
Abstract
Background:
Reduced function and health in individuals with lower limb amputation is well documented. Step count measurement could facilitate rehabilitation and help monitor functional health outcomes.
Objectives:
To determine whether mean daily step count changed between in-patient rehabilitation and consecutive leave periods.
Study Design:
Observational study.
Methods:
Nine individuals with bilateral traumatic amputations attending rehabilitation at the Defence Medical Rehabilitation Centre during a 4-month period were invited to participate in the study (two bilateral transfemoral, two bilateral transfemoral/knee disarticulation, two transfemoral/transtibial, one bilateral transfemoral plus transradial, one bilateral transfemoral plus transhumeral and one transfemoral/transtibial/transradial). Prostheses worn by each participant were fitted with an activity monitor (LAM2TM;
Results:
Nine participants completed the study (time since injury: 19 ± 7 months, age: 26 ± 6 years). Mean daily step count significantly decreased from 2258 ± 192 during in-patient rehabilitation to 1387 ± 363 at home (p < 0.01).
Conclusion:
The step count decreased when away from rehabilitation, confirming the hypothesis that the mean daily step count would change between in-patient rehabilitation and consecutive leave period.
Clinical relevance
These data provide an indication of the step count achievable by young, military male personnel with bilateral lower limb amputations and highlights differences between intensive in-patient rehabilitation and consecutive leave periods. It is suggested that further investigation and support of clinical monitoring could facilitate rehabilitation tailored to the individual.
Background
The functional outcomes and complications of traumatic amputation with regard to pain, mental health, decreased physical and vocational function and increased cardiovascular morbidity and mortality are well documented.1–5 It has generally been accepted that prosthetic mobility and participation in daily activities are likely to decrease these issues. 6 As discussed by several authors4,6,7 and stated by Park et al. 8 ‘walking is the most basic form of human locomotion and one of the most important components of many daily physical activities; it can therefore represent a significant index of human health’.
Accurate monitoring of activity levels, via a device such as a step counter, has the potential to facilitate better care and rehabilitation of individuals with amputations. It can assist clinicians to select therapies and prosthetic components and measure rehabilitation progress.7,9–15 As discussed by Parker et al., 14 it is also important to consider what the individual with an amputation is confident to do ‘in real-life’ (performance) as opposed to when they are in a ‘safe’ rehabilitation environment (capacity) with regard to utilising their prostheses in day-to-day life.
It is generally accepted that the outcomes of younger patients who undergo amputation for trauma or cancer cannot be compared with the outcomes of patients with diabetes and their associated co-morbidities, as these two groups are likely to have different expectations and health status.16,17 Military personnel who have sustained amputation due to trauma are primarily younger (18–35 years of age) and generally have better pre-injury conditioning, robust support and have expectations for recovery and rehabilitation that reach far beyond traditional outcomes achieved by standard rehabilitation practices.18,19 During recent conflicts, the characteristic injury was the bilateral transfemoral amputation, but there is little research reporting outcomes or performance in individuals with bilateral transfemoral amputation.20,21
Numerous studies have tested the validity of accelerometers to ascertain accurate activity levels in many different patient populations.9,15,22–24 Two studies incorporating unilateral transfemoral populations, with age ranges that were close to the British military population, have measured step count. Klute et al. 25 reported that five individuals with unilateral transfemoral amputation (four traumatic, one tumour, age 48 ± 12 years, time since amputation 21 ± 11 years) achieved a count of 2709 ± 536 steps/day. Halsne et al., 17 studied 17 individuals with unilateral transfemoral amputation (13 male, age: 49 ± 16 years, 58% traumatic and time since amputation: 17 ± 18 years) and reported a mean count of 1540 ± 726 steps/day. 17 It is pertinent to note that both studies used versions of the StepWatch activity monitor (Orthocare Innovations; Oklahoma City, Oklahoma), which records step data that are representative of the monitor-side limb only. In contrast, it is generally expected that healthy adults (age: 20–50 years) take 7000–13000 steps/day, where both limbs are included in the step count. 26
No published studies have measured step count in individuals with bilateral lower limb amputation, but some have captured walking performance and energy expenditure. Wright et al., 27 in their study of the physiological cost of walking in 10 males with bilateral amputations (age: 40.5 ± 11.9 years), suggested that psychological factors such as walking confidence, self-belief, and motivation as well as walking situation and cardiovascular levels of fitness could be very important in gait performance and walking speed. They reported that physiological cost ranged from 0.3–0.87 beats/m, with walking speeds of 0.68–1.3 m/s and cadence of 65–125 step/min. Ebrahimzadeh et al. 28 investigated 291 individuals with war-related bilateral lower limb amputations, an age range of 37–89 and a follow-up time after amputation of 21–28 years. They reported participants ‘were able to walk 10 m in an average of 15 ±33 s and could walk continuously 315 ±295 m with their prostheses’. Most recently, a study by Jarvis et al. 29 reported that 10 males with bilateral transfemoral amputations (age: 29 ±4 years, time from injury: 35 ±7 months, cause of injury being improvised explosive devices) walked at 1.00–1.24 m/s and cadence of 89–103 steps/minute. They concluded that participation in advanced rehabilitation programmes undoubtedly improved the functional outcomes achieved by individuals with amputation. 29 However, none of these studies have captured and compared what level of activity is possible when an individual is undergoing in-patient rehabilitation to how active they are at home.
British military personnel with amputations undergo rehabilitation within the Complex Trauma Team at the Defence Medical Rehabilitation Centre (DMRC). The Complex Trauma Team is an interdisciplinary department including physiotherapists, exercises rehabilitation instructors, occupational therapists, nurses, social workers, medical team, prosthetists, orthotists, podiatrists, psychologists and rehabilitation assistants. The rehabilitation programme run by this team, also described by Jarvis et al., 29 provides 7-h/day, 5 days a week. This includes approximately 1-h daily physiotherapy for manual therapies and prosthetic training; 3–4 h daily exercise therapy in both group and one-to-one sessions; occupational therapy for adaptation of, and training in, activities of daily living, socialisation and vocational support; social work services and mental health support. The rehabilitation programme runs for between 2 and 6 weeks at a time, over repeated admissions, with ‘recovery leave’ breaks in between, of approximately 2–8 weeks, dependent upon need. Recovery leave can be used for rest at home or return to work depending on an individual’s requirement. Rehabilitation for those with bilateral lower limb amputations can run over 2–3 years, depending on their progress and other medical interventions, for example, further surgeries. It is not known whether individuals undergoing prosthetic rehabilitation increase, maintain, or decrease their activity levels when they go on recovery leave, nor what it is realistic to expect them to achieve. The aim of this study is to characterise the daily step count levels of military personnel with bilateral lower limb amputations due to trauma and to compare the step count levels during and between in-patient rehabilitation intervals. It is hypothesised that step count will change between in-patient rehabilitation and recovery leave.
Methods
Following convenience sampling, nine participants were invited to participate in this observational study during a restricted timescale of December 2011–March 2012. Ethical approval was obtained through both the Ministry of Defence Research Ethics Committee (220/Gen/11) and the University of Strathclyde Ethics Committee (UEC 112/08). All participants were provided with written study information, and signed informed consent had to be received for inclusion in the study.
Inclusion criteria required that participants were current serving military personnel with bilateral lower limb amputation, who were undergoing amputee rehabilitation in the Complex Trauma Team at DMRC. Participants had to be more than 1-month post-delivery of primary prostheses to facilitate fine-tuning of initial fit and prosthesis comfort and allow commencement of prosthetic training. Exclusion criteria required that there was no active infection or further surgery planned during the study. In addition, due to the nature of the injuries expected, concomitant injuries (including upper limb amputation) were not a cause for exclusion, unless the individual had sustained a traumatic brain injury. Demographic data collected included age; time since injury/amputation; level of amputation; time since delivery of primary prostheses; body mass and pre-injury height. Concurrent injuries were also documented, as were prosthetic components.
One prosthesis from each pair that the participant used was fitted with an activity monitor. The Long-term Activity Monitor (LAM2TM) made by PAL Technologies Ltd, Glasgow, was selected due to its long recording time accommodating the variable rehabilitation and recovery leave timescales. It can also be located within the prosthetic shin tube eliminating risk of damage or detachment and the requirement for daily attachment to the body or prosthesis. The LAM2TM is part of the ActivPALTM family and uses the same accelerometer and a simplified data system. The reliability and validity of the ActivPALTM has been confirmed for treadmill walking, jogging and self-paced walking.30–34
From the point of activation to the point of download, the LAM2TM collected the start time and date, stop time and date, elapsed time (days) and daily number of unilateral monitor-side steps/day. The data collection process commenced with fitting activity monitors to one prosthesis for each set of devices used by the participant. The monitors were fitted at the start of one admission and data were then recovered for analysis on the subsequent admission. The analysis of the LAM2TM data involved calculation of the ‘mean unilateral monitor-side steps per day’ for 2-weeks of in-patient rehabilitation data and the consecutive 2 weeks of recovery leave data. Where a variety of prostheses were used, the step counts were summated, as this study was primarily investigating overall step count rather than any specific activity choices. Using a case record form for each participant, relevant qualitative feedback was also recorded. This was done on the next admission for each participant following their second phase of data collection and utilised two questions; what frequency and types of activities were carried out during recovery leave (e.g. sports, work, holiday) and were there any problems that stopped the individual using their prostheses (e.g. issues with residual limb comfort or socket fit).
Statistical analysis
Data were analysed using SPSS, version 22 (IBM). Skewness and kurtosis were assessed, Kolmogorov–Smirnov and Shapiro–Wilks tests of normality were also used, and the data were classified as parametric. The two-tailed paired t-test was used to compare in-patient with out-patient pairs of data with <0.05 set as the threshold for statistical significance.
Results
Nine participants completed the study; all male, age: 26 ±6 years, time since injury: 19 ±7 months and time on prostheses: 15 ±7 months, none used walking aids (Table 1). All had sustained their injuries because of explosive blasts and had been undergoing rehabilitation at Headley Court for up to 2 years at the time of this study. Five participants had sustained bilateral transfemoral amputation with two individuals having an additional upper limb amputation. Two had sustained bilateral transfemoral and knee disarticulation amputation. Two had sustained bilateral transfemoral and transtibial amputation, and one of those individuals had an additional upper limb amputation.
Participant characteristics, step count and percentage change for each participant as an in-patient and at home. Mean difference between in-patient and at home was compared using a dependent t-test (p < 0.001).
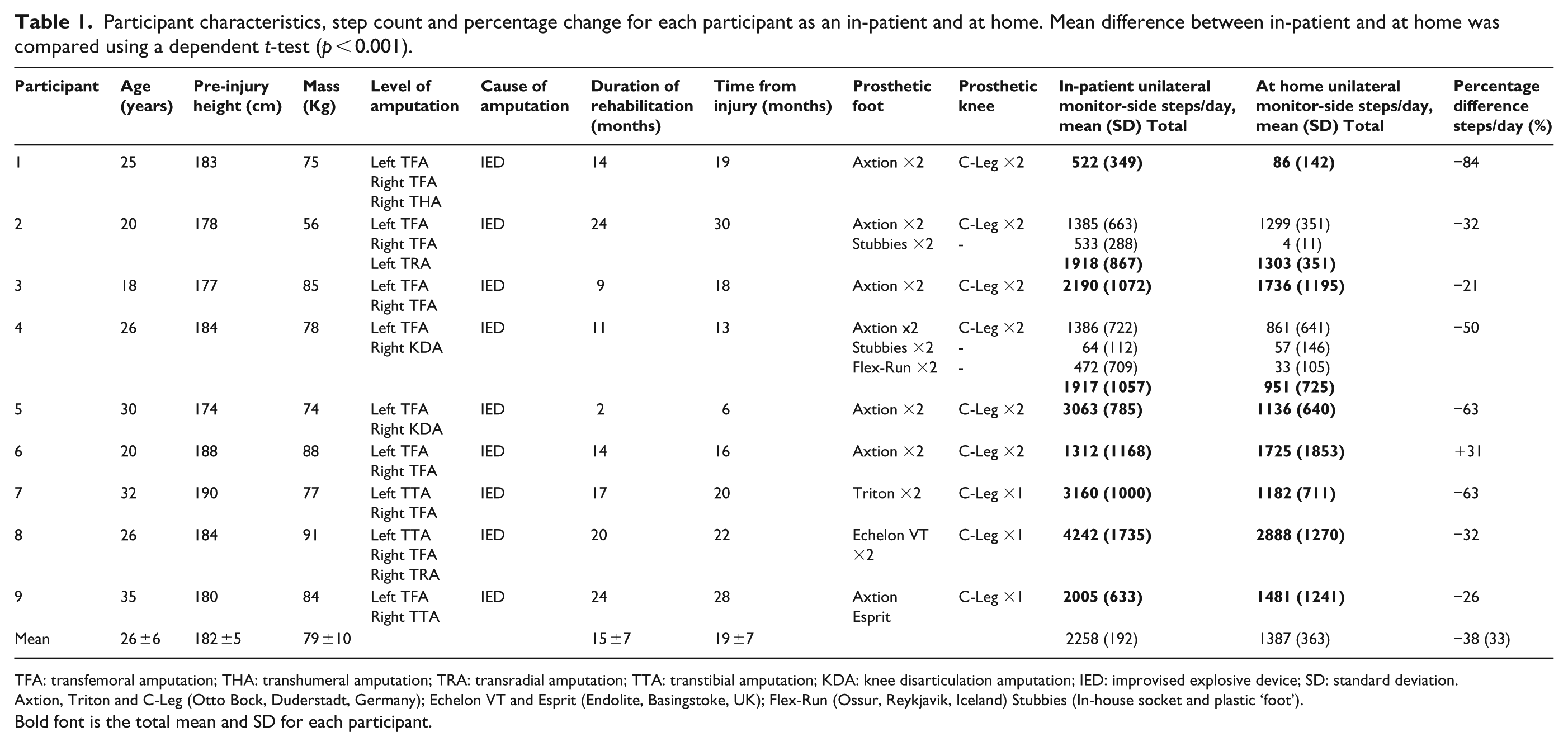
TFA: transfemoral amputation; THA: transhumeral amputation; TRA: transradial amputation; TTA: transtibial amputation; KDA: knee disarticulation amputation; IED: improvised explosive device; SD: standard deviation.
Axtion, Triton and C-Leg (Otto Bock, Duderstadt, Germany); Echelon VT and Esprit (Endolite, Basingstoke, UK); Flex-Run (Ossur, Reykjavik, Iceland) Stubbies (In-house socket and plastic ‘foot’).
Bold font is the total mean and SD for each participant.
Significantly more steps were taken as an in-patient (2258 ± 192) than when away from rehabilitation (1387 ± 363, t(8) = 3.38, p < 0.01) as indicated by Table 1 and Figure 1.
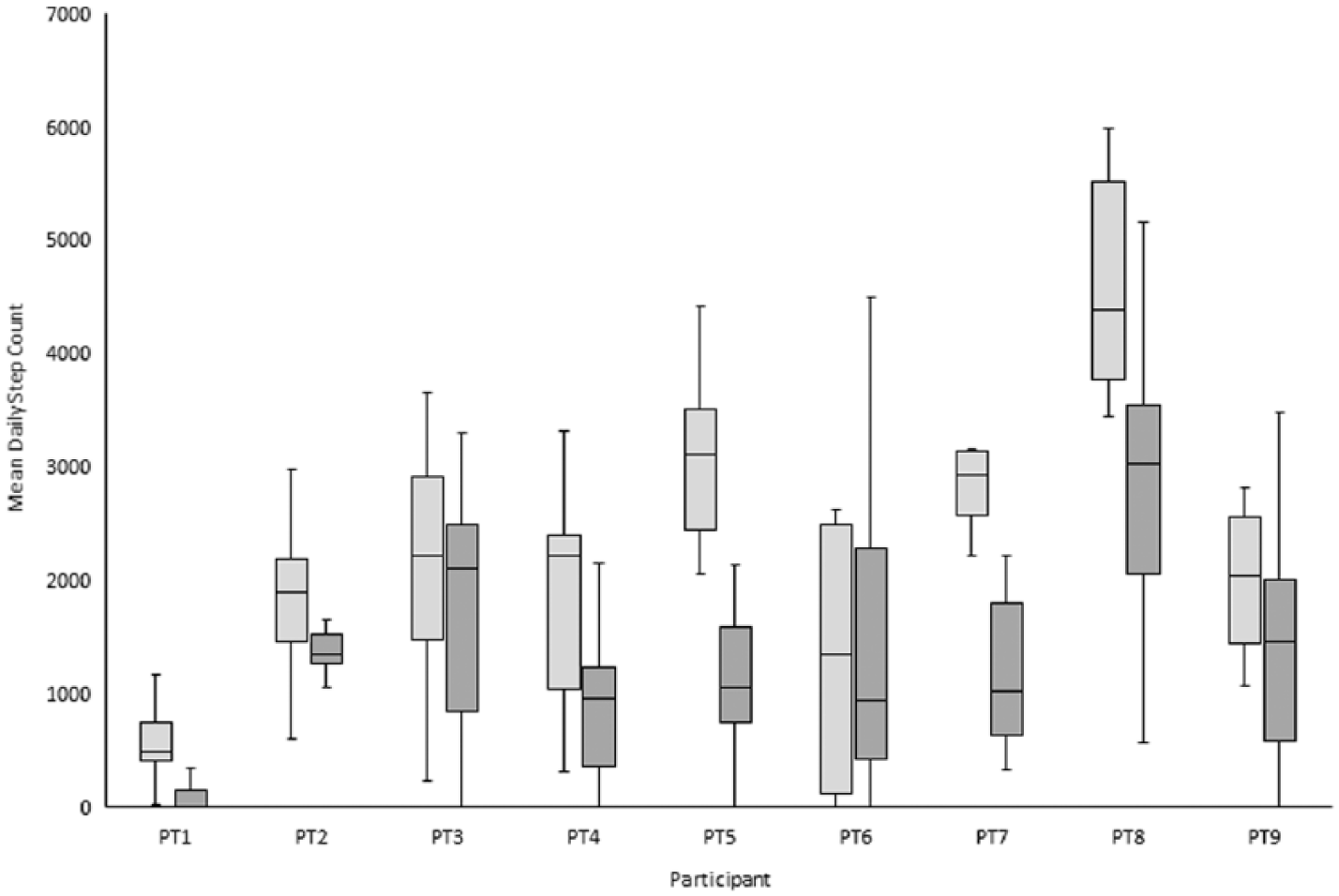
Clustered box plot of unilateral monitor-side steps per day achieved by a participant during in-patient rehabilitation (light grey bars) and when they are at home (dark grey bars). The median step count is the middle solid black line, either end of each box represents the inter-quartile range of step count per person and the whiskers indicate the maximum and minimum daily step counts, respectively. Solid circle and star represent outlier data. PT represents participant (e.g. PT1).
Three participants gave qualitative feedback regarding reasons for change in their daily physical activity when at home. Participant 4 reported that he had been on a week’s adventurous training and had not used his lower limb prostheses when taking part in activities such as scuba-diving, sky-diving and water-skiing. Participant 5 reported that on return to work he had been given an office job and that he realised this had noticeably decreased the amount of walking he was doing. Participant 8 reported that he had gone sit-skiing the first week of his leave and had therefore not been using his prostheses for part of each day. The other six participants did not report any activities or problems that they felt might have changed their activity levels.
Discussion
The aim of this study was to ascertain what the step count levels were in British military personnel with bilateral lower limb amputations, both during and between in-patient admissions for rehabilitation. This study reports that the mean number of unilateral monitor-side steps per day taken by the participants reduced from 2258 ± 192 to 1387 ± 363 when away from rehabilitation. This could be due to the 7-h rehabilitation day at Headley Court, which focuses on therapies including gait re-education, exercise conditioning and functional training for activities of daily living. This amount of activity might be considered challenging to replicate when the individual is away from rehabilitation and back in their normal home or work environment. However, working with the patient to maintain a high level of activity and continue using their rehabilitation skills when at home should be a key aim of therapy.
Three participants had a drop of more than 50% in their mean steps per day, although two of these participants reported reasons for their decreased step count. One participant did not report any reasons for a change in activity and yet increased his step count by 31% when he was away from rehabilitation. It is possible that he could have reduced his stride length when outside of the rehabilitation environment, which would have artificially increased his step count over the same distance; however, as this was not measured it is not possible to confirm. In future, we would recommend that both step count and cadence are captured simultaneously to fully understand the relationship between both parameters. As the participants were informed that their prostheses were fitted with step count monitors, this participant could have altered the amount he walked both as an in-patient and when away from DMRC because he knew he was under observation. However, as reported by Bussmann et al., 35 in their study on 10 wheelchair users, wearing an activity monitor does not necessarily cause an individual to adapt their normal behaviour.
Obtaining qualitative feedback played an important role in understanding what level of activity participants were undertaking away from rehabilitation. For example, this was demonstrated by the findings that one participant was already using running prostheses and went on adventurous training to participate in a variety of sports; while another participant went skiing during his leave. One participant returned to an office-based job, arguably an excellent outcome yet it likely decreased his step count. A reduction in step counts in administrative and managerial roles is supported by Steele and Mummery. 36 However, not all participants highlighted changes in activity or reasons for their activity level during their recovery leave. Accurate self-reporting was a problem highlighted by Stepien et al. 15 when they compared self-report to step activity monitoring and they suggested that an objective measure was therefore a more appropriate record of daily activity.
The population studied here could be considered to have a multitude of circumstances that may have an effect on their step count, both in and out of rehabilitation. While a young population, they were still undergoing in-patient rehabilitation with a high complexity and number of injuries and/or amputations as well as on-going surgical input. They have to learn to cope with these life-changing injuries and re-adjust to both their lives and how they integrate with their families, friends and surroundings.21,37 They are military personnel who were previously fit, healthy young men and this dramatic change to their lives can have an impact not only physically but psychologically too.38,39 In addition, they will need to rest after an intensive phase of rehabilitation, and relaxing and socialising with family and friends is as an important part of adjustment and rehabilitation as carrying out activities on their prostheses. 40 Ultimately, prioritisation of interdisciplinary rehabilitation to maximise social participation, functionality and physical activity could help benefit quality of life outcomes and mitigate future healthcare costs.3,29,41,42 Furthermore, it is worth considering that those with amputations and other injuries of this severity and complexity may not find it practical to only use lower limb prostheses, and there may be times when it is more appropriate to use a wheelchair. This multitude of considerations is similar to those discussed by Karmarkar et al., 43 who studied 42 military veterans and observed that ‘the interaction of demographics, health-related characteristics and mobility device characteristics affected functional performance and influenced the use of prostheses, wheelchairs or both in persons with lower limb amputation’.
Limitations
The convenience sample used to recruit participants resulted in a standardised study population all of whom were individuals with bilateral lower limb amputations. While it may not be possible to generalise the results to individuals with unilateral amputation; there was variability in other aspects of our population that suggests that our results may be applicable to a wider group. For example, the participants in this study were all at different stages of their rehabilitation; from 6–30 months post injury and 2–24 months post-delivery of prostheses, which could have had an effect on the differences in mean daily step count across participants. The restricted timescale allowed for this study limited the researchers to two blocks of 2 weeks per participant. If this could have been run over a longer period, it would have been interesting to look at repeated admissions and recovery leave periods for each individual and analyse how they progressed over time. As discussed by Boone and Coleman, 44 ‘step activity measures should be made for at least one to two weeks to get a true representation of day-to-day variability and weekly routine’. The simplified data system in the LAM2TM may not have the robust validity of the ActivPALTM, unfortunately no papers could be found to confirm or deny this. It would be recommended that either further studies were done to validate the LAM2TM individually, or that an alternative step counter could be used for future studies in this area.
Conclusion
This study aimed to determine whether individuals’ mean daily step count changed between in-patient amputee rehabilitation and the consecutive recovery leave. The data provides an insight into what step count may be possible in young, military personnel with traumatic bilateral amputations during their first 2-years of rehabilitation after injury, with the present combination of technology and rehabilitation delivered within British defence medicine. However, the considerable reduction in mean step count when participants were away from the rehabilitation environment is of clinical importance. These findings suggest that using step count data as part of rehabilitation could more accurately direct expectations and the rehabilitation process, when considered alongside the individual’s own goals. This could balance what an individual can expect to achieve in rehabilitation with what they actually do away from the rehabilitation environment.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The MSc Research for this study was funded by the Defence Medical Services, Ministry of Defence.