
Abstract
Background:
Prediction of in-orthosis curvature at pre-orthosis stage is valuable for the treatment planning for adolescent idiopathic scoliosis, while the position of spinal curvature assessment that is effective for this prediction is still unknown.
Objectives:
To compare the spinal curvatures in different body positions for predicting the spinal curvature rendered by orthosis.
Study design:
A prospective cohort study.
Methods:
Twenty-two patients with adolescent idiopathic scoliosis (mean Cobb angle: 28.1°± 7.3°) underwent ultrasound assessment of spinal curvature in five positions (standing, supine, prone, sitting bending, prone bending positions) and that within orthosis. Differences and correlations were analyzed between the spinal curvatures in the five positions and that within orthosis.
Results:
The mean in-orthosis curvature was 11.2° while the mean curvatures in five studied positions were 18.7° (standing), 10.7° (supine), 10.7° (prone), –3.5° (prone bending), and −6.5° (sitting bending). The correlation coefficients of the in-orthosis curvature and that in five studied positions were r = 0.65 (standing), r = 0.76 (supine), r = 0.87 (prone), r = 0.41 (prone bending), and r = 0.36 (sitting bending).
Conclusion:
The curvature in recumbent positions (supine and prone) is highly correlated to the initial in-orthosis curvature without significant difference. Thus, the initial effect of spinal orthosis could be predicted by the curvature in the recumbent positions (especially prone position) at the pre-orthosis stage.
Clinical relevance
Prediction of in-orthosis correction at pre-orthosis stage is valuable for spinal orthosis design. This study suggests assessing the spinal curvature in recumbent position (especially prone position) to predict the initial in-orthosis correction for optimizing the orthosis design.
Background
Adolescent idiopathic scoliosis (AIS) is three-dimensional (3D) spinal deformity with lateral curvature and vertebral rotation in adolescence with unknown causes. 1 The incidence of AIS has been reported as 2%–4%. 2 Orthotic treatment is generally prescribed for the patients with moderate AIS and surgical treatment will be considered if the deformity becomes severe. Until now, orthotic treatment has served as an important non-surgical treatment for the patients with AIS. 3
Prediction of in-orthosis curvature at the pre-orthosis stage is valuable for orthosis design, while it is normally estimated according to the clinical experience in current practice. To optimize this empirical practice, some proposed to use the curvature in a body position which induced curve correction (such as lateral bending position) to estimate the curvature corrected by orthosis. Wong et al. 4 and Vidyadhara and Mak 5 assessed the curvature when the patient was lying down (supine position), but the prediction accuracy of supine position was unclear because detailed statistical results were not provided in their studies. Chekryzhev et al. 6 reported that the curvature in lateral bending position correlated to the curvature after fitting orthosis (correlation coefficient = 0.68), while the reliability of their measurements was unclear as “Spinal Mouse” was used to measure the coronal spinal curvature. Another study used radiography to assess the lateral bending curvature and reported no significant difference with the in-orthosis curvature. However, this finding may only be applicable to the nighttime orthosis used in their study. 7 Kuroki et al. 8 proposed standing with traction position for estimating the in-orthosis curvature, but the predictability of this method was affected by the diverse maturity status of their subjects (at 9–18 years with Risser 0–5). Up to now, the position which could better predict the in-orthosis correction has not been fully studied.
To assess and compare the spinal curvature in different positions, traditional X-ray imaging and computed tomography (CT) may not be feasible as high dose of ironizing radiation increases the risk of breast cancer on adolescents. 9 Magnetic resonance imaging (MRI) and EOS imaging, a low-dose stereography system are not readily used due to the limited assessment positions: MRI may only be conducted with patients in recumbent positions and EOS mainly adopts standing position. Ultrasound imaging technique, which has been proved reliable and valid to assess scoliosis in research and clinical practice,10,11 would be an option for the radiation-free assessment in various body positions. Therefore, this study aims to compare the spinal curvature in different body positions for predicting the spinal curvature rendered by orthosis using ultrasound imaging technique.
Methods
Patients with AIS were recruited at a tertiary referral scoliosis clinic with the inclusive criteria: (1) Cobb angle: 25°–45° in major curve; (2) age: 10–14 years; (3) Risser sign: 2 or less; (4) prior to the first orthotic treatment. Human Subjects Ethics was approved by the local Institutional Review Board. Written consents were obtained from all the subjects and their guardians.
At pre-orthosis stage, spinal curvatures were assessed by an ultrasound system “Scolioscan” (Model SCN801; Telefield Medical Imaging Ltd, Hong Kong). The gain and dynamic contrast settings of the ultrasound system were adjusted by viewing the B-mode image from T1 to T12. Ultrasound frequency, focus, and scanning depth were set at 7.5 Hz, 3.5 cm, and 7.1 cm, respectively. For ultrasound scanning, the aqueous gel was applied on the back of the patient for better conduction between the probe and skin. Then the probe moved uprising from L5 to T1 slowly and steadily with the patient relaxed and breathing naturally (approximately 20–40 s). Afterward, all B-mode images (500–700 frames), corresponding spatial position, and orientation data were saved for the reconstruction of coronal ultrasound image by volume projection approach. 12 The above ultrasound scanning procedure was conducted in five positions (Figure 1), namely standing, supine, prone, sitting with lateral bending, and prone with lateral bending position in a random order. Standing position required patients to stand straight with feet shoulder-width apart, meanwhile pelvis was kept level. Recumbent positions (supine and prone) required patients to lie down facing up/down on a scanning couch with legs straight. Lateral bending position (sitting or prone with lateral bending) required patients to bend the trunk to the convex side of the curvature from neutral to their maximum limit (patients with double curves need to bend to both left and right sides). All subjects were requested to practice the positions three times to meet the above-mentioned requirements. In each position, the ultrasound scanning was conducted for two times with 1-min rest in between. Apart from ultrasound assessment, the routine pre-orthosis whole spine X-ray was taken in the standing and supine positions.

Assessment positions: (a) standing, (b) supine, (c) prone, (d) sitting with lateral bending, (e) prone with lateral bending, and (f) in-orthosis.
The spinal orthoses (Hong Kong orthoses) were designed and fabricated following standardized protocol by a team of orthotists who had more than 5-year clinical experience. Hong Kong orthosis is a kind of symmetric underarm rigid spinal orthoses constructed of high-temperature thermoplastics, polyurethane. It is designed with posterior opening and chest opening. Correcting pads are located strategically corresponding to different curve patterns in order to provide posterolateral controlling forces. The pelvic module is intimate with the pelvis to create a stable foundation. A reduction of lumbar lordosis is incorporated in the orthosis to achieve contact of the corrective force with the lumbar transverse processes and induce correction of the thoracic deformity. Subjects were instructed to wear the orthosis 23 h a day for 2–3 weeks (adaptation period). Afterward, the patients returned to the clinic for in-orthosis assessment first by a radiographic system (standing whole spine posteroanterior radiograph) and followed by the ultrasound imaging system. Before loosening the orthosis straps for ultrasound scanning, the width of posterior opening was recorded and a purpose-design fixture 13 was used to anchor the spinal orthosis around the trunk of patient. After unfastening the straps, the width of posterior opening of the orthosis was kept (same orthosis tightness) and the in-orthosis ultrasound scanning was conducted for two times on the exposed region of scoliotic spine in standing position.
The ultrasound images were measured using custom-developed software. The spinous process of each vertebra was identified and a line joining the spinous process at each level was drawn. Then, the levels of the upper and lower end-vertebrae were selected basing on the radiograph in standing position. The spinal curvature formed by the end-vertebrae was calculated by the software, which represented the curve angle of the spinal curvature.
Statistical analyses were performed using the IBM SPSS Statistics, Version 21 (IBM, Armonk, New York, USA). The mean value of the two scans was calculated as the curvature in the corresponding position. In order to reduce the influence of curve magnitude and location, the curves were analyzed in four subgroups: mild thoracic curves (<25°), moderate thoracic curves (25°–45°), mild thoracolumbar/lumbar curves (<25°), and moderate thoracolumbar/lumbar curves (25°–45°). The confidence interval was set at 95% (p < 0.05). One-way repeated analysis of variance (ANOVA) with least-squared differences (LSD) post hoc tests was used to compare the curvature in the five positions and that within orthosis. The Pearson product-moment correlation was performed to determine the correlation between the curvature in the five positions and the curvature within orthosis (correlation coefficient 0.00–0.24 indicates no correlation, 0.25–0.49 indicates low correlation, 0.50–0.74 indicates moderate correlation, 0.75–1.00 indicates high correlation 14 ).
Results
Totally, 22 subjects (mean Cobb angle: 28.1° ± 7.3°; mean age: 12 ± 2 years; Risser sign: 0–2) were recruited. The demographic data of subjects were presented in Table 1. The typical ultrasound images of a patient with AIS were demonstrated in Figure 2.
Patient demographic data.

BMI: body mass index.
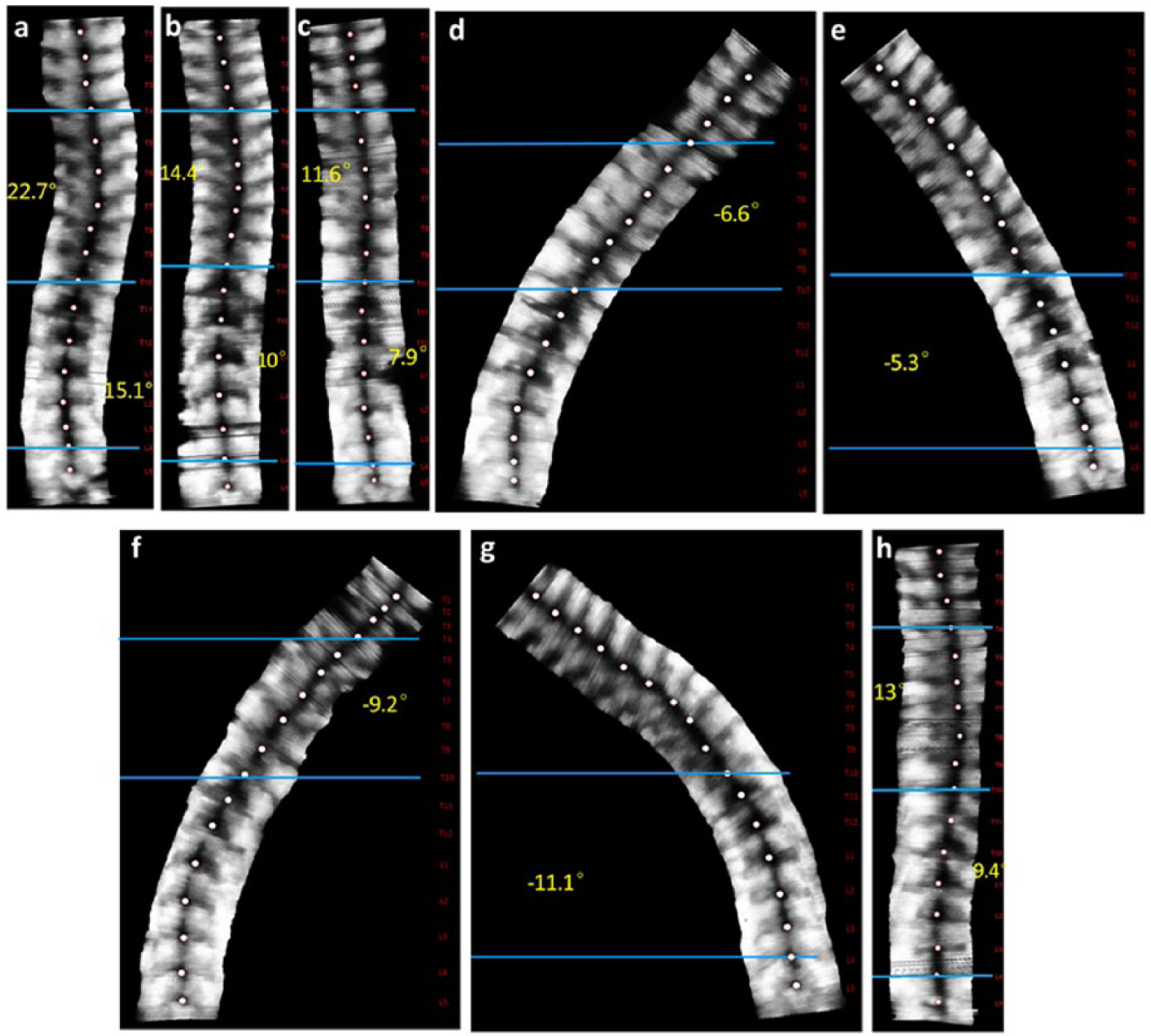
Ultrasound images. The angle of the right thoracic curve was 22.7° (standing), 14.4° (supine), 11.6° (prone), –6.6° (prone with lateral bending), –9.2° (sitting with lateral bending), and 13° (in-orthosis). The angle of the left lumbar curve was 15.1° (standing), 10° (supine), 7.9° (prone), –5.3° (prone with lateral bending), –11.1° (sitting with lateral bending), and 9.4° (in-orthosis). (a) Standing, (b) supine, (c) prone, (d, e) prone with lateral bending, (f, g) sitting with lateral bending, and (h) in-orthosis.
Curvature in five positions versus curvature within orthosis
The ultrasound measurements in the five positions and that within orthosis were presented in Table 2; the corresponding correlations were shown in Figure 3. For curvature in the standing position, it was significantly higher than (p < 0.05) and moderately correlated with (r = 0.65) the in-orthosis angle. In subgroups, the standing curvature was also higher than (p < 0.05) and moderately correlated with (0.5 < r < 0.75) the in-orthosis angle, except for the mild thoracic curves (r = 0.32). For curvature in recumbent positions, both supine and prone curvatures were not significantly different from (p = 0.27 and 0.16) and highly correlated (r = 0.76 and 0.87) with the in-orthosis angle. In subgroups, the supine and prone curvatures were similar with the in-orthosis angle without significant difference (p > 0.05), except for mild thoracic curves (p = 0.03). The supine curvature showed moderate correlation with the in-orthosis angle (0.5 < r < 0.75) in all subgroups except for mild thoracic curves (r = 0.92). The prone curvature showed high correlation with the in-orthosis angle (r > 0.75) in all subgroups except for mild thoracic curves (r = 0.64). For curvature in lateral bending positions, the spinal curvatures tended to be corrected to the opposite direction, thus demonstrating negative value of the curvature. Sitting and prone with lateral bending induced much higher curve correction than the in-orthosis correction (p < 0.05). The curvature in sitting and prone with lateral bending position showed low correlation with the in-orthosis correction (r < 0.3). In subgroups, significant higher curve correction (p < 0.05) than and low correlation with the in-orthosis angle (r < 0.5) were found as well.
Curvature in five studied positions and curvature within orthosis.
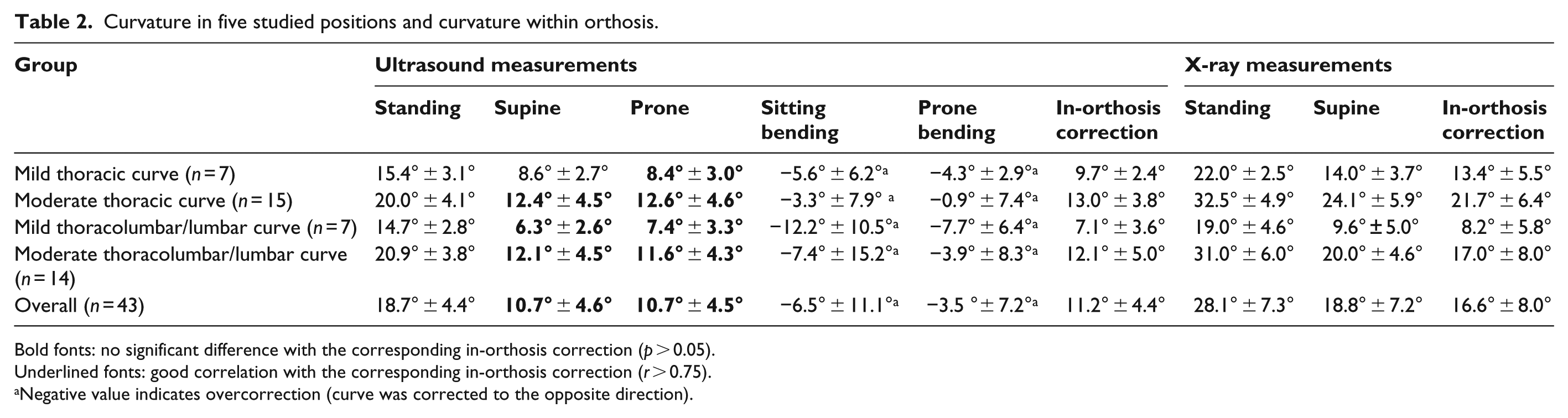
Bold fonts: no significant difference with the corresponding in-orthosis correction (p > 0.05).
Underlined fonts: good correlation with the corresponding in-orthosis correction (r > 0.75).
Negative value indicates overcorrection (curve was corrected to the opposite direction).
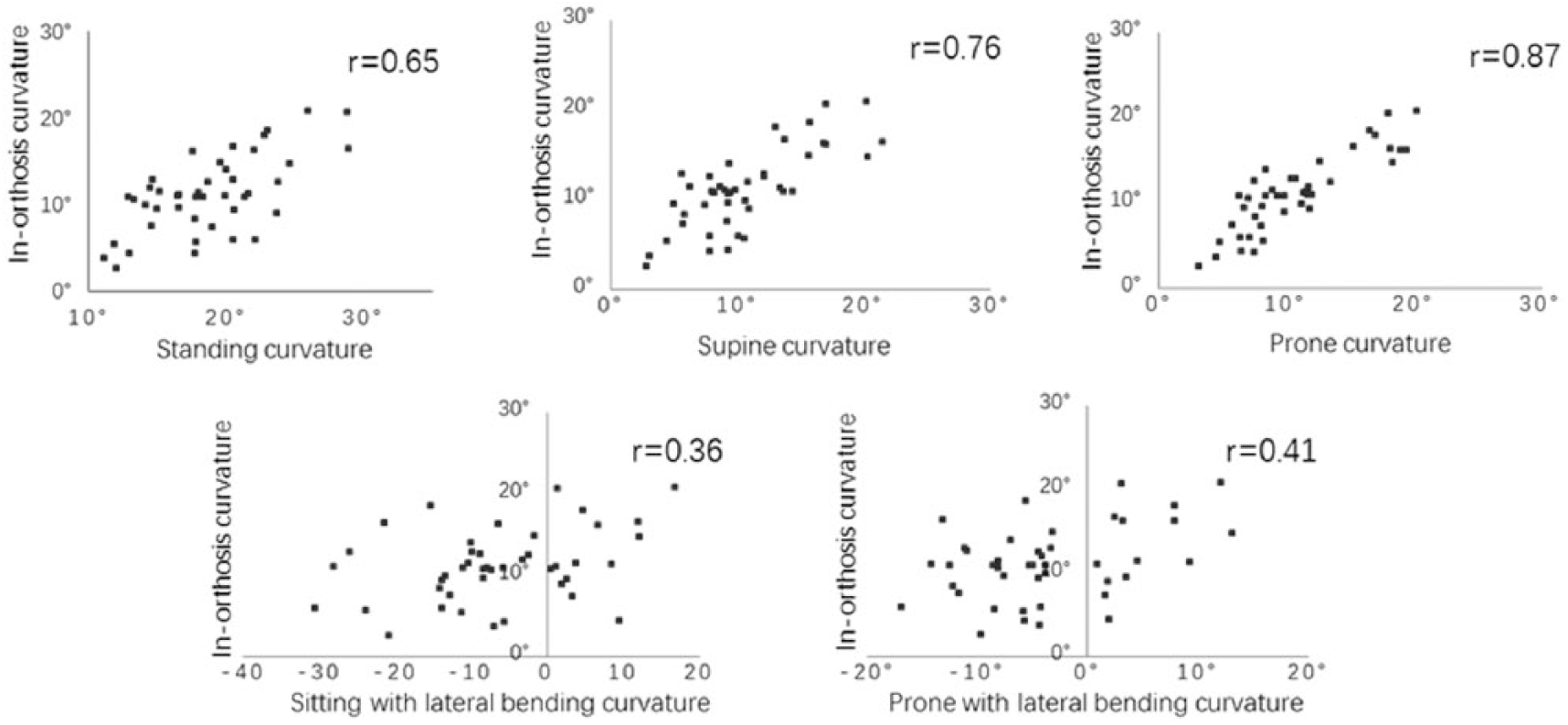
Correlation between curvature in five studied positions and curvature within orthosis.
The X-ray measurements in standing and supine positions and that within orthosis were presented in Table 2. For curvature in standing position, it was significantly higher than (p < 0.05) and moderately correlated with (r = 0.67) the in-orthosis angle. In subgroups, the standing curvature was higher than (p < 0.05) the in-orthosis angle with a low correlation (0.25 < r < 0.5) except for mild thoracolumbar/lumbar curves (r = 0.64). For curvature in supine position, it was significantly higher than (p < 0.05) and moderately correlated with (r = 0.73) the in-orthosis angle. In subgroups, significant difference was only found in moderate curves (p < 0.05), moderate correlation was showed in thoracic curves (0.5 < r < 0.75), and high correlation was found in thoracolumbar/lumbar curves (r ⩾ 0.75).
Supine versus prone; supine bending versus prone bending
Comparing curvature in supine and prone positions, they were not significantly different (p > 0.05) and highly correlated (r = 0.84) in both overall group and subgroups; only the mild thoracolumbar/lumbar curves showed moderate correlation (r = 0.61). Comparing curvature in sitting and prone with lateral bending position, the sitting bending curvatures were significantly higher (p = 0.00) than and highly correlated (r > 0.8) with that in the prone bending position in overall curves. In subgroups, significant difference was found (p < 0.05) except for moderate thoracic curves; high correlation was found (r > 0.8) except for mild thoracic curves (r = 0.6).
X-ray and ultrasound measurements
Comparing ultrasound and X-ray measurements in overall curves, ultrasound curvature was significantly lower and highly correlated with X-ray curvature in standing, supine, and in-orthosis position (r = 0.77, 0.82, 0.84, respectively). In subgroups, ultrasound measurements were also significantly lower except for the mild thoracolumbar/lumbar curves within orthosis; moderate to high correlation was found in all subgroups (0.57 < r < 0.94).
For predicting the in-orthosis angle, X-ray in-orthosis angle was moderately correlated with the X-ray supine angle (r = 0.73) with a significant difference (p < 0.05); ultrasound in-orthosis angle was highly correlated with the ultrasound recumbent angles (r > 0.75) without significant difference (p > 0.05), especially the highest correlation was found between the ultrasound prone angle and ultrasound in-orthosis angle (r = 0.87).
Discussion
Ultrasound technique was first used in this study to assess the spinal curvature in five positions, it was found that the curvatures in the recumbent positions were not different from and highly correlated with the initial in-orthosis curvature. This finding indicated that the recumbent curvatures (especially prone curvature) could be a predictor of the initial effect of orthotic treatment in the patients with AIS.
Curvature in five positions versus curvature within orthosis
This study found that the curvature in recumbent positions (supine and prone) could better predict the curvature within orthosis among the five studied positions, as the recumbent curvatures showed close value (p > 0.05) to and high correlation (r > 0.75) with the in-orthosis curvature, while the lateral bending curvatures (sitting and prone bending) revealed much higher curve correction than the orthotic correction (p < 0.05) with a low correlation (r < 0.25). It was also found that this correlation was not affected by the curve magnitude and location, which indicated a consistent trend in the subgroups and overall curve group in this study. Recumbent positions induced spinal curvature correction, which mainly resulted from the reduced axial gravitational loading and upward forces from the supporting surface. Spinal orthosis corrected the spinal curvature mainly via the correcting pads that applied posterolateral forces to the spine. Despite of different correction mechanisms, the response of spine to lying down position and orthosis application revealed the biomechanical properties of the intervertebral disc, ligaments, capsules of the facet joints, morphology of vertebrae and rib cage. These similar correction effects of the two methods indicated that recumbent test could be an appropriate method to reveal the biomechanical property of the spine and predict the initial effect of orthotic intervention. This finding suggested a quantitative method to assess the biomechanical property of the spine, which could be used to guide and improve the spinal orthosis design. This finding also provided a patient-specific method to predict in-orthosis curvature at the pre-orthosis stage, which might assist clinicians to differentiate the patients who were unlikely to benefit from orthotic treatment (such as patients with rigid spine and high progression risk); thus, closer monitor and special attention could be paid to this group of patients at earlier stage.
Supine versus prone; supine bending versus prone bending
The curvatures in the supine and prone positions were found of no significant difference (mean curvature = 10.7°) in this study. In both positions, the gravitational effect on the spine was eliminated axially and some muscle groups were at relaxation, while the upward force from the supporting surface was from the dorsal side during supine position and from the ventral side during prone position. Despite the difference in force direction, both forces tended to reduce and derotate the rib cage deformity. This may explain why the curve angles were close in the two positions. Whereas for the patients with larger curves, the severe rib hump or anterior chest deformity may disrupt the alignment of the shoulder and pelvis, hence leading to slightly different results. A study on 62 AIS patients with surgical treatment reported close curvature in the supine and prone positions (54° vs 57° for the thoracic curves; 33° vs 35° for the lumbar curves) but with significant difference. 15 The curvatures in the sitting and prone with lateral bending positions were highly correlated (r > 0.8), but sitting bending achieved higher correction than that of the prone bending (mean curvature was −6.5° and −3.5°, respectively). The possible reason was that the gravity contributed to the bending movement and assisted pelvic balance, flexed hip, and knee joints helped stabilize the trunk which facilitated muscle contraction to bend laterally in the sitting position. In the prone position, the lower body was less controllable; thus, more muscle contraction was involved in preventing pelvic tilting and lower extremities shifting during bending movement.
X-ray and ultrasound measurements
Ultrasound technique was applied in this study to assess the spinal curvature in five positions. The feasibility and validity of ultrasound measurements were confirmed via comparing to the X-ray measurements (gold standard). This study found that the ultrasound measurements were lower than and highly correlated with the X-ray measurements, which is in alignment with previous studies.10,11,16 The relatively lower correlation in the standing position (r = 0.77) than in the supine and in-orthosis positions (r = 0.82, 0.84, respectively) might arise from 1 to 3 months of time lag of the ultrasound and radiographic standing evaluation, while ultrasound supine/in-orthosis evaluation was performed immediately after X-ray supine/in-orthosis evaluation. The predictability of supine curve angle to in-orthosis angle was slightly lower in X-ray (r = 0.73) than in ultrasound (r = 0.76) measurements, especially the highest correlation (r = 0.87) between ultrasound prone angle and ultrasound in-orthosis angle was found among all measurements. Ultrasound technique allows repetitive assessment of spinal curvature in various body positions without radiation, it also enables a quick assessment (20–40 s) with real-time image display and immediate feedback of spinal curvature. These advantages make ultrasound a potential technique in assissting orthotic design and the other related applications.
Limitations
The curvature in the coronal plane was analyzed in this study, the vertebral rotation in the transverse plane will be elaborated after the 3D image analysis software is fully developed. Besides, this study focuses on the initial effect of orthotic treatment and the long-term effect of spinal orthosis needs follow-up studies. In addition, the time restriction and ethical issues do not allow the reliability and validity tests in all the five positions in the current study.
Conclusion
The curvature in the recumbent positions (supine and prone) is highly correlated to the initial in-orthosis curvature without significant difference. Thus, the initial effect of spinal orthosis could be predicted by the curvature in the recumbent positions (especially prone position) at the pre-orthosis stage.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.