
Abstract
Background: Patient satisfaction is an important measurement in healthcare for administrators, clinicians and patients.
Objectives: This study investigated the role of gait deviation in patient satisfaction following lower-limb amputation and prosthesis prescription.
Study design: A cross-sectional study was done.
Methods: Twenty community-based unilateral lower-limb amputees, 12 transtibial and 8 transfemoral, were recruited from support groups. Participants completed the prosthesis evaluation questionnaire (PEQ) with embedded satisfaction-related questions, the timed-up-and-go test and the six-minute walk test, and also underwent quantitative three-dimensional analysis. Kinematic deviation was summarized using the gait profile score (GPS).
Results: Satisfaction levels were generally high (median 80 + /100). Sociodemographic variables did not correlate significantly with any of the satisfaction measures (−0.35 ≤ r ≤ 0.54). Satisfaction correlated strongly with the PEQ scales, particularly ambulation, prosthetic utility, frustration, perceived response and social burden (r ≥ 0.70). By contrast, the relationships between satisfaction and performance-based outcome measures were not significant (−0.45 ≤ r ≤ 0.43), and the GPS did not correlate with any satisfaction measures (−0.23 ≤ r ≤ 0.15).
Conclusions: In this study of high functioning amputees, gait deviation was unimportant to the amputee, while self-reported functional ability and attitudes toward the prosthesis were the strongest correlates of satisfaction following lower-limb amputation.
Introduction
Patient satisfaction is an important measurement in healthcare for administrators, healthcare providers and patients. From an administrative perspective, the primary reason to measure satisfaction is that patient satisfaction and quality of care, although distinct, are highly correlated. 1 This correlation is so well recognized that healthcare providers view satisfaction as a legitimate measure of quality of care, 2 making it a necessary component of quality management systems. 3 The measurement of satisfaction offers several benefits to both the clinician and the patient in healthcare provision. Research has shown that satisfied patients are more likely to seek medical assistance, comply with treatment and continue using medical services. 4,5 Quality of life and satisfaction can be measured by the healthcare provider, but a discord between the perception's of the healthcare provider and those of the patient may be present. 4,6 – 8 This can be overcome through the use of self-report measures. These measures capture patient perspective, which provides the clinician with an alternative opinion and aids in the prescription of necessary interventions. Further, involving the patient in the decision-making process has been shown to improve functional outcomes. 9
Satisfaction has been defined as the disparity between expectation and experience, 10 which is affected by interpersonal factors (lifestyle, previous experiences and values of the individual and the society) and variability over time. 4 For these reasons, satisfaction is difficult to quantify in a uni-dimensional index. Measures of satisfaction must be time-specific and address distinct dimensions of healthcare. 11 Whereas quality of life addresses general well-being in areas such as physical, emotional and mental health, satisfaction is a rating from the patient perspective with respect to a number of aspects of healthcare and its outcomes. Numerous generic and disease-specific measures of satisfaction have been developed to address various dimensions of healthcare provision, including physician conduct, service availability and outcomes. Popular generic instruments used to assess satisfaction with healthcare provision include the patient satisfaction questionnaire (PSQ) 12 and the client satisfaction questionnaire (CSQ). 13 Prosthetic satisfaction has been assessed using a variety of measures, such as the SAT-PRO, 14 the prosthesis evaluation questionnaire 15 and the Trinity amputation and prosthesis experience scales. 16
In an effort to streamline and optimize healthcare, interest has been focused on determining the correlates and predictors of satisfaction for both administrative and clinical purposes. However, research into correlates of satisfaction in general populations remains ambiguous, although trends exist: older persons and women tend to report high levels of satisfaction, while pre-existing health concerns also influence satisfaction levels. 5 Research into satisfaction amongst lower-limb amputees has found that satisfaction with overall performance of the prosthesis is generally high, 17 but prosthesis comfort remains a source of dissatisfaction. 18 Correlates of satisfaction in this population group include psychosocial factors (body image, social inclusion and mental health), pain in the residual and intact limbs, prosthetic utility, and self-reported physical functioning, 6,19 – 22 while demographics and level of amputation do not correlate with satisfaction.
The majority of studies investigating satisfaction amongst lower-limb amputees have relied on self-report data, that is, information obtained from the patient perspective. O’Toole et al 6 used social and clinical demographics and self-report data in conjunction with outcomes, including range of motion, muscle strength and self-selected walking speed (SSWS) to determine the correlates of patient satisfaction with progress during recovery. Lower-limb amputees comprised 28.5% (n = 132) of the total sample in this study. Of the outcomes investigated, return to work, mental health, self-reported physical functioning, SSWS and pain were most strongly correlated with satisfaction. However, the role of gait quality or gait deviation in determining patient satisfaction has not been reported.
Gait training constitutes a significant proportion of rehabilitation following prosthesis prescription. Both patient and clinician strive to minimize gait deviation in order to restore functional ability. 23 Given the attention gait training receives throughout the rehabilitation process, it seems prudent to understand the influence of gait deviation on patient satisfaction in people ambulating with a prosthetic limb. This study aimed to investigate the role of gait quality in patient satisfaction following lower-limb amputation and prosthesis prescription. Secondary analyses were performed to compare the roles of gait deviation, self-report measures and performance-based outcomes in patient satisfaction. It was hypothesized that self-reported mobility, rather than gait deviation, correlates strongly with patient satisfaction in patients with a lower-limb amputation. This study investigated patient satisfaction related to the use of a prosthesis. Patient satisfaction with healthcare was not examined.
Materials and methods
Participants
Direct mail to a number of regional and urban support groups was used to recruit 20 unilateral lower-limb amputees. Exclusion criteria were upper limb amputation, multiple amputations, lower-limb amputation at a level other than transfemoral or transtibial, less than six months of consistent prosthesis use, use of aids other than walking sticks, and cognitive disabilities. A control group of 28 able-bodied controls was recruited from a sample of convenience. Known gait pathology was an exclusion criterion, and the control group was gender-matched and similar in age and body mass index to the lower-limb amputee group. Juveniles (under 18 years) were not eligible to participate. Informed consent was obtained prior to participation in this study, which was approved by the university’s Human Research Ethics Committee (UNSW HREC 07247).
Measurements
Demographic characteristics were provided by the subjects and included age, time since amputation, level of amputation and reason for amputation.
Three-dimensional gait analysis (3DGA)
An eight-camera ViconTM 612 motion capture system (Oxford Metrics) was used to perform three-dimensional gait analysis (3DGA). Two force plates (Kistler) embedded midway along the 15 m walkway were used to detect initial contact and toe-off. Temporospatial and lower-limb kinematic data were collected for each subject.
Gait profile score and movement analysis profile
The gait profile score (GPS) is an overall summary index that quantifies the difference between pathological and able-bodied kinematic patterns. It is considered a measure of kinematic deviation, calculated using kinematic data from the pelvis, hip, knee, ankle and foot, and a higher score represents greater deviation from able-bodied gait. The GPS has proven useful in communicating overall gait patterns, differentiating between levels of impairment, and analysing the impact of clinical and surgical intervention in children with cerebral palsy. 24 Early results have shown that the GPS is also applicable for lower-limb amputees. 25
The GPS is calculated using individual elements of the movement analysis profile (MAP), designed to elucidate underlying causes of gait pathology through the provision of a score for each of the kinematic variables, for example, pelvic tilt or knee flexion/extension. Like the GPS, higher scores reflect greater deviation from able-bodied kinematic patterns.
Performance-based outcomes
Two performance-based outcomes were investigated – the timed up-and-go test (TUGT) 26 and the six-minute walk test (6MWT). Both measures provide an indication of functional ability in terms of mobility, and both have demonstrated validity for use with lower-limb amputees. 27,28
Self-reported outcomes
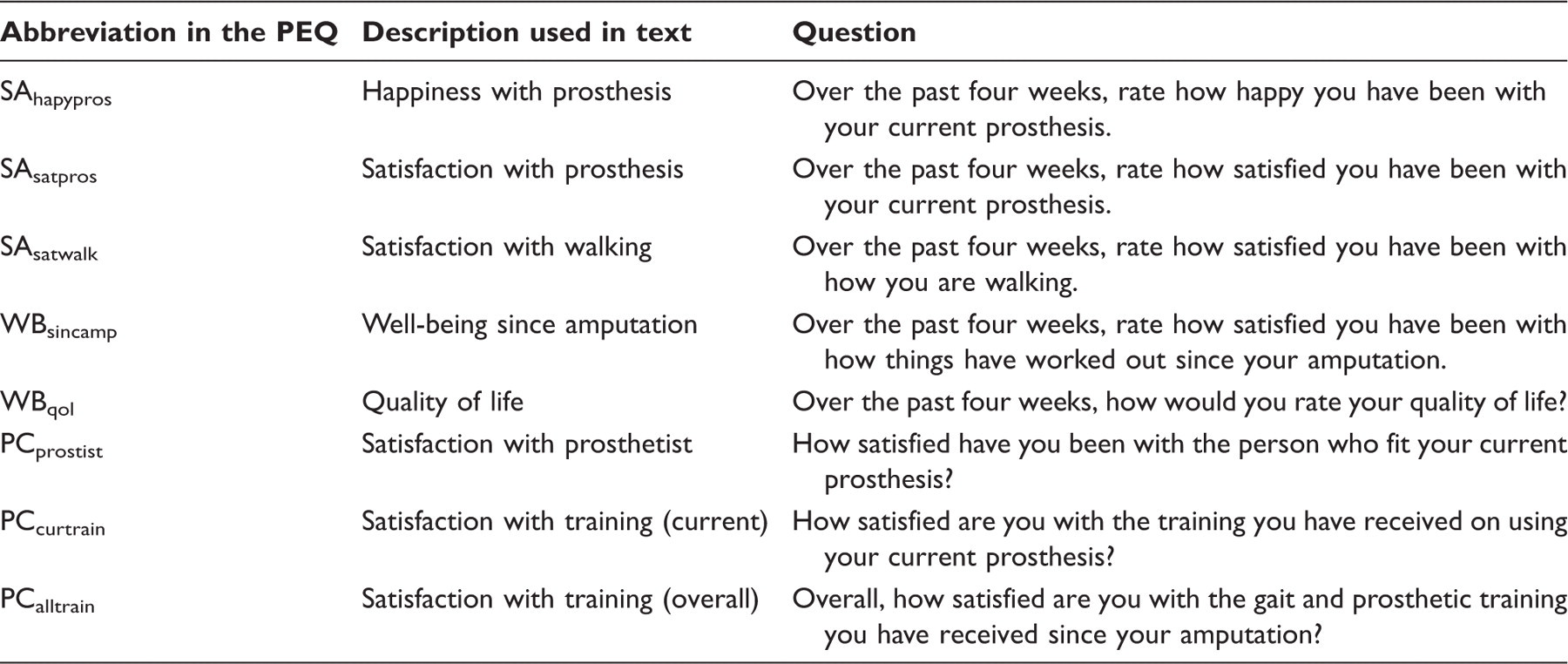
Self-reported outcomes were measured using the prosthesis evaluation questionnaire (PEQ). The PEQ is an amputee-specific measure designed to address prosthesis-related quality of life. 15 It consists of nine subscales and additional individual questions, all of which were utilized in this study.
Satisfaction measures
Satisfaction questions contained in the PEQ.
Procedure
Lower-limb amputee participants first underwent 3DGA wearing their everyday prosthesis (with shoes) and using regular walking aids (if normally used). Subjects were dressed in shorts, a vest and low cut socks (with shoes) throughout data capture. Markers were placed according to a modified Helen Hayes marker set 29 with additional markers placed over the anterior portion of the pelvis to address anterior pelvic marker drop-out during gait in overweight subjects. 30 Subjects were asked to walk 15 m at a comfortable, self-selected walking speed, and data were collected for six trials. Following 3DGA, participants completed the TUGT, which was performed as described in the literature. 26 Participants were permitted practice tests prior to data collection. Data were collected for three trials. The test protocol concluded with the 6MWT, which was conducted as described in the literature. 31 Participants were asked to complete the PEQ in rest periods through the test protocol. The able-bodied participants completed 3DGA as described for the lower-limb amputee group while also wearing shoes.
Data analysis
Lower-limb kinematics were calculated using the Plug-In-Gait model (Vicon, Oxford Metrics), which was also used to calculate step length and walking speed. Self-selected walking speed and average step length were normalized against average leg length. The MAP and GPS were calculated as described by Baker et al 32 for each limb, and the average of the prosthetic and intact limbs were used in subsequent analyses. Able-bodied data, derived from the control group, were used to calculate the gait summary measures for each of the lower-limb amputee subjects. The three TUGTs were averaged and the mean value used in further statistical analyses.
Normality of data was assessed using the Anderson-Darling test. In general, data did not conform to a normal distribution, which necessitated the use of nonparametric statistical analyses. Differences between levels of amputation were determined using the Mann-Whitney U-test, with p ≤ 0.05 considered significant. Relationships between the satisfaction measures and continuous variables were investigated using the Spearman’s rank correlation coefficient. Point-biserial correlation coefficients were used to analyse relationships between the satisfaction measures and binary variables, such as level of amputation and gender. Significance levels for correlation coefficients were set at p ≤ 0.001 or |r| ≥ 0.70. 33,34 Correlation coefficients were deemed strong if significant, moderate if 0.57 ≤ |r| < 0.70 (0.01 ≤ p < 0.001) and small if 0.45 ≤ |r| < 0.57 (0.05 ≤ p < 0.01). For correlations between satisfaction measures and overall gait deviation (measured using the gait profile score), 95% confidence intervals were calculated for the correlation coefficient. 34 All tests were performed using Minitab 15 (Minitab® Statistical Software).
Results
Participant characteristics
Participant characteristics.
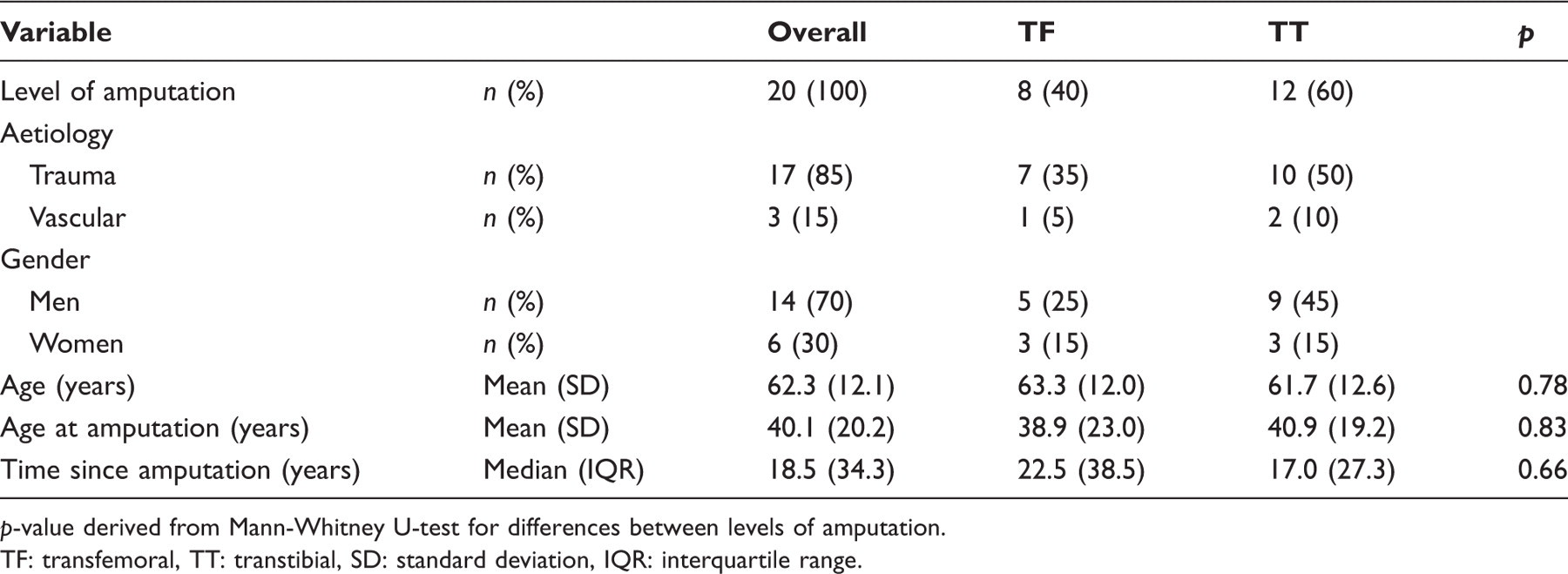
p-value derived from Mann-Whitney U-test for differences between levels of amputation.
TF: transfemoral, TT: transtibial, SD: standard deviation, IQR: interquartile range.
Outcome measures
Summary of results.
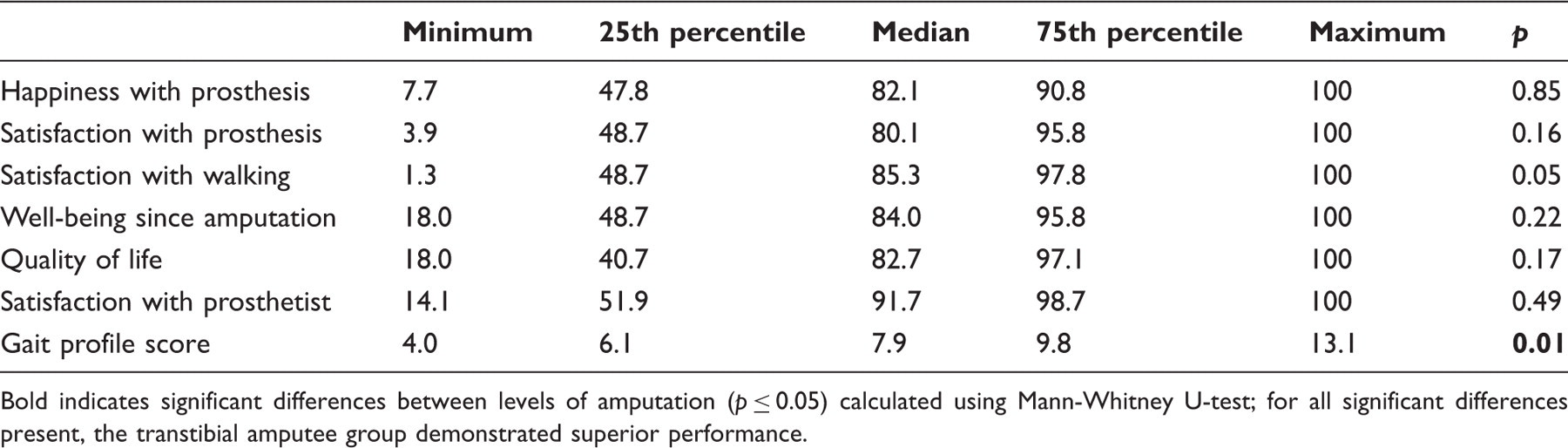
Bold indicates significant differences between levels of amputation (p ≤ 0.05) calculated using Mann-Whitney U-test; for all significant differences present, the transtibial amputee group demonstrated superior performance.
The prosthesis evaluation questionnaire demonstrated a wide range of responses, with many scales recording the highest possible score (100). Median scores were generally similar across the scales, with the exception of perceived response and social burden, with both recording substantially higher scores than the other scales. All performance-based measures exhibited a wide range of functional abilities amongst the lower-limb amputees in this study. This result was reinforced by the outcomes of gait analysis, where a wide range of gait patterns were observed and measured by the MAP and GPS. Results for these measures can be found in the supplementary material appendix.
Correlates of satisfaction
Spearman’s rank correlation coefficient relating satisfaction measures to demographics and functional outcome measures.
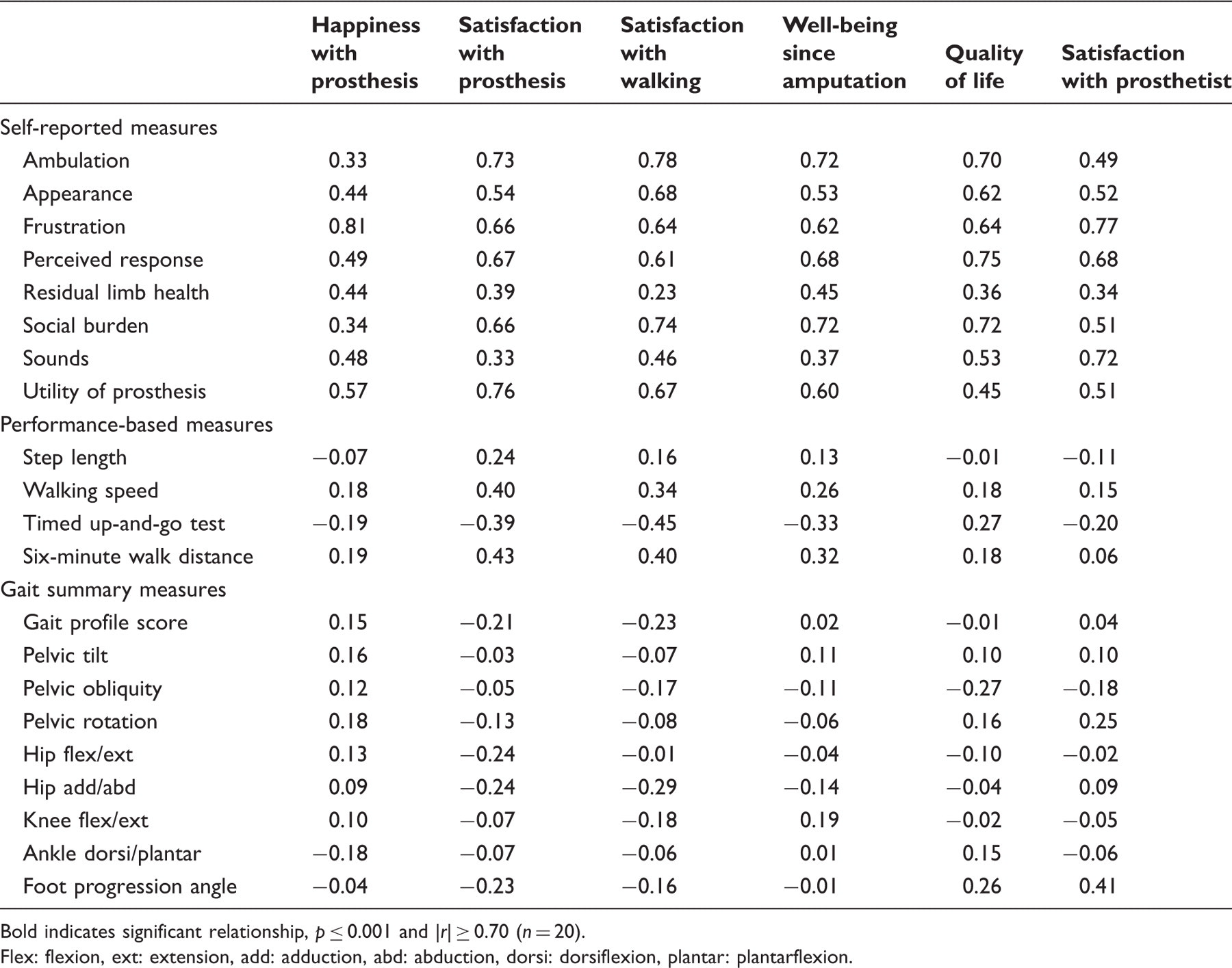
Bold indicates significant relationship, p ≤ 0.001 and |r| ≥ 0.70 (n = 20).
Flex: flexion, ext: extension, add: adduction, abd: abduction, dorsi: dorsiflexion, plantar: plantarflexion.
The 95% confidence intervals for Spearman’s rho between satisfaction measures and overall gait deviation.
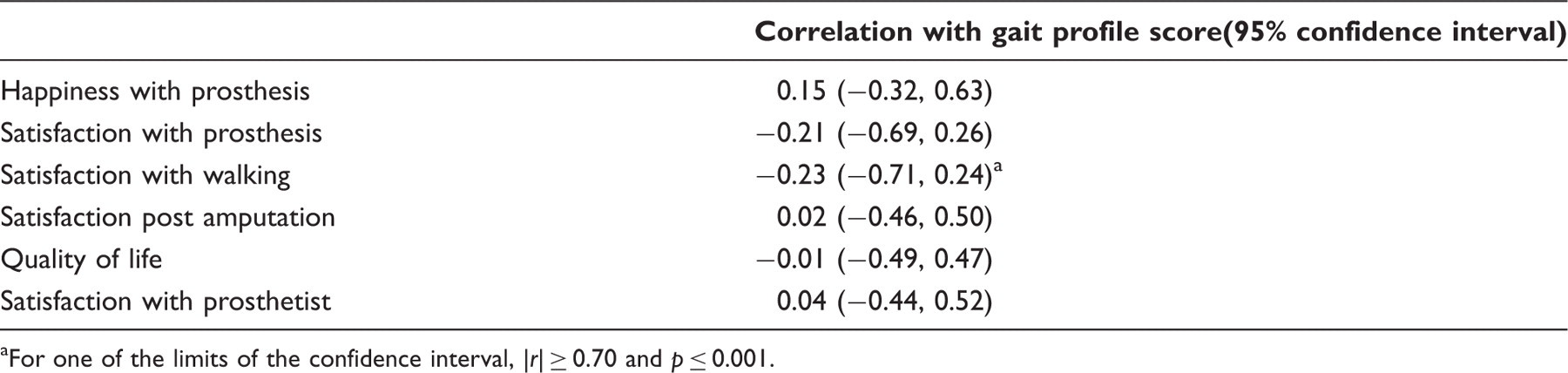
For one of the limits of the confidence interval, |r| ≥ 0.70 and p ≤ 0.001.
Discussion
Satisfaction is neither constant nor concrete. Defining and measuring satisfaction is complicated by interpersonal and over-time variability, 4 and therefore any instrument developed to quantify satisfaction must be both activity- and time-specific. 1 The questions relating to satisfaction contained in the PEQ meet these criteria. Questions generally begin with “over the past four weeks” and address particular aspects of the prosthesis and life with the prosthesis. Further, the PEQ has been validated for use as a QOL instrument with lower-limb amputees. 15
The strongest correlates of satisfaction were the scales in the PEQ self-report instrument (Table 4), which were related to functional ability, frustration, prosthetic utility, social burden and perceived response from family and friends. This is in concordance with previous research, which found satisfaction to be related to self-reported physical functioning, 6,20 comfort, function and appearance of the prosthesis, 20,22 and to social factors such as return to work and burdensomeness on family and friends. 6,20,22 Pain was also found to correlate strongly with satisfaction, 6,19,20,22 but was not examined in this research.
No significant relationships were detected between satisfaction and performance-based measures assessing functional ability. O’Toole et al 6 found that self-selected walking speed correlated with satisfaction, but this was not reproduced in this work for a number of reasons. Firstly, O’Toole et al asked participants about their satisfaction with the recovery progress. The questions used in this study addressed satisfaction with prostheses and walking, as well as general QOL questions. Secondly, the sample size in this study was substantially smaller and consisted of only persons with unilateral transtibial and transfemoral amputations. The sample group investigated by O’Toole et al was large and composed primarily of patients with traumatic leg injuries (71.5%). Individuals with lower-limb amputation constituted only 28.5% of the sample. Further, O’Toole et al investigated satisfaction at 24 months post injury, while in this study the time since amputation was not controlled.
In this study, gait summary measures did not correlate significantly with satisfaction measures (Table 4). Only the correlation between gait deviation and satisfaction with walking reached significance at the limit (upper or lower) of the 95% confidence interval. Thus, in this cohort of relatively high functioning amputees, it can be speculated that gait deviation was unimportant compared to self-reported functional ability in determining patient satisfaction. Functional ability requires the physical, social and mental ability to perform activities of daily living, and therefore rehabilitation following prosthesis prescription must focus not only on mobility, but also on rehabilitation in other health domains, as has been advocated for several decades. 35 Maximizing satisfaction requires the refocusing of amputee opinion on their own functional ability, importantly, promoting patient independence and social acceptance of limb loss by patients as well as family and friends. The correlation, although non-significant, between time since amputation and satisfaction measures demonstrates that this occurs naturally (to an extent) over time, probably due to a response shift and acceptance of the amputation. Resolution of acute injuries and comorbidities, particularly amongst traumatic amputees, may also contribute to this finding. However, the results of this study indicate that it may be possible to maximize satisfaction sooner after amputation through appropriate prosthetic and social interventions. a view supported by previous research investigating perceived results of amputation. 20
Satisfaction can be defined as the degree to which experience meets expectation. Given the relationship between functional ability and satisfaction shown in this study, it appears important that patients enter rehabilitation with an appreciation of the process and an awareness of potential obstacles. Setting realistic and achievable goals seems imperative to avoid a disparity between expectation and experience, and thus improve satisfaction levels. Additionally, patients are more likely to adhere to and be motivated by a programme with realistic goals, 36 thus beginning the cycle of greater achievement and therefore higher levels of satisfaction.
Study limitations
Statistical analyses were limited by the small sample size utilized in this study. The sample was not heterogeneous, nor was it representative of the general amputee population. The inclusion criteria set for this study required participants to be unilateral amputees at the transfemoral or transtibial level, and the majority of subjects had lost a limb as a result of a traumatic event. This study considered only prosthetic users and did not assess comorbidities. Further, functional ability amongst participants in the sample was generally high, probably due to the large proportion of traumatic amputees 37 and the exclusion criteria set for this study – individuals who required aids other than walking sticks were not eligible to participate. Satisfaction levels were generally high amongst the sample group, which may have been a reflection of the high functional levels of the participants. Increasing sample size and heterogeneity would provide insights into the satisfaction levels of people with an amputation for reasons other than trauma, and enable generalizations about patient satisfaction following lower-limb amputation.
Gait deviation was quantified using gait summary measures. These types of measures cannot and do not substitute for complete quantitative gait analysis. Instead, gait summary measures provide a convenient means of communicating overall gait pathology. The MAP and GPS were developed for use with children with cerebral palsy, but have been shown appropriate for use with lower-limb amputees. 25 Although the MAP and GPS do not summarize gait in its entirety (indeed, they consider only kinematics and neglect kinetics), they provide a practical summary of overall gait pathology, making a useful measure for this study.
Correlation coefficients do not prove cause and effect, and the vast number of relationships investigated in this study may have revealed correlations by chance. However, strict significance criteria for the correlation coefficients were set (p ≤ 0.001) to exclude any coincidental findings. Moreover, correlations in this study are sensible for each of the satisfaction measures.
Conclusions
Gait deviation did not correlate significantly with any of the satisfaction measures examined in this study, nor did demographic variables or objective indicators of functional ability. The strongest correlates of patient satisfaction were derived from the scales contained in the self-report questionnaire. In this cohort of relatively high functioning amputees, gait deviation was relatively unimportant to the amputee. Self-reported functional ability in a variety of areas (including physical, mental and social domains) had the greatest influence on patient satisfaction. Attention should therefore be paid to physical, mental and social functioning throughout the rehabilitation process following lower-limb amputation.
Footnotes
Acknowledgements
The authors would like to acknowledge the Amputee Association of NSW Inc. and its affiliated branches for assistance with recruitment; Deborah Vickers for her role in data collection; and Timothy Bach and staff members from La Trobe University for their assistance in project conception.
Funding
Although Kark was in receipt of an Australian Postgraduate Award at the time the research was conducted, this research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
The authors alone are responsible for the content and writing of the paper, and report no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.