
Abstract
Background:
The problems of prescribing a prosthesis for a young girl with severe congenital vascular malformation deformity leading to a transtibial amputation.
Case description and methods:
Due to the high risk of recurrent bleeding and limitations regarding full weight bearing of the stump, a normal socket fitting process was not possible. Using a multidisciplinary approach, a prosthesis was designed to enable full weight bearing in a flexed knee position with ischial tuberosity support to prevent full weight bearing on the tibial part of the stump.
Findings and outcomes:
After training and adjustments to the design, a definitive prosthesis with a free motion mechanical knee joint could be used. During the training with this prosthesis, no skin problems were observed, and at the end of the rehabilitation, the patient had a high level of activities of daily living and sports.
Conclusion:
The above prosthetic solution with an adjusted socket design proved to be successful in this case.
Clinical relevance
In a patient with severe congenital vascular malformation deformity leading to a transtibial amputation, fitting of a good prosthesis without full weight bearing of the stump proved to be successful.
Keywords
Background
In this case presentation, the authors studied the prosthetic design of a lower limb prosthesis for a girl with vascular malformations (VMs). VMs are slow-flow and hemodynamically inactive VMs. In the literature on VMs, similar nomenclature has often been applied to different conditions.1,2
VMs are present at birth and worsen slowly with advancing age, showing no tendency toward regression. Hemangiomas and other vascular tumors are present at birth or develop during infancy. Males and females are equally affected. Limb VMs can involve not only the skin but also the muscles and joints. The severity of functional impairment depends on the location of the lesion and on its extension in the deep structures. Abdominal VMs can involve the gastrointestinal and genital tracts and can cause bleeding. 1
Hemangiomas and VMs of the limb can be present in a variety of different ways. Symptoms include pain, bleeding, swelling, limb length discrepancy, and cosmetic distortions. VM can lead to significant functional impairment, especially when the hemangioma or VM extends into deeper tissue. In these cases, patients often require surgical intervention. Sometimes, amputation of part of the limb is the only curative option. 2
In the case under consideration, the normal procedure of fitting a prosthesis after a lower limb amputation could not be met. The authors searched for solutions having total-surface force distribution on the stump in order to have a safe weight distribution on the VMs. Total surface bearing, shape-matching suction sockets, and gel liners are designed to transfer ground reaction forces from the prosthesis to the skeleton in an efficient manner by optimizing the stiffness of the socket/stump interface.3,4 This minimizes movement of the stump relative to the socket and simultaneously maximizes comfort. Van der Linde et al. 5 concluded in their review that a vacuum (total-surface bearing) socket guarantees a better skin contact than a normal suction or suspension socket and a better control over the prosthetic limb. Due to a high risk of bleeding in the stump with VM after a lower limb amputation in this case, the fitting of a prosthesis is not possible due to the excessive forces applied on the end of the stump. The end bearing forces in a patellar-tendon-bearing (PTB) 6 socket design are a risk factor to start the VM bleeding. The aim of this case report is to describe an alternative fitting process of a prosthesis in a girl with a transtibial amputation after a congenital VM of the right leg.
Case description and methods
A young girl had a congenital VM of the right leg with osteohypotrophy of the metatarsal bones and fibula on the right side. A magnetic resonance imaging (MRI) scan (Figure 1) showed an enormous VM in the upper and lower right leg, right hip region, pelvic region, lower back region, and internal genital organs. The venous pump function was disturbed and there was a marginally developed deep venous system. This caused extensive swelling of the right lower limb in standing position.
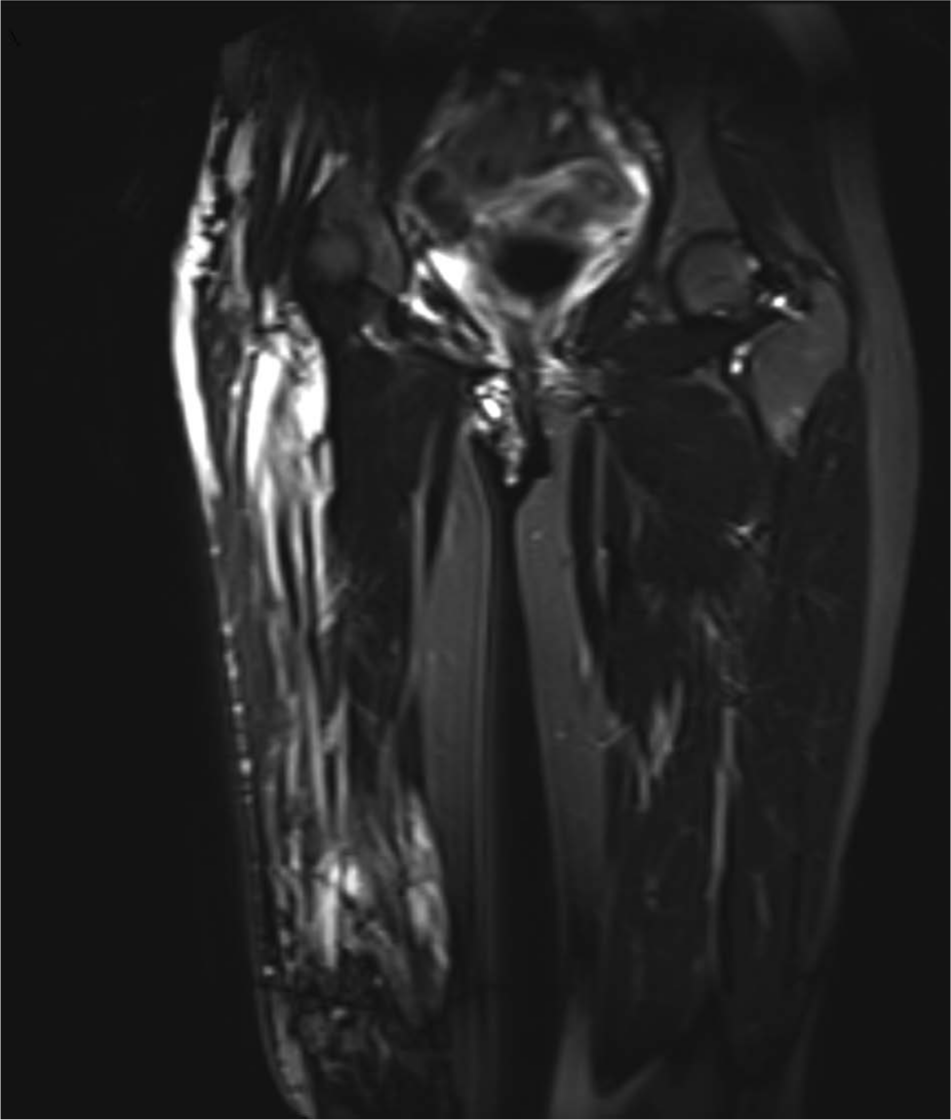
Magnetic resonance imaging (MRI) of the patient with an enormous vascular malformation in the upper right leg, right hip region, and pelvic region.
When she was 12 years of age, the girl reported pain and swelling of the right foot. Walking was increasingly difficult and she had to use a wheelchair on a regular basis. Her right leg was shorter and there was a valgus deformity of the right ankle. After extensive consultation and examination, the patient, her parents, and both the pediatric and orthopedic surgeons decided to perform a transtibial amputation which would ensure a good knee function and enough stump length for a good prosthetic fitting. In the immediate postoperative period after amputation, recurrent bleedings of the stump occurred. Corrective surgery resulted in a tibial length of the stump of 6 cm below the knee joint. The stump had a slightly protruding fibula and a short tibia. The mobility of the hip was not compromised, and the mobility of the right knee was 0-0-90°. Hyperpathy of the skin on the distal part of the stump was evident and gave problems with further stump formation and hardening of the tissues involved. After 3 months, the patient began to mobilize her right knee with the help of a physiotherapist. She learned to walk with two crutches and was independent in a wheelchair. She could stand and jump on the left leg without a walking aid. She had phantom pain and hyperpathy of the right transtibial stump.
Prosthetic prescription was discussed in the rehabilitation team. There were 3 concerns to be considered: (1) risk of re-bleeding in the stump by pressure of the socket on the VMs; (2) the short length of 6 cm of the transtibial stump after the re-operation; (3) stump pain and fear of weight bearing on the stump when walking again. The surgeons were very concerned about the risk of a re-bleeding and advised that distal weight bearing was not favorable for primary prosthetic construction.
An outpatient rehabilitation program was established to evaluate the prosthetic walking possibilities for the subject. After evaluation by the prosthetist and rehabilitation team, a two-step approach was decided. The first step was fabrication of an individually made silicone liner to gradually increase pressure on the stump. The second step was manufacturing of a well-fitting prosthesis in a more stilt-like position (fixed knee in extended position). The prosthetic design was made to off-load the stump by weight bearing through the ischial tuberosity, with a knee flexion of 30° to prevent full end weight bearing. (Figure 2)
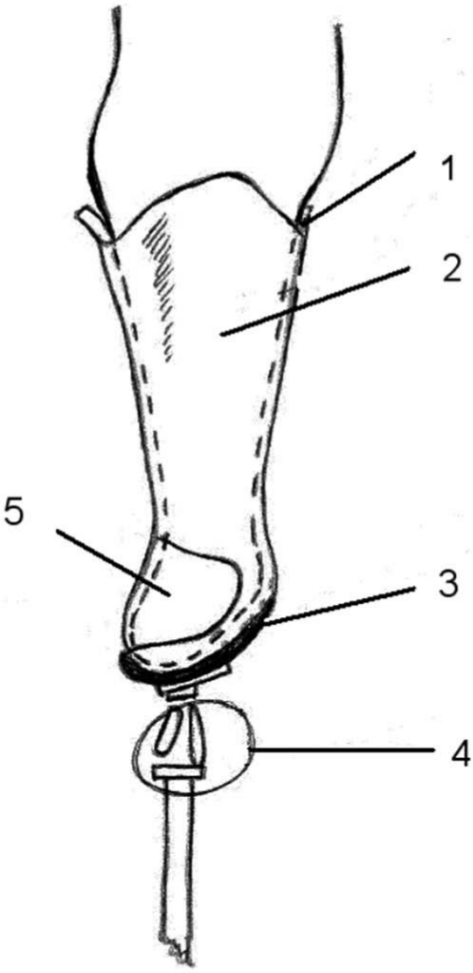
Picture of the lower limb prosthesis. (1) Liner, (2) resin socket, (3) memory foam, (4) fixed knee, and (5) opening for stump to pass through.
It was expected that the patient could be functioning at K4 level 7 (walking without mobility aids and with long endurance). She started with a multidisciplinary rehabilitation program and was treated by a physiotherapist, occupational therapist, social worker, and psychologist. She participated in different kinds of training, for example, walking training and training in the swimming pool.
During the rehabilitation period, the prosthetist made further adjustments to the prosthesis by a mechanical knee-locking-type mechanism and a conventional solid ankle cushion heel (SACH) foot 8 for weight distribution.
Findings and outcomes
The patient enrolled in an extensive training program with the first prosthesis made following the described prosthetic design. No complaints about stump pain, re-bleeding, or other complications were noted. After 5 months of outpatient rehabilitation program, she was able to walk with this prosthesis with a fixed mechanical knee without walking aids at home and outside using two crutches. She could ascend and descend a flight of stairs and was able to ride a bicycle.
One year after the end of the outpatient rehabilitation, the patient could walk well with the first prosthesis with a fixed mechanical knee. School performances were very good and she played wheelchair basketball. Due to limitations in sports and leisure activities, she asked about a new prosthesis with a free-moving prosthetic knee joint and ankle to enable easier walking and cycling. A new prosthesis was manufactured, designed for weight bearing through the ischial tuberosity, with a four-bar parallel titanium knee joint 8 with normal range of motion and a more mobile foot (Figure 3). The position of the flexed knee of the patient in the socket was as in the previous design that had proven good and safe in weight distributions. The Otto Bock dynamic Trias 8 prosthetic foot was chosen because it had more functional capabilities, for example, more flexibility in walking. During the training, no stump problems were observed.

Photo of the second lower limb prosthesis.
At the final follow-up 3 years later, the patient was able to walk without walking aids for more than 1 km with full weight bearing, but without full weight bearing on the end of the stump. With the second prosthesis, she could perform leisure and sporting activities. Because of the VM, repeated embolization of the blood vessels of the right leg and pelvis has been performed in order to decrease the risk of bleeding in the existing VMs.
Discussion
A normal fitting process for a regular PTB 6 prosthesis after transtibial amputation was not possible in this case because of severe vascular abnormalities in the stump. This was due to the VM and a stump length of 6 cm below the knee joint. The prosthetic fitting process was complicated. From an amputation level perspective a knee disarticulation could have been a solution, but in this case it was not possible because of the VM and the risk of extensive bleedings. Due to the short stump length and the non-distal weight bearing capacity of the stump, the knee joint of the patient could not be used during prosthetic walking. The first prosthesis design had a knee-locking mechanism and the second prosthesis design had a free-moving, parallel 4-axis knee joint. However, in this prosthetic design, the knee of the patient was in a flexed position of 30° to prevent full weight bearing of the stump, thereby minimizing the risk of bleeding.
In the literature, there are a few examples of prosthetic fitting after an amputation due to a severe VM. Umaran et al. 9 reported 4 cases with an amputation due to the complication of Klippel–Trenaunay Syndrome. The girl in this case report did not have the Klippel–Trenaunay Syndrome, but a VM. The Klippel–Trenaunay Syndrome has 3 major features: hemangioma, hypertrophy of soft tissue and bony overgrowth, and varicose veins. This syndrome is similar to VM. The problems in patients with Klippel–Trenaunay Syndrome are problems with weight transmission of the prostheses on the stump in areas of swelling, scarring of the skin and subcutaneous tissues, and continuous volume changes of the stump.10, 11
In this case report, the surgeon, prosthetist, and the rehabilitation team discussed different possibilities to make and fit an individually designed weight bearing prostheses for the patient. A prosthetic socket with full weight bearing was not possible due to the excessive forces on the end of the stump during walking. A PTB socket applies too much pressure in the pretibial area of the stump, and in this patient, the stump was too short for a good socket fitting. The two-step approach used was to increase weight bearing of the stump by a silicone liner. This worked well without any adverse reaction of the skin and underlying tissues. In order to prevent excessive pressure on the distal stump, a prosthesis design had to be developed with a proximal support. The socket design with the knee of the patient in a 30° flexed position helped to ensure good weight distribution. With this prosthesis, the patient enrolled in a multidisciplinary outpatient rehabilitation program. At the end of the rehabilitation program, the patient had a good functional level; she was able to walk without mobility aids for more than 1 km and could perform sporting activities without damage to her stump.
The problems found in this case can be generalized to other cases where full weight bearing of the stump is not possible; for example, the prosthetic design could be used in skin problems such as that found with skin transplantation.
Conclusion
In this article, the prosthetic solution is described for this rare case of severe VM deformity leading to a transtibial amputation. The fitting of a prosthesis without full weight bearing of the stump proved to be successful. After a 3-year period, the extensive use of the prosthesis was possible with good walking capacities and performing sporting and leisure activities. A multidisciplinary approach is necessary in these complex cases. Intensive consultation between the rehabilitation team, surgeon, and the prosthetist to solve the problems in such cases is advised.
Footnotes
Acknowledgements
The authors thank the patient and her parents for their kind permission to use the patient’s material.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.