
Abstract
Introduction: Physiotherapists routinely prescribe the use of two different early walking aids (EWAs) to individuals who have recently undergone unilateral transtibial amputation. No research to date has investigated the kinematic gait patterns of transtibial amputees walking with an EWA during early rehabilitation. The aim of the current RCT study was to compare gait patterns when walking with two different EWAs and whether either EWA provided patients with greater gait benefits.
Methods: Patients were randomly assigned into one of two EWA groups, one group using the Amputee Mobility Aid and another using the Pneumatic Post-Amputation Aid, prior to receiving their functional prosthesis. A 3D motion capture system recorded kinematic data from their first steps up to discharge from rehabilitation.
Results: Walking velocity increased significantly (p < 0.01) during rehabilitation. Control of the prosthetic knee improved during rehabilitation in both groups. A lack of conclusive differences between EWAs was noted at discharge from rehabilitation.
Discussion: Both groups displayed changes in gait patterns in different gait measures during rehabilitation. However, these changes were not the same for both groups. Gait adaptations occurred soon after walking with a functional prosthesis.
Conclusion: The results from this study would suggest that neither EWA was more beneficial for gait retraining during rehabilitation.
Keywords
Introduction
In order to re-learn how to walk with new lower limb mechanics, transtibial amputees typically follow a course of prosthetic rehabilitation or physiotherapy treatment. The Chartered Society of Physiotherapy guidelines1,2 advocate the use of early walking aids (EWA) in the assessment and treatment of lower limb amputees. Early walking aids are generic prosthetic devices used for initial gait re-education and partial weight-bearing, prior to casting for a functional prosthesis.3 Their use has documented benefits such as accelerated healing of the residuum4 and reduced time from surgery to functional prosthesis casting.3
Several previous studies have investigated the kinematics, kinetics and temporal-spatial parameters of transtibial amputee gait.5-8 One study investigated the relationship between static weight-bearing, self reported pain and walking velocity in transtibial amputees during the first four weeks of prosthetic training. This study reported significant improvement in amputee's self-reported pain and static weight bearing together with a 0.23 m/s increase in walking velocity from the first to the fourth week of rehabilitation when walking with a prosthesis.9 The literature suggests that, with experience, transtibial amputees are able to walk proficiently.5 However, most studies have generally investigated the gait patterns of experienced patients, with the average time since amputation ranging from 2–22.3 years.5-8,10
Previous research has not investigated the influence of different EWAs on relearning independent gait or how the prior use of an EWA affects early prosthetic gait. However, understanding how individuals modify their gait as they learn to walk with a prosthesis in a rehabilitation setting could have important implications for both patients and therapists.
In the UK, there are currently two different EWAs that are routinely used by physiotherapists in transtibial amputee rehabilitation: The Amputee Mobility Aid (AMA, Ortho Europe Ltd., Alton, UK) (Figure 1) and the Pneumatic Post Amputation aid (PPAM aid, Ortho Europe Ltd., Alton, UK) (Figure 2). The functional difference between the two devices is that the AMA allows the biological knee to flex and extend during gait by using a simple hinge mechanism. However, the PPAM aid maintains the biological knee in a relatively extended position within a rigid external frame that does not articulate at the knee. To the authors' knowledge, no published study to date has assessed the short or long-term impacts of using different EWAs on kinematic gait patterns during early gait retraining.
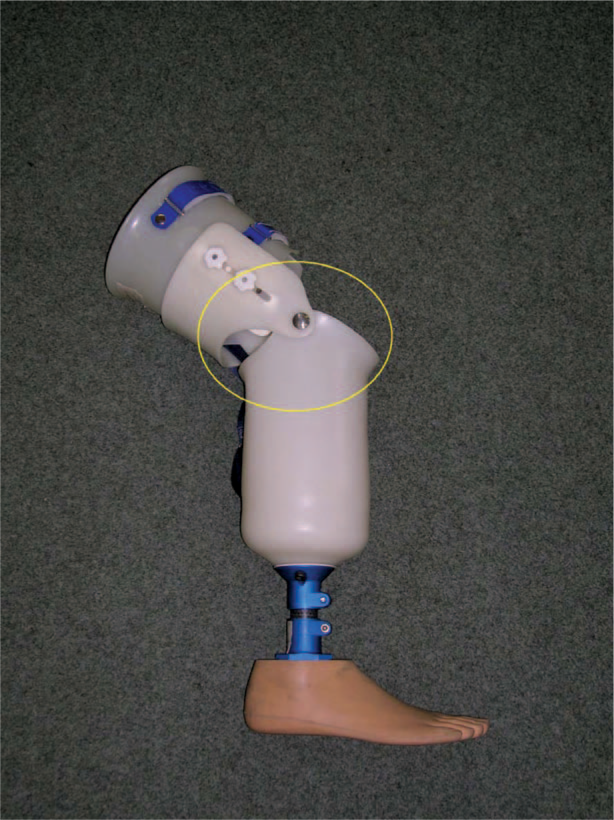
The Amputee Mobility Aid (AMA), with articulated knee circled. Image used with permission (Ortho Europe Ltd, Alton, UK) (www.ortho-europe.co.uk).

The Pneumatic Post-Amputation Aid (PPAM Aid) (left) and inflatable residuum bag (right). Image used with permission (Ortho Europe Ltd, Alton, UK) (www.ortho-europe.co.uk).
One previous study investigated gait adaptations when able-bodied patients were required to walk with a prosthetic simulator, designed to mimic a prosthetic-like experience.11 Similar to gait with the PPAM aid, prosthetic knee flexion was not possible. Results demonstrated that gait adaptations occurred early in the learning process when performing the novel walking task.11 Although the study examined young, able-bodied patients, results indicated that the early stages of learning a novel ambulatory task were particularly important. This may have important implications for amputee rehabilitation.
The aims of the current randomized controlled trial (RCT) study were three-fold: (i) The study investigated the gait patterns of unilateral transtibial amputees using either the AMA or PPAM aid; (ii) the study investigated how the previous use of either EWA influenced gait as individuals started to walk with their functional prostheses for the first time; and (iii) the longitudinal changes in gait that occurred from the first use of the functional prostheses to discharge from prosthetic rehabilitation were investigated. As the AMA group practiced gait with an articulated knee joint whilst using their EWA, it was hypothesized that amputees having previously used the AMA would display a larger improvement in gait measures than those having previously used the PPAM aid.
Methods
Patients
Fifteen patients (12 men and three women) who had recently undergone unilateral transtibial amputation and were expected to receive, but had not yet received, a functional prosthesis were recruited into the RCT. Written informed consent was given by each patient prior to data collection.
Patient characteristics of unilateral transtibial amputees.
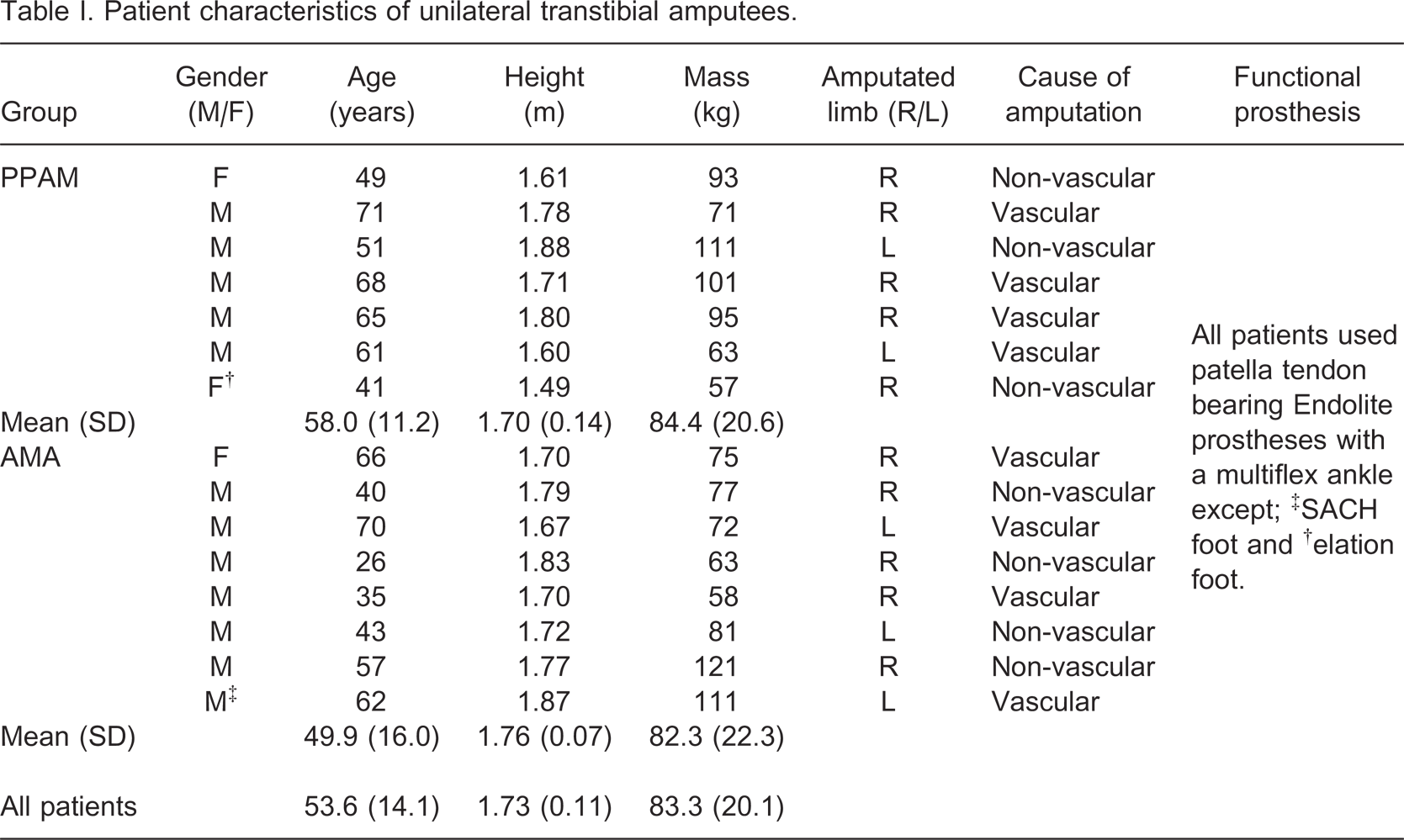
To satisfy inclusion criteria patients were at least 18 years of age and had recently experienced a unilateral transtibial amputation. In addition, patients were required to tolerate the use of an EWA and walk independently, but within parallel bars, under the supervision of a physiotherapist and were expected to receive a functional prosthesis. Patients were excluded from the study if they had not been able to walk prior to amputation due to a medical condition (e.g., rheumatoid arthritis) or had previously experienced amputation of the contralateral limb. Participants were also excluded if they were not expected to receive a functional prosthesis or were unable to follow instructions and/or unable to follow a programme of rehabilitation. Ethical approval was awarded by the Local NHS research ethics committee.
Experimental design
Data were collected when patients attended a specialist amputee rehabilitation physiotherapy unit staffed by physiotherapists with clinical expertise in this area. The unit serves as both an in- and out-patients clinic as part of the Regional Limb Fitting service. Patients attended treatment as often as physiotherapists felt was appropriate to their stage of rehabilitation. Patients followed an individually designed programme consisting of goals negotiated and agreed with the patient. Prior to data collection, patients were randomly allocated into experimental groups using the sealed envelope method; one group using the AMA (n = 8) the other using the PPAM aid (n = 7).
Assessments
Patients attended a different number of gait retraining sessions as walking ability with either EWA or patients' first functional prosthesis progressed at different rates. The majority of data were collected when patients attended as outpatients. To enable comparisons between patients, data collection sessions were standardized to five time points during their rehabilitation. Data were collected during Visits 1 and 2 when patients attended the initial and final rehabilitation sessions, respectively, whilst using their specified EWA. Visit 3 measured patients whilst using their functional prosthesis for the first time and data were then collected two weeks later at Visit 4. Assessing patients at Visit 4 allowed the measurement of gait adaptations that occurred in the short time following receipt of the functional prosthesis. The final data collection was completed when patients were discharged from rehabilitation at Visit 5.
Patients participated in the current study during normal rehabilitation treatment. Early walking aids were only available during physiotherapy treatment, limiting the time patients could practice walking with such devices. Once patients had received their functional prosthesis they were then assessed by physiotherapists to ensure safe mobilization outside of the rehabilitation setting. The amount of time they used their prosthesis outside of the rehabilitation setting varied according to their needs and abilities. EWAs and functional prostheses were fitted by experienced physiotherapists according to the manufacturer's guidelines.
Protocol
Patients' height (m) and mass (kg) were recorded post-surgery using a free-standing height measure and beam column scale (Seca, Birmingham, UK). Data collection took place in the amputee physiotherapy room. An eight-camera motion capture system (Qualisys, Gothenburg, Sweden) captured 3D kinematic data at a sampling frequency of 100 Hz using Qualisys Track Manager software (Qualisys, Gothenburg, Sweden).
Patients wore their own comfortable, flat footwear during all data collection sessions. The PPAM aid has a convex rocker ‘foot’ at the distal end (Figure 2), thus patients only wore a shoe on the intact limb. Once patients had been fitted with their specified EWA or functional prosthesis, reflective markers were attached to specific anatomical landmarks by the same investigator according to the six degrees of freedom marker model set, described previously.12 Marker placement on the prosthetic limb was estimated from intact limb anatomical landmarks, a procedure previously reported in the literature.6
Patients were required to walk between parallel bars at a self-selected velocity, resting as required. Walking velocity was not controlled for in the current study. Previous studies have found walking speed to be a good overall descriptor of changes in gait performance when adapting to a novel walking task.11 A minimum of five walking trials were recorded per session.
Data analysis
Data frames of steady-state walking were analysed and averaged for the five walking trials. 3D coordinate data were interpolated using a cubic spline algorithm and filtered using a low pass filter with a cut-off frequency of 6 Hz in Visual 3D Software (C-Motion, MD, USA). Gait events were identified visually from the motion capture data and group mean (SD) temporal-spatial parameters were calculated and normalized to the gait cycle. Kinematic data of the ankle, knee, hip and pelvis were measured in the frontal and sagittal planes and normalized to the gait cycle. Frontal plane (hip and pelvis) and sagittal plane (ankle, knee, hip and pelvis) joint angles were analysed at foot contact and toe off. Peak joint angles were also compared during the swing phase and, for the knee only, during the loading response. In order to display the effects of using either EWA when walking with a functional prosthesis during rehabilitation, data were presented from the first (Visit 3) to the last (Visit 5) use of functional prostheses.
Statistical analysis
Group averaged means were used for statistical analysis. Differences in each group characteristic were analysed using an independent samples t-test. A mixed design repeated measures analysis of variance (ANOVA) was performed: Limb (prosthetic vs. intact) × Group (AMA, PPAM) × Time (visit number), with repeated measures on the last factor. In the instance of a significant time main effect or interaction effect, post-hoc comparisons were conducted using a Sidak adjustment in SPSS v.15.0 (SPSS Inc., Chicago, USA). Underlying assumptions of the ANOVA analysis were verified and where sphericity was violated, adjustments to the degrees of freedom following the Greenhouse-Geisser method were applied. The alpha level of statistical significance was set at p < 0.05.
Results
The mean (SD) time interval for all participants between Visits 1 and 5 was 78.1 ± 25.3 days (range 40–126 days). There were no significant differences between the PPAM group and the AMA group in age (years) (p = 0.28), height (m) (p = 0.29) or mass (kg) (p = 0.85). There were no significant differences between the PPAM group and the AMA group in terms of total rehabilitation time (days) (p = 0.36), time to receipt of prosthesis (days) (p = 0.25) or the total number of physiotherapy treatments received during rehabilitation (p = 0.71).
Temporal-spatial characteristics
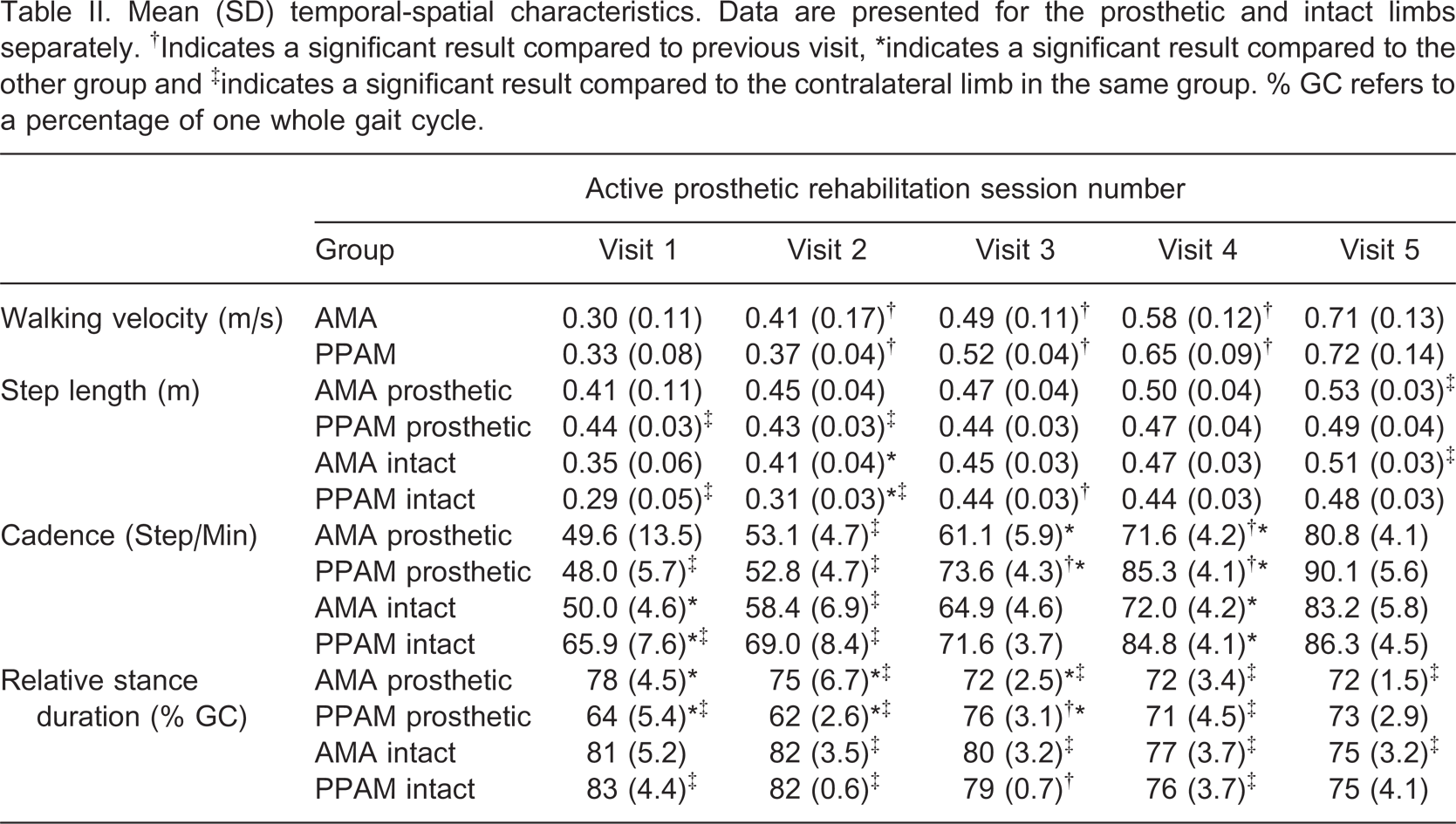
Temporal-spatial variables across all visits are presented in Table II with complete statistical analyses provided in Table III. Post-hoc comparisons for the walking velocity time main effect revealed that walking velocity increased significantly during rehabilitation, except between Visits 4 and 5 (p = 0.07). However, there were no significant differences in walking velocity between groups.
Mean (SD) temporal-spatial characteristics. Data are presented for the prosthetic and intact limbs separately. †Indicates a significant result compared to previous visit, ∗indicates a significant result compared to the other group and ‡indicates a significant result compared to the contralateral limb in the same group. % GC refers to a percentage of one whole gait cycle.
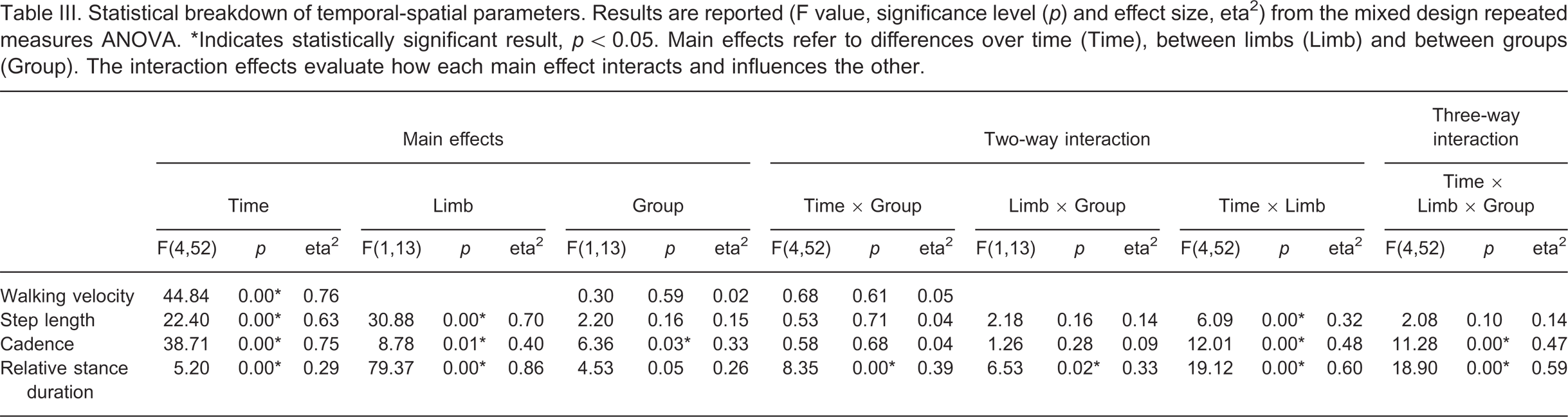
Statistical breakdown of temporal-spatial parameters. Results are reported (F value, significance level (p) and effect size, eta2) from the mixed design repeated measures ANOVA. ∗Indicates statistically significant result, p < 0.05. Main effects refer to differences over time (Time), between limbs (Limb) and between groups (Group). The interaction effects evaluate how each main effect interacts and influences the other.
Post-hoc comparisons for the significant time by limb interaction revealed that prosthetic step length was significantly longer than intact limb step length at Visits 1, 2 (p = 0.00) and 5 (p = 0.02). However, from Visit 3 to discharge from rehabilitation, intact limb step length increased significantly (p = 0.01), reducing between limb differences, although prosthetic step length was still longer than intact limb step length at Visit 5.
During Visits 1 and 2, the PPAM group displayed significantly larger between limb differences in cadence compared to the AMA group (p = 0.01). Also increases in prosthetic limb cadence from Visits 2–3 and Visits 3–4, were significantly larger in the PPAM group compared to the AMA group (p = 0.04).
Finally, post-hoc comparisons for the relative stance duration three-way interaction effect showed that during Visits 1 and 2, the PPAM group showed significantly larger between limb differences than the AMA group, due to shorter relative stance duration in the prosthetic limb (p = 0.01). The between limb differences for the AMA group were somewhat, but not significantly reduced over time, as relative stance duration decreased in both limbs. The PPAM group displayed a significant increase in prosthetic limb relative stance duration from Visit 2 to Visit 3 (p = 0.01).
Joint kinematics
Group mean joint kinematics from functional prosthetic gait are presented in the sagittal plane (Figure 3) and frontal plane (Figure 4). Significant three-way interactions were found for all sagittal plane ankle and knee angles throughout the gait cycle. However, at Visit 1 and 2 the ankle joint of both EWAs and the knee joint in the PPAM aid were non-articulated. Therefore, statistically significant differences in ankle and knee joint kinematics might be expected once the patients were able to move their joints through a greater range of motion using a functional prosthesis.
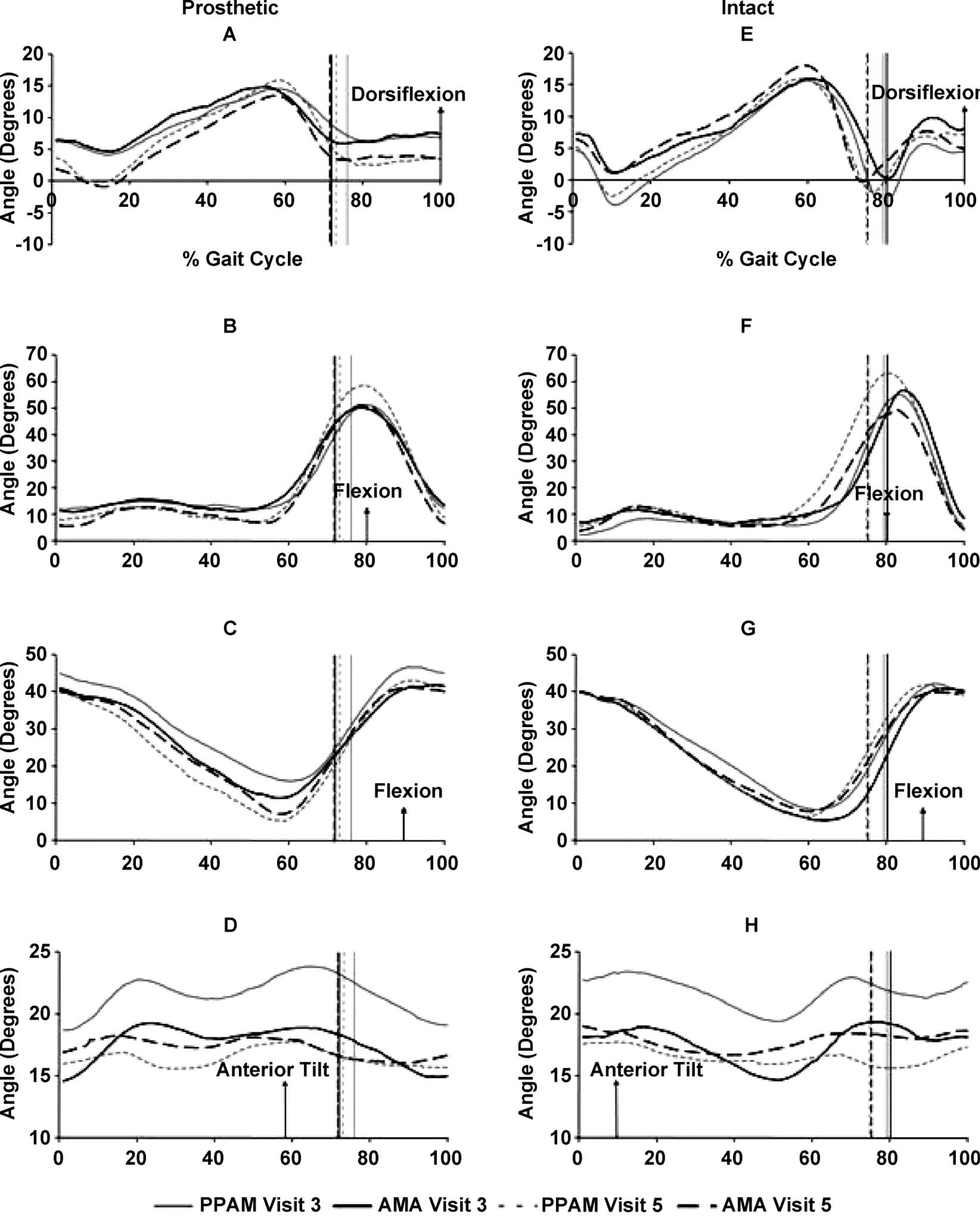
Group mean sagittal plane kinematics of the prosthetic limb (A) ankle, (B) knee, (C) hip and (D) pelvis and intact limb (E) ankle, (F) knee, (G) hip and (H) pelvis. All values in degrees (°). Time normalized to 100% of gait cycle. Vertical lines represent toe off.
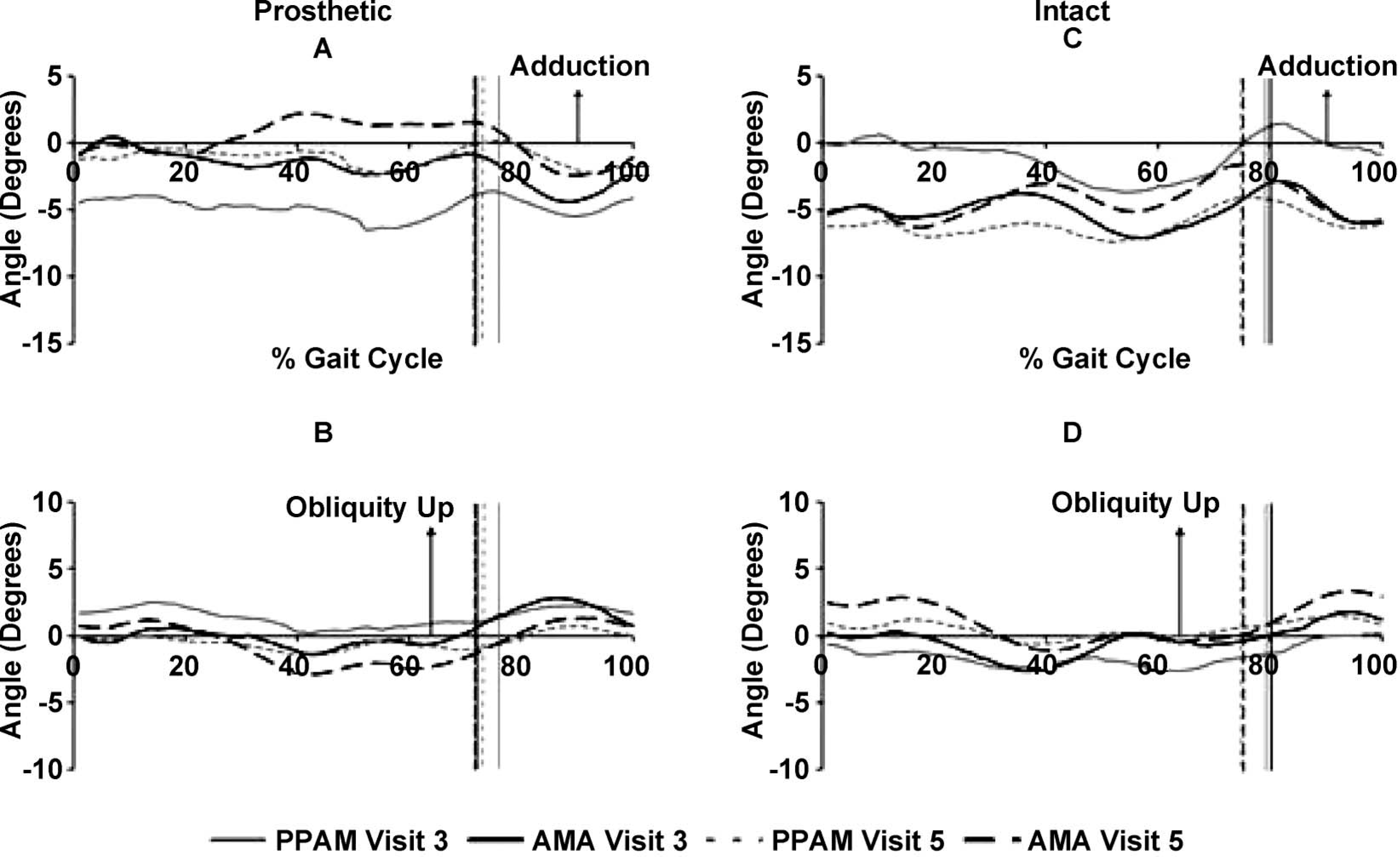
Group mean frontal plane kinematics of the prosthetic limb (A) hip and (B) pelvis and intact limb, (C) hip and (D) pelvis. All values in degrees (°). Time normalized to 100% of gait cycle. Vertical lines represent toe off.
Sagittal plane kinematics
Active plantarflexion was not possible given the passive nature of the ankle-foot complex of the observed prosthetic limbs. The intact limb in the PPAM group achieved greater ankle plantarflexion during early stance and early swing phase at Visit 5 (Figure 3).
The prosthetic knee for both groups was generally flexed throughout stance at Visit 3, and gradually became more extended during early and late stance by discharge (Figure 3). Peak knee flexion in the loading response was not significantly different during rehabilitation or between groups. Throughout rehabilitation, the intact limb of the AMA and PPAM aid groups did not fully extend at the knee during mid-stance. However, peak knee flexion during the loading response occurred somewhat before in the intact limb compared to the prosthetic limb (Figure 3). The reduction of peak intact knee flexion between Visit 3 to 5 in the AMA group during swing can be observed in Figure 3, whereas, the PPAM group peak intact knee flexion increased during the same period.
Throughout rehabilitation, neither limb in either group achieved full hip extension during the gait cycle. The PPAM group displayed a larger change in prosthetic limb hip range of motion from Visits 3 to 5, almost reaching full extension at the pre-swing phase (Figure 3). At foot contact (p = 0.02) and toe off (p = 0.00), post hoc analysis revealed that the PPAM group's prosthetic limb hip flexion significantly increased from Visits 2 to 3 resulting in significant three-way interaction effects.
No significant interaction effects were found in pelvic tilt, reflecting the low magnitude of changes in pelvic motion. Pelvic tilt remained anterior in direction, although reduced pelvic range of motion was observed at Visit 5 in both prosthetic and intact limbs (Figure 3).
Frontal plane kinematics
The AMA group displayed an observable reduction in intact hip abduction from mid-stance to early swing during Visits 3–5, whereas the PPAM group displayed a general increase in intact hip abduction (Figure 4). Post-hoc analysis revealed that PPAM group intact limb hip abduction significantly decreased between Visits 2 and 3 at foot contact (p = 0.00) and toe off (p = 0.01), resulting in significant three-way interactions for peak hip abduction. Prosthetic limb hip abduction generally decreased during the gait cycle in both group from Visits 3 to 5 (Figure 4).
At Visit 5, hip-hiking had reduced on the prosthetic side and increased on the intact side in relation to Visit 3, for both groups (Figure 4). Profiles of pelvic obliquity remained similar but changed in magnitude. However, post-hoc analysis revealed that, in the PPAM group, intact hip-hiking significantly decreased between Visits 2 and 3 at foot contact (p = 0.02) and toe off (p = 0.01), resulting in significant three-way interactions.
Discussion
The current RCT study investigated the frontal and sagittal plane kinematic differences between unilateral transtibial amputees using an articulated (AMA) and a non-articulated (PPAM aid) EWA during gait retraining. The current study also investigated how the previous use of either EWA influenced subsequent gait patterns, and if either EWA had any gait benefits during rehabilitation.
EWA gait
Walking velocity increased similarly between groups as patients progressed through rehabilitation. At the end of EWA use, velocities observed in the current study (0.39 ± 0.12 m/s) were slower than previously reported in transtibial amputees, four weeks into their rehabilitation (0.51 ± 0.40 m/s).9
The PPAM group displayed larger between limb differences in cadence at Visits 1 and 2 and achieved increases in walking velocity more as a function of greater prosthetic limb cadence at Visit 3. The AMA group took longer steps with both respective limbs to increase walking velocity. This is a novel finding and suggests that the type of EWA used during rehabilitation results in different gait adaptations but similar increases in walking velocity. The consequences of this finding are unknown and would benefit from further investigation.
Between limb differences have been reported in studies of experienced amputees, as was the case in temporal-spatial measures of the current study, supporting the notion that gait asymmetry is an inherent characteristic of amputee gait.5,10,13 Therefore during gait retraining and rehabilitation, achieving gait symmetry may not always be the goal. Rather, returning patients to a functionally stable and comfortable level of mobility may be more realistic. Further improvement in limb symmetry may be anticipated with additional prosthetic use post-discharge, as previous studies found that kinematic gait patterns of transtibial amputees, with more experience of walking with a prosthesis than the patients in the current study, demonstrated minimal distinguishing features from able-bodied individuals.5
Transfer to functional prosthesis
At Visit 3 the prosthetic knee had a small range of motion and was mainly flexed during weight acceptance. At Visit 5, there was an increase in knee range of motion during weight acceptance. In both groups, the knee was more extended at initial contact, there was a greater knee flexion during the loading response with the knee then extending towards mid-stance. The greater range of motion suggested that patients improved their ability to control the knee joint on the prosthetic side. With practice, patients seemed to gain proficiency in controlling the knee musculature especially during the loading response. Despite the fact that the AMA group had more practice controlling the knee of the prosthetic limb since Visit 1, the knee flexion profiles for both groups were remarkably similar at discharge, with the PPAM group showing increased knee flexion during swing (Figure 3). Patients in the current study appeared to adapt the intact limb more than the prosthetic limb, as between limb differences were reduced during rehabilitation, especially in temporal-spatial measures. This may have reflected the amputees increased ability to adjust their intact limb during gait whilst progressively developing the control of their prosthetic limb, an adaptation strategy that has been reported previously.11
Hip-hiking on the prosthetic side reduced over time during the gait cycle, however, there were no observable differences between groups. This indicated that the amount of ‘hip-hiking’ measured at Visit 1 in both groups, reduced towards discharge. This suggests a greater ability to flex and extend the prosthetic knee, thus reducing the need to elevate the pelvis and flex the hip on the prosthetic side to ensure adequate ground clearance.
Prosthetic gait
Walking velocity did not significantly increase during the latter stages of rehabilitation, reflecting a plateau in progress at discharge from physiotherapy. This indicated that physiotherapists were only discharging patients once a consistent level of mobility had been achieved. Prior to discharge from physiotherapy treatment, patients that had the capability, practised more functionally demanding tasks such as walking at different velocities, turning, stair climbing, carrying loads and walking on different terrains. Practice of such tasks, may be necessary to produce further improvements in walking ability at discharge.
At discharge from rehabilitation, walking velocity and cadence values were still below values reported in the literature.5-7,13 However, previous studies did not investigate gait patterns of new prosthetic users5-8,10,13 and some of the previous research investigated gait patterns from a younger, healthier population undergoing amputation following trauma, with a greater potential for speedier rehabilitation.5,7
Both groups of patients displayed decreased prosthetic stance duration. This has previously been explained as a compensatory mechanism employed by amputees to protect their residuum from experiencing high peak vertical ground reaction forces.7 Prosthetic stance duration increased during rehabilitation such that stance duration was similar between prosthetic and intact limbs of both groups. This suggested that patients became more comfortable and confident whilst weight-bearing on the prosthetic limb during the course of rehabilitation.
All patients displayed a reduction in intact limb ankle plantarflexion between 50 and 80% of the gait cycle, compared to values reported in literature.5 Keeping the intact limb in dorsiflexion during early swing may assist in reducing step length and between limb asymmetry as well as aiding ground clearance. This kinematic adaptation may also explain the observed reduction in walking velocity, as plantarflexor muscle contribution was absent on the prosthetic limb.
Hip flexion profiles revealed that across all visits, neither limb reached full extension in either group.5,14 No patient displayed a hip flexion contracture, as assessed by Thomas' test. However, there was an improvement in prosthetic hip extension in both groups, as the hip extended more between 50 and 65% of the gait cycle between Visit 3 and 5. The lack of extension at the hip (late stance) and knee (initial contact, mid stance), as well as ankle dorsiflexion and anterior pelvic tilt gave the impression of a more flexed hip, knee and ankle gait pattern.
These findings suggest that transtibial amputees may benefit from additional home or therapy-based exercise programmes that target increasing muscle length, strength and joint mobility of the lower limb musculature. Future studies may also consider assessing muscular strength and activity during amputee gait relearning. The flexed hip, knee and ankle gait pattern and associated lowered centre of gravity coupled with lower walking velocities, could also reflect a lack of confidence in mobility of the new amputees in the current study.
Conclusion
The findings from the current RCT study contribute to our understanding of how amputees achieve levels of gait proficiency required for independent living. Some kinematic and temporal-spatial differences were found between the two groups of transtibial amputees during EWA rehabilitation. When patients transferred from EWA to their functional prosthesis, differences in gait between groups were still apparent. However, at discharge, both groups had improved walking performance and had reached an acceptable level of walking ability, despite very different gait patterns with the EWAs during early rehabilitation. This suggests that the most significant gait adaptations occurred following receipt of a functional prosthesis. Our results did not show a clear benefit in gait patterns at discharge following use of either EWA. Increased patient numbers and kinetic analysis of amputees would help to further illicit the origin of differences observed between the AMA and PPAM groups.
Footnotes
Acknowledgements
This project was financially supported by the Owen Shaw Award from the Circulation Foundation, UK and the East Yorkshire Hospitals NHS Trust.