
Abstract
Background: Little data have been reported on the factors that are important in bilateral amputee walking ability especially the role of hip strength.
Study Design: Observational, case-control study where participants were evaluated at a single point in time.
Objectives: The aim of this study was to investigate the factors involved in bilateral amputee walking ability by assessment of walking speed, perceived exertion, exercise intensity, physiological cost index (PCI) and hip muscle strength.
Methods: For a group of 10 bilateral amputees, with different levels of amputation, and a non-pathological reference group, walking ability was assessed using the two-minute walk test. Hip muscle strength was assessed using isokinetic strength tests.
Results: Bilateral amputees were found to have slower walking speeds and increased PCI of walking which were correlated to higher levels of amputation. Peak hip torques were reduced in the amputees, which was only significant for concentric extension torque (p = 0.029), and approaching significance for concentric flexion (p = 0.061) and abduction (p = 0.057). Bilateral amputee peak hip strength suggested a positive trend with increasing walking ability.
Conclusions: Bilateral amputee walking ability was reduced and mainly related to level of amputation. The role of hip strength in bilateral amputee walking ability requires further investigation.
Clinical relevance
In bilateral amputee prosthetic rehabilitation, amputation levels are a key factor in walking ability. Besides level of amputation, and assuming general fitness, hip strength may be a key factor in achieving functional walking mobility as a bilateral amputee.
Background
Bilateral lower limb amputees comprise a small, but challenging group in the prosthetic rehabilitation practice, as they lack compensation from a normal limb, and the prostheses need to be synchronised for optimum performance. In the UK, bilateral amputees take up only 6% of lower limb prosthetic referrals. 1 Although there are many more bilateral amputees, most of them are not referred for prosthetic rehabilitation and do not regain walking mobility, mostly due to other diseases, age and physical problems. 2 When compared to able-bodied people and unilateral amputees, bilateral amputees show significantly slower walking speeds with increased energy costs of walking.3-8 For unilateral amputees, higher levels of amputation have been found to be positively correlated to increasing energy costs of walking and slower walking speeds.9-13 This relationship has not been observed in bilateral amputees, partly due to the small number of studies investigating bilateral amputee walking.
Besides the relationship between level of amputation on energy cost and walking speeds, hip muscle strength has been found to be positively correlated with walking speed and mobility levels in unilateral amputees.14-16 After unilateral transtibial (TT) or transfemoral (TF) amputations, muscle atrophy and a reduction in muscle strength are commonly observed in the residual amputated limb, which is weaker than the intact leg.15-21 Interestingly, in sports active TT amputees, hip strength of the residual leg was found to be increased and stronger than for the intact leg and also stronger than in able-bodied athletes. 22 These data suggest that, in order to achieve good walking ability, additional hip strength at the amputated leg is needed to compensate for the loss of leg function caused by the amputation. No literature has been found that investigates the role of hip muscle strength in bilateral amputee walking. As bilateral amputees do not have an intact leg to compensate for the loss of function of their amputated leg, any loss of muscle strength at their residual legs can have an effect on their walking performance. In bilateral amputee walking, hip moments and power have been found to be increased23,24 and, therefore, hip muscle strength is expected to be of significant influence on the walking ability of bilateral amputees. Better understanding of the role of hip muscle strength in bilateral amputee walking may help improve success rates of bilateral amputee prosthetic rehabilitation.
The aim of this study was to investigate bilateral amputee walking ability, by assessing walking speed, perceived exertion, exercise intensity, physiological cost index (PCI), and hip strength. The investigations included a two-minute walk test and an isokinetic hip torque assessment. It was hypothesised that bilateral amputee walking ability is reduced compared to able-bodied mobility, and negatively correlated to increasing levels of amputation and decreased hip muscle strength.
Methods
Participants
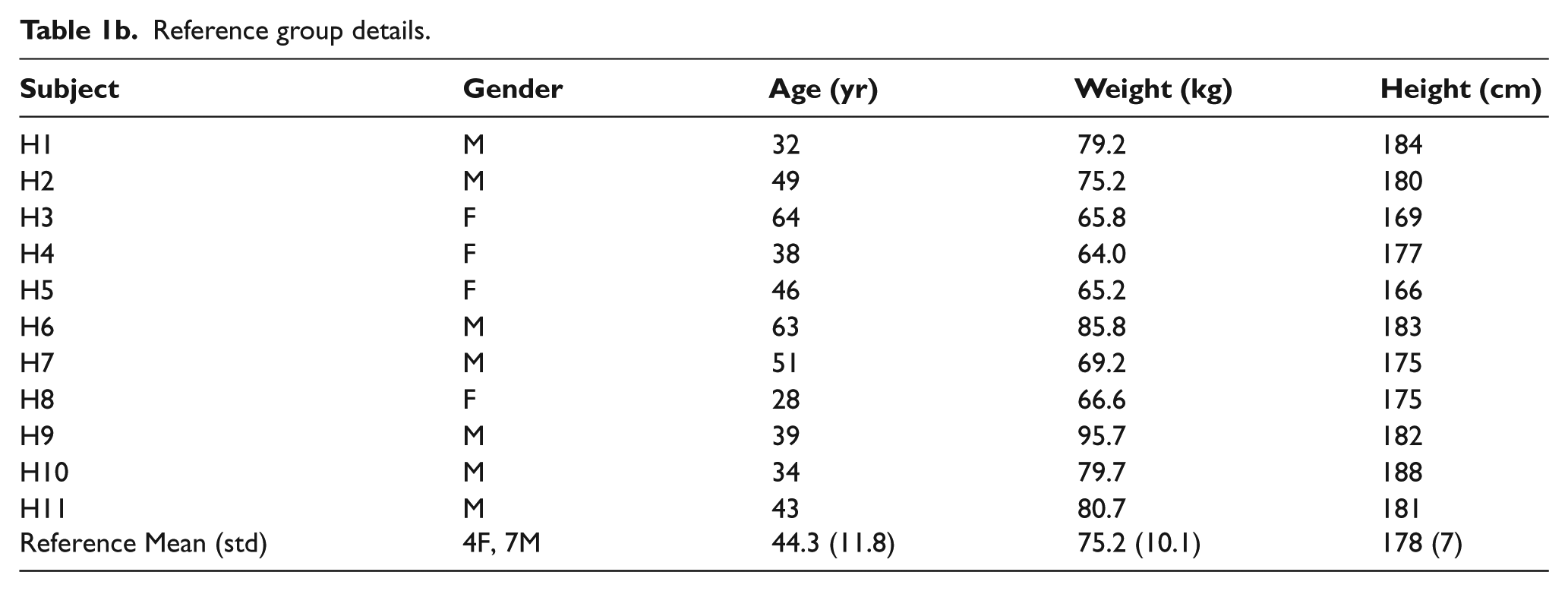
Ten bilateral amputees participated in the study. The amputations had taken place a minimum of two years prior to the start of this study. The amputee participants were free from cardiovascular disease, and were able to walk for a minimum of 20 m in one go with or without the aid of a walking stick. These minimal requirements were set to ensure that the participants were established walkers who were able to perform the tests in the protocol. On the basis of these criteria the amputees were selected and recruited from the Limb Fitting Centre at the Royal National Orthopaedic Hospital (RNOH) Stanmore patient database. Three amputees had bilateral Syme amputations, three amputees had bilateral TT amputations, and four had a combination of one TF and one TT amputation. Eleven non-pathological reference subjects with a similar range in age and gender were recruited from the Royal Veterinary College London community. The details of the participants are summarised in Tables 1a and 1b.
Amputee details.
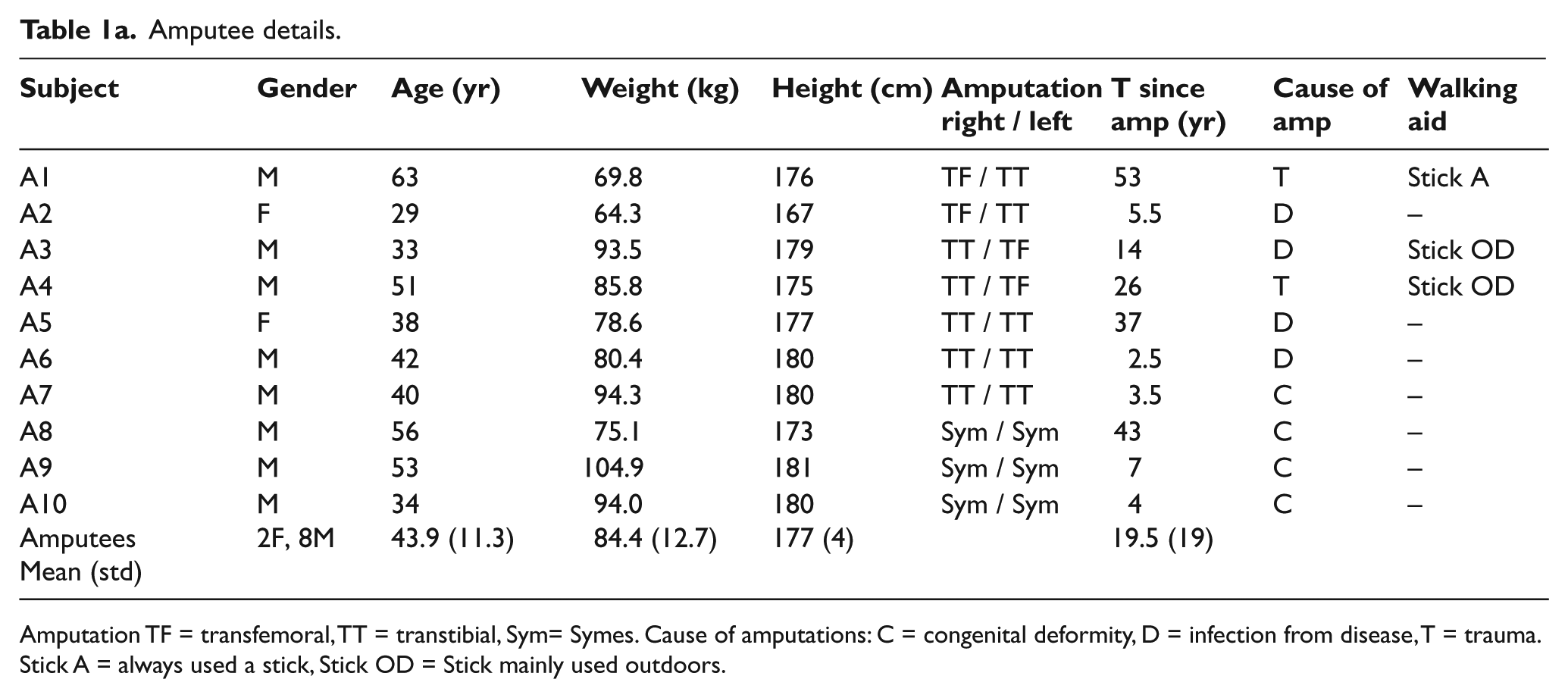
Amputation TF = transfemoral, TT = transtibial, Sym= Symes. Cause of amputations: C = congenital deformity, D = infection from disease, T = trauma. Stick A = always used a stick, Stick OD = Stick mainly used outdoors.
Reference group details.
The study was approved by Royal Veterinary College London. Written consent was obtained from all participants prior to their participation in the study.
Walking ability
In the current study walking ability is expressed by average walking velocity, perceived exertion, exercise intensity and PCI during the two-minute walk test. For the two-minute walk test, 25 each participant was instructed to walk as far as possible in two minutes round an indoor track of 55 m in length. The total distance covered in the two minutes was recorded. Walking velocity was defined as the average speed over the two-minute walk test in m/s. Directly after the walk test, the participants were asked to rate their exercise intensity on the Borg scale. 26 The heart rate of the participant was recorded continuously during the test via a heart rate monitor (Polar™). The momentary resting heart rate was recorded preceding the walk test directly after the participant had been seated for five minutes. Exercise heart rate was defined as the maximum heart rate recorded during the two-minute walk test. The peak heart rate was chosen as it shows the maximum attained during the test. PCI is a frequently used measure for energy expenditure 27 based on heart rate. Exercise intensity and PCI were calculated as follows:


in which HRexercise is the maximum heart rate during the two-minute walk test, HRrest is the resting heart rate and HRmax is the estimated maximum heart rate, which is 220 minus age in years.
Differences between the reference and amputee group in walking speed, PCI and exercise intensity were statistically tested using the Mann–Whitney U test, and the ranked parameter, rate of perceived exertion, was tested using the Fisher’s exact test. Walking speed and PCI were tested for correlations with level of amputation using Kendalls tau correlation.
Hip muscle strength
Isokinetic peak hip torques for both the left and right legs were assessed using an isokinetic dynamometer (KinCom) in three anatomical directions: hip flexion, extension and abduction. For each subject both legs were tested (except for participant A01 whose right stump was too short to be able to perform the flexion and extension test).
For the flexion and extension torque tests, participants were positioned supine on the bed with their hip rotation centre aligned with the axis of the dynamometer as shown in Figure 1. The pelvis was stabilised with a velcro strap. The resistance pad was placed on the thigh at a comfortable position just above the knee (anterior for hip flexion and posterior for hip extension) and secured with a velcro strap. The subject was properly positioned when no sliding of the pad or of the subject on the bed was observed during movement. To account for the effect of gravity, the leg was weighed at the neutral position with no muscular tension, and the KinCom software corrected the torque data automatically. Maximum isokinetic torques were recorded over a range of motion from neutral (straight leg) to approximately 90º of hip flexion.
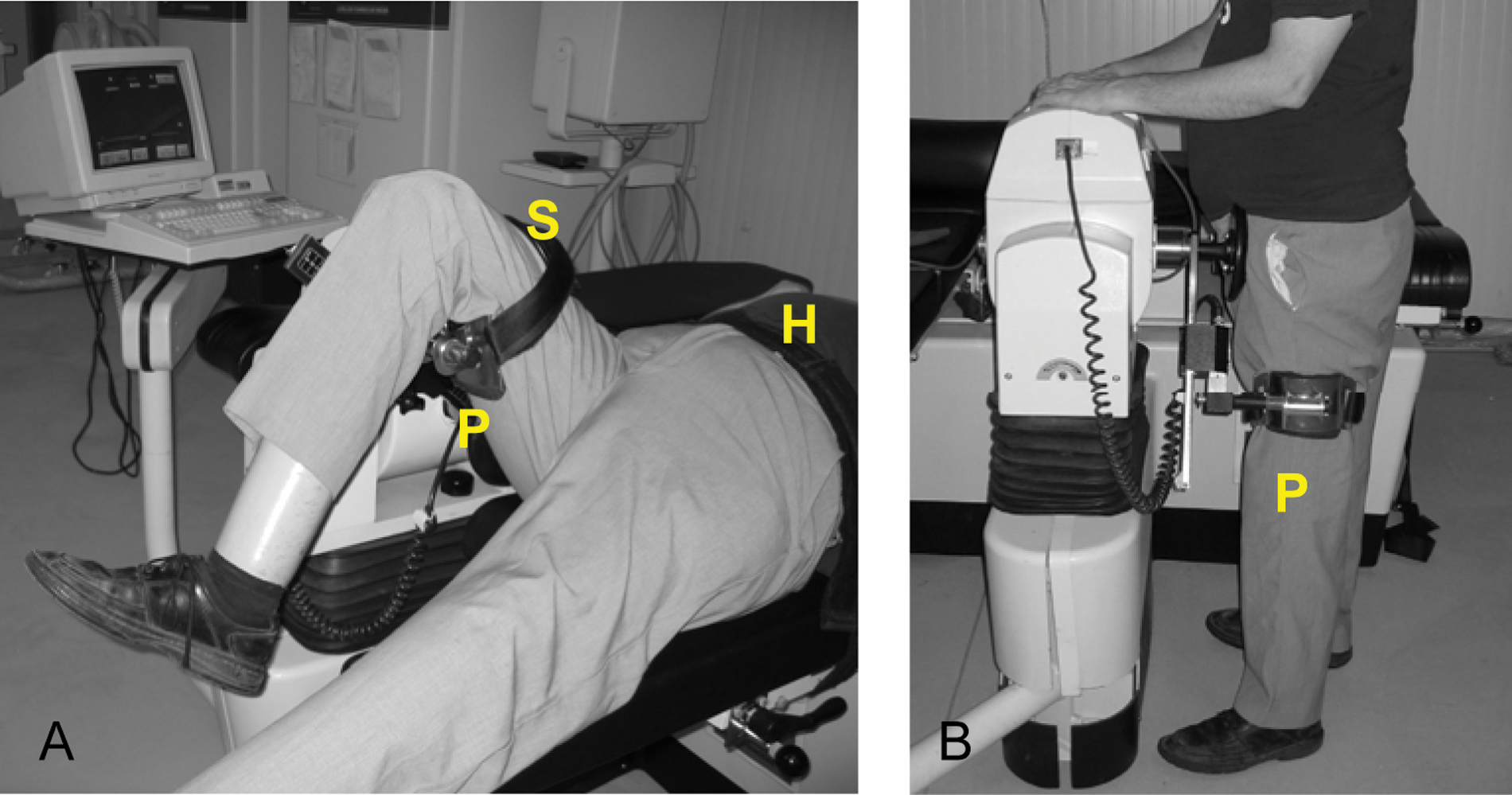
Setup for isokinetic hip torque assessment (A): hip extension, (B): hip abduction. H = hip strap, P = resistance pad, S = leg strap.
For hip abduction torque assessment the participants were standing upright with their hip centre of rotation aligned with the rotational axis of the KinCom machine arm. They rested their hands on the top of the machine for balance. The bed was positioned laterally against the standing leg for additional stability. The force pad was placed on the lateral side just above the knee of the tested leg (Figure 1). The abduction torques were assessed at a range of motion from anatomical zero to maximal hip abduction angle while standing straight (30º–50º). Before and during the torque measures the participants were instructed to keep their body upright and push with maximum effort using their hip rather than their whole body.
Each test was performed in a concentric and eccentric direction at a constant rotational velocity of 30º/s. Before each measurement of maximum torque, the participants were allowed a few submaximal warm-up movements to familiarise themselves with the test. During the measurements the participants were instructed to push with maximum effort using their hip muscles. Verbal encouragement was given to the participants during the test. Four repetitions of maximum hip torque measurement were undertaken for each of the six exercises. Between each repetition, a minimum of 20 seconds of rest was given, and a minimum of three minutes rest was given between muscle group tests. The highest torque record out of the four repetitions was selected for further analysis.
All peak hip torques were measured in Nm and normalised by body weight, to facilitate comparison across subjects, and the values for both legs were pooled to be used as one subject-specific value. Peak hip torque data were not normally distributed, therefore the differences between the means of the bilateral amputees and reference group were tested for significance using the Mann-Whitney U test and correlations of hip torques with walking speed were analysed using Spearman’s rank correlation and with level of amputation using Kendalls tau correlation.
Results
Walking ability
The two-minute walk test results are presented in Table 2. The average walking speed of the bilateral amputees was 33% slower (p < 0.001) than for the reference group, and showed a negative correlation with increasing level of amputation (kt = −0.55, p = 0.044). Exercise intensity was 7.6% higher for the amputees (p = 0.049), but the rate of perceived exertion was similar for both groups. The PCI for the bilateral amputees was increased by 51% compared to the reference group (p = 0.009), and was found to be positively correlated to their level of amputation (kt = 0.75, p = 0.005), as shown in Figure 2. In this figure, one of the reference subjects showed a very low PCI, but this does not have much influence on the mean PCI of the reference group since the PCIs of the other reference subjects were very similar.
Two-minute walk test parameters for bilateral amputees.
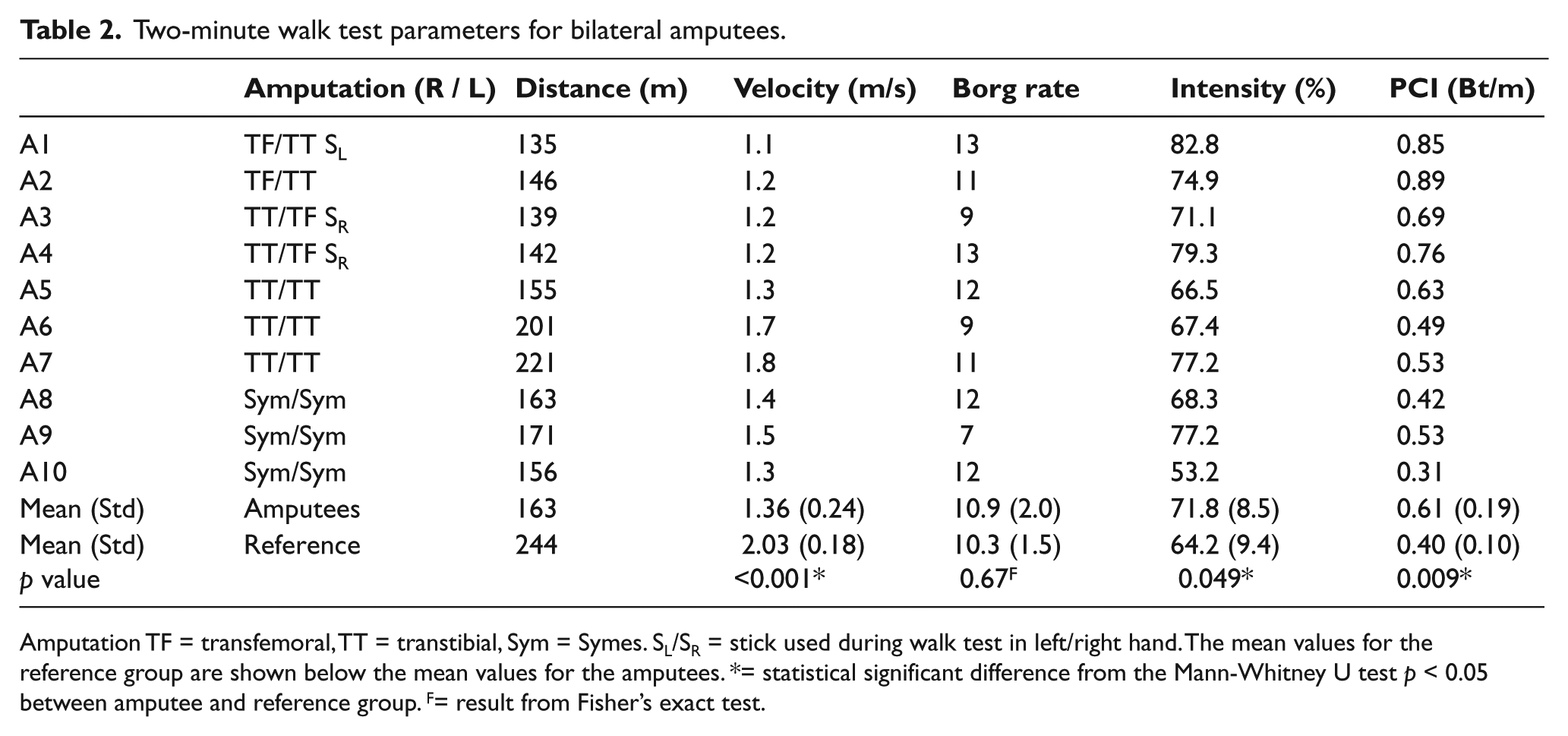
Amputation TF = transfemoral, TT = transtibial, Sym = Symes. SL/SR = stick used during walk test in left/right hand. The mean values for the reference group are shown below the mean values for the amputees. *= statistical significant difference from the Mann-Whitney U test p < 0.05 between amputee and reference group. F= result from Fisher’s exact test.
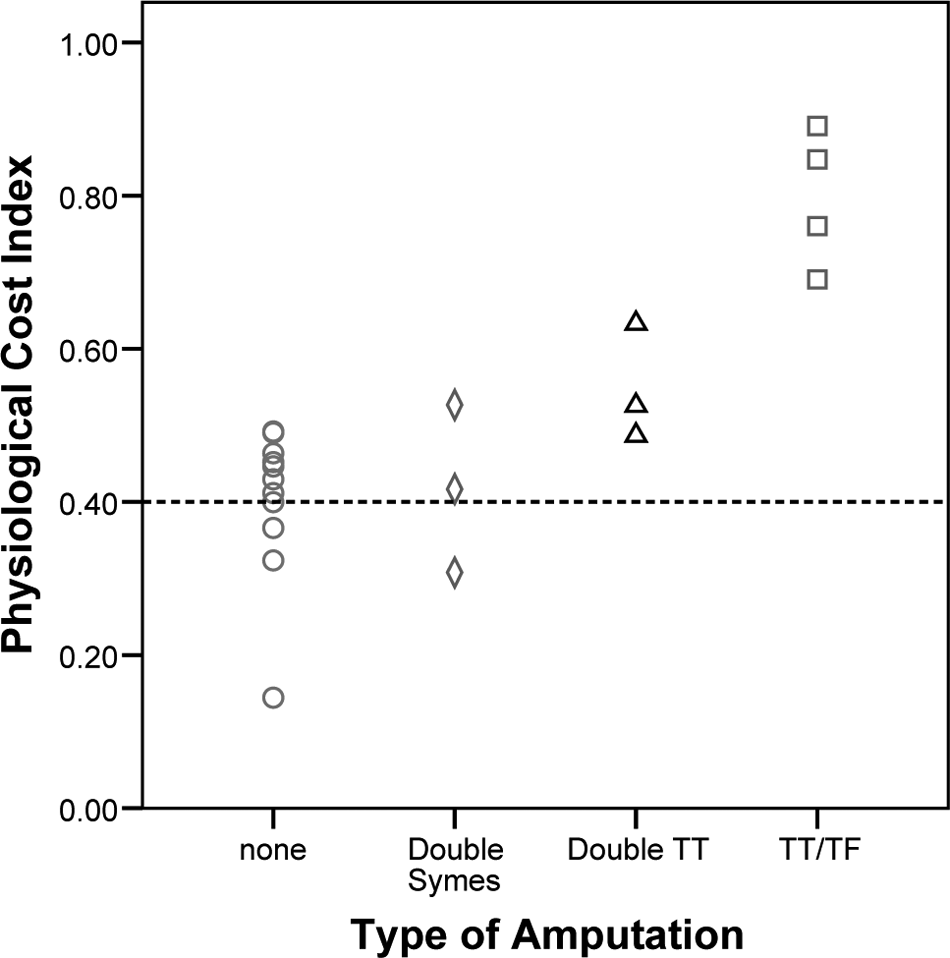
PCI (Bt/m) plotted against level of bilateral amputation. --- = mean PCI for the reference subjects.
Hip muscle strength
The mean peak isokinetic hip torque values for the bilateral amputees and reference group are presented in Figure 3. The mean hip torques were 29–34% lower for the amputees compared to the reference group in both concentric and eccentric measurements for all three directions. This difference was only statistically significant for concentric hip extension (p = 0.029), although differences for both concentric flexion (p = 0.061) and abduction (p = 0.057) approached statistical significance. Only two amputees showed peak hip torques in the range of the reference subjects.
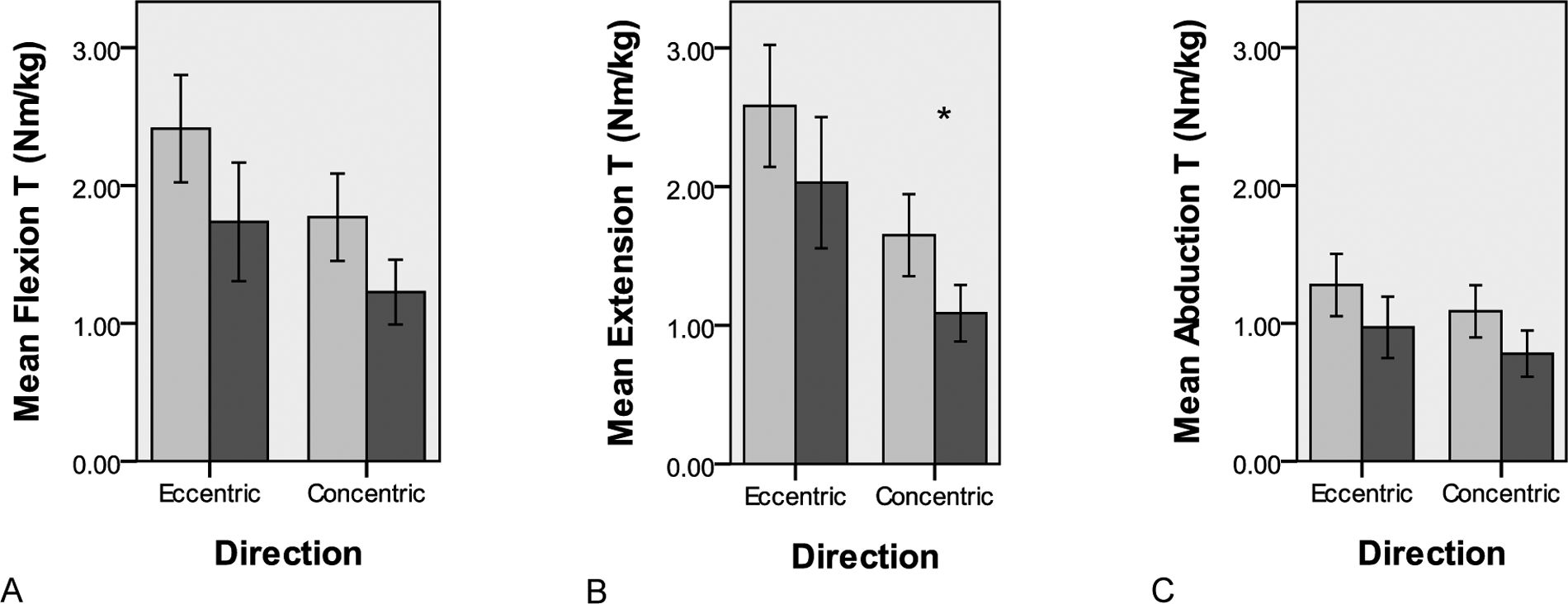
Concentric and eccentric hip flexion (A), extension (B) and abduction (C) torques. Normalised by body mass. Mean (+/- SE) values for reference group (light grey) and bilateral amputee group (dark grey). *= significant difference p < 0.05 between amputee and reference group.
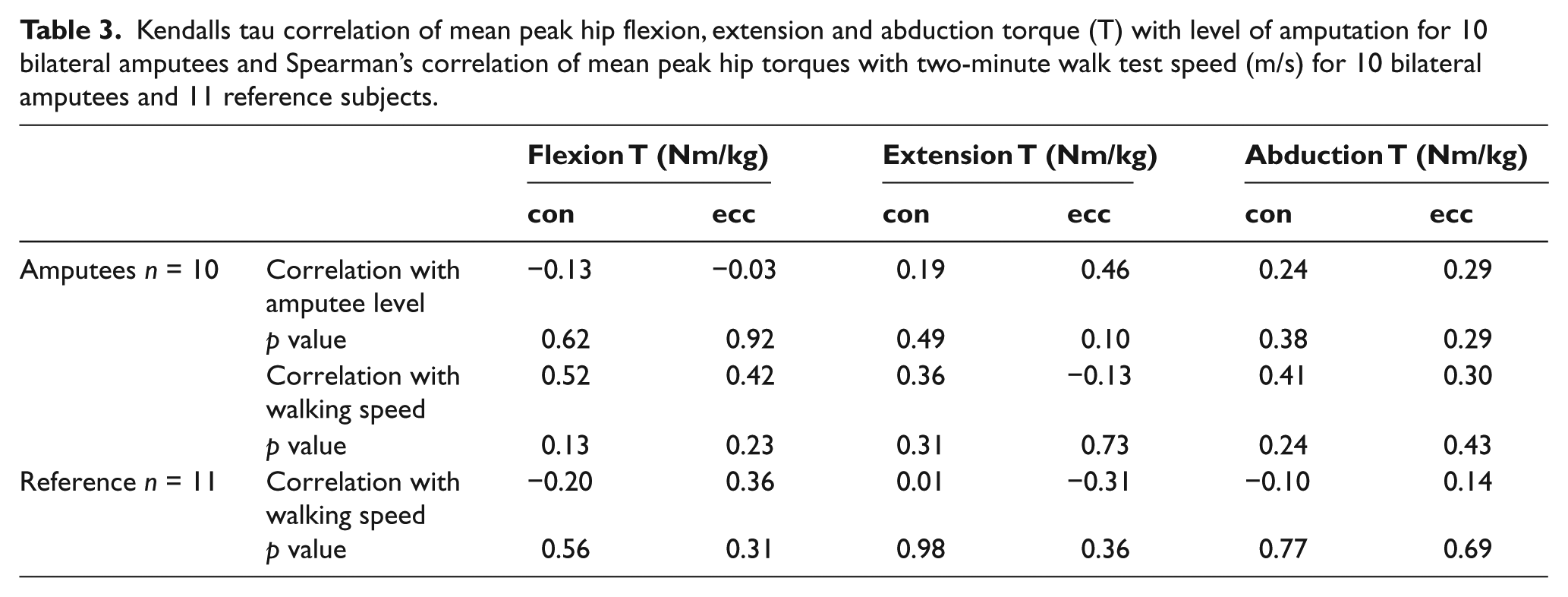
The correlations of the peak hip torques in flexion, extension and abduction with level of amputation and two-minute walk test speed, for the bilateral amputees and reference group are presented in Table 3. The peak hip torques showed no correlation with either walking speeds during the two-minute walk test or amputation level for both the amputees and the reference subjects. However, in Figure 4, a slight trend can be seen between walking speed and hip flexion strength for the bilateral amputees.
Kendalls tau correlation of mean peak hip flexion, extension and abduction torque (T) with level of amputation for 10 bilateral amputees and Spearman’s correlation of mean peak hip torques with two-minute walk test speed (m/s) for 10 bilateral amputees and 11 reference subjects.
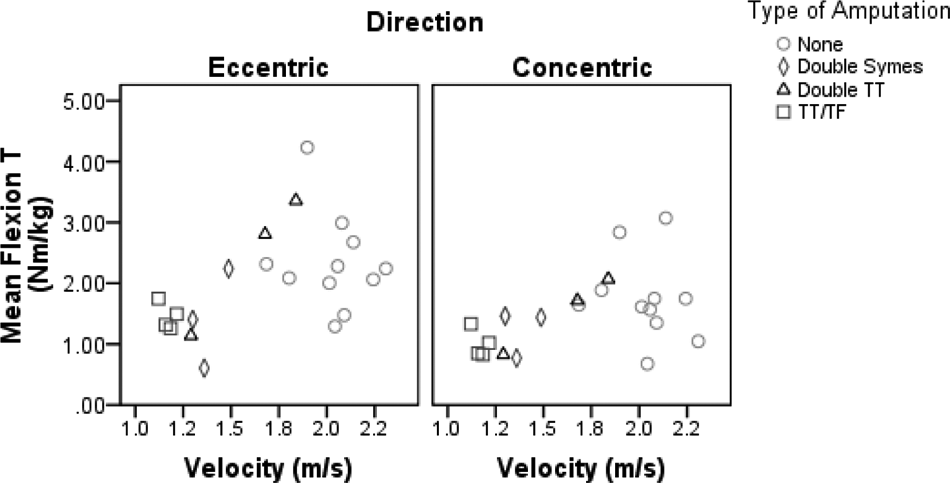
Peak eccentric and concentric hip flexion torque plotted against two-minute walk test velocity for the bilateral amputees and reference subjects (none).
Discussion
This study was the first investigation into the role of hip muscle strength in bilateral amputee mobility. Only a small number of bilateral amputees could be recruited for this study due to the limited number of bilateral amputees who manage to achieve functional walking. Even though the number of subjects was small, significant reductions were observed in bilateral amputee mobility and hip strength when compared to the able-bodied subjects. The bilateral amputees were found to walk with a slower walking velocity and increased energy costs, and their hip strength was reduced.
Walking ability
On average, the amputees walked 33% slower than the reference group in the two-minute walk test, but they had fairly similar perceived exertions and heart rate exercise intensities, resulting in an increased PCI. This supports previous findings of bilateral amputee walking.3-8 For the bilateral amputees, walking speed was negatively correlated to higher levels of amputation (kt −0.55, p = 0.044) and PCI was positively correlated to higher levels of amputation (kt 0.75, p = 0.005). These findings suggest that the more proximal the amputation, prosthetic walking becomes less energy efficient, and bilateral amputees reduce their walking speed to regulate their exercise intensity, resulting in a higher PCI, but similar exercise intensity levels. This corresponds with findings in unilateral amputee gait9,11 but has not previously been observed in bilateral amputees. From these results it may be recommended that bilateral amputees increase their overall level of cardiovascular fitness, to cope with the higher energy costs of prosthetic gait, and improve their walking speed. It may also explain why many older bilateral amputees are unsuccessful in achieving functional mobility as they have little or no potential for increasing physical fitness.
Hip muscle strength
The mean peak isokinetic hip torques are a good indicator of total hip strength. 28 For the amputee group, the peak hip torques were on average 29–34% lower than for the reference group, although most differences were not statistically significant. Since the mean differences between both groups were relatively large, the non-significant results were possibly related to the small subject number and the large variation within groups. The reduced hip strength in bilateral amputees was not expected, since bilateral amputees have been observed to increase moments and work at the hip in walking.23,24 These increased moments are most likely related to an increased use of the hip muscles, possibly to compensate for the loss of active push-off at the ankle. 24 Furthermore, for the Syme and TT amputees, in whom the hip muscles are not directly affected by the amputation. These findings could suggest that reduced hip muscle strength is a result of reduced muscle use. Bilateral amputees are generally less active than healthy people, related to the high energy cost of walking and possible discomfort. It is quite possible that the bilateral amputees in this study were fairly inactive. It may also be that hip strength in the bilateral amputees was reduced because the amputees adapted their gait and compensated for the lack of active ankle function by additional use of their upper body instead of their hip.
No significant correlation was found between hip muscle strength and level of amputation. Only two of the amputees participating in this study showed similar peak hip torques as the reference group, and these two were TT/TT amputees with the most active lifestyle of the amputee participants. This suggests again that increased activity levels for bilateral amputees are related to greater hip strength, as was previously found in sport-active unilateral amputees. 22
Despite the lack of significant correlations, a positive trend was seen between peak hip flexion and abduction torque and the walking speed in the two-minute walk test for the bilateral amputees. The data presented in Figure 4 depict that amputees who walked fastest generated the highest isokinetic hip flexion torques, but that the remaining amputees were grouped within a small range of peak hip torques and walking speeds. Interestingly, the TF/TT amputees showed higher pooled hip torques than some of the bilateral Syme or TT amputees, which may be explained by their increased reliance on the hip since they have also lost knee function in one leg. These results agree with those reported for unilateral amputees,15,16 and indicate that hip strength is an important factor in bilateral amputee walking. It is not clear, however, if the reduced walking ability of most amputees was caused by their limited hip muscle strength or that their muscle weakness was caused by their lack of everyday activity, which can be the result of other factors, such as pain or discomfort at the stump, fear of falling, or increased PCI of walking.
Interestingly, the bilateral amputee walking speed did not show a trend with increased peak hip extension torque. Since bilateral amputees do not have a healthy limb to compensate for the lack of active ankle function, they will have to use their hip muscles as the main stabiliser and actuators throughout their walking. When looking at the role of the hip extensors in the normal gait cycle, the hip extensors are known to produce active work in the early stance phase of gait. In early stance the hip is the main actuator, and it is likely that the early stance phase is not much affected by the reduced ankle (and knee) function for the bilateral amputees, and there is little increased reliance on the hip extensors. The hip flexors have, however, been found to show increased activity throughout the stance phase in unilateral amputee gait 29 which was thought to be important for additional body support in absence of the plantar-flexors of the ankle. 30 The hip abductors are mainly activated for lateral balance, which is also increasingly important if active ankle function is lost. The differences in function between the hip extensors and flexors and abductors in amputee walking may explain why mainly the hip flexor and abduction strength showed a trend with increased walking speed in bilateral amputees. A further investigation into the lower limb kinematics, kinetics and muscle activation patterns in bilateral amputee walking can give further insights into the relation of bilateral amputee hip strength and mobility.
Further research with a larger group of subjects, including more active bilateral amputees, is needed to confirm if the relationship between increased hip strength and improved mobility is significant in all, or only certain, directions. In addition, the effect of a specific training programme, targeted to improve hip strength in bilateral amputees, would confirm whether reduced mobility is the cause or effect of weak hip musculature.
Conclusion
This study was the first to investigate the factors in bilateral amputee walking ability, expressed by walking speed, perceived exertion, exercise intensity, PCI and hip strength. Even though the sample size was small, results were observed that were statistically significant or approached statistical significance.
Bilateral amputee walking ability was found to be significantly reduced compared to able-bodied walking, walking speed was slower and PCI was increased and correlated with level of amputation. Since exercise intensity in bilateral amputees was not increased, it is possible that amputees reduce their walking speed to achieve a comfortable exercise intensity level, indicating that cardiovascular fitness levels may be important in amputee walking ability.
The overall hip strength for the bilateral amputees was reduced and, even though there was no strong correlation between hip strength and walking ability, hip strength may be a key factor bilateral amputee walking, irrespective of amputation level.
Therefore, specific cardiovascular and hip strength training programmes may improve the outcomes of bilateral amputee prosthetic rehabilitation. These findings require further investigation to better understand the cause and effect relationship between hip strength and walking ability and the underlying kinematic and kinetic mechanisms.
Footnotes
Conflict of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This work was funded by a grant from Royal National Orthopaedic Hospital Special Trustees.