
Abstract
Background:
International Classification of Function, Health and Disability provides a common framework and universal language for rehabilitation professionals across the globe.
Objectives:
To identify problems in functioning and mobility relevant to persons with lower-limb amputation from an expert’s point of view and quantify these problems using the International Classification of Function, Health and Disability.
Study design:
Qualitative study using electronic and paper surveys.
Methods:
Electronic or paper survey was done across six countries targeting clinicians involved in pre- and post-amputation care. Meaningful concepts were extracted from the responses and linked to suitable second-level and where applicable third-level International Classification of Function, Health and Disability categories. Categorical frequency analysis was completed for the combined data and for each location.
Results:
A total of 183 experts from 6 different countries responded to the survey. A total of 2171 concepts were identified, 82% of which could be linked to a second-level International Classification of Function, Health and Disability category. The categorical frequency analysis revealed that the categories of walking, design and construction of buildings for public and private use and sensation of pain were the most frequently occurring concepts and was similar across the six countries.
Conclusion:
The International Classification of Function, Health and Disability can be utilised as a common framework for communication among clinicians involved in rehabilitation of persons with lower-limb amputation across the globe. The most important factors that were identified by experts in amputee rehabilitation working in different international locations were similar.
Clinical relevance
The challenges faced by the clinicians involved in care of persons with lower extremity amputation vary across different parts of the world. The overarching goal for the clinician irrespective of the location is to improve mobility and quality of life of their clients. The International Classification of Function, Health and Disability provides a common language between the various stakeholders in amputee rehabilitation across the globe.
Background
The International Classification of Functioning, Disability and Health (ICF) provides a common framework and universal language for rehabilitation professionals across the globe. 1 Considerable efforts are undertaken to increase its use in clinical practice.2–4 One way to increase its use in clinical practice is to develop assessment tools based on the ICF framework. An international collaboration has been set up to develop an ICF-based mobility assessment tool. The first phase of the project aims to develop a tool based on ICF categories through literature review, getting perspectives from individuals who have a lower-limb amputation and from experts involved in their rehabilitation (Egen Cristoph, 2014, #370). 24 This model is based on the same methodology used for the development the ICF core sets.5–7
The challenges faced during the process of rehabilitation can vary between various countries depending on the resources, the demographics of the persons with lower-limb amputation and the social and cultural characteristics.8–11 Including experts and persons with lower-limb amputation from the different parts of the world in the development of any mobility assessment tool will aid for such a tool to be valid across various health care settings and countries. Inclusion of several of the World Health Organization (WHO) regions is required to ensure the diversity of cultural settings is accommodated. 12
The expert survey aimed to identify the concepts that clinicians involved in the provision of rehabilitation services to persons with lower-limb amputation, as well as manufacturers of mobility aids, consider essential to a ‘gold standard’ mobility assessment tool to measure mobility outcomes for their clients following rehabilitation.
Methods
An electronic/paper survey was administered in six countries: Argentina, Australia, Austria, China, Germany and the United States, targeting expert clinicians involved in pre- and post-amputation care. The clinicians surveyed belonged to a variety of professions including medical, nursing, occupational therapy, physiotherapy, prosthetics, psychology, social work and experts from the prosthetic manufacturing industry. The experts were recruited through group emails to various professional organisations and hospitals involved in the care of persons with lower-limb amputation and those attending the scientific meetings of these organisations. The experts were given a project overview either electronically or in paper depending on their preference. For the electronic survey, a web-based survey through survey monkey and email were used. Surveys returned in the publicised survey period between August and December 2013 were included in the analysis. The surveys were administered in the most frequently used language of the individual study centre that recruited the respondents. The responses were translated into English by the main researcher in each of the study centres. The coordinating centre collated the survey results. Meaningful concepts were extracted from the responses and linked to suitable second-level and where applicable third-level ICF categories according to the published linking rules.13,14 A concept that was repeated more than once in the response from a single participant was not coded more than once. Analysis of the data included an ICF category frequency analysis of the combined data and separately for each location.
The survey contained six broad exploratory questions:
If you think about the body and mind of individuals with lower-limb amputation what does not work the way it is supposed to?
If you think about the body of individuals with lower-limb amputation, in which parts are their problems?
If you think about the daily life of individuals what are their problems?
If you think about the environment and the living conditions of individuals with lower-limb amputation, what is supportive and/or what is hindering for them?
If you think about individuals with lower-limb amputation what is important about them and the way they handle their condition?
If you think about measuring mobility and how it affects individuals with a lower-limb amputation what are the most important factors to measure?
The questions are open-ended and were approved by the project steering committee before the commencement of the survey.
An expert was defined as a Clinician who had at least 2 years of experience of working with lower-limb amputees. The questions were aimed to elicit a comprehensive list of items corresponding to the four domains of the ICF which are body structure, body function, activities and participation and environmental factors. The fifth question was about personal factors that are not coded in the current version of ICF. The sixth question was to explore mobility-related factors that were important in rehabilitation of persons with lower-limb amputation.
The project was funded by a grant received from Otto Bock Healthcare Products and Össur.
Ethics approval for the project was obtained from the Ethics committees across the six study centres.
Results
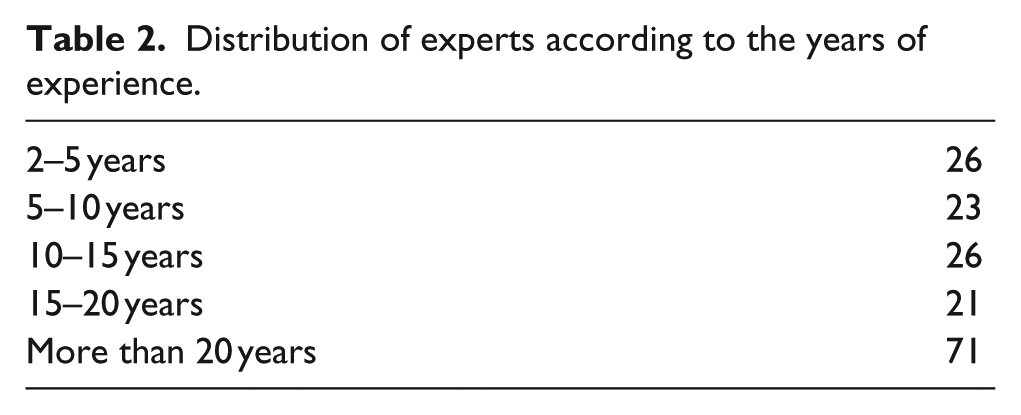
A total of 183 experts from the six countries responded to the survey. The distribution of experts according to the country, profession and experience are represented in Tables 1 and 2. The discrepancy between numbers in the table is due to missing data.
Distribution of experts according to study centres and profession.
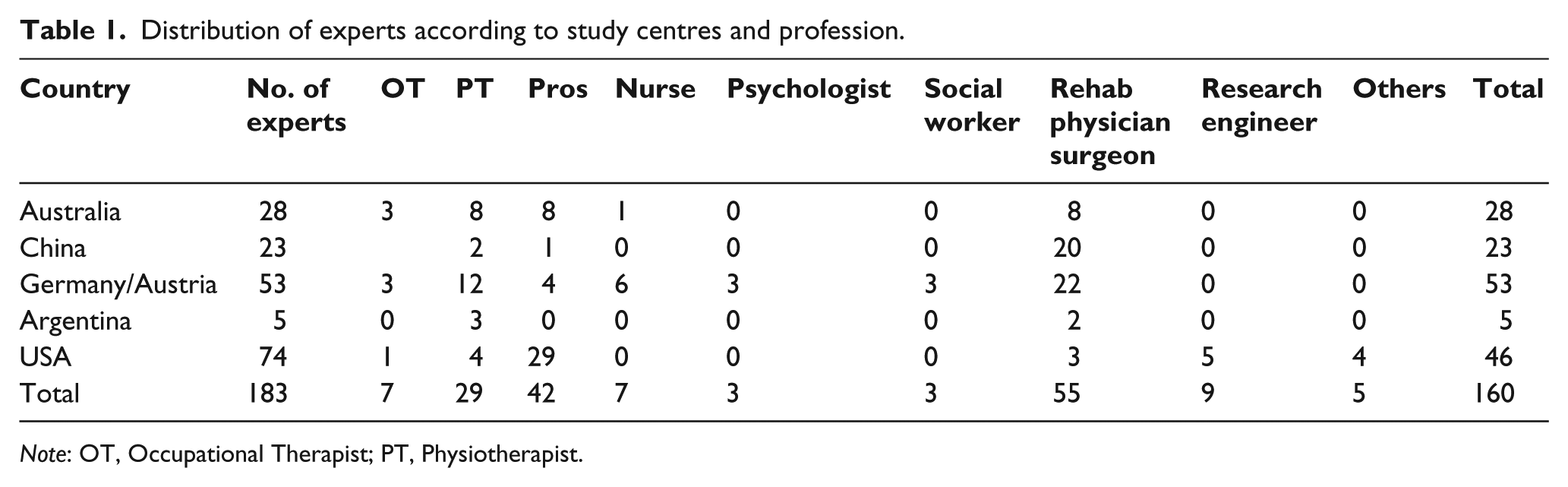
Note: OT, Occupational Therapist; PT, Physiotherapist.
Distribution of experts according to the years of experience.
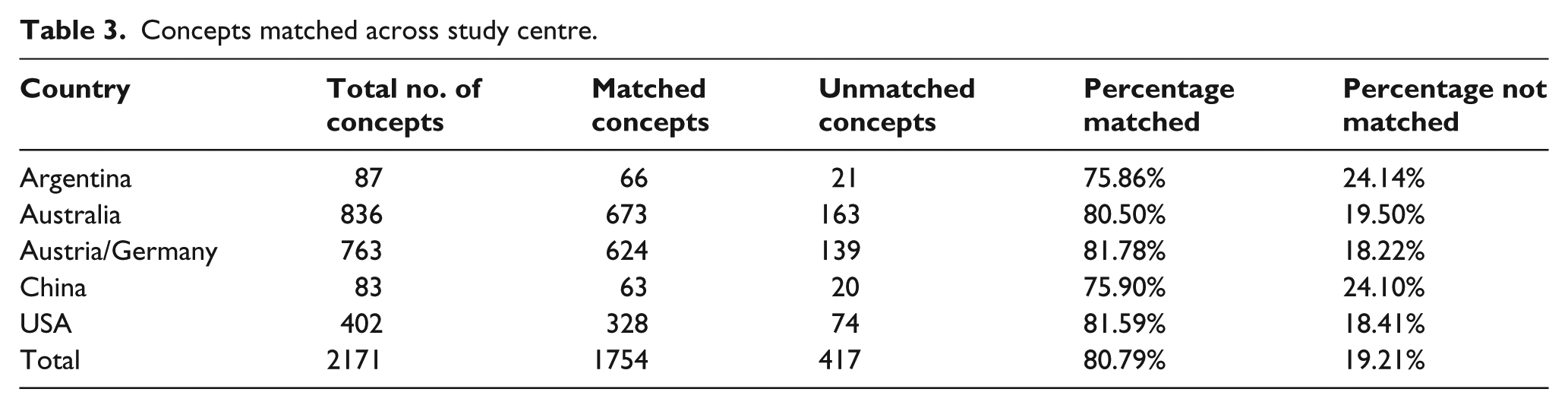
A total of 2171 concepts were identified, of which, 82% could be linked to a second-level ICF category. Of the 100 second-level ICF categories that were identified, seven were in the body structure domain, 29 in the domain of body function, 31 in the domain of activity and participation and 33 in the environmental factors domain. The proportion of concepts that were matched and not matched according to the country is shown in Table 3. Concepts that could not be matched were either very broad such as self-care which could only be linked to a chapter in the ICF framework or were personal factors such as age and comorbidities which are not coded in the ICF. There were also concepts like energy efficiency which are not defined in the ICF. Tables 4–6 show the distribution of categories across various domains of the ICF and various study centres.
Concepts matched across study centre.
Distribution of categories in body function across the study centres.
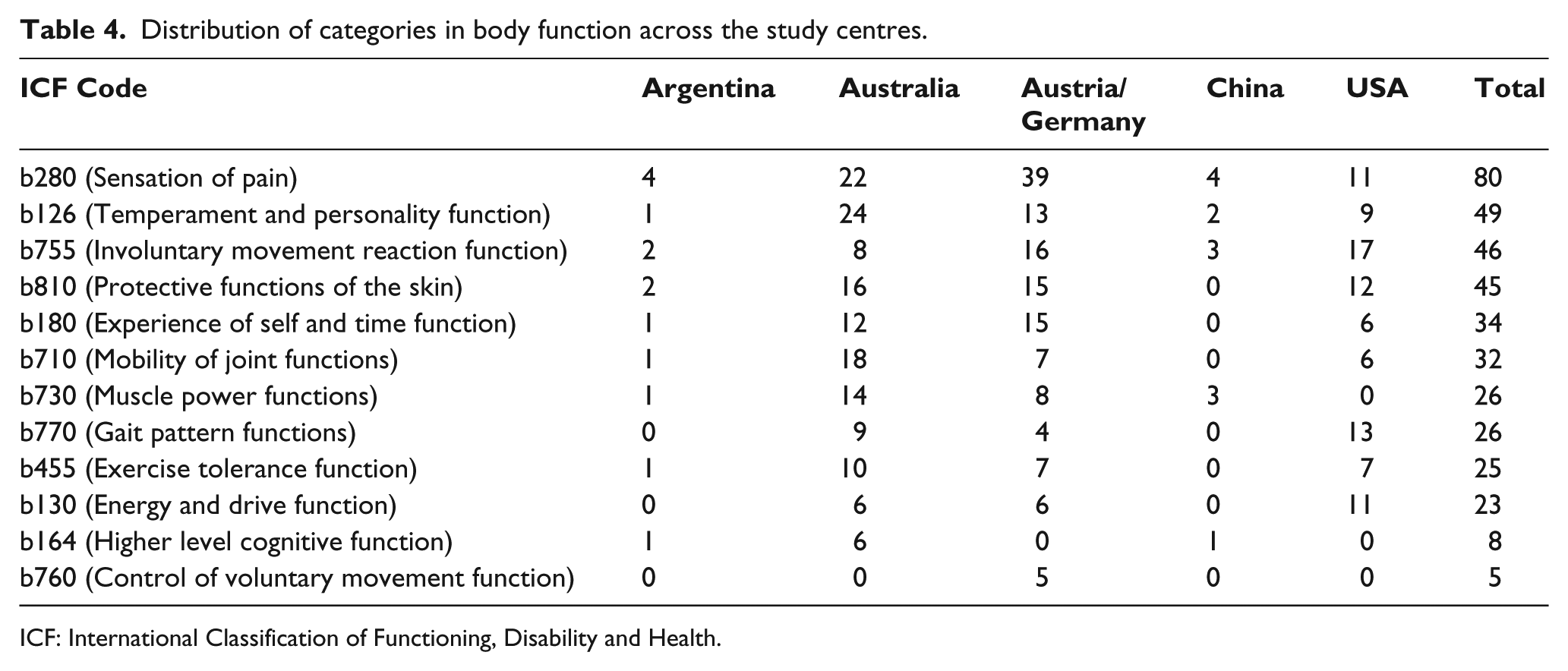
ICF: International Classification of Functioning, Disability and Health.
Spread of activity and participation items across study centres.
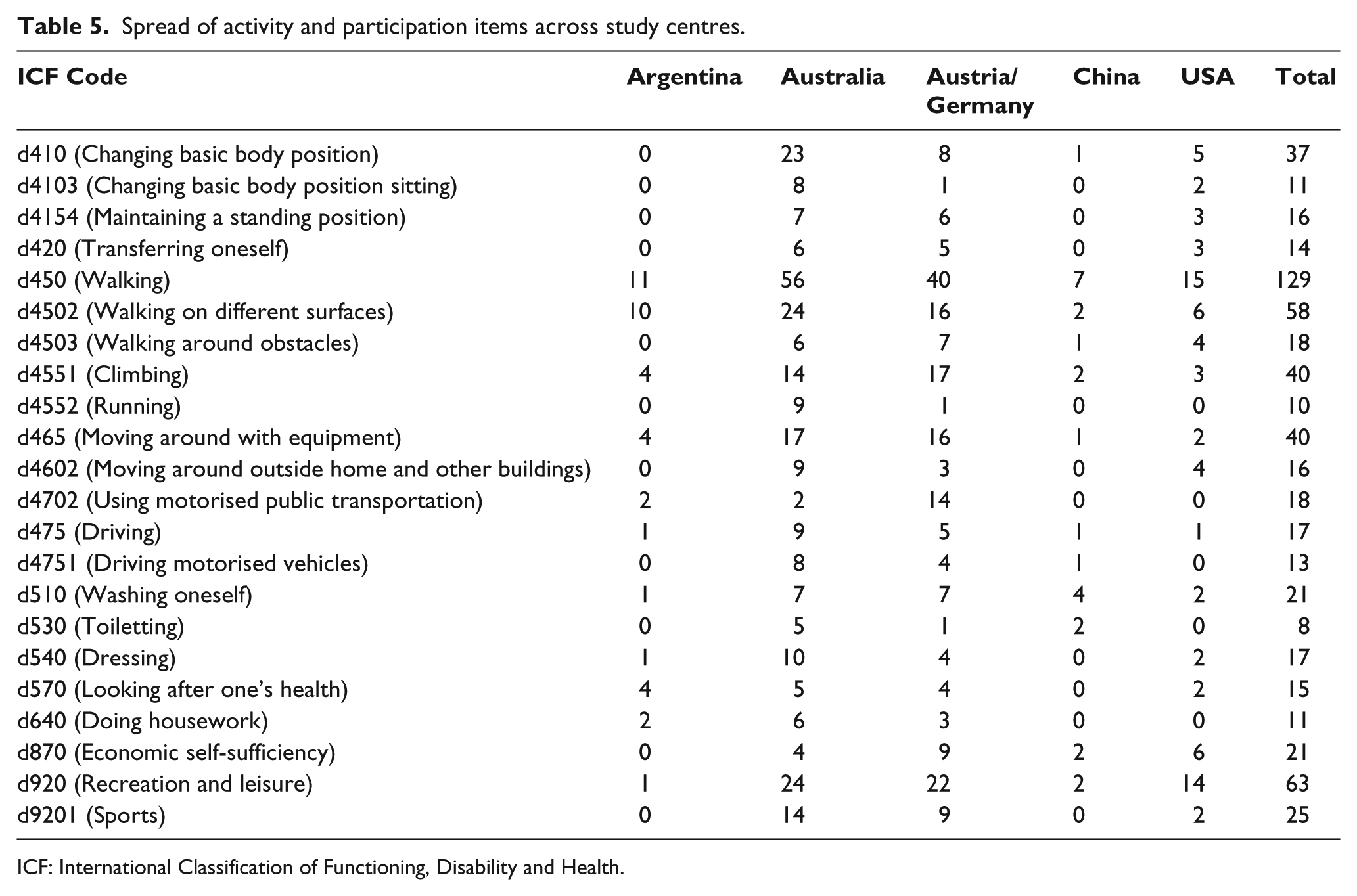
ICF: International Classification of Functioning, Disability and Health.
Frequently occurring categories in the environmental factors domain across the study centres.
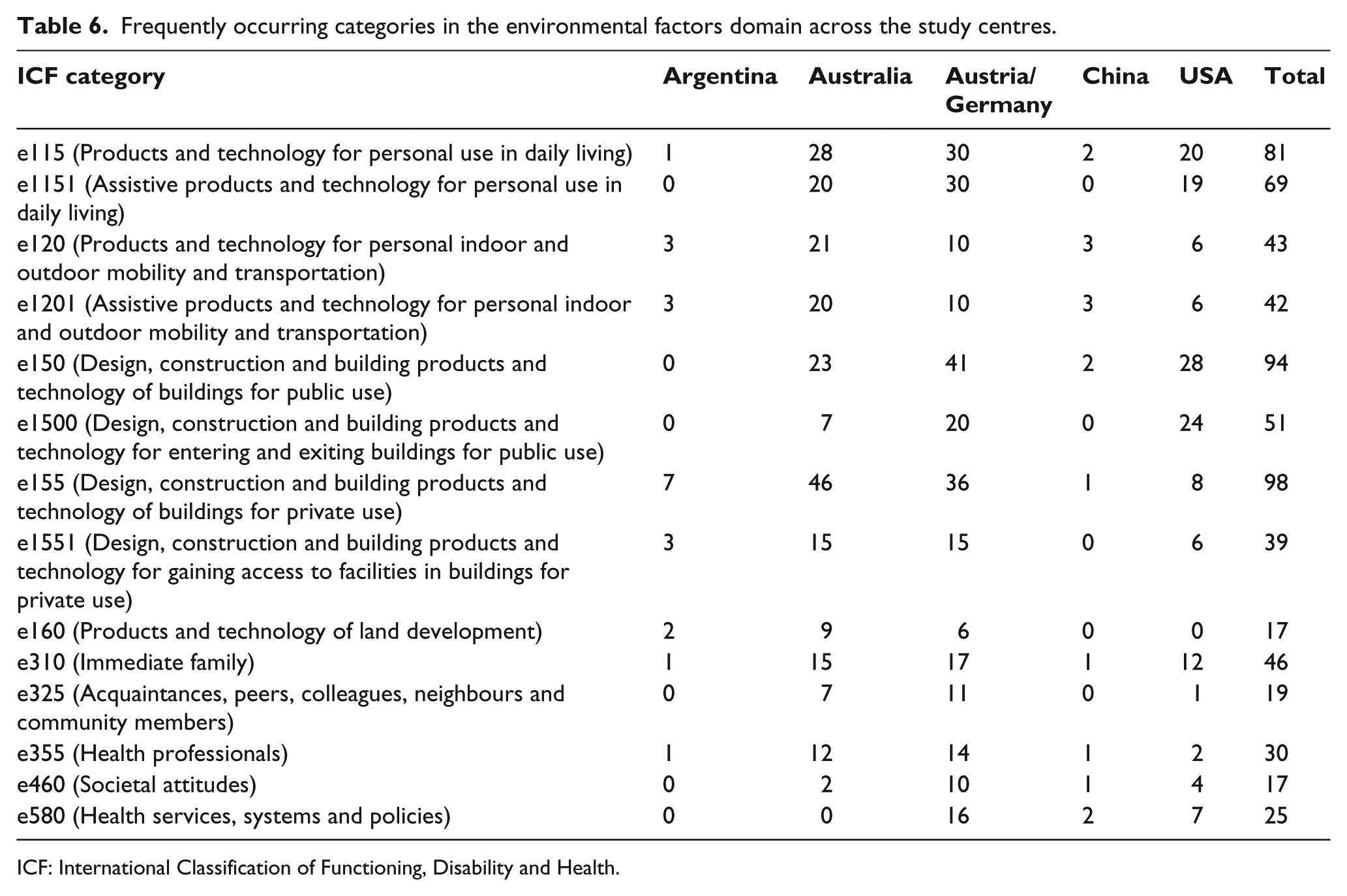
ICF: International Classification of Functioning, Disability and Health.
Pain and temperament and personality functions were the most frequently occurring categories from the body structure and body function domains of the ICF (Table 4).
The most frequently occurring categories in the activities and participation domain were walking on different surfaces and moving around especially climbing (Table 5). In the environmental factors domain use of a prosthesis, access into and inside public and private buildings and assistive technology being helpful in accessing public and private modes of transportation were the most common categories (Table 6).
Discussion
Expert surveys have been used to develop outcome tools for patients with an amputation previously.15–17 However, there is a lack of published literature that has analysed in detail the expectations from experts involved in the rehabilitation of persons with lower-limb amputation.
The large proportion of concepts that could be matched to the various ICF categories illustrates the comprehensiveness of the ICF and its potential to be used as a communication tool between rehabilitation professionals worldwide. Similar results have been noted in previous studies linking concepts from expert surveys to ICF categories.18–20 The critical factors that were identified by the experts in amputee rehabilitation working in different health care settings were similar across the six countries.
In amputation rehabilitation, as well as in the rehabilitation of other health conditions, personal factors do have a significant influence on the outcomes. The importance of personal factors was uniformly accepted by the experts irrespective of their geographic location. The largest spread of concepts and the most frequently occurring concepts belonged to the domain of activities and participation followed by environmental factors domain. It accentuates the close relationship of the environmental factors on a person’s function. This is in keeping with the definition of disability in ICF: ‘disability is a difficulty in functioning at the body, person, or societal levels, in one or more life domains, as experienced by an individual with a health condition in interaction with contextual factors’. 21 The least number of concepts were identified from the domain of body structures.
There was a good spread of experts across the different clinical specialities involved in amputation rehabilitation. More than 50% of the respondents had more than 10 years’ experience which increases the credibility of the survey. More experts responded through electronic means than paper. There was a wide variation in the length of the responses to individual questions. Those responses received via email surveys which involved answering the questions in a word document contained more information than paper surveys. The answers were more elaborate on the questions of activity and participation as well as of environmental barriers and facilitators. By involving experts from a wide variety of backgrounds including the field of practice, experience and country of practice, we have attempted to capture the challenges that are faced by clinicians across the globe to improve the outcomes for persons with lower-limb amputation. There was no substantial difference between the number of concepts identified based on the experience of the participants.
The distribution of concepts varied according to professional groups. Analysis of responses from physiotherapists showed an even distribution of concepts across their domains body function, activity and participation and environmental factors. The compiled data from social workers showed greater proportion of coded concepts belonged to the environmental factor domain while those from psychologists and occupational therapists showed a preponderance of concepts from the domain of activity and participation. The social workers gave more importance to the concept of moving around when compared to responses from other professional groups where the concept of walking appeared in higher relative frequency. This could be an artefact of translation or interpretation as walking and moving may not be identified as distinctly separate in some languages.
Among the concepts in body functions, pain was identified by all the professional groups as the most important factor. Protective function of the skin was the other important concept identified especially by nurses, prosthetists and physiotherapists. Among the environmental factors, access to and within public and private buildings were identified by most professions as most important for functional mobility apart from the prosthesis itself. Rehabilitation physicians, psychologists and physiotherapists in particular also identified general social support services, systems and policies among the most important environmental factors in the rehabilitation process.
The most frequently occurring categories varied between the different study centres. In the domain of activities and participation, walking, moving around and moving around in different locations appeared the most number of times from the analysis of all centres. This is expected when the primary aim of any interventions in amputation rehabilitation is to improve the mobility either through prosthesis or through mobility aids including wheel chair. Using motorised public transportation is one of the most frequently occurring third-level categories in Germany/Austria in contrast to other centres. This could be due to the fact that these nations have very well-developed and accessible public transport systems and rely much less on cars. It would also suggest that the sample is mainly from the cities where individuals rely even more on public transport. General social support services, a third-level ICF category in the domain of environmental factors, appear only in the expert surveys from Australia and Austria/Germany. One of the reasons for this is because these nations have social support system infrastructures that are more accessible. Temperament and personality along with pain was rated as the most important determinant from the body function domain, on the outcome of rehabilitation by clinicians from Australia. The gait pattern function and the involuntary movement reaction function were ranked first by the survey respondents from the United States. Sensation of pain appeared in the surveys from all the centres. Management of pain was as important as return to walking in the process of rehabilitation of persons with lower extremity amputations by Austrian/German experts.
The percentage of concepts matched is less than the proportion of matched concepts from a recent patient focus group analysis (Radhakrishnan, 2016, #619). 25 The importance given to concepts related to mobility especially walking on different surfaces was very similar in both expert and patient surveys. Among the environmental factors, the experts tended to rate the design of the buildings including exit and entry higher compared to clients with lower-limb amputation who rated the prosthesis or other assistive devices for mobility.
Limitations
There were gaps in the information as not all the experts responded to all the questions and the detail to which the questions were answered varied. There were some concerns that the actual questions were vague. This may have been due to the lack of familiarity of some of the experts with the ICF framework as the questions were intended to elicit concepts from the various domains in the ICF. There was a lot of overlap between the answers for the different questions. In some cases, it was difficult to differentiate between individual responses; the information from some surveys were received as responses of various individuals to a single question rather than one individual’s responses to the six questions. This made comparisons between different disciplines more difficult. Conducting online surveys has inherent disadvantages including multiple email addresses for the same person, multiple responses from participants, and invalid/inactive email addresses which make random sampling online a problematic method in many circumstances.22,23 There were more experts from developed regions that could have impacted on the concepts identified. We were not able to obtain surveys from Africa.
The surveys were collected in languages that were commonly used by the experts in the individual study centres, for example, in Mandarin for Chinese experts and German for the Austrian/German experts and translated into English by the researchers in these study centres. The English translations were then used for identifying meaningful concepts and subsequent linking to suitable ICF categories. It is possible that some of the concepts may have lost or altered by this process (Van Nes, 2010, #439). 26 Another drawback of the study is that other methods of qualitative data collection such as focus groups and individual interviews which could have added to the depth of data collected were not used.
The combination of experts that answered the surveys was different for the different centres. For example, 70% of the surveys from the United States were completed by prosthetists, while 87% of those who completed surveys from China were rehabilitation physicians. There was an even distribution of clinicians according to their area of practice among those who participated from Austria/Germany and Australia with each speciality contributing 20%–30% of the total number of experts. This may account for some of the differences between the study centres for distribution and frequency of different concepts.
Conclusion
The survey provides an extensive list of factors considered relevant to achieving optimal function in a person with lower-limb amputation by professionals involved in their care based on the geographic location and the discipline of practice. It has identified a number of frequently occurring categories in the activities and participation domain of ICF that could be part of a mobility assessment tool.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.