
Abstract
Background: Quality of life (QoL) is increasingly being recognized as an important outcome for rehabilitation programs, and has mainly been used to compare the efficacy of interventions or to compare amputees with other diseased populations. There is relatively a limited number of studies primarily focusing on analyzing the multitude of factors influencing QoL in amputees.
Objectives: To identify important background and amputation related factors which affect quality of life (QoL) in lower limb amputees, and to compare QoL profile of amputees’ to that of general population.
Study design: Cross-sectional.
Methods: Lower limb amputees 18 years and above from a rehabilitation centre, a limb-fitting centre and four limb-fitting camps were interviewed (n = 605). Structured questionnaires included patient background and amputation characteristics, and the MOS short-form health survey (SF-36) for assessing QoL. The SF-36 was administered to a general adult population using purposive sampling (n = 184).
Results: SF-36 PCS and MCS scores were found to be significantly lower for amputees when compared to those for the general population. In this study, employment status, use of an assistive device, use of a prosthesis, comorbidities, phantom-limb pain and residual stump pain were found to predict both PCS and MCS scores significantly, and explained 47.8% and 29.7% of variance respectively. Age and time since amputation accounted for an additional 3% of variance in PCS scores.
Conclusions: The abovementioned factors should be addressed in order to ensure holistic reintegration and participation, and to enable the amputees to regain or maintain QoL. Prospective longitudinal studies are recommended to systematically study the change in QoL over time and to assess its determinants.
Proper appraisal of abovementioned factors in the rehabilitation programme would assist in establishing a treatment protocol, which would adequately address QoL in amputees.
Introduction
Amputation leads to a permanent disability and brings a dramatic change in the life and function of the individual. This changed situation is experienced more by lower limb amputees than by upper limb amputees. 1 The incidence of lower limb amputation is also higher than that of the upper limb. 2 In developed countries, vascular complications are the major contributors to lower limb amputations, 3 – 5 whereas in developing countries, traumatic accidents are the major cause of amputation. 5 Vascular complications and diabetes are burgeoning health issues in developing countries, 6 and diabetic ulcers are precursors of lower limb amputation. 7,8
Limitations in body structure and function due to amputation affect the activity level and thereby the participation of the individual in society. 9 Additionally, personal and environmental factors play important roles in determining outcomes after amputation and long-term functioning of amputees. 9,10 Psychosocial support has already been demonstrated as an important determinant for adjustment to amputation. 11
Mobility is considered an important rehabilitation goal, 12 – 15 but additional factors also affect the functioning and well-being of amputees. Quality of life (QoL) is increasingly being recognized as an important outcome of rehabilitation programmes, 16,17 and also as an indicator to assess adjustment to prosthesis. 18 QoL has mainly been used to compare the efficacy of interventions, such as limb salvage procedure versus amputation, 19 – 22 or to compare amputees and other diseased populations. 23 A relatively limited number of studies 1,24,25 focus primarily on analysing the multitude of factors influencing QoL in amputees.
The purpose of this study was to identify the important background and amputation-related factors that may affect QoL in lower limb amputees. Additionally, the amputees’ QoL profile was compared to that of the general population to ascertain the impact of amputation on QoL.
Methods
Participants and data collection
Lower limb amputees 18 years and above visiting a rehabilitation centre (All India Institute of Physical Medicine and Rehabilitation), a limb-fitting centre (Bhagwan Mahaveer Viklang Sahayata Samiti) in Mumbai and four limb-fitting camps based in and around Mumbai were included in the study. This cross-sectional study was conducted in 2005 and 2006 following convenience sampling. The QoL study in the general adult population was conducted in Mumbai, its suburbs and a village (Nera, Raigad district) in its vicinity in 2006, following purposive sampling. This data was used to compare QoL profiles of general and amputee populations.
The study was approved by the Institutional Review Board of International Institute for Population Sciences, Mumbai. Subjects were provided with information on the study and signed consent was requested. Face-to-face interviews among amputees and among the general population were performed by three and two trained interviewers, respectively. In total, 622 amputees were included in the study: 360 (58%) from the limb-fitting centre, 99 (16%) from the rehabilitation centre and 163 (26%) from the camps. Of these, 17 were excluded from the study, the reasons being unwillingness to participate (8), hearing or speech impairment (4), mental incapacity (3) and other reasons (2). In the general population, 186 people were included in the study out of which two people did not participate, the reasons being lack of time (1) and psychological disturbance due to death of a family member (1).
Questionnaires
Questionnaires were administered to collect the patients’ background and amputation characteristics, and to assess QoL. Amputation characteristics included reason for amputation, amputation level, skin-problems of the stump, stump pain and phantom-limb sensation, as these have been found to be important factors determining health outcomes in lower limb amputees. 24 – 27
QoL was measured using the MOS short-form health survey (SF-36). 28 The SF-36 is a multi-purpose short-form health survey consisting of 36 questions, and has been used as an outcome measurement instrument to assess QoL in amputees. 19 – 22 The SF-36 measures health status in eight dimensions: physical functioning (PF), role limitations due to physical health problems (RP); bodily pain (BP); general health perceptions (GH); vitality, energy and fatigue (VT); social functioning (SF); role limitations due to emotional problems (RE); and general mental health covering psychological distress and well-being (MH).
The first four dimensions of the abovementioned SF-36 contribute more to the Physical Component Summary (PCS) scores, and the last four dimensions to the Mental (MCS) Component Summary scores, 29 where a higher score implies a better QoL. The PCS and MCS scores are statistically easier to interpret due to smaller confidence intervals, lower floor and ceiling effects, and fewer statistical tests required, thus lowering Type I error. 30 Moreover, PCS and MCS scores provide a comprehensive approach to the application of results in clinical decision making. 31
Statistical analyses
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS version 15). Descriptive statistics were performed for background and amputation characteristics. Cross-tabulations were used to summarize the prevalence of different amputation-related factors and comorbidities per amputation level. Bilateral and other (hip/pelvis/foot/ankle) amputees were excluded from further statistical analyses due to their lower representation.
The PCS and MCS scores were obtained from the eight SF-36 scales using a correlated (oblique) physical and mental health factor model. 32,33 Forward stepwise multivariate linear regression 34 analyses were performed for PCS and MCS scores using several background and amputation-related factors. In total, four background variables (age, sex, comorbidities and employment status) and nine amputation-related variables (time since amputation, cause of amputation, level of amputation, stump skin problems, stump pain, phantom-limb sensation, phantom-limb pain, use of an assistive device and use of a prosthesis) were entered into the initial regression analysis. Binary coding was done for each level of the categorical variables to enable forward regression. 35 The regression procedure resulted in a parsimonious model based only on the factors which achieved statistical significance (p < 0.05).
QoL scores of amputees were compared to those of the general population to assess the impact of amputation on QoL. The PCS and MCS scores were compared between amputees and the general population using a one-way, between-groups analysis of covariance (ANCOVA) with the four background variables (age, sex, comorbidities and employment status) as covariates. Bonferroni’s 36 adjusted alpha level of 0.025 was used to determine statistical significance.
Results
Background and amputation characteristics of the study population.
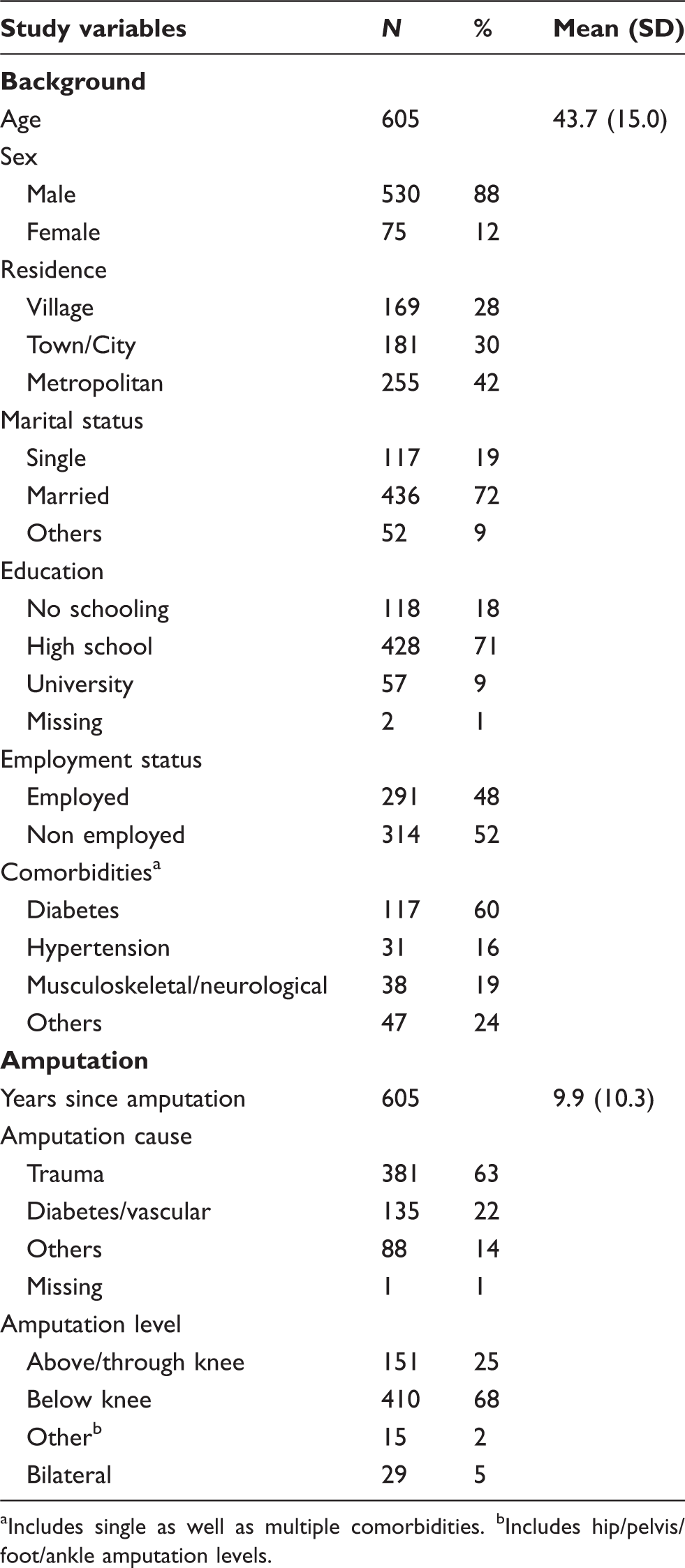
aIncludes single as well as multiple comorbidities. bIncludes hip/pelvis/foot/ankle amputation levels.
Reported prevalence (%) of amputation-related factors and comorbidities as per the level of amputation.
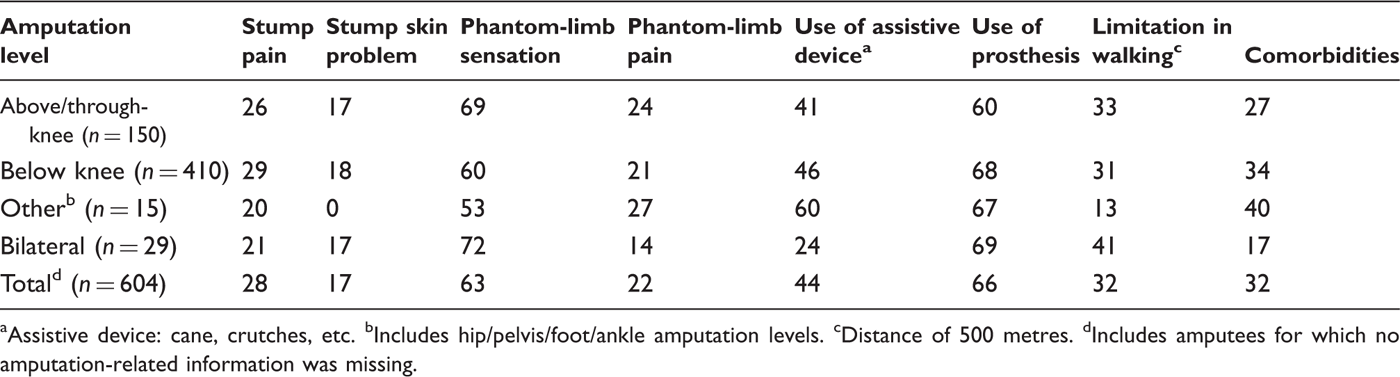
Assistive device: cane, crutches, etc.
Includes hip/pelvis/foot/ankle amputation levels.
Distance of 500 metres.
Includes amputees for which no amputation-related information was missing.
Approximately one-third of amputees (32%) reported having comorbidities. Use of a prosthesis was reported by 66% of amputees. Bilateral amputees were most limited in walking (41%) followed by above-knee (33%), below-knee (31%) and other amputees (hip/pelvis/foot/ankle, 13%). Almost half of the amputees (44%) were using assistive devices such as canes or crutches.
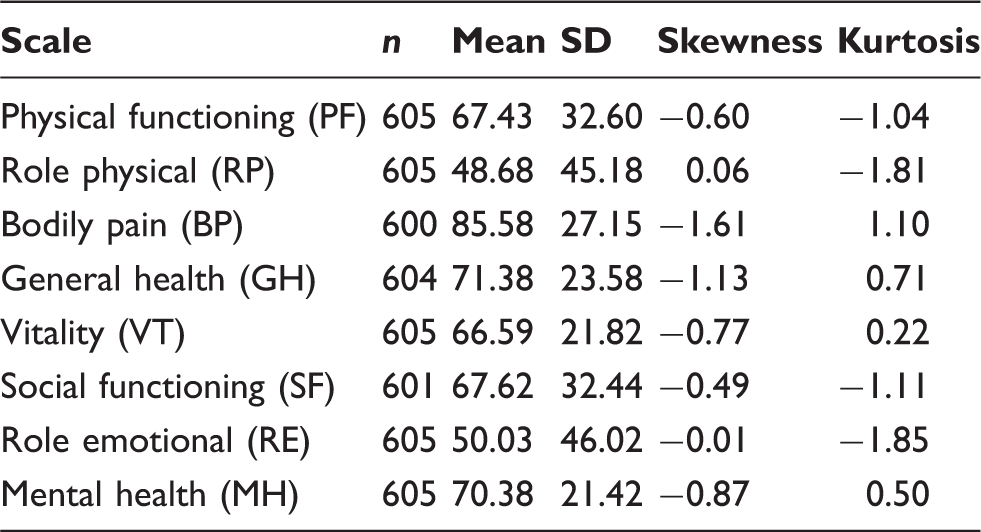
Descriptives of SF-36 scales for amputee population.
Multivariate regression of SF-36 PCS scores.
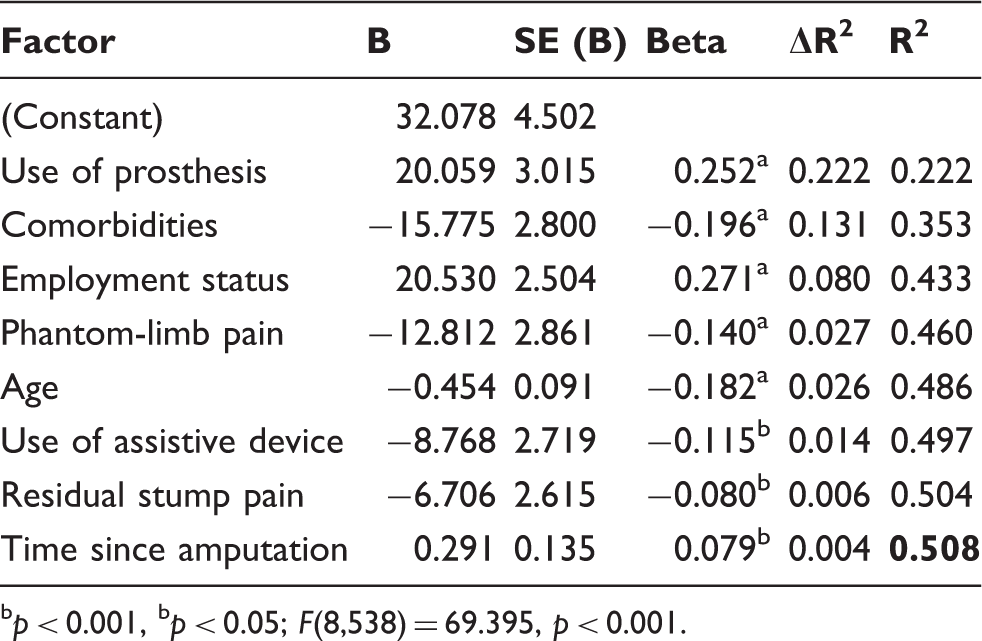
p < 0.001, b p < 0.05; F(8,538) = 69.395, p < 0.001.
Multivariate regression of SF-36 MCS scores.
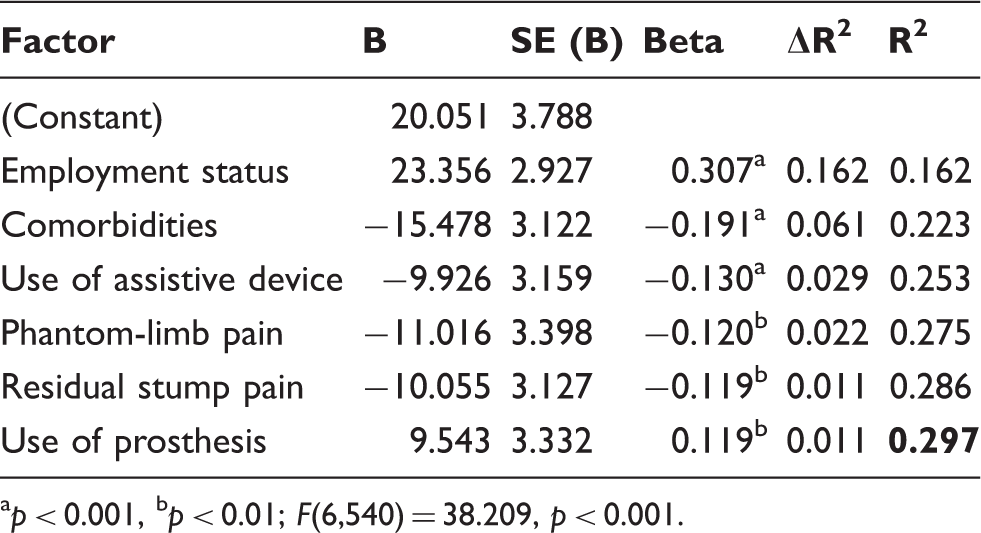
p < 0.001, b p < 0.01; F(6,540) = 38.209, p < 0.001.
Summary of ANCOVA results for SF-36 PCS and MCS scores for lower limb amputees compared to the general population.
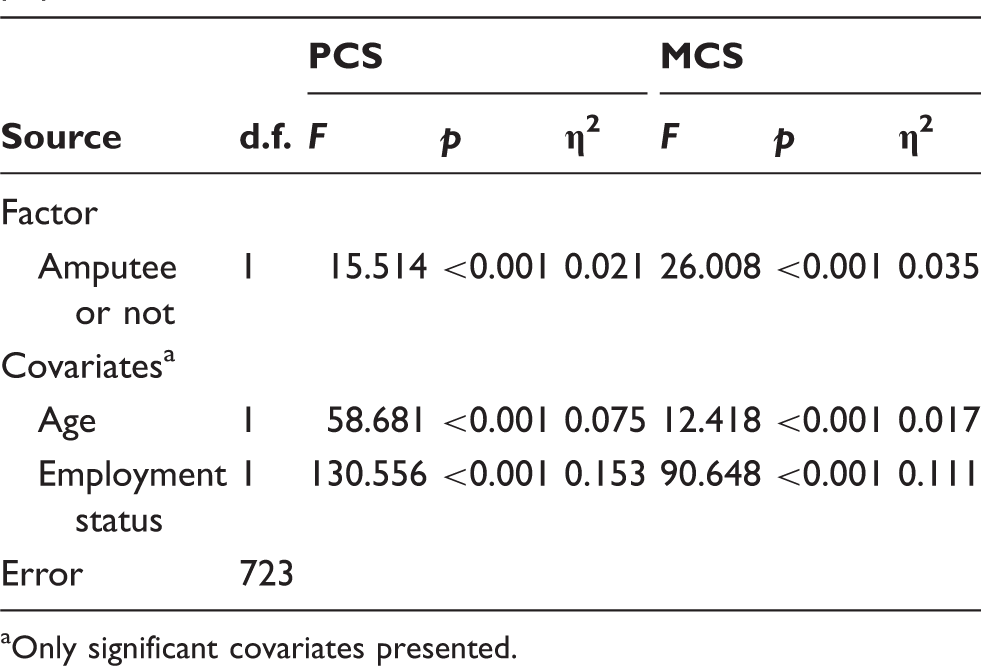
Only significant covariates presented.
Discussion
People with lower limb amputation had worse QoL as compared to the general population. This finding has been corroborated by various other studies 19,24,37,38 and indicates that amputation is a major life event potentially affecting QoL many years after the event. In this study, use of a prosthesis and comorbidities were found to be the most important factors influencing the physical health component of QoL, whereas employment status and comorbidities impacted mainly the mental health component of QoL in amputees.
Almost half of the amputees (52%) were unemployed at the time of the study, 80% of whom reported being employed prior to amputation. Of this group, 82% reported loss of employment as a direct consequence of amputation. This suggests that amputation has a significant impact on employability, and should be addressed by vocational rehabilitation and other means.
Employment prospects can be further limited due to lack of academic training and qualifications. 39 In the current study, 71% of amputees had a high school academic training and around 9% had a university education. Finding a less physically demanding job might be an impediment for the amputees due to lack of appropriate educational qualifications mandatory for such jobs.
Two-thirds of the study population comprised male amputees. A similar higher prevalence of amputation among males has been observed in other studies. 40,41 The unemployed status of male members can have a direct impact on the family’s income and living standards, since in India the male is traditionally the primary earning member of the family. 42,43 This might explain the important role of employment status in determining QoL in amputees, as unemployment may be distressing for an individual and potentially affect his mental functioning, as observed in this study. Asano et al. also reported a significant impact of employment on QoL. 25
Use of a prosthesis was found to affect the physical health component more positively than the mental health component of QoL. The importance of mobility on physical functioning has been reported in other studies. 24,25,44,45 Use of assistive devices (such as canes and crutches) had a negative impact on both PCS and MCS scores. The use of assistive devices has been studied by Hagberg and Branemark, 37 however, its impact on QoL has not been reported. Use of an assistive device might indicate an increase in the limitations experienced by amputees, and could be attributed to a lack of appropriate infrastructure. Social acceptance of the use of assistive devices, delayed proprioception 46 and lack of amputee confidence in prostheses 47 might be additional precursors to the use of assistive devices. This brings forth the importance of patient-oriented and more aggressive gait training in order to develop confidence in walking with a prosthesis and attaining greater capabilities with the prosthesis on different terrains and when performing community or work activities.
Presence of phantom-limb pain affected the physical health component more negatively than the mental health component of QoL. It seems to hinder mobility and also impact the psychological and mental state of a person. The importance of phantom-limb pain in predicting QoL has also been emphasized in other studies. 24,26,44 The prevalence of phantom pain decreases with time since amputation. 24 The average time since amputation was close to 10 years in this study, which might explain the relatively lower number of persons (22%) reporting phantom-limb pain. However, this factor was still found to significantly affect both physical and mental health components of QoL in this study. Therefore, phantom-limb pain needs to be adequately addressed not only during treatment, but also after discharge.
Proper appraisal of the relevant factors in the rehabilitation programme would be helpful in establishing an effective treatment protocol. Effective use of prostheses and employment reintegration measures would be helpful in improving the QoL in amputees. Since the presence of comorbidities negatively affected both the PCS and MCS scores, proper medical attention that could address these in tandem would be beneficial.
Comparing the findings to those obtained in developed countries, despite contextual differences such as culture and infrastructure, similar factors were found to adversely impact the QoL. 1,24,25 However, the role of employment status in QoL has not been predominantly reported in developed countries. This could be due to the presence of social-financial support mechanisms. Also, lower limb amputees in these countries are generally above 65 years of age, and would therefore usually receive a retirement pension plan and have no financial and family liabilities.
Non-participation and non-responsiveness were low in the current study due to face-to-face administration. This mode of administration ensures data completeness and enables appropriate interpretation of the questionnaire. 48 In the present study, this administration mode was also chosen due to the difficulty of retrieving addresses from the available patient databases, anticipation that a considerable number of potential participants would have a low level of education, and to circumvent the possible issue of non-response.
Since the study population was derived from a secondary source, the possibility of selection bias cannot be excluded. Recruiting patients from the primary source, such as a hospital, may have ensured a more comprehensive patient coverage. The background and amputation characteristics were self-reported by amputees and not derived from patient charts, therefore the chance of recall bias and subjectivity in reporting cannot be excluded.
Conclusion
Lower limb amputees reported worse QoL as compared to the general population. The important role of employment status and use of assistive devices in determining QoL were the key findings of this study. Use of a prosthesis, comorbidities, phantom-limb pain and residual stump pain were found to be other important factors affecting QoL. All these factors should be addressed during the treatment phase, the rehabilitation programme and after the discharge of amputees, in order to ensure their holistic reintegration and participation and to enable them to regain or maintain QoL. Prospective longitudinal studies are recommended to systematically study the change in QoL over time and to assess its determinants.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.