
Abstract
Background:
Wellness activities can benefit health, yet committed adherence is challenging.
Objectives:
Identify factors associated with committed participation in an amputee wellness-walking program and determine benefits of committed participation.
Study design:
Prospective longitudinal cohort.
Methods:
Two former Paralympians led the wellness-walking sessions. Participants provided medical history and self-reported balance confidence and prosthetic functional measures. Physiotherapy professionals/paraprofessionals assessed balance and gait. Committed participants—those attending three sessions within 3 years—were compared to one-time-only participants using Fisher’s exact and independent t-tests. First and third sessions for committed participants were compared with t-tests. A bootstrapped multivariable logistic regression model was developed using significant univariate predictors.
Results:
A total of 305 volunteers averaged 55.7 ± 15.2 years, including 68.4% men, 78.4% White race; 51.8% with dysvascular amputations, 40.5% with ⩾1 prosthetic knee; and 49.1% independent community walkers. Committed participants were initially similar to one-time-only participants (p > 0.05) except for fewer years since amputation (p = 0.007), better balance ability (p = 0.001), and greater likelihood of dieting (p = 0.030). The final model—balance ability (odds ratio = 2.4), dieting (odds ratio = 3.3), and years since amputation (odds ratio = 0.94)—identified 88.0% of committed participants (p = 0.007). Balance confidence and functional improvements after three sessions were not significant (p > 0.07).
Conclusion:
Committed participants were more likely to diet, have better balance ability, and have more recent amputations than one-time-only participants.
Clinical relevance
Knowing which characteristics identify people most likely to become committed participants—such as people with recent amputations, an interest in dieting, and better balance ability—may help health practitioners from different professions promote consistent participation in wellness activities that may benefit self-reported function.
Background
Exercise-related wellness activities can provide health benefits to people with conditions such as cardiovascular disease, obesity, arthritis, and cancer.1–4 Wellness activities include exercise such as walking, cycling, playground games, or other physical activity, combined with relaxation, health, nutrition, and lifestyle education.1–4 Health benefits include improved cholesterol level, 1 physical activity,1,3,4 diet,1,2 obesity prevalence, 2 and cancer incidence. 4 Beyond physical health benefits, social participation skills and mental health conditions such as depression and somatization have improved in wheelchair athletes compared to non-athletes including people with limb loss. 5 Despite the health benefits, maintaining committed participation in wellness activities remains a challenge.1–4
People with lower limb loss face medical, physical functioning, social and community integration difficulties that impact quality of life. 6 Physical abilities may play an integral role, given that higher degrees of social integration have been associated with higher prosthetic functioning levels. 7 A consistent factor in limited prosthetic walking function has been limited balance ability, 8 while limited capacity to sustain physical activity can limit social and community integration for people with limb loss. 9 Beyond supervised exercise programs to improve balance and walking ability, 10 people with lower limb loss may benefit from home or community walking programs to help maintain progress. 11
People with lower limb loss engage in a variety of recreational and community wellness activities. 12 By age 60, however, most choose low-energy activities such as fishing or boating as opposed to moderate-energy activities such as dancing or regular exercise. 12 Sports participation prior to amputation make sports after amputation more likely, while age, amputation etiology, and surgical level have not been significantly associated with sports participation. 13 Structured wellness activities for people with lower limb loss have included walking and running programs, and adaptive sports such as soccer. 14 Wellness activities promoting physical activity are thought to provide potential physical and social benefits that may ease community integration. 5 However, committed participation for people with lower limb loss, particularly those without a history of sports participation, can be difficult to sustain.12,13
For people with limb loss, common barriers to continued participation in exercise-related activities include the energy cost of exercise-related activities, prosthetic problems, medical comorbidities, fear, and limited access.12,13 Committed participation, in general, can be influenced by inter-related motivations, conceptually defined by a three-component model of commitment as the feelings that an individual “wants to,” “needs to,” or “ought to” participate—though no criteria were established for committed participation other than continued participation. 15 Understanding factors associated with committed participation in exercise-related wellness activities may help practitioners encourage ongoing participation that can lead to potential health benefits. 9
The purpose of this study was to determine factors associated with and potential benefits of committed participation in an exercise-related wellness activity for people with lower limb loss. Aim 1 was to identify factors associated with committed participation in a wellness-walking program designed for people with lower limb loss. Aim 2 was to determine potential benefits of committed participation in the wellness-walking program.
Methods
This prospective longitudinal cohort study was approved by the participating university medical center Institutional Review Board (#AAAL9508). A wellness-walking program for people with lower limb loss provided data from people who volunteered to participate in the study and provide de-identified coded data for observational analysis, thus consent was not required. Full participation in the wellness-walking program was not contingent on participation in study activities. A committed participant was defined as someone attending ⩾3 sessions within 3 years. Because committed participation was not defined beyond continued participation, 15 we defined continued participation as at least once per year, which suited the wellness-walking program schedule.
The wellness-walking program was held in 10 outpatient facilities in 6 states during 2014–2016, drawing volunteer participants from 11 different Mid-Atlantic, Midwest, and Southeastern American states. All facilities held a minimum of annual wellness-walking program sessions, with most sites scheduled quarterly, and some sites holding monthly events in different years. Inclusion criteria included participants of any age, sex, or race; with one or more amputations of any etiology and surgical level; using prostheses of any kind, with or without use of a walking aid to walk. Exclusion criteria included anyone unable to safely participate for any reason in the wellness-walking program.
The wellness-walking program provided lecture and motivational speaking with prosthetic walking and exercise demonstrations intended for both people with limb loss and the professionals who work with them by two group leaders who were former Paralympic athletes with limb loss. Participants, caregivers, and physiotherapy and prosthetics professionals/paraprofessionals engaged together in supportive group discussion, exercise, and walking activities.
The group leaders introduced the study activities and assisted participants when needed to complete the study questionnaire, which included demographics, medical history, and self-report data. Demographics included the state participants lived, age, sex, and race. Medical history included amputation cause, surgical amputation level, and years since amputation; an active effort to diet daily, occasionally, or not at all; and concurrent medical comorbidities. Self-reported data included height and weight, the Activities-specific Balance Confidence (ABC) scale, 16 Prosthetic Evaluation Questionnaire mobility subscale (PEQ), 17 and Houghton Scale (HS) of prosthetic use for mobility. 18
Amputation-adjusted body mass index (BMI) was calculated using the Amputee Coalition BMI calculator which adjusts for lost limbs and correlates closely with BMI while significantly higher than non-adjusted BMI to provide insight into weight-related health status. 19 The ABC assesses balance confidence in daily activities and has been reliable 20 and valid compared to self-reported and clinical assessments of function for people with lower limb amputation. 21 The PEQ and HS, both shown reliabile 21 and valid,21,22 assess prosthetic function and use. The HS has been validated against objective clinical criterion to differentiate between community and home walking ability classifications.18,23 Independent community walking ability was categorized as HS scores of 9 or more, limited community/independent household walking ability was categorized as scores of 6 through 8, and limited household walking ability was categorized as scores of 5 or less.18,23
Physiotherapy professionals/paraprofessionals obtained balance and gait assessment data. Balance was assessed with two Berg Balance Scale (BBS) tasks. 24 The BBS has been shown to be valid for a wide range of balance abilities among people with lower limb loss. 25 The two BBS tasks—looking over both shoulders (#10) and turning 360 degrees (#11)—rated with the standard 4-point scale 24 demonstrate excellent reliability across raters of varied training. 26 Balance ability was reported as the mean of the two BBS tasks. The 2-min walk test (2MWT) was used to assess gait, marked out with a standard 20 m walk track measured with a metal tape measure and timed by participating professionals/paraprofessionals. Considered simple to perform with minimal training, 27 timed walking measures like the 2MWT have strong reliability and validity for people with lower limb loss.28,29
Statistical analysis
Participants who attended ⩾3 sessions during the 3 years were defined as committed participants to take into account the inter-relationship between commitment, persistence, and participation. 30 To determine differences between committed participants and casual participants, first-session data for participants attending only one session—heretofore referred to as one-time-only participants—were compared to committed participants using Fisher’s exact tests and independent t-tests (p < 0.05). To clearly differentiate between one-time-only and committed participants, the 41 participants who attended twice-only were excluded. No differences at outset existed among people attending once, twice, or three times (analysis of variance (ANOVA) or Fisher’s exact, p > 0.05), except that balance ability was better for three-time participants than for one- or two-time attendees. Bootstrapping with 1000 iterations was used for all t-tests and logistic regression procedures to protect against distribution variability within a sample with uneven distribution and a small subgroup and potential non-normal distributions for some variables.31,32
Univariate logistic regression using significant bivariate variables, preserving confounding variables with p < 0.10 to maintain potentially relevant variables, was performed to determine variables that could identify committed participants. 32 Independent variables not meeting the p < 0.10 threshold were excluded. For logistic regression, the balance score was converted to a dichotomous variable with a 3.5 cutoff score determined by receiver operating curve (area under the curve = 0.68, 95% confidence interval (CI) = 0.58–0.78, p = 0.002). All significant univariate predictors were entered together to develop a multivariable logistic regression model. The initial model was reduced by separately removing each non-significant variable to produce the most parsimonious final model, with Hosmer–Lemeshow goodness-of-fit chi-square to determine model fit adequacy. Odds ratio (OR) estimated the potential influence of each factor on committed participation. To determine whether any change had occurred among committed participants by the third session, first- and third-session data were compared with paired t-tests (p < 0.05).
Results
Attendees living in 11 states volunteered to participate (Table 1). Of the 305 volunteer participants, a total of 234 one-time-only participants attended only once; 30 committed participants attended ⩾ 3 times within the 3 years of the study. Of the 264 participants for analysis, 68.4% were men, 78.4% were of White race, and the mean age was 55.7 ± 15.2 years. A mean 6.2 ± 11.9 years had passed since the primary ampu-tation, with 51.8% undergoing amputation for dysvascular reasons (31.7% had diabetes with or without peripheral artery disease). For 40.5%, at least one prosthetic knee was required—such as for a transfemoral amputation—and 60.7% used a walking aid or wheelchair; with 49.1% categorized as independent community walkers, 30.2% categorized as limited community walkers, and 20.7% categorized as limited household walkers.18,23 Participants had an average amputation-adjusted BMI of 30.2 ± 6.4 kg/m2 and 58.4% reported dieting at least occasionally (Table 1).
Characteristics of wellness-walking program participants.
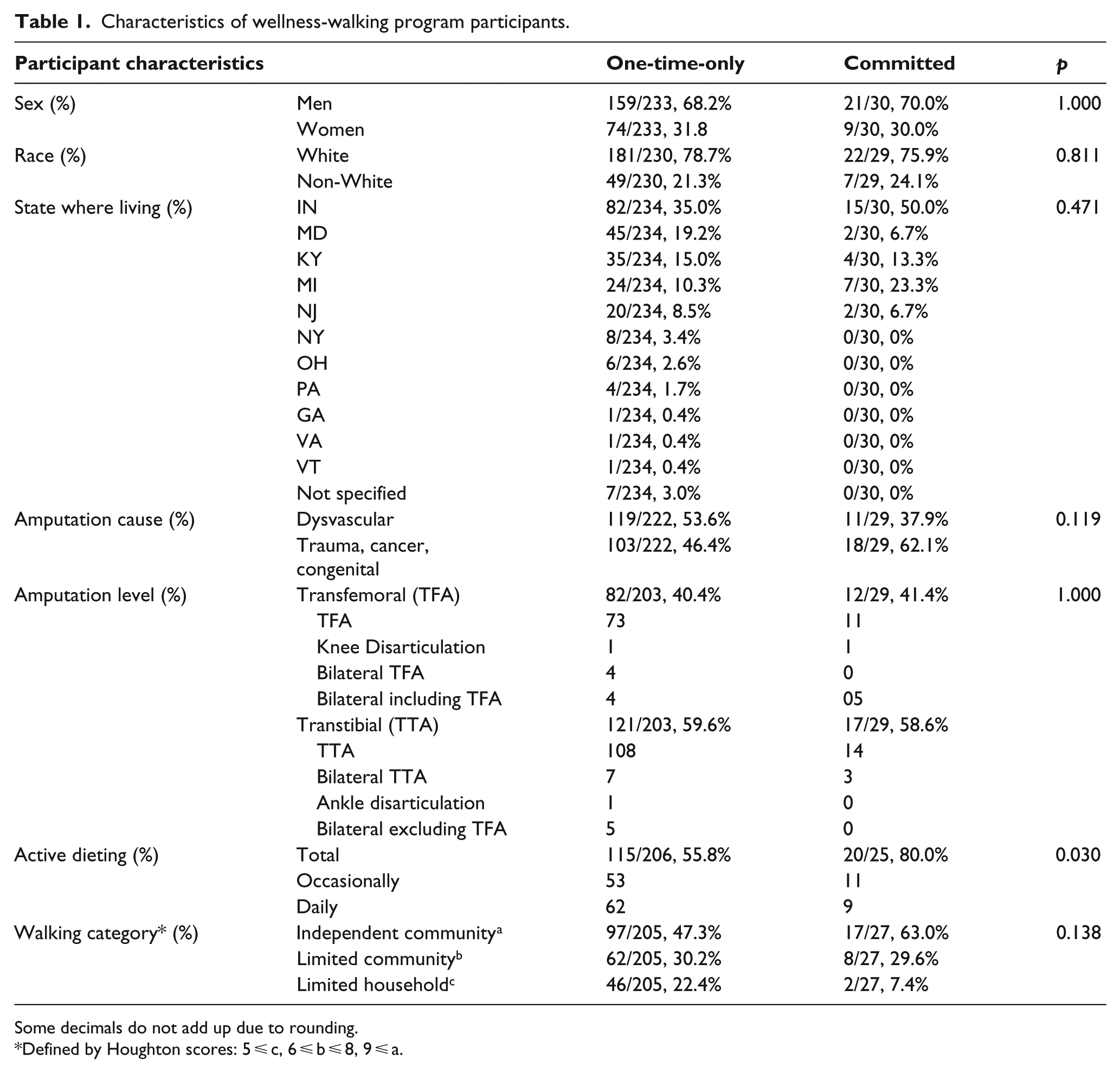
Some decimals do not add up due to rounding.
Defined by Houghton scores: 5 ⩽ c, 6 ⩽ b ⩽ 8, 9 ⩽ a.
Group comparison
At the time of their first session, committed participants were similar to one-time-only participants in all respects (e.g. sex, amputation etiology and level, all comorbidities; p > 0.05) except that committed participants were fewer years removed since amputation (p = 0.007), demonstrated better balance (p = 0.001), and were more likely to be dieting (p = 0.030). Community prosthetic walking ability determined with the HS (p = 0.062) and 2MWT walking speed (p = 0.085) did not reach significance (Table 2).
Comparison between one-time-only and committed participants.
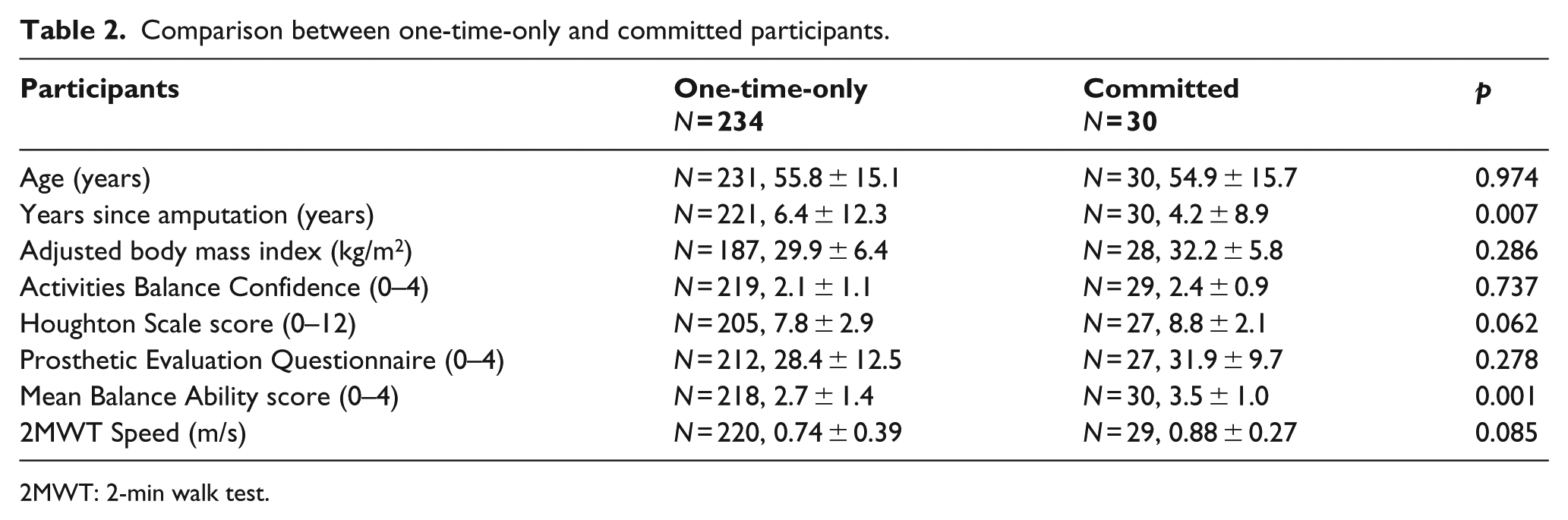
2MWT: 2-min walk test.
Factors associated with committed participation
The initial model included only variables found significant in univariate logistic regression, all entered together: total HS score, 2MWT, years since amputation, average balance ability score ⩾ 3.5, and active dieting. The final model (Table 3) identified 88.0% of people who became committed participants (p = 0.007, goodness of fit = 0.84) and included only years since amputation (OR = 0.943, 95% CI = 0.874–1.018, p = 0.028), balance ability (OR = 2.416, 95% CI = 1.003–5.820, p = 0.042), and active dieting (OR = 3.262, 95% CI = 1.157–9.194, p = 0.021). In short, participants at session one who reported actively dieting were over three times more likely to become committed participants than those not dieting. Furthermore, participants successfully performing the two balance tasks (average score ⩾ 3.5 out of 4) were over two times more likely to become committed participants than those with less balance ability. Finally, with each year since amputation, participants became approximately 6% less likely to become a committed participant.
Determinants for people with lower limb loss who became committed wellness-walking participants.
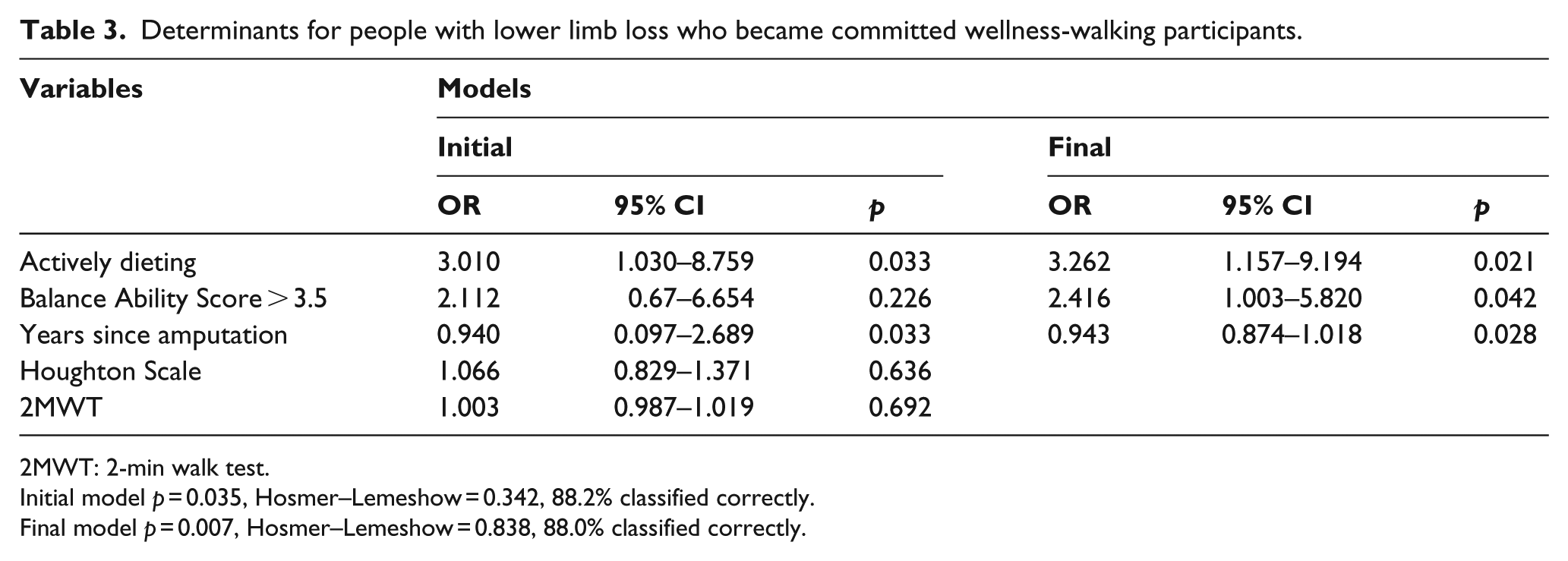
2MWT: 2-min walk test.
Initial model p = 0.035, Hosmer–Lemeshow = 0.342, 88.2% classified correctly.
Final model p = 0.007, Hosmer–Lemeshow = 0.838, 88.0% classified correctly.
Potential benefits
From first to third session, committed participants demonstrated no significant change in outcome measures after participation in three sessions (p > 0.05). Balance Confidence increased from 2.4 to 2.8 on the 4-point ABC scale (p = 0.074). Prosthetic use for mobility increased from 8.8 to 9.8 on the 12-point HS (p = 0.072).
Discussion
The primary study finding was that at their first session people with limb loss who later became committed participants in a wellness-walking program were different in several ways than people who came only once. People who became committed participants were more likely to be actively dieting, were fewer years removed from amputation, and had better balance ability.
People with better balance ability were approximately three times more likely to become committed participants, possibly because sufficient balance allows access to the community to attend events. Balance impairment has been consistently noted as the primary limiting factor in prosthetic functioning. 8 An inability to look over one’s shoulder (BBS #10) and turn in a circle (BBS #11) without assistance, as required for successful completion of the balance tests,24,25 may limit ongoing participation in wellness activities. The impact of balance limitations may extend to home exercise and walking program adherence, making improving balance ability a critical goal for rehabilitation professionals to enable committed participation in wellness activities.
People who reported actively dieting were also approximately three times more likely to become committed participants. The perceived need to diet may be a motivating factor for people to develop their individual commitment to ongoing wellness activities. 30 Actively dieting may suggest a need to control weight gain that can impact prosthetic fit and could indirectly influence prosthetic use. A detailed exploration of nutritional intake may provide insight into the need to diet for optimal health 1 in people with limb loss. Intention to actively diet may be a factor for wellness activity organizers and rehabilitation professionals to highlight in encouraging continued participation. In addition, fewer years since amputation increased the likelihood of becoming a committed participant. The need for or perceived benefit of a wellness-walking program may be more acute in the early years after amputation.
While self-reported and objective measures of community walking ability were not significant between one-time-only and committed participants, the 8.8 mean HS score for committed participants approached the cut-off score of 9 that demarcates the independent community walking category,18,23 compared to the 7.7 mean score for one-time-only participants. Indeed, the 0.88 m/s mean walking speed of committed participants exceeded the 0.8 m/s cut-off used to describe independent community walking ability in people with disabilities including those with lower limb loss, 23 as opposed to the 0.74 m/s mean walking speed of one-time-only participants. Knowing what factors predispose an individual to become a committed participant may help wellness program organizers or referring rehabilitation clinicians target people who need more encouragement to participate or those most likely to be interested in wellness activities.
A secondary finding was that committed wellness-walking program participants may potentially benefit from continued participation as indicated by self-reported balance confidence and prosthetic function. Outcome measures for committed participants did not differ by the third session (p > 0.05). However, the increased scores on self-reported measures for balance confidence (ABC) and prosthetic functional use (HS) had p < 0.075, suggesting a potential trend with a >92% chance that observed differences did not result from mere chance. The 9.8 mean HS score for committed participants after three sessions exceeded the cut-off score of 9 demarcating the independent community walking category.18,23
That no corresponding statistical trend was apparent for objective balance and walking speed measures (2MWT) underscored that self-reported and objectively assessed measures are not interchangeable. Participant perception of their confidence and sustained walking ability may impact community integration and determine an individual’s assessment of their quality of life. 9 Attending three wellness sessions within a 3-year period was insufficient to provide enough exercise to lead to a significant physical improvement. However, prolonged low levels of physical activity have been associated with faster declines in quality of life through aging. 33 Committed participation in a wellness-walking group may lead to increased independent activity and perceived benefits among participants that could potentially improve the quality of life of people with limb loss. Future research exploring the efficacy of wellness activities on physical functioning and quality of life would provide insight regarding the possible impact of wellness activities on people with lower limb loss.
Committed participation may be related to program adherence, which includes both participation and follow through with health recommendations. Adherence to wellness programs has proven challenging despite the health benefits conferred, with adherence rates ranging from 33.9% to 93.0% for conditions such as cardiac disease, obesity, arthritis, and cancer.1–4 Only 9.5% of participants with lower limb loss in the wellness-walking program became committed participants. The low rate of commitment cannot be directly compared to adherence rates in other studies due to the range of adherence measures1–4 and also the fact that the wellness-walking program made no specific attempt to develop committed participation. Among people with lower limb loss, factors identified as influential for enhanced adherence to physiotherapy programs have been clear communication and feedback between patients and clinical practitioners. Interactions in a stimulating exercise program—particularly in a group setting—and a lack of feeling pain or emotionally stigmatized were considered positive influences. 34 Other than presence of pain, these factors may well be provided by the wellness-walking program design. However, adherence may be further enhanced by emphasizing factors that predispose people to become committed participants.
The feelings influencing a commitment to participate were described as three components: “want to,” “need to,” and “ought to.” 15 That participants volunteered for the study activities may demonstrate “want to.” That most participants had not yet reached the independent community walking level and were more likely to become committed when fewer years removed since amputation may be consistent with “need to,” to improve their walking. That committed participants were more likely to be actively dieting may suggest “ought to.” The three-component model was developed for employment, however, not wellness activities. That committed participants were more likely to have good balance suggests a fourth component may be relevant for developing committed participation in wellness programs for people with limb loss: “able to.” Understanding the factors influencing committed participation and the potential health benefits of a wellness-walking program may help rehabilitation practitioners encourage people to continue participating in exercise-related wellness activities in socially supportive environments.9,34
Strengths and weaknesses
Study strengths include the longitudinal design, a broad sample of people with limb loss, and novel assessment of a wellness program designed exclusively for people with lower limb loss. This retrospective study of de-identified coded data precluded knowledge of the number of people who declined to participate, use of specific prosthetic componentry and medications. A notable weakness is that the dieting measure was not validated. Other weaknesses include varied time between sessions, variable attendance, and different assessors. Some participants attending during the last year may have gone on to become committed participants but were not captured as such in the data collection window. As with any cohort study, no conclusions can be drawn regarding cause and effect of any potential benefit of committed participation. Future randomized control trials are warranted.
Conclusion
Participants who later became committed participants in a wellness-walking program could be identified using data from their first session: people with limb loss were approximately three times more likely to become committed participants if they were actively dieting and demonstrated better balance. Committed participants showed potential improvement in self-reported balance confidence and prosthetic walking ability.
Footnotes
Acknowledgements
The authors would like to thank Dennis Oehler and Todd Schaffhauser and the Amputee Walking School for their participation in this study. Without their dedicated and sustained efforts this research would not have been possible.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (Grant/Award Number: “1 R49 CE002096”). Its contents are solely the responsibility of the authors and do not represent the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services.