
Abstract
The objectives of this study were to evaluate the clinical features and outcomes of 43 bilateral lower limb amputees. The clinical features obtained included the causes of amputation, level of amputation, concurrent medical problems, and stump condition. Outcome measures were obtained using the activities of daily living (ADL) index, the Frenchay Activities Index (FAI), and mobility grading with prostheses or wheelchair. Of 33 amputees who were prosthetic ambulators, 22 (67%), mainly bilateral trans-tibial (TT) amputees, were community ambulators, and participated in activities which included stair-walking, and six of 11 household ambulators were combination trans-femoral (TF) and TT amputees. Of 10 amputees who were wheelchair ambulators, only one was able to perform wheelchair transfers independently and five were independent wheelchair ambulators. Using the ADL index and FAI, there was no significant difference in scores according to the level of amputation (p > 0.05), but the scores of community prosthetic ambulators were significantly higher than those of wheelchair ambulators (p < 0.05). Age was found to be negatively correlated with ADL index and FAI scores (r = −0.518 vs. r = −0.550) (p < 0.01). This study concludes that overall independence in ADL after bilateral lower limb amputation improved with young age and prosthetic mobility.
Introduction
Bilateral lower limb amputations are currently being performed much more frequently than in the past, largely as a result of an aging population with an increased incidence of peripheral vascular disease and diabetes mellitus (Bowker and Michael 1992). Throughout the industrialized world, improved medical management has continually increased the life expectancy of the population. As people live longer, the complications of diabetes, peripheral vascular disease, and other chronic diseases progressively increase the frequency of lower limb loss. Since these disease states are systemic, previous studies (Bodily and Burgess 1983; Ebskov and Josephsen 1980; Keragy et al. 1986) have shown that approximately 33 – 50% of surviving patients can be expected to lose their second limb within the 2 – 3 years following the first amputation. The number of bilateral lower limb amputees has also increased as a result of trauma and congenital limb deficiencies (Bowker and Michael 1992). Rehabilitation of bilateral lower limb amputees poses a considerable challenge to both the rehabilitation team and the amputees themselves (Datta et al. 1992).
In general, the prosthetic usage status is assessed in terms of the evaluation of the functional status of lower limb amputees (Kim et al. 1999). A few guidelines are used to determine the feasibility of prosthetic ambulation following major lower limb amputation, but it is difficult to determine precise ambulatory function. Successful prosthetic ambulation has been defined as prosthetic usage for ambulation on a daily basis with or without external support (Moore et al. 1989). However, various results have been reported regarding prosthetic usage status in bilateral lower limb amputees; differing results may be influenced by the selection criteria of subjects, the interval of follow-up, and the definition of successful prosthetic ambulation used in each study (Pernot et al. 1997; Traballesi et al. 1998). Moore et al. (1989) reported that 19% of bilateral lower limb amputees achieved functional prosthetic ambulation and, in their experience, the presence of dysvascular disease and preservation of at least one knee joint were important predictors for a successful rehabilitative outcome. Volpicelli et al. (1983) demonstrated that 5.3% of functional prosthetic ambulators were bilateral trans-femoral (TF) amputees, 23.8% were combination TF and trans-tibial (TT) amputees, and 79.5% were bilateral TT amputees. Of 105 patients with bilateral amputation as a result of severe ischemia, only 26% were able to use bilateral prosthesis, but 74% were independent in their activities, as reported by Evans et al. (1987). As mentioned above, there have been several reports about the clinical features of bilateral lower limb amputees in the United States.
Datta et al. (1992) reported that 38 of the 41 (92.2%) bilateral amputees, for which dysvascular disease was the primary cause of amputation in 90.2% of the group, had been prosthetically rehabilitated after the loss of their second limb. The majority of bilateral TT amputees continued to do well in terms of their prosthetic mobility, and prosthesis users were more independent in their activities of daily living in the United Kingdom. However, according to reports in The Netherlands and Israel, the prosthetic usage statuses were 10 – 20% in bilateral lower limb amputees, and it tended that less prosthesis usage was observed when follow-up intervals were lengthened (De Fetes et al. 1994; Wolf et al. 1989).
Unfortunately, no reports exist regarding the clinical features and the support of activities of living and prosthetic usage in Korean bilateral lower limb amputees. Also, the majority of previous papers concentrated mainly on prosthetic use and mobility of bilateral amputees, and the criteria used for outcome measures tended to be vague and varied (Datta et al. 1992).
Therefore, the objective of this study is to investigate the outcome in terms of independence in activities of daily living (ADL) and social integration, as well as ambulatory status; we also hoped to evaluate other variables, including the age, level of amputation, etiology, presence of concurrent disease, and prosthetic or wheelchair usage status, and to examine the aspects that differentiate Korean bilateral lower limb amputees from those of other countries.
Methods
Subjects
A retrospective study has been carried out on amputees who had received bilateral lower limb amputation, and went through the process of prosthetic prescription, fitting, and training at the Rehabilitation Hospital, Yonsei Medical Center, from January 1994 to December 2003, a span of 10 years. This study did not include those who had only the toes or feet amputated.
All 61 bilateral lower limb amputees were sampled and a letter of request to join the survey and self-administered questionnaire sheets were mailed to the sampled amputees, followed up by a second mailing to amputees who had not responded after 3 weeks. If the mailed questionnaires contained a missing value or were not returned, the amputees were contacted by telephone. Direct contact was made if the amputees so wanted. Some 43 bilateral lower limb amputees agreed to join the survey: 12 did not respond, and 6 had died at the time of review. Thirty-two of these amputees were male and 11 were female; age at the time of follow-up ranged from 15 – 76 years (mean age 44.7 years).
Data collection
A self-administered mail questionnaire, and its telephone version, were designed to evaluate the factors related to past medical history, causes and level of amputation, ambulatory status, stump condition, status of prosthetic or wheelchair usage, degree of independence in ADL, and social function.
The causes of amputation were classified according to the primary cause only. The large categories of causes of amputation were classified into trauma, dysvascular disease, infection, malignancy, and congenital anomaly. The category of trauma included amputation caused by machinery, industrial injury, traffic accidents, explosions, train accidents, and burn injuries. The category of dysvascular disease included diabetes, arteriosclerosis, ischemic disease, Buerger's disease, and frostbite.
The amputees were separated into three groups: bilateral trans-femoral (TF), bilateral trans-tibial (TT), and combination TF and TT amputees (Volpicelli et al. 1983). The disarticulation of knee and Syme were included in the TF and TT categories because of the similarities of their function (Han et al. 2004).
The ambulatory status of each amputee was recorded using a modification of a grading system described by Volpicelli et al. (1983), consisting of classifications such as community prosthetic ambulators who could walk at least 100 yards or at least one block with prostheses, household prosthetic ambulators, and wheelchair ambulators.
Prosthesis or wheelchair usage status was evaluated according to the ambulatory status of each amputee (Grise et al. 1993). In prosthesis users, factors related to prosthetic use were locomotory abilities with the prosthesis, such as ability to don/doff the prosthesis, standing up, walking ability (indoors, outdoors), stair walking, and need for external support. In wheelchair users, the transfer and propelling activities in a wheelchair were evaluated.
The degree of independence in ADL was recorded using a simple scoring system devised by Datta et al. (1992). As a method of measuring general activities (i.e., other than personal care) and social function, he authors used the Frenchay Activities index (FAI) described by Wade et al. (1985), which measures activities such as preparing main meals, washing up, washing clothes, light/heavy housework, local shopping, social activities, walking outside for more than15 min, active pursuit of hobbies, and driving car/bus travel in the last 3 months, as well as travel outings/car rides, gardening, household/car maintenance, reading books, and gainful work in the last 6 months.
Data analysis
The data was analysed using the SPSS 11.0 software program for Windows (SPSS Inc, Chicago, IL). Kruskal Wallis one-way ANOVA test by ranks test (K-W ANOVA) was carried out to compare the differences among the three groups according to the level of amputation or ambulatory status with regard to the ADL index and FAI. Mann-Whitney U-test was used to analyse the differences between two groups according to the dependency on walking aids, etiology, and sex with regard to the ADL index and FAI. The correlation between ADL index or FAI and age was made by coefficients of correlation. A p-value less than 0.05 was regarded as being statistically significant.
Results
Descriptions of subjects (Table I)
General characteristics of subjects (n = 43).
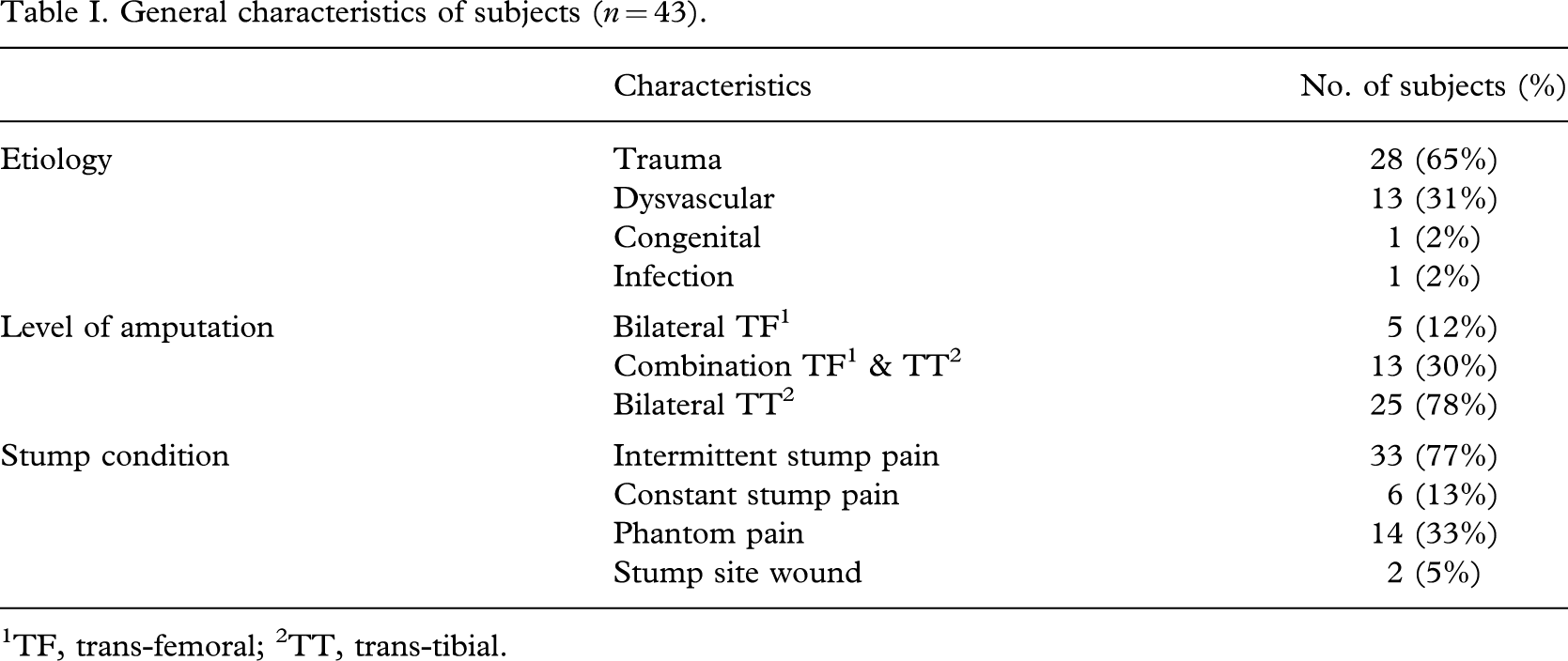
1TF, trans-femoral; 2TT, trans-tibial.
All 43 bilateral lower limb amputees were divided into three groups according to the level of amputation; 5 patients (12%) were bilateral trans-femoral (TF), 25 (58%) were bilateral trans-tibial (TT), and 13 (30%) were combination TF and TT amputees. The amputation level of 1 of the 13 combination TF and TT amputees was changed from bilateral TT.
Trauma was the most common cause of amputation, accounting for 65% of all subjects. The next most common cause of amputation was dysvascular disease (30%).
Twenty subjects were admitted for prosthetic training at the Rehabilitation Hospital, 4 of whom were not using prostheses due to the recent development of cerebral infarction, glaucoma, deep vein thrombosis, or change of amputation level. The main reason for 6 subjects not being fitted with prostheses were problems with concurrent diseases, their general conditions, and poor wound healing.
Of all 43 patients, 39 amputees had stump pain and 14 amputees complained of phantom pain.
Mobility with prostheses or wheelchair
Thirty-three of 43 bilateral lower limb amputees were ambulators with prostheses; 11 ambulated at the household level and 22 ambulated at the community level, including walking up and down stairs. Of 22 amputees who were community ambulators, 18 subjects were bilateral TT amputees; 6 of 11 household ambulators were combination TF and TT amputees (Table II).
Ambulation status according to the level of amputation.
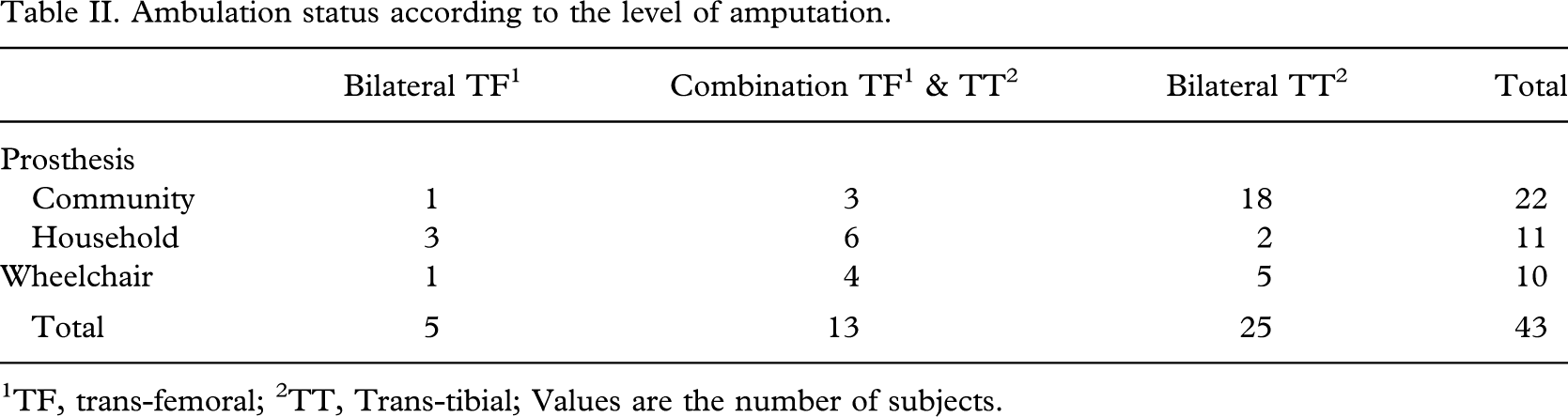
1TF, trans-femoral;
2TT, Trans-tibial; Values are the number of subjects.
The donning and doffing of prostheses were performed independently by 29 subjects. Twenty-one subjects were wearing their prostheses daily; the number of hours prostheses were worn ranged from 3 – 12 h per day. The average interval between the last amputation and the fitting of prostheses was 31.5 months, and 21 of 33 prosthetic ambulators walked without the use of walking aids, 6 used one monocane, and 3 used two monocanes. The other 3 walked with quadcanes or crutches (Table III).
Prostheses users (n = 33).
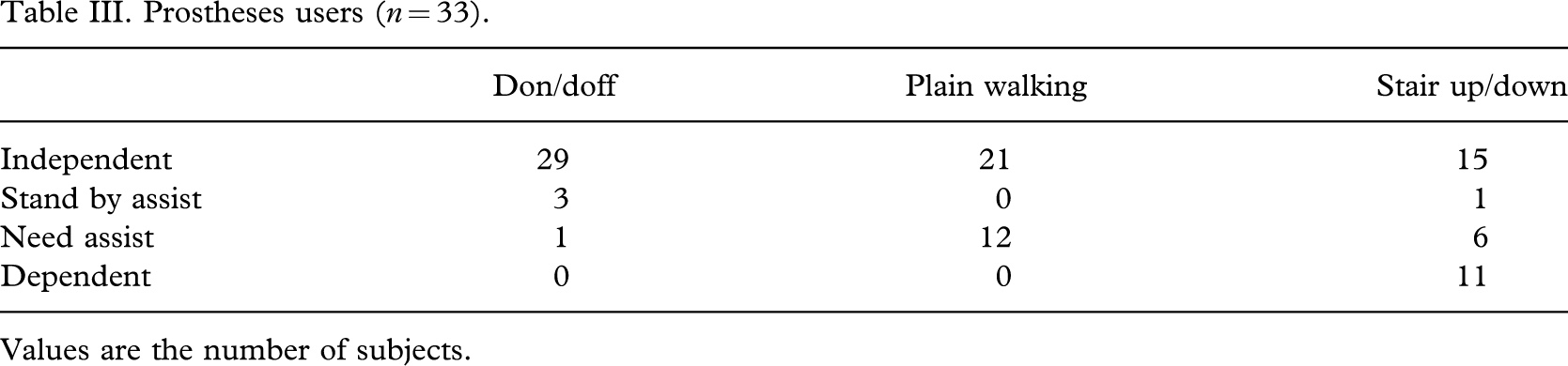
Values are the number of subjects.
Ten of 43 bilateral lower limb amputees were wheelchair ambulators; all 10 wheelchair ambulators were dysvascular amputees. Six subjects were not fitted with prostheses and 4 were not using prostheses due to problems with concurrent diseases, their general conditions, and poor wound healing.
Only 1 of 10 wheelchair ambulators was able to perform transfer activities by himself, and 5 were able to propel their wheelchairs independently at the outdoor level (Table IV).
Wheelchair users (n = 10).
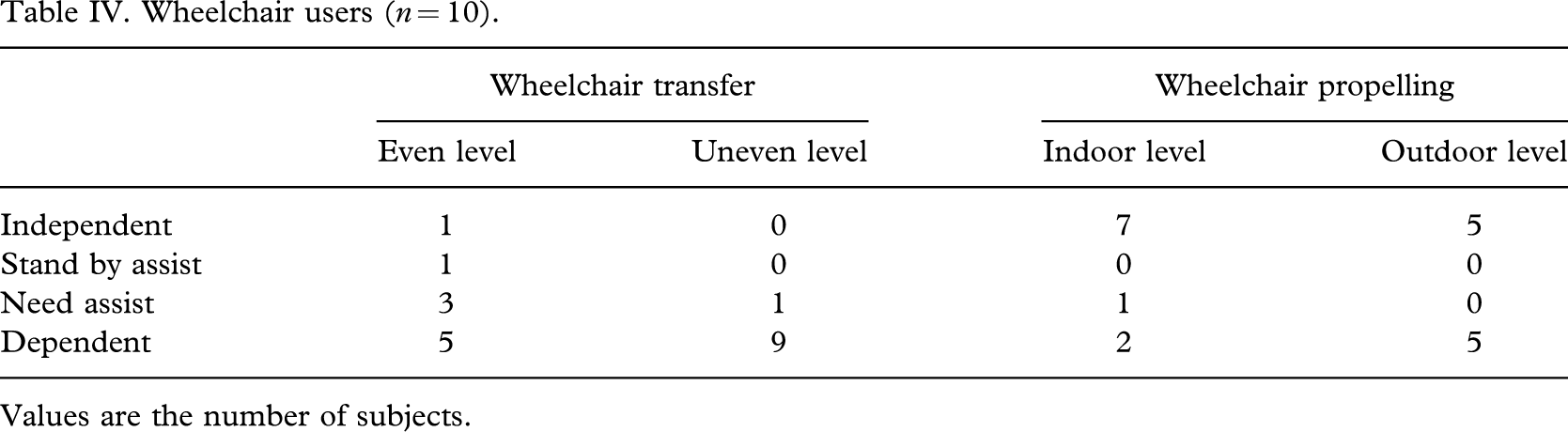
Values are the number of subjects.
Activities of daily living
Assessments of the Frenchay Activities Index (FAI) and the activities of daily living (ADL) index were performed on all 43 subjects. The average score for the ADL index was 31.6, and for FAI, it was 17.3.
As a whole, there did not appear to be any significant difference in the ADL index or FAI between the levels of amputation. However, there were significantly higher scores for community prosthetic ambulators compared with those of wheelchair ambulators (p < 0.05) (Table V). Prosthetic ambulators without walking aids and non-vascular amputees got significantly higher scores in both the ADL index and FAI compared with prosthetic ambulators with walking aids and dyvascular amputees (p < 0.05) (Table VI).
ADL1 index and FAI2 according to the level of ambulation and ambulation status.
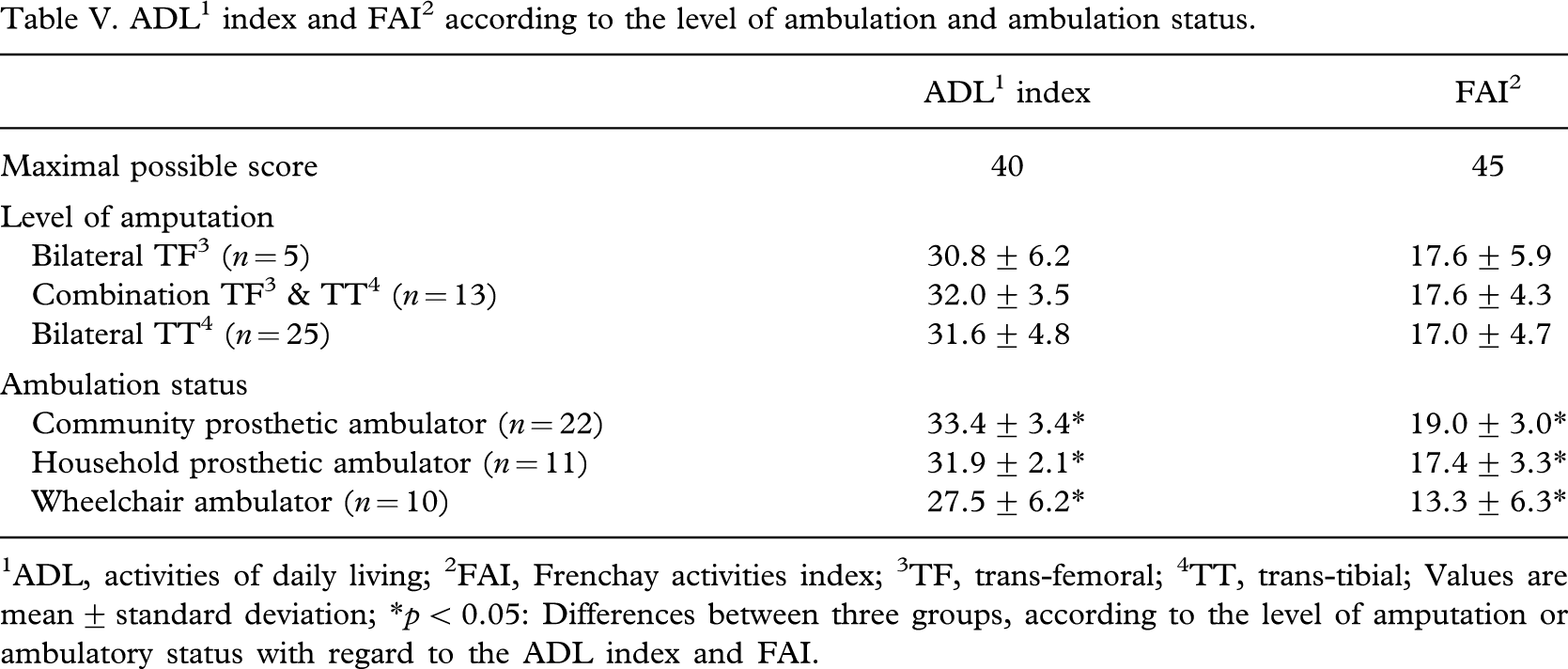
1ADL, activities of daily living; 2FAI, Frenchay activities index; 3TF, trans-femoral; 4TT, trans-tibial; Values are mean ± standard deviation; ∗p < 0.05: Differences between three groups, according to the level of amputation or ambulatory status with regard to the ADL index and FAI.
ADL1 index and FAI2 according to the sex, dependency of walking aids, and etiology.
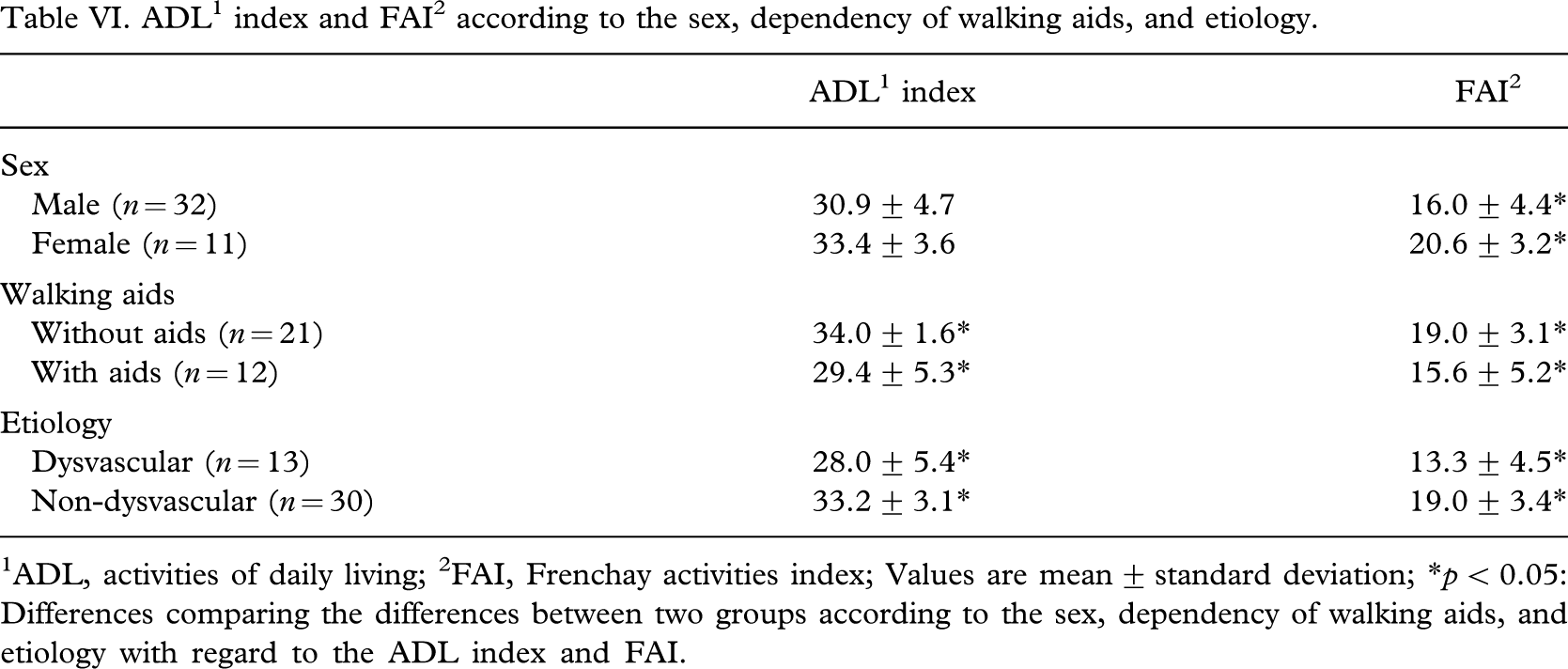
1ADL, activities of daily living; 2FAI, Frenchay activities index; Values are mean ± standard deviation; ∗p < 0.05: Differences comparing the differences between two groups according to the sex, dependency of walking aids, and etiology with regard to the ADL index and FAI.
A negative correlation was observed between age and ADL index (r = −0.518, p < 0.01) (Figure 1), and between age and FAI (r = −0.550, p < 0.01) (Figure 2). In other words, the younger the amputee, the greater was the extent of independence in activities of daily living, social function, and general activities.
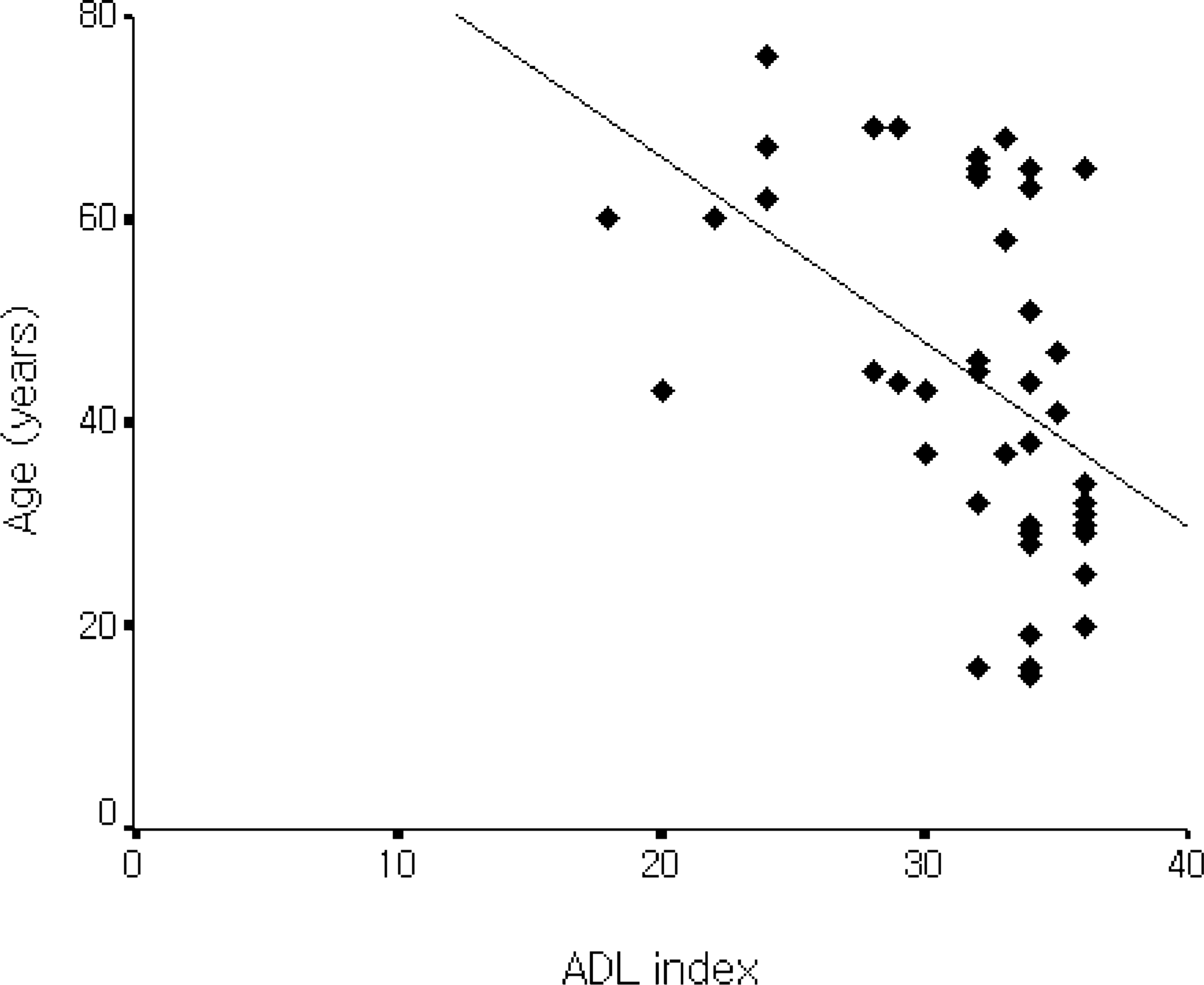
Relationship between ADL1 index and age. The ADL1 index was negatively correlated with age (r = −0.518, p < 0.01). 1ADL, activities of daily living.
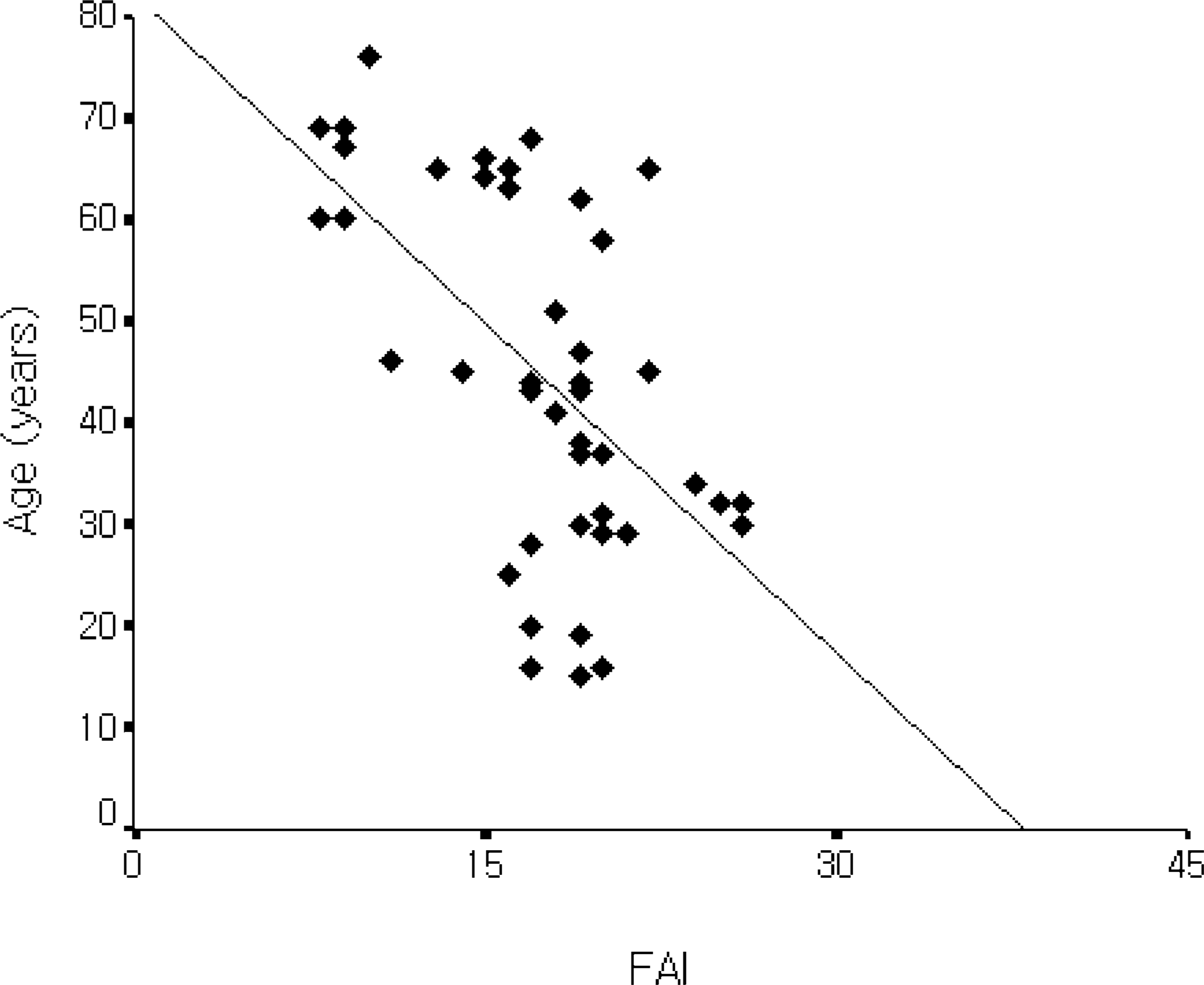
Relationship between FAI1 and age. The FAI1 was negatively correlated with age (r = −0.550, p < 0.01). 1FAI, Frenchay activities index.
Discussion
The characteristics of our study bear certain differences to those of previously reported studies in other countries, with some important additional findings and similarities.
The major cause of bilateral lower limb amputation in a total of 61 amputees, including 12 follow-up losses and 6 deceased amputees, was trauma; this is dissimilar to other reports, which said that dysvascular disease, such as diabetes and arteriosclerosis, was the leading cause of amputation in developed countries (Pernot et al. 1997; Volpicelli et al. 1983). In this study, cases of amputation with severe trauma might be included at relatively higher levels because it was conducted in the university hospital, and 16 amputees who were excluded from this study were mostly of a dysvascular amputation origin and were combination TF and TT amputees. Therefore, it is hard to totally exclude the possibility of selection bias in the choosing of subjects; this study cannot provide statistical information in bilateral lower limb amputation, but can present the clinical features and outcomes following bilateral lower limb amputation as basic data.
A literature search revealed that the majority of papers in the past concentrated mainly on use of prosthetics and mobility of bilateral amputees, and the criteria used for outcome measures tended to be vague and varied (Datta et al. 1992; Pernot et al. 1997). A successful rehabilitation for the bilateral lower limb amputees cannot be confined to the ambulation distance with their prostheses or their ability to walk as community prosthetic ambulators. In particular, the rehabilitation of bilateral amputees is more intensive than that of unilateral amputees because of concurrent medical problems or old age. Therefore, in this study, the outcome in terms of independence in activities of daily living and social integration, as well as ambulatory status, was evaluated using the ADL index and FAI scores. The ADL index is a simple scoring system which records the level of independence in ADL; FAI is a method of measuring general activities including factors other than personal care and social function in the last 3 and 6 months; the scores were low in all subjects, but the scores of the ADL index (31.6) and FAI (17.3) were high compared with those reported by Datta et al. (1992) (26.5 and 11.7, respectively). This may be due to the different selection criteria for subject groups between the two studies. In this study, young traumatic bilateral TT amputees compose the majority of the subjects; in the previous study (Datta et al. 1992), half of the subjects were bilateral TF amputees, and over 90% were of dysvascular etiology, with a mean age distribution of 66.8. Additionally, there did not appear to be any significant difference in ADL index and FAI scores according to the level of amputation. However, there were significantly higher scores for prosthetic ambulators compared with wheelchair ambulators, which is similar to the results reported by other studies (Datta et al. 1992).
In a FAI study conducted in the United Kingdom, men were significantly more active in outdoor activities while women were significantly more active in different domestic chores, and their total FAI scores were well balanced as far as gender domination was concerned (Bond et al. 1995; Wade et al. 1985). On the other hand, Hachisuka et al. (1999) and Hsieh et al. (1995) described that Japanese and Taiwanese females got much higher in total FAI scores and discussed it as a result of cultural roles. In traditional lifestyle, men do not share in household chores at home, while women are exclusively involved with household chores (Hachisuka et al. 1999). In this study, the total FAI scores of Korean female amputees were also higher than those of men, which was a similar result to other Asian studies. But the relationship between gender-related differences and other demographic factors to FAI is unclear and requires further investigation.
Various results have been reported regarding prosthetic usage status in bilateral lower limb amputees; these varying results may depend on the selection criteria of subjects, the interval of follow-up, and the definition of successful prosthetic ambulation (Kim et al. 1999; Moore et al. 1989). It has been reported that prosthesis use reaches 60 – 90% for bilateral TT amputees after intensive clinical rehabilitation (Thornhill et al. 1986). For bilateral TF amputees, these percentages are much lower: 0 – 40% (Couch et al. 1977; Pernot et al. 1997). In this study, 72% of bilateral TT and 23% of combination TF and TT amputees were community prosthetic ambulators. Only 1 of 5 bilateral TF amputees was able to walk with his prostheses with the assistance of one cane at the outdoor level. Approximately half of the amputees required no walking aids at all, and 6 subjects required just one cane. This is comparable with the results of McCollough et al. (1972), which reported that about 42% of bilateral lower limb amputees were able to walk with one stick or with no assistance, and had a lower mean age of 58.1 years.
On the other hand, most of the wheelchair ambulators were dependent for transfer activities, and only half of them were able to independently propel their wheelchairs, which indicates that even if an amputee is not fitted due to poor stump condition or conditional problems, in order to live independently at home, he should be trained in the use of walking aids and wheelchairs and in making transfers. Just less than half (46%) of the subjects were admitted to a rehabilitation centre for rehabilitative training following amputation. Therefore, the systematic and methodical management of therapeutic plans for bilateral amputees is needed in Korea when bearing in mind with the management methods of other countries (Rommers et al. 1996). In other words, after clinical rehabilitation, the amputees must be trained not only in ambulating with prostheses, but also without prostheses, in the use of walking aids and wheelchairs, and in making transfers and using toilet and bathing facilities, which would enable them to live independently at home. A successful prosthetic fitting offers the amputee mobility, and often the possibility to return home after lower limb amputations. The ability of the individual to manage a wheelchair or prosthesis in the home surroundings is an equally important issue.
The authors have no doubt that, in general, wheelchair ambulation will remain a more realistic goal for the elderly bilateral TF amputee. Additionally, it is worth noting that there was no significant difference in the ADL scores of bilateral TF amputees compared with bilateral TT amputees, nor was there a significant difference in the quality of life measured by the FAI. Bilateral TT amputees, however, can achieve reasonably good success rates and outcomes in terms of prosthetic usage. The use of prostheses in this study significantly improved ADL scores and probably altered quality of life as a measure of the FAI. Therefore, the rehabilitation programme should be directed towards a realistic and comprehensive approach to home assessment and wheelchair mobility, as well as improvement in upper-limb functions, improvement of exercise tolerance, and walking training. Prosthetic management for these amputees should only be provided after extremely careful assessment, and can significantly improve independence and quality of life.
Conclusion
Twenty-two of 43 bilateral amputees, for whom trauma was the primary cause of amputation in 65%, were community prosthetic ambulators, and performed activities including walking up and down stairs. Overall independence in activities of daily living (ADL) was significantly higher in community prosthetic ambulators compared with wheelchair ambulators, but there was no significant difference with level of amputation. In conclusion, overall independence in ADL after bilateral lower limb amputation improved with young age and prosthetic mobility. This study on bilateral lower limb amputees in Korea will help in the efforts to provide more comprehensive rehabilitation treatment as well as being used as basic data in establishing future plans.