the passive suction version of the socket than the active vacuum version.
Footnotes
Acknowledgements
The authors thank Ms. Lilly Tran for producing the rectification maps.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.