
Abstract
Background:
Step counts, obtained via activity monitors, provide insight into activity level in the free-living environment. Accuracy assessments of activity monitors are limited among individuals with lower-limb amputations.
Objectives:
(1) To evaluate the step count accuracy of both monitors during forward-linear and complex walking and (2) compare monitor step counts in the free-living environment.
Study design:
Cross-sectional study.
Methods:
Adult prosthetic users with a unilateral transtibial amputation were equipped with StepWatch and FitBit One™. Participants completed an in-clinic evaluation to evaluate each monitor’s step count accuracy during forward linear and complex walking followed by a 7-day step count evaluation in the free-living environment.
Results:
Both monitors showed excellent accuracy during forward, linear walking (intraclass correlation coefficients = 0.97–0.99, 95% confidence interval = 0.93–0.99; percentage error = 4.3%–6.2%). During complex walking, percentage errors were higher (13.0%–15.5%), intraclass correlation coefficients were 0.88–0.90, and 95% confidence intervals were 0.69–0.96. In the free-living environment, the absolute percentage difference between monitor counts was 25.4%, but the counts had a nearly perfect linear relationship.
Conclusion:
Both monitors accurately counted steps during forward linear walking. StepWatch appears to be more accurate than FitBit during complex walking but a larger sample size may confirm these findings. FitBit consistently counted fewer steps than StepWatch during free-living walking.
Clinical relevance
The StepWatch and FitBit are acceptable tools for assessing forward, linear walking for individuals with transtibial amputation. Given the results’ consistenty in the free-living enviorment, both tools may ultimiately be able to be used to count steps in the real world, but more research is needed to confirm these findings.
Keywords
Background
Recent changes in the healthcare landscape are charging clinicians to objectively document patient functional status. Following a lower-limb amputation, a primary goal is to restore a patient’s walking function in order to minimize activity limitations and participation restrictions. Self-report measures of walking function are inherently subjective 1 and have poor correlation to direct, objective measures of function such as physical activity levels.2,3 Thus, the use of objective measures, such as step activity monitors, has been advocated. Activity monitors may be used to evaluate step counts in the free-living environment and provide insight into an individual’s activity level. 4 Activity level is a measure of functional status, 5 which is a key determinant in the ability of individuals with an amputation to live independently 6 and of overall health and quality-of-life. 7 Thus, accurately quantifying activity level may facilitate optimization of prosthesis prescription and, as a result, reduce activity limitations and participation restrictions.
Accelerometer-based activity monitors provide a quantitative tool for assessing step counts1,8 in the free-living environment. For individuals with lower-limb amputations, the StepWatch Activity Monitor (Modus Health LLC, Washington, DC) has historically been the most widely used monitor for research purposes. StepWatch provides minute-by-minute step count data and can be tuned to different walking styles. 9 StepWatch’s high cost, however, makes its use prohibitive for many clinicians.1,10 One newer monitor, FitBit One™ (Fitbit Inc., San Francisco, CA), is a lower cost option that provides easily accessible minute-by-minute step count data, thus potentially providing an affordable method to objectively assess walking function. While both monitors have been validated in other patient populations,10–15 step count accuracy assessments of these monitors are limited among individuals with lower-limb amputations. Thus, the purposes of this study were to (1) evaluate the step count accuracy of both monitors during forward, linear walking and complex walking and (2) compare step counts recorded by StepWatch and FitBit One during walking in the free-living environment. We hypothesized that both StepWatch and FitBit One would demonstrate acceptable accuracy during forward, linear walking, but step counts would be less accurate during complex walking. Secondarily, the study aimed to identify if self-selected gait speed and 6-min walk test distance influenced step counts recorded by the two monitors in the free-living environment. We hypothesized that step count differences between the monitors in the free-living environment would be higher for participants with a slower self-selected walking speed and shorter distance walked in 6 min, as slower walking speeds are known to contribute to step count inaccuracies in other patient populations.10,16,17
Methods
A total of 50 prosthetic users, aged 18–85 years, with a unilateral transtibial amputation were recruited for this Institutional Review Board for Human Subjects Research-approved study. Participants were recruited over a period of 9 months (September 2015–May 2016) through local prosthetic clinics, flyers posted at the university, and a local newspaper advertisement. Participants were excluded if they had amputations of their sound limb (i.e. bilateral amputation), current issues with their residual limb that limited their walking ability, weight-bearing restrictions, or health conditions that precluded their safe completion of this study, such as unstable blood pressure.
Procedures
After completing the informed consent process, individuals participated in a standardized evaluation by a licensed physical therapist. The 10-m walk test (10MWT), in which participants walked along a 10-m straight pathway with time recorded during the middle 6 m to allow for acceleration and deceleration,18,19 was used to assess self-selected walking speed. Three trials were taken and averaged to determine each participant’s self-selected walking speed. When a second trained examiner was available and time allowed, participants completed a four-square step test 20 (FSST) immediately followed by a figure-of-eight walk test 21 (F8WT) to evaluate step count accuracy of the monitors during complex walking. Participants completed two FSST trials, walked over to the F8WT course, and then completed the F8WT, with steps counted during the entire testing series. Finally, the majority of participants completed a 6-min walk test (6MWT), a test of cardiovascular fitness, 22 to evaluate step count accuracy of the monitors during forward, linear walking. Participants were instructed to walk as quickly, but safely, as possible, covering as much ground as possible in 6 min. The examiner refrained from conversation with the participant to encourage a maximal effort and walked slightly behind the participant to avoid pacing. Participants were provided standard encouragement at each minute.
During the FSST/F8WT and 6MWT, participants were equipped with a StepWatch and FitBit One, both secured about the distal aspect of their prosthetic pylon using straps provided with each monitor (Figure 1). Monitors were placed on the prosthesis to optimize wear compliance, which has been an issue in prior studies during free-living portion of the study. Prior to testing, StepWatch was set up for each participant as per manufacturer instructions. Upon completion of both FSST/F8WT and 6MWT, the steps recorded by StepWatch were extracted and recorded and the monitor was reset. For FitBit, initial and final step counts were recorded prior to and immediately upon completion of FSST/F8WT and 6MWT. In addition, an investigator, blinded to monitor step counts, manually counted and recorded the steps taken during each test.

Picture of sample placement of activity monitors on prosthesis. Activity monitors were placed about the distal aspect of their prosthetic pylon using straps provided with each monitor. Depending on the design of the prosthesis and whether a cover was worn, FitBit was either placed directly above StepWatch (left) or directly on top of StepWatch (right).
Following the standardized evaluation, participants were sent home with the activity monitors for a 7-day observation period, which began the day after the in-clinic evaluation. Participants were instructed to perform their regular daily activities, wearing the monitors at all times they were wearing their prosthesis. Participants were instructed on how to properly place the monitors on their prosthesis, but they were encouraged to leave the monitors on their prosthesis for the duration of the study (checking monitor placement daily) to optimize compliance with wearing the monitors. Participants were also provided with a daily activity log to record the time they donned and doffed the monitors. Participants were instructed to mail the monitors and daily activity logs back after the 7-day observation period using a prepaid addressed envelope that was provided.
Data analysis
Since StepWatch counts strides while FitBit counts steps, for all analyses the number of strides counted by StepWatch was multiplied by two so that monitor counts were comparable. For the in-clinic accuracy assessments, the absolute percentage errors in steps counted by StepWatch and FitBit relative to the manual step counts during the 6MWT (forward, linear walking) and FSST/F8WT (complex walking) were calculated (equation 1). In addition, for each monitor and each test, an intraclass correlation coefficient (ICC (2,1)) with a 95% confidence interval was used to statistically evaluate the step count accuracy of each monitor compared to manual step counts. Finally, the Bland–Altman method with 95% confidence interval was used to investigate absolute reliability between the monitor-determined and manual step counts

For the step count assessment in the free-living environment, once the monitors were returned, daily step counts for each day were determined for each monitor. Step counts were extracted directly from StepWatch. Fitabase, a cloud-based data aggregation platform, was used to extract FitBit step counts. Data were inspected for inconsistencies between monitor-recorded activity (including activity-bout inconsistencies between the two monitors) and participant activity logs. If inconsistencies could not be explained, data were considered invalid, likely due to device failure, and were excluded from analysis. In addition, participants’ data were excluded from analysis if there were fewer than 5 days of valid data recorded for both monitors.
For each monitor, daily step counts were summed across days to determine each participant’s total step count during the observation period. The absolute percentage difference in free-living total step counts between StepWatch and FitBit was calculated (equation (2)). To determine if the free-living step counts recorded by the two monitors were associated, a regression analysis was conducted on the two monitors’ total step counts for each participant. Finally, to identify factors contributing to greater percentage differences between monitors, Pearson’s correlations were used to evaluate the relationship between the absolute percentage difference and the 10MWT self-selected speed and 6MWT distance
Results
In total, 68 participants were screened for eligibility. Five of these participants were ineligible as they did not meet the inclusion/exclusion criteria. Thus, 63 participants were scheduled for the in-clinic evaluation. Thirteen of these participants never received the evaluation due to the following reasons: no show and unable to be reached for rescheduling (n = 5), canceled appointment as no longer interested (n = 2), family circumstances precluding participation (n = 2), and scheduling conflict (n = 4). Thus, 50 participants were enrolled in the study. Step count data from 31 and 27 participants were analyzed for the forward, linear walking test, while data from 17 and 16 participants were analyzed for the complex walking test for StepWatch and FitBit, respectively. Data of 42 participants were analyzed for the free-living step count assessment of FitBit compared to StepWatch—37 participants had 7 days of free-living data, 4 participants had 6 days of data, and 1 participant had 5 days of data. Details regarding the number of participants and reasons for data loss for each analysis are provided in Table 1. Participant demographics for each analysis are provided in Table 2.
Participant numbers for each analysis.
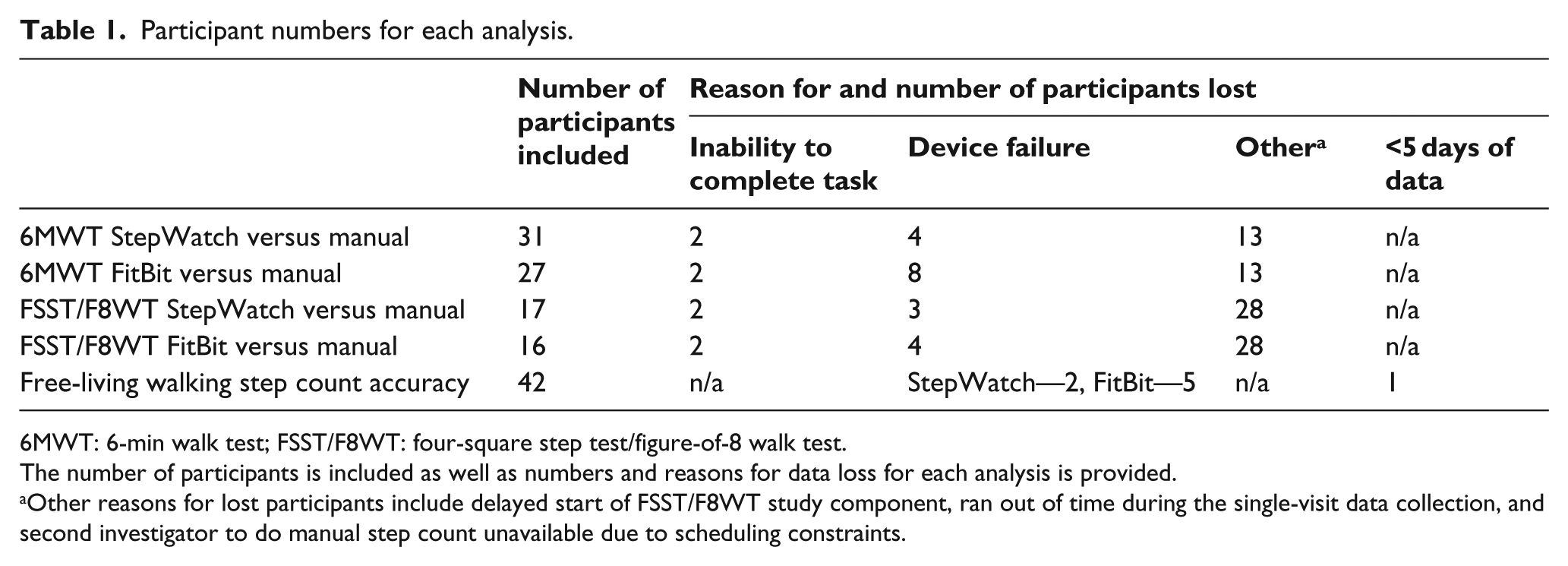
6MWT: 6-min walk test; FSST/F8WT: four-square step test/figure-of-8 walk test.
The number of participants is included as well as numbers and reasons for data loss for each analysis is provided.
Other reasons for lost participants include delayed start of FSST/F8WT study component, ran out of time during the single-visit data collection, and second investigator to do manual step count unavailable due to scheduling constraints.
Participant demographics.
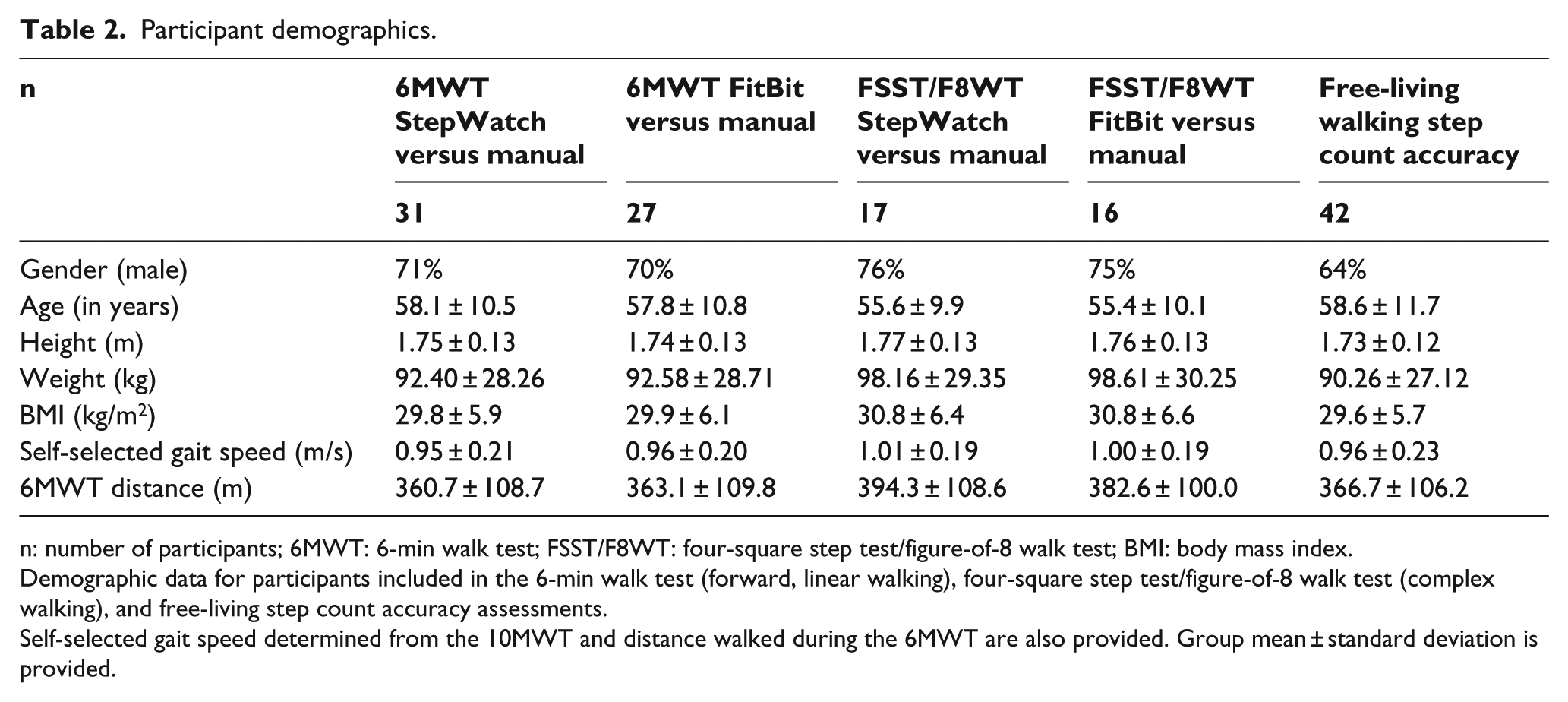
n: number of participants; 6MWT: 6-min walk test; FSST/F8WT: four-square step test/figure-of-8 walk test; BMI: body mass index.
Demographic data for participants included in the 6-min walk test (forward, linear walking), four-square step test/figure-of-8 walk test (complex walking), and free-living step count accuracy assessments.
Self-selected gait speed determined from the 10MWT and distance walked during the 6MWT are also provided. Group mean ± standard deviation is provided.
Both monitors showed excellent accuracy during forward, linear walking when considering both percentage errors and ICCs (Table 3). Inspection of Bland–Altman plots indicated an undercount mean bias for both StepWatch and FitBit, partially caused by outliers, but step count accuracies remained consistent relative to the manual count over the step count range (Figure 2). During complex walking, average absolute percentage errors were greater when compared to data from the forward, linear walking (Table 3). In addition, while ICCs between monitor and manual step counts were good for complex walking, confidence intervals were larger than those for forward, linear walking (Table 3). Bland–Altman plots support these findings, as the step count accuracy data for both monitors during the FSST/F8WT were more widely scattered with a wider 95% confidence interval, indicating the monitors were not as accurate in counting steps during complex walking tasks (Figure 2).
In-clinic step count accuracy data.
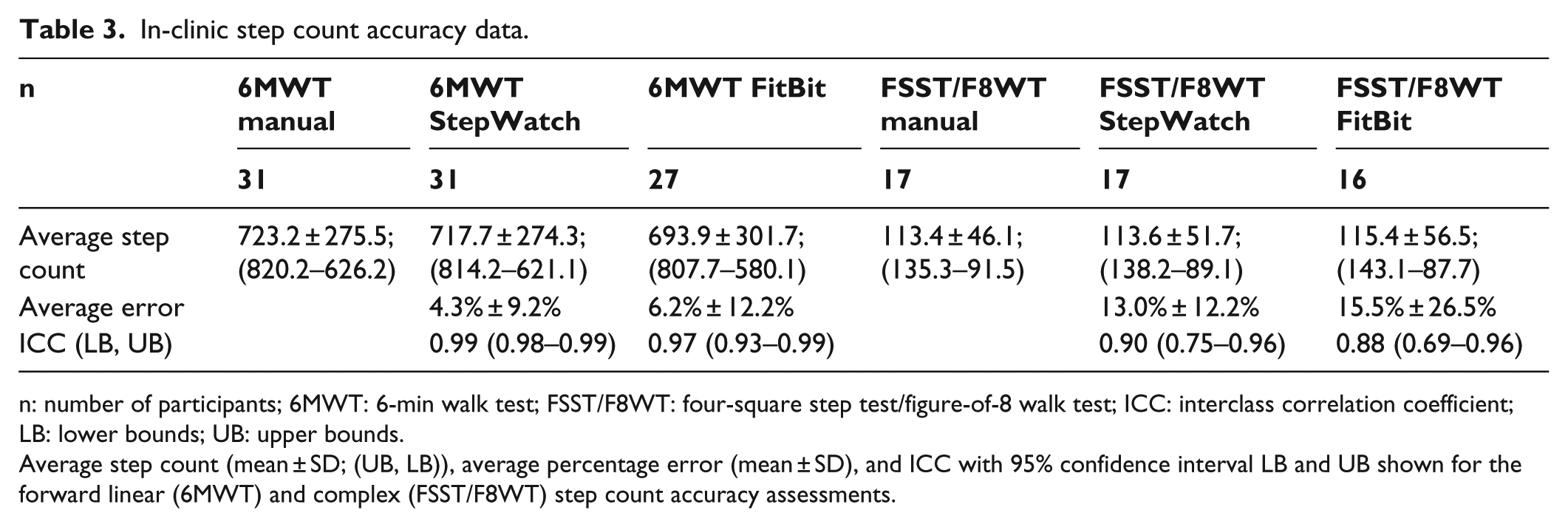
n: number of participants; 6MWT: 6-min walk test; FSST/F8WT: four-square step test/figure-of-8 walk test; ICC: interclass correlation coefficient; LB: lower bounds; UB: upper bounds.
Average step count (mean ± SD; (UB, LB)), average percentage error (mean ± SD), and ICC with 95% confidence interval LB and UB shown for the forward linear (6MWT) and complex (FSST/F8WT) step count accuracy assessments.
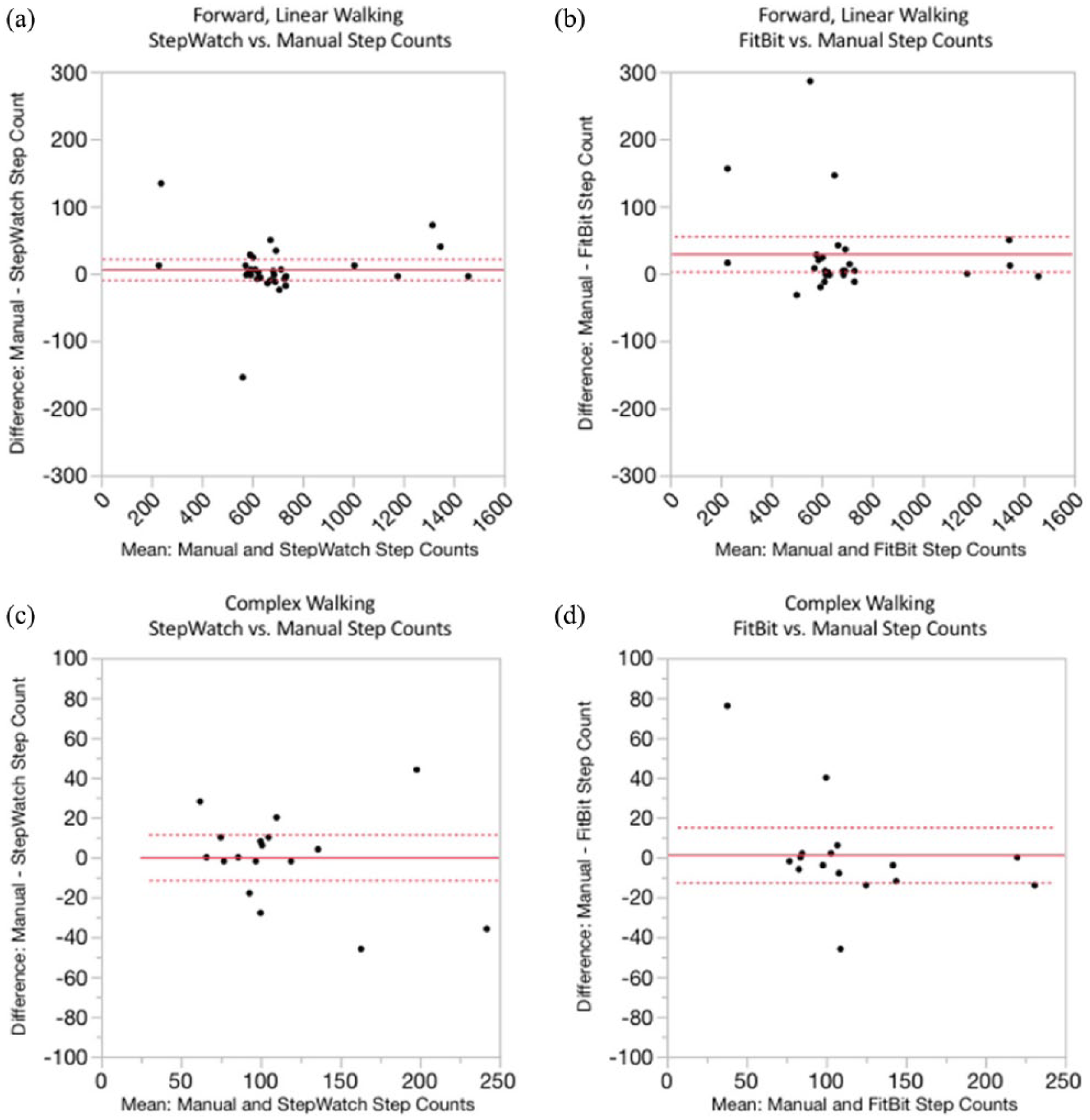
Bland–Altman plots for in-clinic step count accuracy data: (a) StepWatch versus manual step counts during forward, linear walking; (b) FitBit versus manual step counts during forward, linear walking; (c) StepWatch versus manual step counts during complex walking; (d) FitBit versus manual step counts during complex walking.
During free-living walking, StepWatch and FitBit counted between 869 steps and 102,392 total steps during the observation period. FitBit tended to count fewer steps than StepWatch, with FitBit only counting more steps than StepWatch for 7 of the 42 participants. The absolute percentage difference between the two monitor step counts was 25.3% ± 28.6%. This absolute percentage difference had a moderately strong correlation to both the 10MWT self-selected speed (r = 0.59; p < 0.0001) and distance walked during 6MWT (r = 0.53; p = 0.005; Figure 3), with percentage differences decreasing with increased self-selected walking speed and distance walked. Regression analysis revealed monitor step counts had a nearly perfect linear relationship (Figure 4), with StepWatch consistently counting an almost fixed number of additional steps (fixed upward bias) over FitBit (StepWatch step count = 1.06 × FitBit step count + 3573.7 steps, R2 = 0.96).
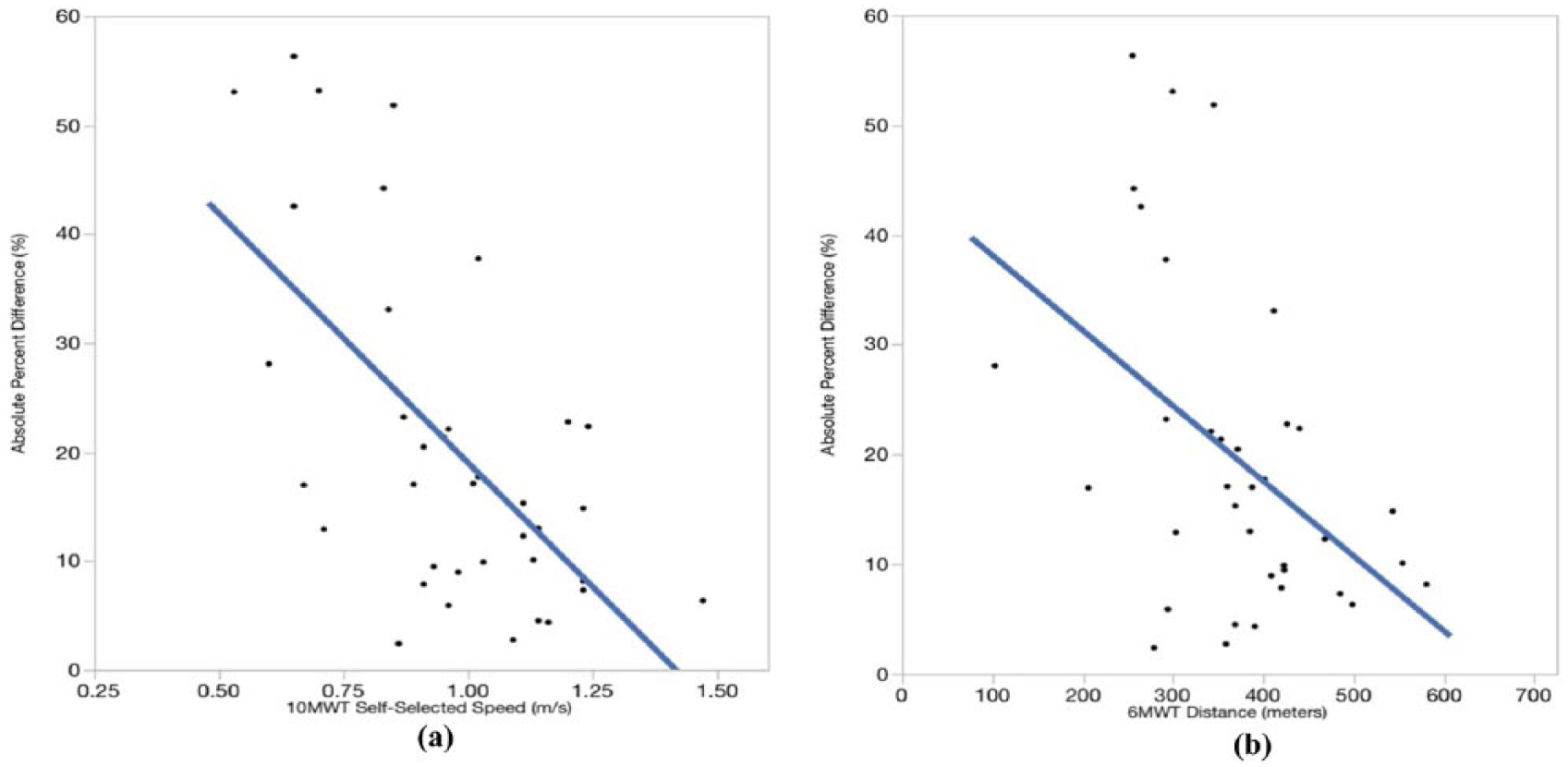
Scatterplots of the absolute percentage difference in step counts recorded by the two monitors in the free-living environment: (a) 10-m walk test self-selected speed and (b) distance walked during 6-m walk test.
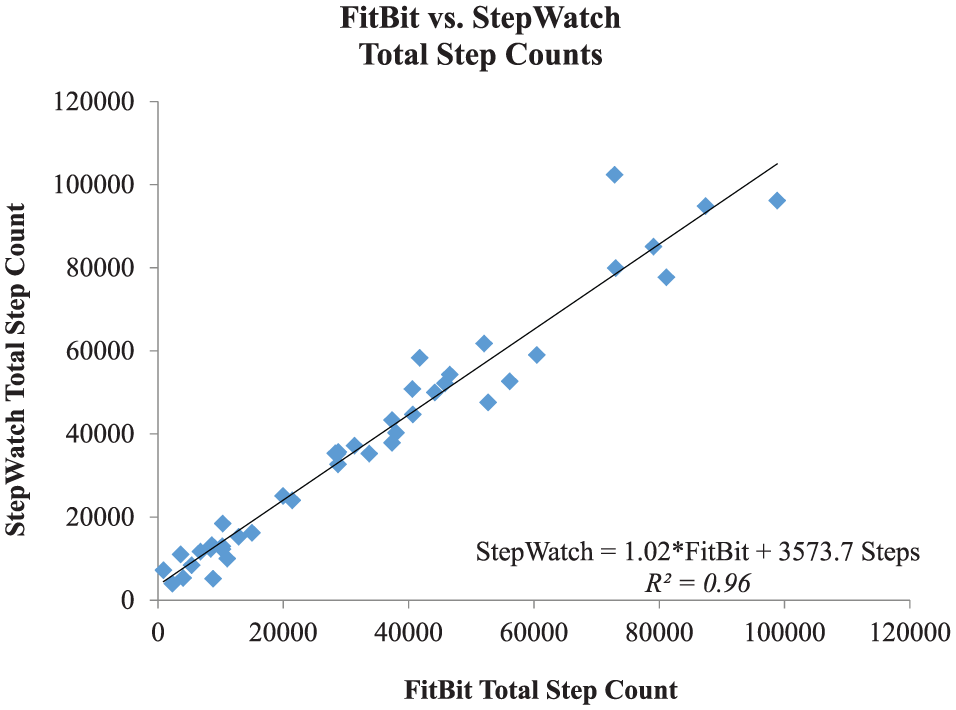
StepWatch versus FitBit average daily step counts during free-living walking. Regression line with equation shown.
Discussion
This study is among the first to evaluate the step count accuracy of StepWatch and FitBit One among individuals with a lower-limb amputation who use a prosthetic device, specifically those with a unilateral transtibial amputation. Results showed that both the monitors accurately counted steps during forward, linear walking in a clinical setting, with high ICCs compared to manual step counts and percentage errors well below the 10% accuracy threshold considered clinically acceptable for similar monitors. 23 During complex walking, StepWatch appeared to outperform FitBit, although percentage errors for both the monitors exceeded the 10% threshold. Step count discrepancies between the two monitors during free-living were high, yet these counts were strongly linearly associated. Furthermore, greater differences between the monitors’ free-living step counts were correlated to a slower self-selected walking speed and a shorter distance walked in 6 min. These findings provide important, novel information regarding the strengths and limitations of using StepWatch and FitBit One to objectively assess walking function among individuals with lower-limb loss.
Our results regarding the monitor’s step count accuracy for forward, linear walking align with and add to prior research. Step count percentage errors in our study (4%–6.5%) were comparable to errors reported by previous investigators (1%–10%) who used the Ossur Patient Activity Monitor accelerometer to assess step counts among individuals with lower-limb amputations.24,25 Other studies have evaluated accuracy of StepWatch and FitBit in adults with lower-limb amputations, but these studies used very small sample sizes (5–9 participants) and accuracy assessments were conducted over short activity bouts (as little as 1 min).9,26 In contrast, our study evaluated the step count accuracy of two monitors on a large sample of individuals with unilateral transtibial amputations for longer periods.
Similar to our findings, prior investigations of other populations found step count accuracies of accelerometer-based monitors to be lower during complex walking tasks compared to forward walking.17,27 Specifically, Hickey et al. 17 evaluated accuracy during side-to-side and multidirectional stepping tasks with StepWatch among healthy adults (n = 15) and found errors ranging from 10%–14%, which is similar to the measurement error found in our study (13% ± 12%). Dudek 27 reported higher percentage errors (~30% ± 10%) among 20 individuals with transtibial amputations, although that study evaluated complex walking via a simulated household environment and used a different activity monitor (Ossur Patient Activity Monitor). While the greater percentage errors and lower ICCs seen during complex walking (compared to forward walking) in our study align with results from prior studies, greater errors and lower ICCs may be a product of sample size or data variability (per Bland–Altman plots). Future research on complex walking with a larger sample may delineate between decreased accuracy secondary to insufficient sampling versus innate heterogeneity of complex walking data.
While the percentage difference between steps counted by StepWatch and FitBit in the free-living environment was high, monitor step counts were strongly, linearly related (regression line slope close to 1.0). FitBit counted an almost consistent number of fewer steps compared to StepWatch. This finding suggests there is a systematic difference in counting steps in the free-living environment between the two monitors. Future research could investigate sources of this difference. For example, the algorithm to identify a step may differ between monitors (StepWatch records on the heel rise, FitBit’s algorithm is proprietary), which could influence the step count accuracy in this population. If the discrepancies are indeed confirmed to be systematic errors, clinicians may ultimately be able to use FitBit as an alternative to StepWatch using an equation to adjust for known error. Moreover, factors identified in this study could be potential sources that could explain the discrepancies in free-living step counts between the monitors. First, differences may be attributed to errors in counting steps during complex walking patterns encountered in the free-living environment. While results from this study suggested that this may be a potential source of error, we were unable to establish which specific complex walking pattern (i.e. backwards, side-stepping, or curvilinear trajectory) caused the greatest errors as FSST/F8WT included a range of patterns. Future research may seek to identify which complex walking pattern results in the highest step count errors for each monitor. In addition, the activity duration could have influenced the results. Accuracy of the monitors during long-duration walking was investigated with 6MWT, while short-duration bouts of walking may be more common in the free-living environment. Future studies should investigate if the step count accuracy of either monitor differs for long and short bouts of activity. Furthermore, as self-selected walking speed and distance walked during the 6MWT (which is dependent, in part, on gait speed) were both correlated to the percentage difference in free-living step counts between monitors, these factors could have contributed to the free-living step count discrepancies. Slower walking speeds are a known source of error for many accelerometer-based monitors in other populations including healthy adults16,17 and individuals post-stroke or post-traumatic brain injury. 10 Results from this study concur with the published literature as differences in monitor step counts increased with decreases in participants’ self-selected walking speeds. Thus, future studies should consider gait speed when investigating discrepancies between monitor counts in individuals with a unilateral transtibial amputation. Finally, additional factors not evaluated in this study, including the type of environment in which the participant ambulated (city vs suburban/more rural living, job requirements, etc.), participant’s motivation to ambulate, and barriers/access to environment that promote increased activity, could have contributed to the step count discrepancies seen in the free-living environment. These types of factors should be investigated in the future to determine if they contributed to step count discrepancies in the free-living environment.
Study limitations
Our study recruited a homogeneous sample of adults with a unilateral transtibial amputation; therefore, future work is needed to evaluate the generalizability of these findings to those with bilateral amputations and/or varying amputation levels. We did not recruit a group of healthy individuals for comparison, which could have enhanced our understanding of monitor discrepancies, that is, whether discrepancies are inherent to the monitors or due to population-specific factors. Furthermore, our results may only be generalizable to patients walking on average 0.95 ± 0.20 m/s or more. While we evaluated both linear, forward walking and complex walking, the tests were not videotaped and, instead, manual step counts were determined in real time. While other published studies have also manually counted steps,11–14,28,29 videotaping would have allowed the manual step counts to be double-checked. That said, investigators conducting the manual step counts in this study were trained to minimize inter-examiner variability and counters were blinded to monitor recordings. In addition, while the manufacturer recommends placing FitBit One at the waist or chest/bra strap, published research studies demonstrate that ankle placement was comparable to, or even more accurate than, waist/chest placement.30–32 Thus, FitBit One was placed at the ankle for this study. Results may differ if the monitor is placed in a different location. While participants were instructed on monitor placement and asked to leave the monitors in place, potential migration of the monitors or improper placement over the 7-day observation period may have influenced results. We acknowledge that the sample size for the complex walking accuracy assessment was smaller than desired, given 95% confidence intervals and data variability. Nonetheless, our results provide novel, preliminary data regarding the accuracy of StepWatch and FitBit One during complex walking for individuals with unilateral transtibial amputations and support further research of step count accuracy during complex walking in this patient population.
Conclusion
Providing a clinical tool that providers can routinely use to objectively assess a patient’s walking function in the free-living environment may help optimize prosthetic prescription, reducing activity limitations and participation restrictions for these patients. Results from this study suggest that StepWatch may be ideal for determining physical activity, as assessed with step counts, among adults with transtibial amputations. FitBit, which appears to under-count steps, but is less costly, may be used to estimate activity level in the free-living environment since there appears to be a consistent offset in FitBit’s step counts relative to StepWatch. Yet, further research evaluating step count accuracy of both monitors during complex walking tasks is needed before definitive conclusions are made regarding either monitor’s accuracy during free-living walking. It is promising, though, that results from this study suggesting inaccuracies for a given monitor appear to be consistent. Thus, even if inaccuracies in counting steps during complex walking patterns persist for both monitors, if the inaccuracies are consistent these inaccuracies can be accounted for when evaluating a patient’s free-living step counts.
Footnotes
Acknowledgements
The authors would like to thank Independence Prosthetics-Orthotics, Inc., Dankmeyer, Inc., and Real Life Prosthetics, LLC for assistance with recruiting participants for this study.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Sions is an independent consultant for Independence Prosthetics-Orthotics, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through funds from the Orthotics and Prosthetics Education and Research Foundation, Inc. (OPERF) under grant number 15A01561. The work was also funded, in part, by the Unidel Foundation, Inc. and an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under grant number U54-GM104941 (PI: Binder-Macleod).