
Abstract
Background:
Osteoporosis is one of the major health problems in aging population and may lead to osteoporotic vertebral fracture that causes severe back pain and reduced functional independency.
Objectives:
To compare the efficacy of SpinoMed® and soft lumbar orthosis at the subacute stage (the second and third weeks of disease onset) of the patients with osteoporotic vertebral fracture.
Study design:
Prospective randomized trial, pilot trial.
Methods:
A total of 51 female subjects aged 55 years or above with osteoporotic vertebral fracture were randomly distributed to the soft lumbar orthosis (control group, n = 24) and SpinoMed® (test group, n = 27) groups after the acute stage (the first week of disease onset). The pain level was assessed by obtaining verbally feedback in 10-point scale scoring, while functional mobility level was estimated with Functional Independence Measure-motor Scores, Elderly Mobility Scale, and Modified Functional Ambulation Category. The thoracic kyphosis angle was measured from standing X-ray on 10 out of 51 subjects.
Results and Conclusion:
Both groups showed significant reduction in the patients’ pain level and limitations of daily life (p < 0.05). The effect of the two types of spinal orthoses on the pain level reduction and functional mobility level gain did not show significant difference (p > 0.05) at the subacute stage.
Clinical relevance
In this study, SpinoMed® could not provide additional treatment benefits to patients with osteoporotic vertebral fracture regarding pain relief and functional independence improvement at the subacute stage. The effects of SpinoMed® in muscle-strengthening and thoracic kyphotic angle reduction for patients with osteoporotic vertebral fracture need to be further verified in a more intensive and longer-term training program.
Background
Osteoporosis is one of the major health problems in the aging population and may result in osteoporotic vertebral fracture (OVF) that could cause severe back pain and reduced functional independency. The incidence of OVF is rising rapidly with aging. 1 OVF could cause hyperkyphosis and nerve compression resulting in acute and chronic back pain and increased risk of falling and further vertebral fractures. In addition, spinal osteoporosis may be associated with limitations in daily activities and emotional problems related to cosmetic appearance.2,3 It was estimated that about one-fourth of the women aged above 50 years suffer from at least one vertebral fracture. 4
Currently, there is no standardized treatment protocol for patients presented with OVF. The majority of patients will be managed with a conservative approach; surgical intervention is only feasible in a minority of cases.5,6 Osteoporosis might be partly alleviated by pharmaceutical interventions including alendronate, 7 risedronate, 8 and raloxifene 9 via improving bone quality. Together with the decline of bone mineral density of the spine, the back muscle atrophy could also contribute to the increment in kyphosis.10,11 Therefore, strengthening exercises for back muscles over spinal orthoses could play an active role in the management.
Spinal orthoses have been traditionally used in the management of thoracolumbar fractures treated with or without surgical stabilization. Spinal orthosis may help to improve spinal alignment, increase intra-abdominal pressure with improved load distribution on the spine, and facilitate muscular strengthening. It could offer an efficacious non-pharmaceutical treatment option for spinal osteoporosis and provide a better quality of life achieved through pain reduction, decreased limitations of daily living, and improved overall well-being. Currently, in our practice, rigid thoracolumbosacral orthosis (TLSO) is used for elderly with OVF at the acute stage (the first week of disease onset), while soft lumbar orthosis is used at the subacute stage (the second and third weeks of disease onset). Unfortunately, the use of this external support in osteoporosis is limited by factors such as atrophy of trunk muscles and restricted respiration, leading to low compliances.12,13 In summary, the conventional orthoses have the following limitations: uncomfortable, unappealing appearance, poor compliance, prolonged use, weakening of spinal muscles, and poor outcomes.
Given the limitations of currently available orthoses, a new orthosis named SpinoMed® (Medi Bayreuth, Bayreuth, Germany) has been developed. Elderly wearing this orthosis can continue their daily activities and remain active and functioning in the orthosis. Pfeifer et al. 14 in a randomized controlled study showed that the use of the SpinoMed® could increase trunk muscle strength and thus improves posture in elderly with OVF resulting in a better quality of life. The SpinoMed® was found to be effective to improve balance in the elderly with thoracic hyperkyphosis, 15 and it was suggested as a supplement to traditional back-strengthening exercises. 16
This study aims to compare the efficacy of “SpinoMed®” and soft lumbar orthosis in patients with OVF at the subacute stage.
Methods
Subjects
Subject inclusion criteria are as follows: (1) age: 55 years or above, (2) female, (3) clinical diagnosis of OVF with radiographs, (4) back pain secondary to OVF, and (5) affected vertebrae between T1 and L5. Subject exclusion criteria are as follows: (1) premorbid: bed-bound, (2) previous spine surgery, (3) vertebral collapse with underlying pathology (e.g. multiple myeloma and metastasis), (4) dementia/cognitive impairment, (5) patients with neurological deficits secondary to osteoporotic fracture, and (6) severe degenerative change of spine such as osteoarthritis and scoliosis.
Ethical approval for the current research study was obtained from the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (CREC). Informed consent forms were obtained from all subjects involved in this research study. All the recruited subjects were randomly assigned to either the SpinoMed® group (test group) or the soft lumbar orthosis group (control group).
Orthoses application
All subjects were prescribed to wear the custom-molded rigid TLSO in the acute stage (the first week of disease onset) for 24 h a day. At the subacute stage (the second and third weeks of disease onset), the subjects of the test group were requested to wear the SpinoMed® orthosis 3 h daily during rehabilitation training and then wore the soft lumbar orthosis for the rest of the time, while the subjects of the control group were prescribed with soft lumbar orthosis. The corresponding orthoses were applied onto the subjects and the subjects’ compliance was closely monitored and recorded.
The TLSO is a custom-made orthosis and consists of two plastic shells directly molded onto the patient’s body (see Figure 1). This orthosis includes anterior and posterior components, which are secured together by Velcro straps, for keeping the patient’s pelvis in place. The TLSO was used to relieve pain via increasing immobilization of thoracolumbar regions for patients with OVF at the acute stage. The biomechanics of TLSO is based on the principle of three-point pressure system.

Patient with TLSO (anterior view).
The soft lumbar orthosis was used on the lumbosacral region of the spine. After placing the soft lumbar orthosis, the involved orthotist would tighten the Velcro straps at the front (see Figure 2). Two posterior metal uprights were bent according to the lordosis contour of the patient’s low back and inserted in between the layers of canvas. The soft corset was used to reduce pain via increasing the abdominal pressure and slightly controlling the mobility of lumbar region at the subacute stage.

Soft lumbar orthosis: (a) fitted on patient and (b) anterior view.
The SpinoMed® orthosis (Medi Bayreuth) consists of a back pad, which is made of metal with soft padding and serves as the primary component to stretch the spine of the patients, and a system of belts with Velcro. This allows adjustment for individual size by the clinicians (see Figure 3). The orthosis weighs 450 g and is worn like a supportive backpack. The SpinoMed® orthosis is designed to strengthen the trunk muscles via straightening the patient posture. In this study, the subjects in the SpinoMed® group were requested to wear the SpinoMed® orthosis for 3 h daily for 2 consecutive weeks during rehabilitation training.
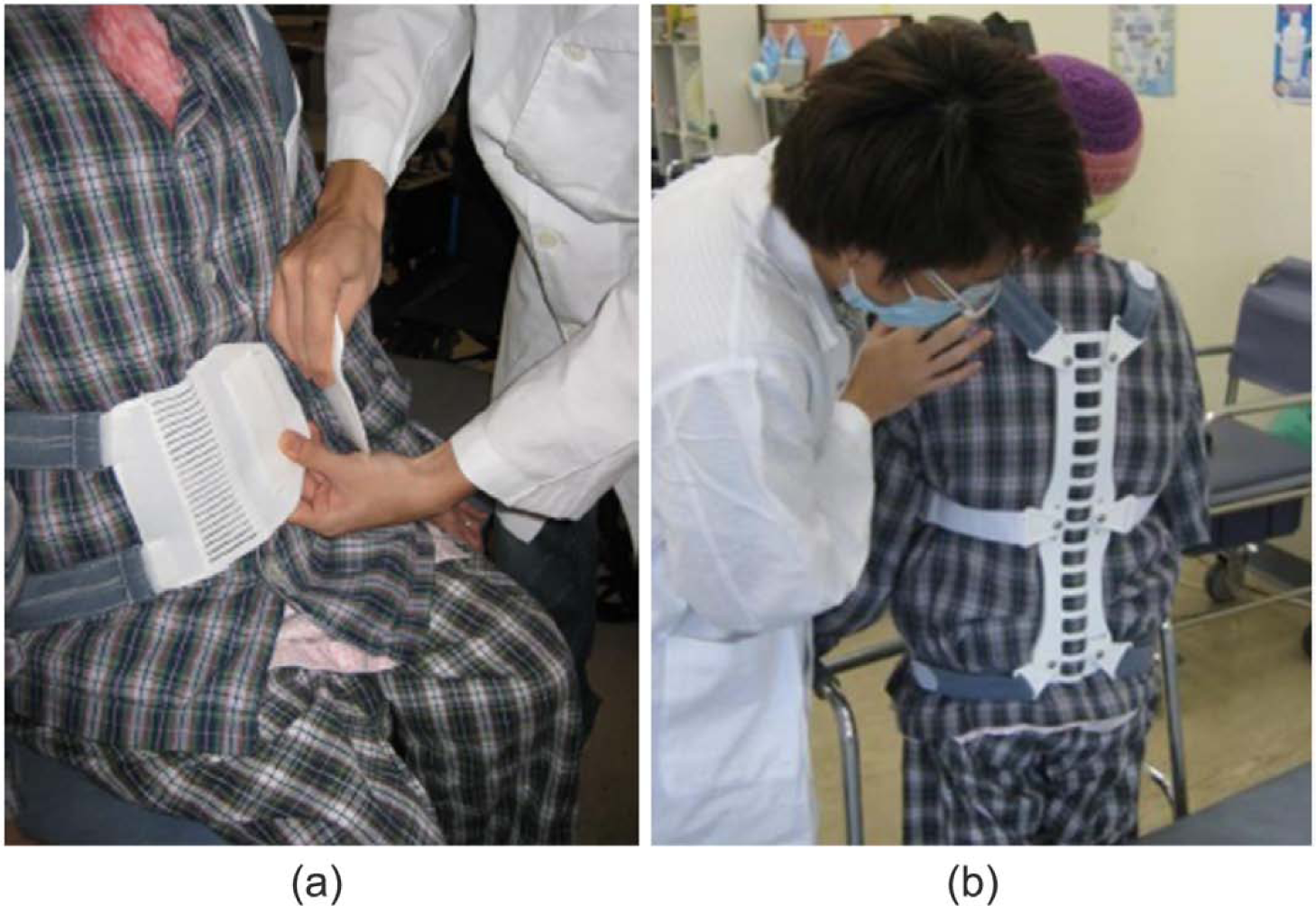
SpinoMed® orthosis: (a) anterior view and (b) posterior view.
Assessments
The change in pain level was assessed by a “10-point scale” system where level 10 means extreme pain and level 0 means no pain at all. The subjects were verbally asked to rate the pain level before fitting the corresponding orthoses (at the end of the first week when the patients were prescribed with SpinoMed® or corset) and on the day of discharge (after 3 weeks of orthotic treatment). The intensity of pain that the subjects suffered was rated from 0 (no pain) to 10 (extreme pain). The gain in functional mobility level was estimated by Functional Independence Measure-motor Scores (FIM-motor Scores), Elderly Mobility Scale (EMS), and Modified Functional Ambulation Category (MFAC).
FIM-motor Scores is widely adopted for assessing basic quality of living activities for persons with disability. It is part of the Uniform Data System (UDS) for Medical Rehabilitation and being used internationally. 17 It includes 18 items to measure how much assistance is required for the individual to carry out activities of daily living. The maximum score of FIM-motor Scores is 126 and the higher scores indicate the more independent.
EMS 18 provides a standardized validated scale for assessment of mobility in more frail elderly patients. This scale assesses seven dimensions of functional performance, which include locomotion, balance, and key position changes in daily living. The maximum score of EMS is 20 and higher scores indicate better performance.
MFAC19–21 is a reliable functional mobility test to classify the patient’s walking capacity, which is separated as seven levels of ambulatory status (i.e. lyer, sitter, dependent walker, assistant walker, supervised walker, indoor walker, and outdoor walker). The maximum score of MFAC is 20 and higher scores indicate more independent in mobility (scores larger than 14 means independent in mobility).
The thoracic kyphosis angle was measured from pretreatment and posttreatment X-ray in the sagittal plane. Cobb’s method was employed to assess the thoracic kyphosis angle (from the level of Thoracic 5 to Thoracic 12).
Data analysis
The data collected were analyzed using the Statistical Package for Social Sciences (SPSS Statistics 17.0, Inc., Chicago, IL 60606-6412, USA). The confidence interval is set at 95% (p < 0.05). The paired Student’s t-tests were applied to analyze the mean difference and the levels of significance for the studied treatment assessments (i.e. pain level and functional mobility level includes EMS, MFAC, and FIM-motor Scores) between the pretreatment and posttreatment for both the SpinoMed® group and the soft lumbar orthosis group. In addition, the independent samples t-tests were used to compare the mean difference and level of significance with reference to the treatment outcomes between the SpinoMed® group and the soft lumbar orthosis group.
Results
The mean ages of the involved subjects are 82 years (standard deviation (SD): 8.3 years; range: 58–93 years) and 81 years (SD: 6.6 years; range: 68–92 years) for the SpinoMed® group and soft lumbar orthosis group, respectively. The levels of vertebral fracture were different among patients (see Table 1). There were 10 patients of soft lumbar orthosis group and 15 patients of SpinoMed® orthosis group who suffered from only one level of vertebral fracture (the levels ranged from T12 to L5). Regarding those who suffered from two levels of vertebral fracture, there were nine from soft lumbar orthosis group and seven from SpinoMed® orthosis group (the levels ranged from T11 to S1). The other patients (five from each group) suffered from at least three levels of vertebral fracture (the levels ranged from T4 to L5).
Levels of vertebral fracture.

Both the SpinoMed® orthosis and soft lumbar orthosis groups were found to provide significant decrease in the patients’ pain level as well as the patients’ limitation in daily life with regarding the FIM-motor Scores, EMS, and MFAC (p < 0.05, see Table 2). However, the effect of different spinal orthoses on pain level reduction and functional mobility level gain did not show any significant difference (p > 0.05). In pain level analysis, the SpinoMed® group (from 6.7 to 4) showed a slightly more mean pain level reduction than that of the soft lumbar orthosis group (from 6.3 to 4.5), although the difference was not statistically significant. For the soft lumbar orthosis group, the gains in FIM-motor Scores, EMS, and MFAC were 18.4%, 113.3%, and 51.6%, respectively, while for the SpinoMed® group, the gains in FIM-motor Scores, EMS, and MFAC were 20.2%, 110.6%, and 48.4%, respectively.
Treatment assessment (SpinoMed® group vs soft lumbar orthosis group).
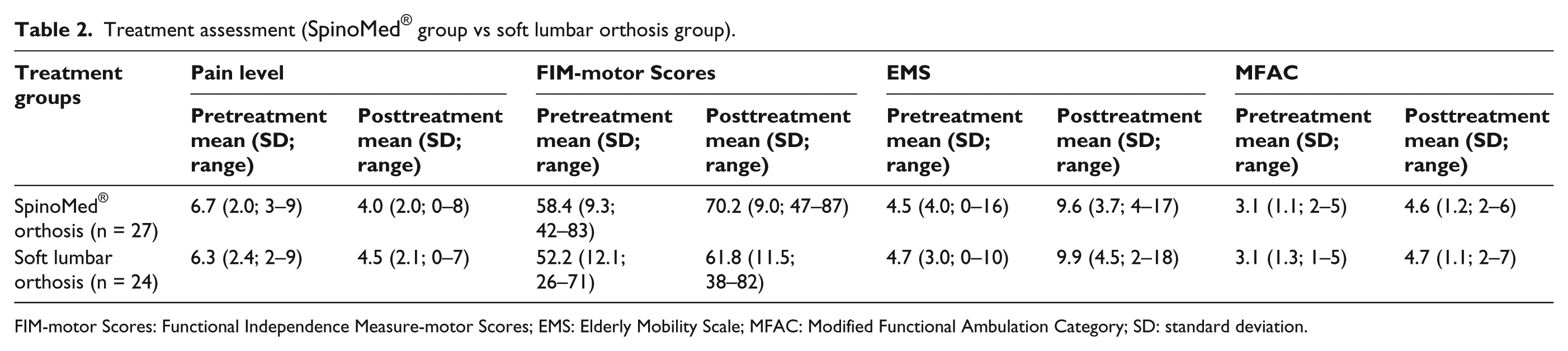
FIM-motor Scores: Functional Independence Measure-motor Scores; EMS: Elderly Mobility Scale; MFAC: Modified Functional Ambulation Category; SD: standard deviation.
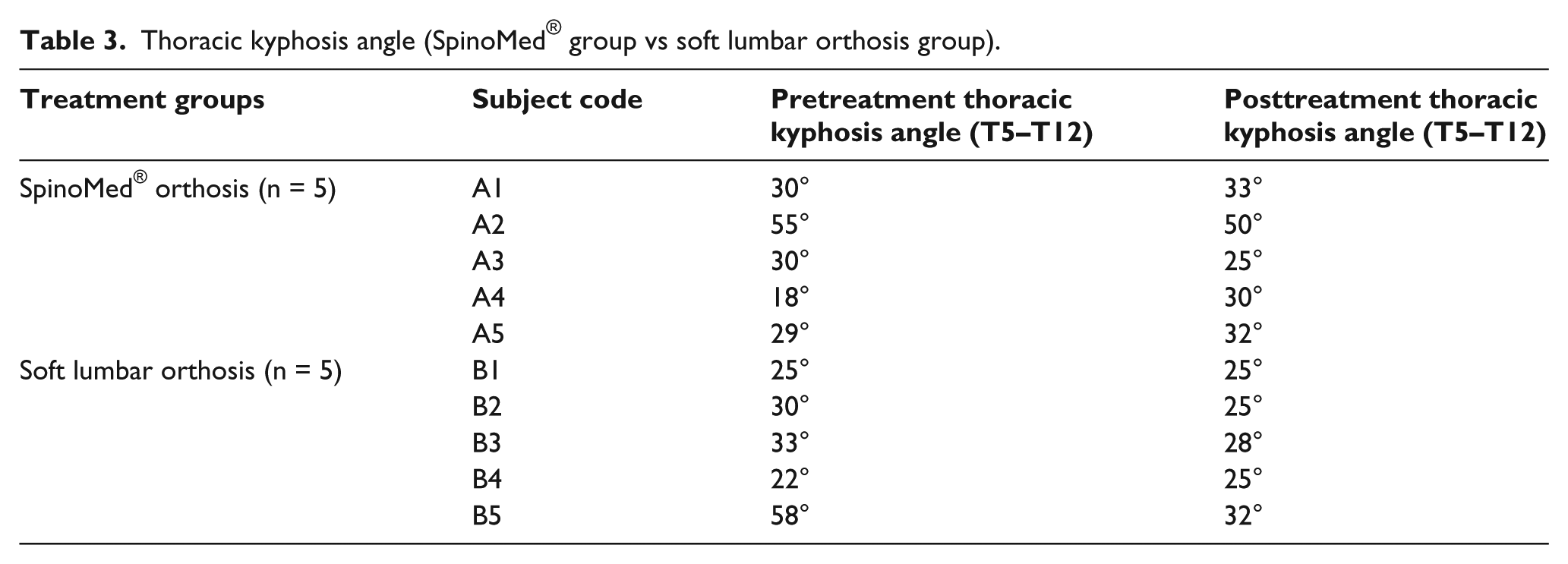
Standing radiographic assessments on the thoracic spine were performed on five subjects from each group. The Cobb’s angles of thoracic kyphosis are shown in Table 3. Through reviewing the 10 subjects, both the SpinoMed® orthosis and soft lumbar orthosis were able to control thoracic kyphosis within normal range except in subject A2 (the SpinoMed® orthosis reduced the hyperkyphosis from 55° to the normal value 50° since the original thoracic kyphotic angle of this subject was quite severe, see Table 3).
Thoracic kyphosis angle (SpinoMed® group vs soft lumbar orthosis group).
Discussion
The spine is one of the most important structures of the body which if injured would seriously affect the quality of life.22–24 In this study, the effectiveness of the two types of spinal orthoses on rehabilitation of patients with OVF was evaluated regarding the ability to relieve pain and improve functional independence. The patients’ pain level and the limitation in daily life with regarding the FIM-motor Scores, EMS, and MFAC (p < 0.05) at the subacute stage were significantly decreased in both SpinoMed® orthosis and soft lumbar orthosis groups. The effect of these two spinal orthoses on reduction of pain level and gain of functional mobility level showed no significant difference (p > 0.05). These findings indicated that the posture training of SpinoMed® orthosis may not produce significant additional treatment effectiveness to the patients with OVF to the conventional orthosis (soft lumbar orthosis) at the subacute stage on the aspects of pain relief and functional independence improvement.
Pfeifer et al. 14 conducted a prospective randomized study to evaluate the effects of the SpinoMed® orthosis using a two-group design. They found that the SpinoMed® orthosis was effective in increasing trunk muscle strength and improve the posture in patients with OVF after intervention period of 6 months (approximately 2 h/day in SpinoMed® orthosis). In addition, the SpinoMed® orthosis could help the patients with OVF to achieve better quality of life through pain reduction, decreased limitations of daily living, and improved overall well-being. However, the compliance was only recorded by the subject’s self-report diary and the reported study did not compare the results with conventional orthoses (including soft lumbar orthosis and rigid orthosis). This study had evaluated the efficacy of SpinoMed® orthosis by a prospective and randomized control trial with the subjects’ compliance monitored by clinicians in hospital.
The SpinoMed® is a lightweight designed orthosis and might be cosmetically acceptable to the patients. This study was pilot trial to evaluate the benefits of SpinoMed® orthosis to patients with OVF. The principle of SpinoMed® orthosis is to increase trunk muscle strength and thus improve posture and body height in patients with OVF. 25 The multidisciplinary rehabilitation concept of spinal osteoporosis should include back-strengthening exercises and postural training to counteract thoracic kyphosis in hyperkyphotic subjects, thus to improve the balance and independence for patients with OVF. 26 However, the effectiveness of SpinoMed® orthosis on the aspects of strengthening trunk muscle and improving posture should be further examined with the user’s compliance under an objective monitoring system, more intensive training program, or longer-term application.
Limitations
In this study, the periods of application and observation of the effects of SpinoMed® orthosis were only 3 h daily for two consecutive weeks. The subjects’ compliance was controlled and monitored by the therapists since all the subjects were inside the hospital during the study period (which was 3–4 weeks). Only the immediate results of the application of the orthoses were recorded. In future studies, the patient’s compliance in daily life after discharge from hospital should be monitored by some compliance sensors (e.g. thermo sensor). Thus, the investigation on the longer-term effect of the SpinoMed® orthosis could be more feasible and convincing.
OVF is usually associated with thoracic hyperkyphosis. An effective management of OVF should offer a control or even decrease in thoracic hyperkyphosis. However, this study could not gather enough radiographic information to prove this observation as there were only 10 subjects with the lateral X-ray of their thoracic spines.
This study focused on the treatment effectiveness of SpinoMed® orthosis and soft lumbar orthosis in pain relief and improvement in quality of life. For comprehensive analysis, more parameters should be investigated in the future study, such as gait and posture, trunk muscular activities, lung functions, and limitations in activities of daily living.
Conclusion
Both groups were found to significantly reduce the patients’ pain level and limitations of daily life (p < 0.05). The effect of the two types of spinal orthoses on the pain level reduction and functional mobility level gain did not show significant difference (p > 0.05) at the subacute stage. Their long-term effects require further study to confirm while the patients’ compliance should also be monitored.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.