
Abstract
Background:
Orthotic treatment for adolescent idiopathic scoliosis is a mainstay in nonoperative treatment to prevent progressive spinal deformity.
Objective:
To determine the effectiveness of the Providence orthosis in the treatment of adolescent idiopathic scoliosis.
Study design:
Retrospective review.
Methods:
Patients treated with a Providence orthosis for adolescent idiopathic scoliosis were reviewed. Inclusion criteria included the following: age of 10–18 years; curve magnitude of 25°–40°; Risser stage of 0–2; and, if female, <1 year post menarche at the time of brace initiation. Failure was defined as curve magnitudes progressing >5° or to >45° or surgery. Radiographs and clinical information were recorded and compared between treatment success and failure cohorts.
Results:
56 patients (51 female and 5 male; average of 12.26 years) were identified with average of 2.21-year follow-up and a 57.1% success rate for preventing curve progression. Factors associated with successful treatment included curve apex T10 and caudal and Risser sign ⩾ 1. Multivariate analysis identified Risser ⩾ 1 and curve apex T10 and caudal as independent predictors of successful treatment.
Conclusion:
The Providence nighttime orthosis can be an effective treatment for adolescent idiopathic scoliosis. Curve Apex at T10 or caudal was an independent predictors of treatment success.
Clinical relevance
This study identifies variables associated with treatment success using the Providence nighttime orthosis in a consecutive series of adolescent idiopathic scoliosis patients. This information provides the foundation for identifying ideal patients for nighttime bracing to guide clinical treatment.
Background
Adolescent idiopathic scoliosis (AIS) is a common condition present in 0.5%–3.0% of children between 10 and 16 years of age and accounting for the majority of spinal deformity cases in the adolescent population.1–3 Of these cases, only a minority has been found to progress with skeletal maturity, with surgery being recommended to prevent the progression of deformity. 4 Findings in large population samples have identified large curve magnitude, skeletal immaturity, and double curve patterns as factors associated with increased risk of progression.4,5 Lonstein and Carlson 5 found that skeletally immature patients (Risser 0 or 1) with curves 20°–29° who were not treated had a 68% risk of curve progression.
Spinal orthoses play a significant role in the treatment of AIS. The goal of orthotic treatment is to alter the natural history of the patient’s spinal deformity, specifically, to prevent curve progression in children where progression has been observed or in children identified as at-risk for progression. 6 The Bracing in Adolescent Idiopathic Scoliosis Trial (BrAIST) study performed a prospective, randomized control trial to assess the effectiveness of a thoracolumbosacral orthosis (TLSO) in the treatment of AIS, finding a 58% rate of curve progression >50° for children in the observational cohort, in comparison to a 93% success rate for children who wore their TLSO a minimum of 12.9 h per day. 7
Despite wide acceptance of bracing as a successful treatment option for AIS, orthosis treatment is difficult to scientifically analyze, 8 especially when considering the many different brace designs. The Providence TLSO, originally described by D’Amato et al., 9 is a nighttime orthosis that applies derotational and translational forces to reduce the spinal curvature while the orthosis is donned. Although a commonly used orthosis, there is limited and conflicting literature regarding the efficacy and indications for the Providence TLSO.9–15
The purpose of this study is to determine the effectiveness of the Providence TLSO in the treatment of AIS. We hypothesized that the Providence TLSO would be effective at altering the natural history of scoliosis.
Methods
After approval by the Institutional Review Board, a retrospective intention to treat analysis of adolescent patients treated with a Providence TLSO between February 2008 and November 2011 at a tertiary care referral center was performed. All patients who received a Providence TLSO were considered for inclusion in this study. Patients were instructed to wear the brace for 8–10 h each day, while sleeping. Inclusion criteria were selected based on the Scoliosis Research Society (SRS) guidelines and included the following: patient age of 10–18 years; curve magnitude of 25°–40°; Risser stage of 0–2; and, if female, <1 year post menarche at the time of brace initiation. 16 For identified patients, demographic and clinical information was recorded (Table 1).
Summary of recorded demographic and clinical variables for study analysis.
Radiographs were reviewed at three time-points: initial, pre-brace presentation; in-brace; and final follow-up after brace discontinuation. Radiographs were reviewed by a certified orthotist and a pediatric orthopedic surgeon and assessed with the measurement of curve magnitude according to the Cobb method and SRS classification of curve type and Risser sign. In-brace correction was recorded as a percent of curve correction. If a subject presented with more than one initial curve, data was recorded for each individual curve. For subjects with more than one curve, the primary curve was identified as the curve with the largest initial magnitude and a double curve pattern was defined as two curves with magnitudes within 5° of one another. 17 All other curve patterns were categorized as single thoracic, single thoracolumbar (apex T12 or L1), or single lumbar. Thoracolumbar and lumbar curve were combined and analyzed as one group secondary to sample size.
Success of bracing treatment was defined according to SRS recommendations as ⩽5° of curve progression and/or curve progression to <45° when comparing initial curve magnitude to the latest available follow-up after brace discontinuation. 16 Conversely, failure was defined as >5° of curve progression and/or curve progression to >45° or surgery. 16 All subjects with intent to treat were studied, regardless of stated compliance during treatment. The Providence TLSOs were fabricated by Spinal Technology, Inc. (West Yarmouth, MA, USA), using the principles as described by D’Amato et al. 9 Each orthosis was designed and fit by a certified orthotist with radiographs obtained after fitting to ensure appropriate fabrication.
Statistical analyses were performed using SAS 9.2 (Cary, NC, USA) or R version 3.3.1 (r-project.org). Descriptive statistics were calculated for all variables of interest. Recorded variables were assessed for association with bracing treatment success. Paired t-tests were used to compare continuous measurements (e.g. primary curve degree and in-brace correction), and chi-square analyses were for categorical variables (e.g. gender, Risser sign, and location of curve). Identified variables were then assessed in a multivariate logistical regression analysis to identify factors predictive of treatment success. Statistical significance was pre-determined at 0.05.
Results
Of the 323 patients presenting for scoliosis examination over the study period, of which 252 had at least one exclusionary criteria (18 with prior surgery, 21 with curve magnitudes of 25° or less, 3 curve magnitudes > 40°, 37 previous brace treatment, 32 with a neuromuscular diagnosis, and 144 with Risser stage >2 or >1 year post menarchal). The remaining 68 patients were prescribed a Providence TLSO for the treatment of AIS, with 12 having insufficient follow-up leaving a total of 56 patients (51 female and 5 male; average age of 12.26 ± 1.45 years) who met inclusion criteria.
At the time of brace initiation 43 (72.8%) of the female subjects were pre-menarche and 16 (27.1%) were post-menarche, with 77.9% (N = 46) of all patients being classified at Risser 0. The average initial curve magnitude was 29.89° (±4.63°; range of 25°–39°) with 49 (87.5%) between 25° and 35°, and 7 (12.9%) >35°. SRS curve pattern distribution consisted of 21 single thoracic curves, 23 single lumbar or thoracolumbar, and 12 double major curves.
Patients were followed for an average of 2.21 years from brace initiation and were treated for an average of 730 days (410–908 days) in the Providence orthosis with an average follow-up of 725 days from brace initiation and 229 days after brace discontinuation. The overall success rate of the Providence orthosis in preventing curve progression > 5° was 51.78% (N = 29), with a 57.1% (N = 32) success rate at preventing progression > 45° or surgery.
A summary of potential predictive variables for treatment success with the Providence brace is listed in Table 2. Clinical differences were present for treatment success, defined for as both curve progression > 5° or magnitude > 45° and/or surgery, with male gender, Risser 0, and curve apex cephalad to T10 having higher failure rates. Curve magnitude > 35° (70% failure vs 40.8%) and pre-menarchal status at brace initiation (45% failure vs 23%) had a higher rate of treatment failure, defined as curve magnitude > 45° and/or surgery. However, univariate analysis for treatment success, defined as curve progression <5°, identified only Risser ⩾ 1 (78.6% vs Risser 0: 40.0%, p = 0.012). When defined as magnitude ⩽ 45° or surgery, univariate analysis only identified curve apex at T10 or caudal (69.4% vs 40.6%, p = 0.0103) as significantly associated with treatment success. In-brace correction did not significantly affect curve progression > 45° or surgery (88.3% in-brace correction for treatment success vs 80.5% correction in treatment failure cohort, p = 0.19).
Summary of univariate analyses for identified variables and treatment success with the Providence brace for AIS.
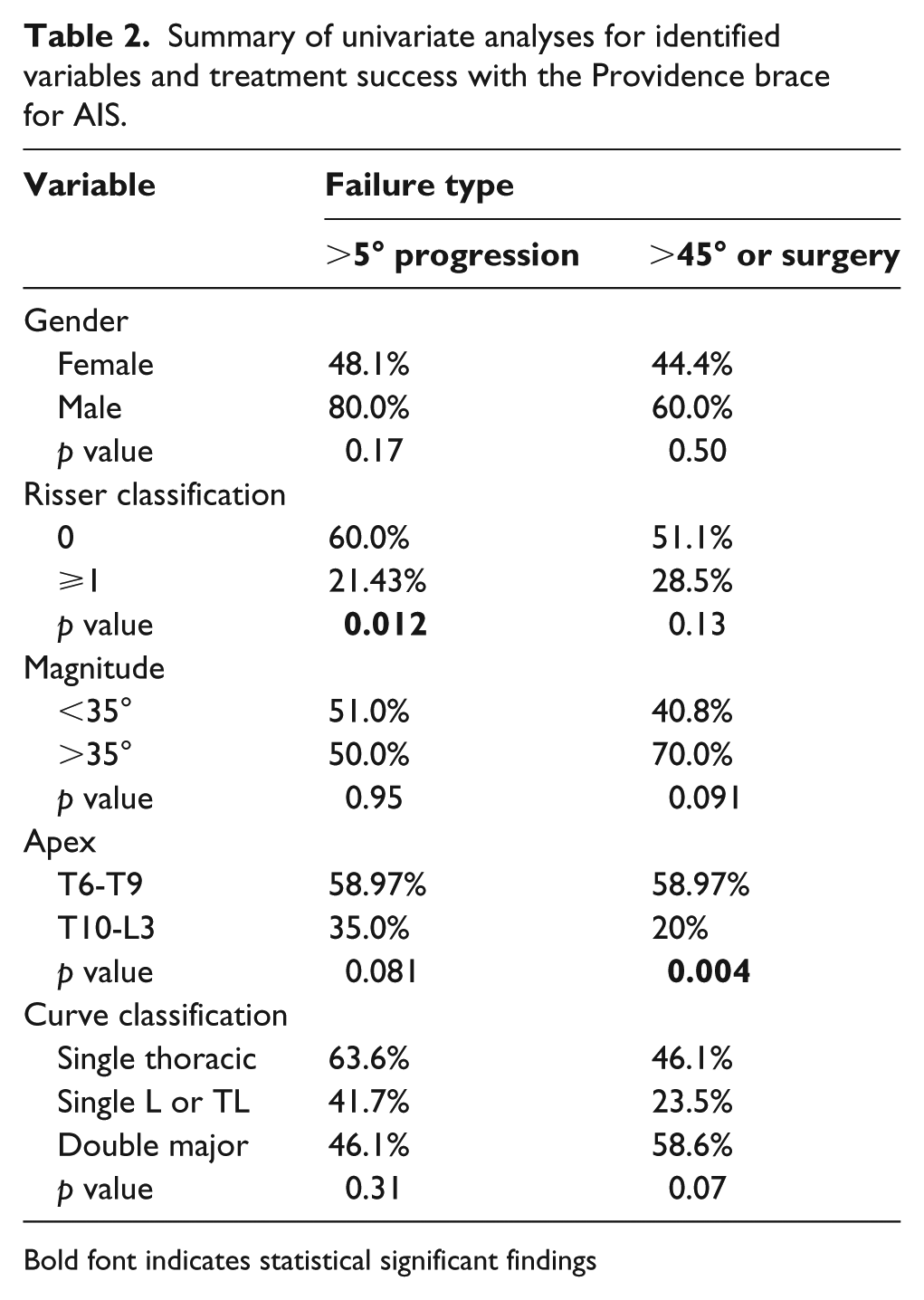
Bold font indicates statistical significant findings
When combining Risser ⩾ 1, initial curve magnitude < 35°, and curve apex T10 and caudal, treatment success—defined as curve progression < 5°—reached 100% for children when all three variables were present, 64% for 2/3 variables, 25% with only 1 variable present, and 0% if none were present. For treatment success defined as curve magnitude < 45°, 100% of children met success when all three variables were present, 75% if 2/3 variables were present, 29.1% with only 1 present, and 0% with no variables.
Entering Risser classification (0 or ⩾1), curve classification, curve magnitude (<35° or ⩾35°), curve apex (T9 and above or T10 and below), and patient age into a multivariate logistic regression analysis identified curve apex as an independent predictive variable for treatment success, defined as curve magnitude < 45° and/or surgery with decreased odds of failure of 0.21 for curve apex T10 or caudal (95% confidence interval (CI): 0.06–0.75, p = 0.016). For treatment success defined as curve progression < 5°, only Risser ⩾ 1 was predictive of treatment success with a decreased odds of failure of 0.17 (95% CI: 0.04–0.70, p = 0.0138).
Discussion
Orthosis treatment for AIS is the standard of care in an attempt to abate or slow the progression of curve magnitude. Despite this acceptance in the literature, there remain several types of orthoses without a clear acceptance as to which orthosis is superior.9,12,13,18–20 Using a Providence nighttime orthosis for consecutive patients presented with previously untreated AIS, we found a 51.78% overall success rate of in preventing curve progression > 5°, with a 57.1% success rate at preventing progression to > 45° or surgery.
Weinstein et al. 7 established bracing as the standard of care for treatment of AIS. Their prospective randomized control trial was prematurely halted due to the overwhelming success of bracing in preventing the progression to surgery in comparison to observation. 7 Subsequent studies have mirrored these results, finding the need to treat three patients in order to prevent progression to surgery. 21 The amount of brace wear is strongly correlated with the rate of success6,15,22–24 and can be maximized with the utilization of compliance monitors combined with patient counseling. 22
Nighttime orthoses were designed with the ability to ensure brace compliance while mitigating the negative effects of brace wear on quality of life without compromising the overall effectiveness of brace treatment. 15 Finite element analyses have shown that nighttime bracing takes advantage of the positive effects of supine positioning on coronal curve with the addition of a bending moment which places a rebalancing of pressures across the vertebral physes that may reduce asymmetric growth. 25 In addition, it is theorized that by harnessing the enhanced output of growth hormones released during sleep combined with improved compliance, brace wear can contribute to success of nocturnal bracing. 26
The Charleston nocturnal orthosis represented the first generation of nocturnal orthosis and was identified as an option for patients presenting by curve magnitude < 35°. 27 Since the introduction of the Providence orthosis in 2001, several studies have reported on the clinical outcomes of treatment in adolescent patients. These studies have shown an overall success rate in preventing >5° curve progression between 31% and 74%.9,11,13,15 Our results align with these previous studies, reporting a 51.78% success rate in preventing >5° curve progression and 57.1% success rate at preventing progression to > 45° or surgery. In addition, curve apex has been shown to impact success rates, with curve apices below T8 having a 79% success rate. 9 This finding is reinforced in the current series with patients whose curve apex is at T10 or caudal having significantly higher treatment success rate at preventing curve progression > 45° or surgery (80% vs 41.0%).
Several studies have compared the results of the Providence orthosis with other bracing options. Yrjonen et al. 15 performed a matched cohort comparison of the Providence nocturnal brace with full-time Boston TLSO bracing in patients with AIS and a curve apex below T10. They found at average in-brace correction of 92% with a 73% success rate in preventing curve progression > 5° compared with a 50% in-brace correction in the Boston brace cohort with a 78% success rate. Janicki et al. 13 performed a similar comparison of previous untreated AIS patients, without a restriction based on curve apex. Although reporting much lower success rates than in previous studies, the Providence orthosis was more effective in avoiding surgery and preventing curve progression (31% vs 15%).
Several additional factors have been associated in the literature with treatment success of AIS. Skeletal maturity has a significant effect on the risk of curve progression. Risser sign ⩾ 1 and curve apex at T10 or caudal were associated with bracing success in the current series with both factors identified as independent predictors of successful treatment. Lonstein and Carlson 5 identified presenting curve magnitude, Risser stage, and patient chronological age as significant factors associated with curve progression, with Risser stage and age used as proxies for skeletal maturity. In addition to Risser stage, open triradiate cartilage, 24 Sanders maturity stage, 28 and pubertal status 29 have all been identified as factors associated with bracing success.
These results must be viewed with attention to their limitations. As a retrospective review, this study has certain, inherent limitations and as a single center, a tertiary care center with a geographic referral base, the reported results may not extrapolate to all patient populations. Compliance with bracing is a significant factor that can influence the effectiveness of bracing in preventing curve progression.7,21–23 Given the lack of compliance monitors, we are unable to determine the exact amount of time each patient spent wearing the brace and if the amount of time in the brace correlated with the success of treatment. It can be assumed, based upon previous compliance studies, that the brace was worn less often than the prescribed wear time.7,23 The small sample size also limits the interpretation of the presented data. Several variables demonstrated clinically significant differences with regard to treatment success (gender, Risser stage, curve magnitude, and menarchal status); however, these differences were not statistically significant which could reflect an underpowered study. In addition, patients were not all followed to skeletal maturity which could have a significant effect on the rate of treatment success as there may be an even higher rate of failure as the patients are followed.
Conclusion
In conclusion, curve apex at T10 or caudal and Risser stage ⩾ 1 were independent predictive factors of treatment success. These data suggest that nighttime bracing with the Providence brace may be ideal for adolescent patients with a curve apex at T10 or caudal who are beyond Risser stage 0. However, further research in the form of a prospective clinical study incorporating compliance monitors is needed to further evaluate the efficacy of the Providence TLSO.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.