
Abstract
Background:
Investigating population changes gives insight into effectiveness and need for prevention and rehabilitation services. Incidence rates of amputation are highly varied, making it difficult to meaningfully compare rates between studies and regions or to compare changes over time.
Study Design:
Historical cohort study of transtibial amputation, knee disarticulation, and transfemoral amputations resulting from vascular disease or infection, with/without diabetes, in 2003–2004, in the three Northern provinces of the Netherlands.
Objectives:
To report the incidence of first transtibial amputation, knee disarticulation, or transfemoral amputation in 2003–2004 and the characteristics of this population, and to compare these outcomes to an earlier reported cohort from 1991 to 1992.
Methods:
Population-based incidence rates were calculated per 100,000 person-years and compared across the two cohorts.
Results:
Incidence of amputation was 8.8 (all age groups) and 23.6 (≥45 years) per 100,000 person-years. This was unchanged from the earlier study of 1991–1992. The relative risk of amputation was 12 times greater for people with diabetes than for people without diabetes.
Conclusions:
Investigation is needed into reasons for the unchanged incidence with respect to the provision of services from a range of disciplines, including vascular surgery, diabetes care, and multidisciplinary foot clinics.
Clinical relevance
This study shows an unchanged incidence of amputation over time and a high risk of amputation related to diabetes. Given the increased prevalence of diabetes and population aging, both of which present an increase in the population at risk of amputation, finding methods for reducing the rate of amputation is of importance.
Background
Incidence rates of transtibial amputation, knee disarticulation, and transfemoral amputation are highly variable. In a recent systematic review, it was reported that the rate of major amputations is between 3.6 and 68.4 per 100,000 person-years. 1 Variations in incidence may occur not only because the actual rates differ, but also because of differences in research methodology. These differences include how the population is defined, that is, minimum age cutoff; the level of amputation, which refers to (non)inclusion of partial foot amputations; and the method for identifying inclusion of cases, namely, retrospective versus prospective collection from surgical records or national databases. 2 These differences make it difficult to meaningfully compare rates between studies and regions or to compare changes over time.
Studies which have reported long-term changes in incidence of amputation show a general trend toward a decreasing rate.3–9 Most studies focus on amputations in people with diabetes. 1 For the Netherlands, a reduction from 550 to 363 amputations per 100,000 people with diabetes was reported. 10 Whether this decline is consistent in people without diabetes is unknown.
Investigating population changes can give insight into whether preventive intervention and rehabilitation services are being provided effectively and to the right population. In order to look at changes in amputation for people with and without diabetes, while avoiding the limitations in comparing rates across studies, we replicated an earlier study in the Northern provinces of the Netherlands. 11 In addition, using the same methodology as that study, we reviewed the medical records directly, gaining deeper insight into individual factors that are available in the national database in which preamputation history is not available and side of amputation is not stated.
The aim of this study was to report the incidence of first transtibial amputation, knee disarticulation, or transfemoral amputation in 2003–2004 and the characteristics of this population, and to compare these outcomes to an earlier cohort from 1991 to 1992. 11
Methods
Data collection
The medical ethics committee of University Medical Center Groningen ruled that a formal application and approval was not required for a retrospective medical record review.
The study was conducted in all 14 hospitals of the three Northern provinces of the Netherlands: Groningen, Friesland, and Drenthe. This region had a total population of approximately 1.7 million people in the study period of 1 January 2003 to 31 December 2004. 12
Data collection was matched to the previous study. 11 The population included from the previous study was modified and data were reanalyzed, focusing only on transtibial level and above. Each hospital compiled a list of people who had a transtibial amputation, knee disarticulation, or transfemoral amputation in 2003 or 2004. People who had an amputation at any of these levels before 1 January 2003 were excluded. People with a previous amputation distal to and including ankle disarticulation were included. Where multiple amputations occurred within the study period (either reamputation to a higher level or a bilateral amputation), cases were counted once, and the highest level of amputation is presented. Amputations that were the result of trauma, cancer, complex regional pain syndrome, or congenital causes were excluded, thus leaving a cohort with amputation resulting from vascular disease or infection, with/without diabetes. Medical records for all cases were reviewed between August 2010 and June 2011. The years 2003–2004 were chosen as major changes in the way that data are recorded in the Netherlands occurred from 2005 onwards. This presented concerns on the reliability of data from later years that would not have enabled the direct comparison to our earlier cohort.
Analysis
The original dataset was obtained from the authors of the 1991–1992 study for analyses. 11 Population data were obtained from the Central Bureau of Statistics (CBS), 12 including the number of people residing in each province, and their age and sex. There are no large ethnic groups in the region requiring separate analyses. The population structure in our region did not change substantially from 1991–1992 to 2003–2004, with 2% more people aged ≥45, and 0.7% more people aged ≥75 years, 12 so actual (crude) incidence rates are presented for comparison of the two time periods. Age-adjusted rates were checked and presented no differing results, and thus, they are not presented.
The population with diabetes was estimated from prevalence rates obtained from the CBS for the years 2003 and 2004 separately. These prevalence rates are only available for the population aged ≥45 years. The majority of the population aged <45 years is not considered to be at high risk of amputation resulting from vascular disease or diabetes (although admittedly, there are exceptions), Therefore, it was reasonable to exclude these younger cases from the denominator in calculating incidence of those with diabetes. The population without diabetes was calculated by subtracting the estimated population with diabetes from the total population for each year. A total-population incidence rate is also presented, for comparison to other studies.
Population-based incidence rates were calculated per 100,000 person-years, for the seven different age and sex categories, with a Poisson distribution assumed for calculation of the 95% confidence interval (CI).
Age was compared using t-tests and categorical variables, and incidence rates were compared with chi-square tests. Statistical significance for all analyses was set at 0.05. Analyses were performed using Microsoft Excel 2003, PASW Statistics 18 and Confidence Interval Analysis version 2.2 (Trevor Bryant, University of Southampton).
Results
A total of 342 people underwent transtibial amputation, knee disarticulation, or transfemoral amputation due to vascular disease, infection, with/without diabetes, in 2003 or 2004. A total of 43 people were excluded as they had undergone amputation proximal to the ankle before the study period. This resulted in 299 people, the majority of which were men (60%), with a mean age of 74.0 years (Table 1).
Characteristics of people with first ever major lower limb amputation in 1991–1992 11 .
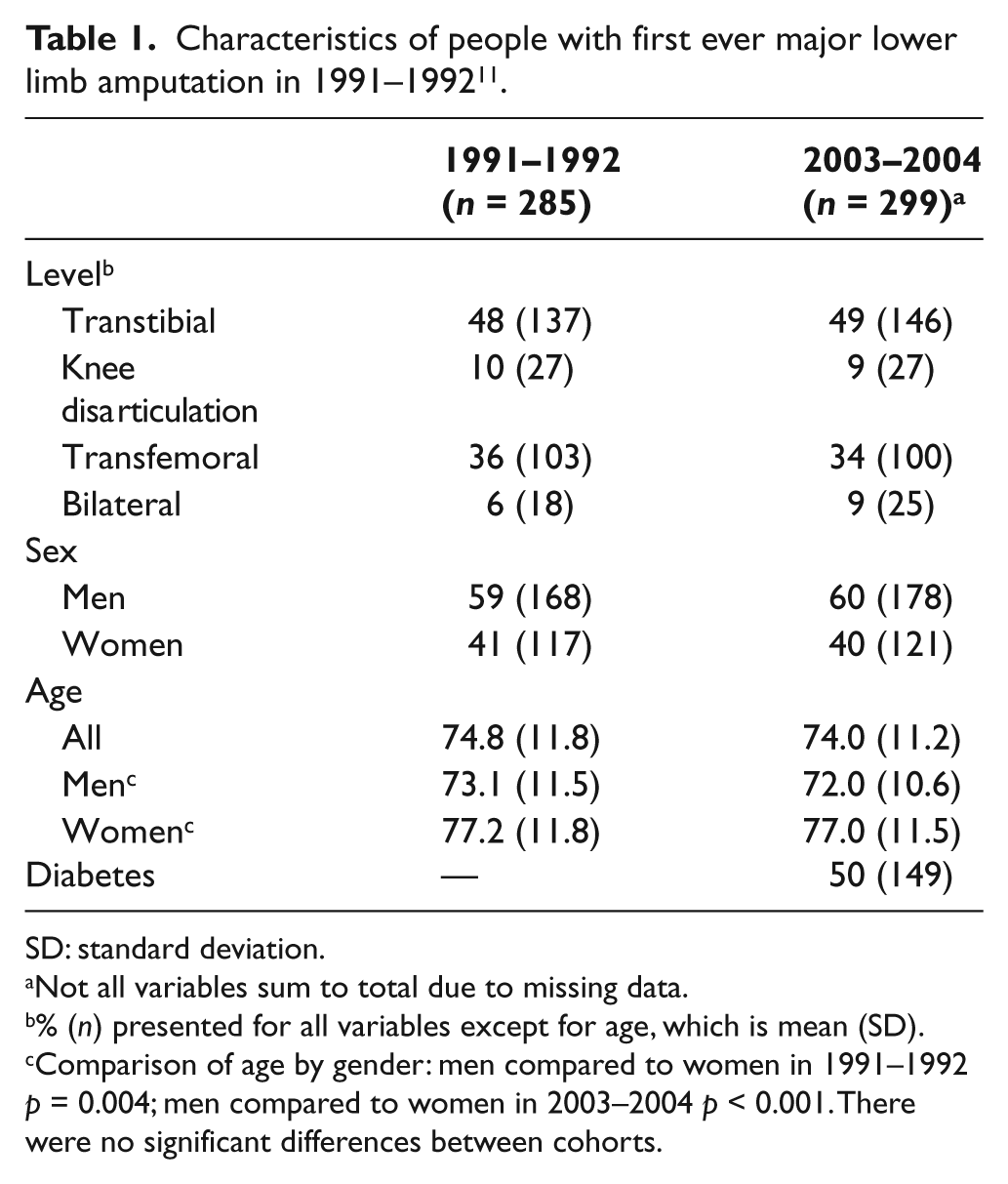
SD: standard deviation.
Not all variables sum to total due to missing data.
% (n) presented for all variables except for age, which is mean (SD).
Comparison of age by gender: men compared to women in 1991–1992 p = 0.004; men compared to women in 2003–2004 p < 0.001. There were no significant differences between cohorts.
The population characteristics of 2003–2004 showed no major differences compared to 1991–1992. A significant difference in age between men and women within each time period remained consistent: in 1991–1992, men were 4 years younger than women (73.1 years compared to 77.2 years, p = 0.004), and in 2003–2004, men were 5 years younger than women (77.0 years compared to 72.0 years, p < 0.001).
The 2003–2004 incidence for the all-age population was 8.8 per 100,000 person-years, and for the population aged ≥45, it was 23.6 per 100,000 person-years (Table 2). Incidence was higher in the older age groups. The incidence for the total population, as well as by sex and by age, showed no significant changes from 1991–1992 to 2003–2004 (Figure 1). The oldest group (≥75 years) had a reduced incidence of almost 12 per 100,000 person-years (from 80.4 to 68.8, p = 0.150).
Comparison of incidence rates for first amputation in 1991–1992 11 and 2003–2004.
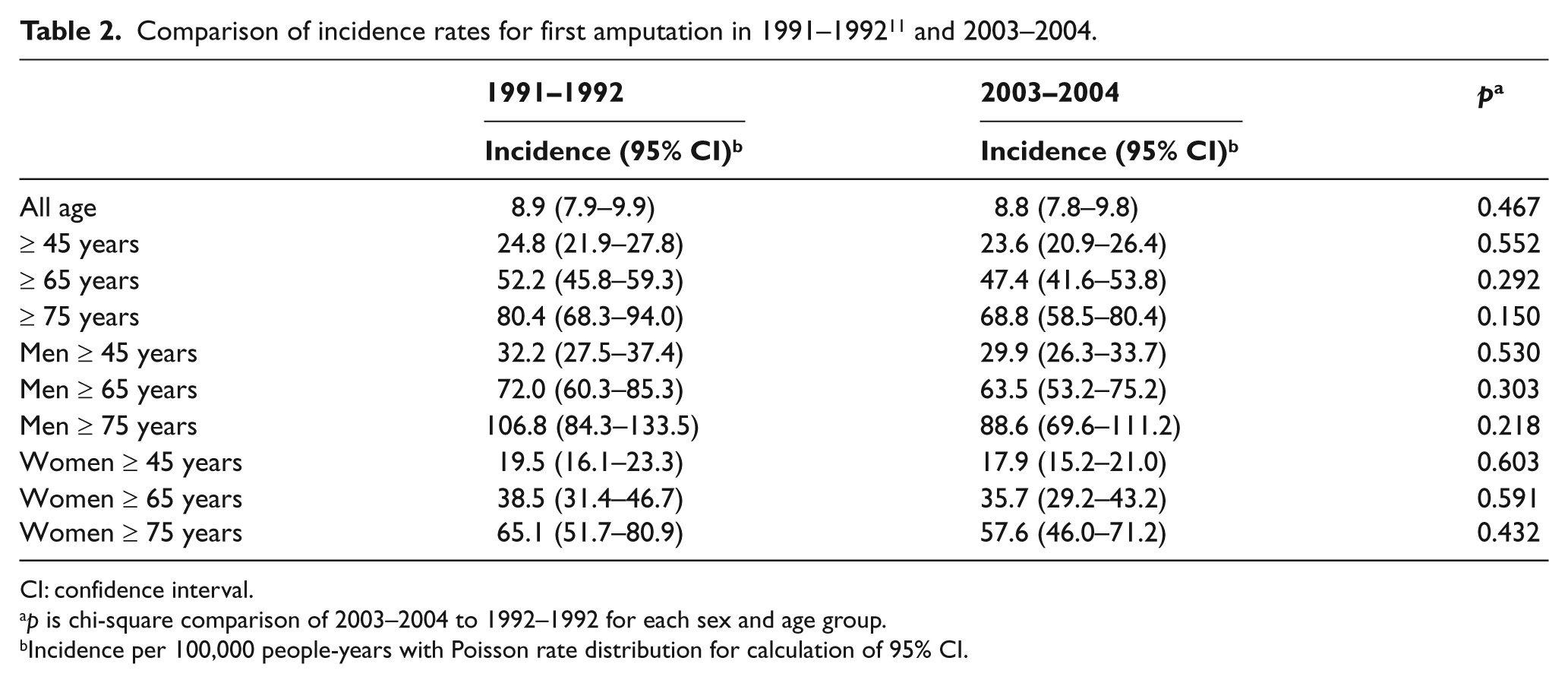
CI: confidence interval.
p is chi-square comparison of 2003–2004 to 1992–1992 for each sex and age group.
Incidence per 100,000 people-years with Poisson rate distribution for calculation of 95% CI.
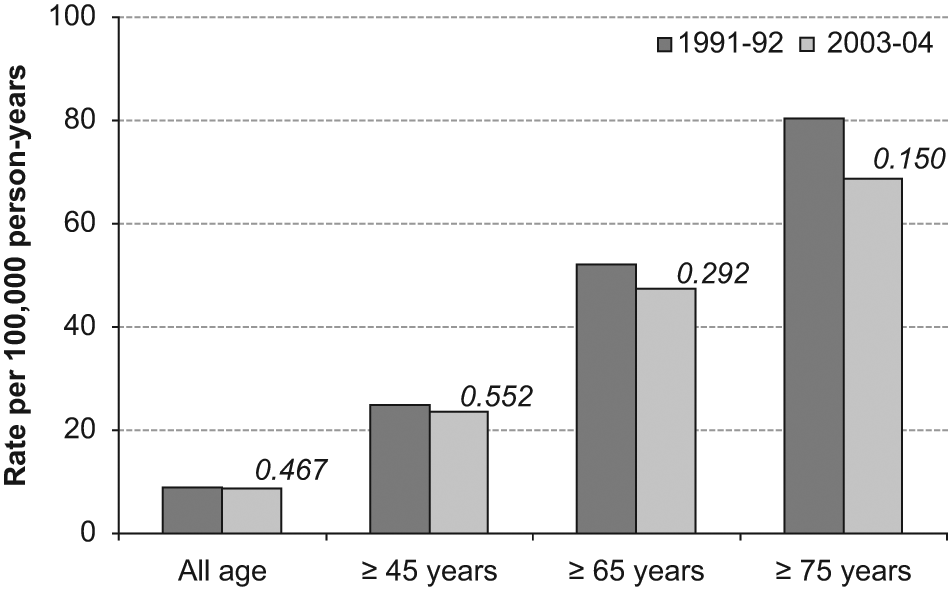
Change in incidence by age groups from 1991-92 to 2003-04. The p are presented from chi square comparison, seen in Table 2.
Diabetes was diagnosed in 50% of people with amputation in the period 2003–2004. The ratio of transfemoral and knee disarticulations to transtibial amputations in people without diabetes is 2:1, whereas the ratio in people with diabetes is 1:1 (p = 0.017; Table 3). Women with diabetes were 3.1 years younger than women without diabetes (p = 0.095). Men were significantly younger than women both in people with diabetes (71.4 years compared to 76.4 years, p = 0.003) and without diabetes (73.0 years compared to 79.5 years, p < 0.001).
Characteristics of people with lower limb amputation aged ≥45 years with and without diabetes.
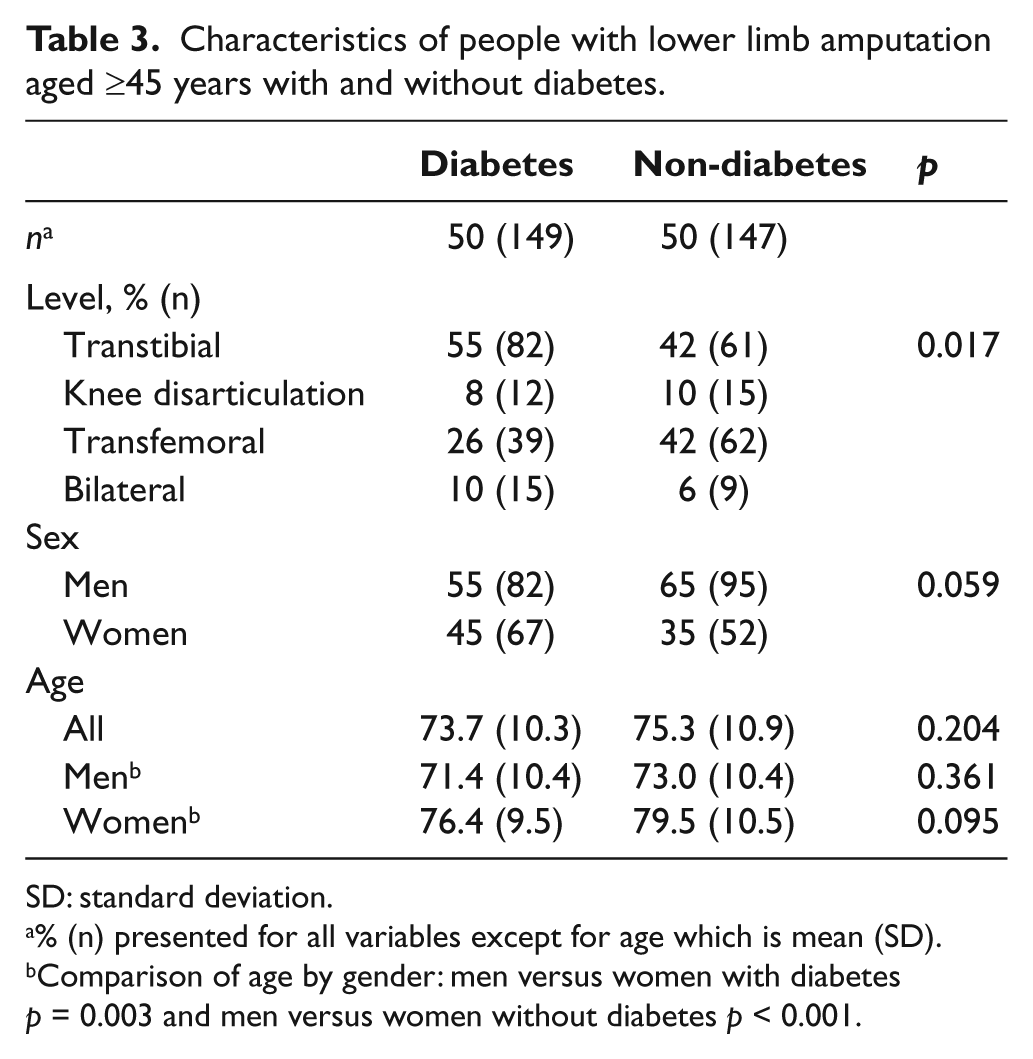
SD: standard deviation.
% (n) presented for all variables except for age which is mean (SD).
Comparison of age by gender: men versus women with diabetes p = 0.003 and men versus women without diabetes p < 0.001.
For people aged ≥45 years with diabetes, the incidence of amputation was 150.9 per 100,000 person-years, a relative risk (RR) 12.3 (95% CI: 9.7–15.4) times higher than people without diabetes (Table 4).
Incidence of people with first lower limb amputation aged ≥45 years, with and without diabetes.
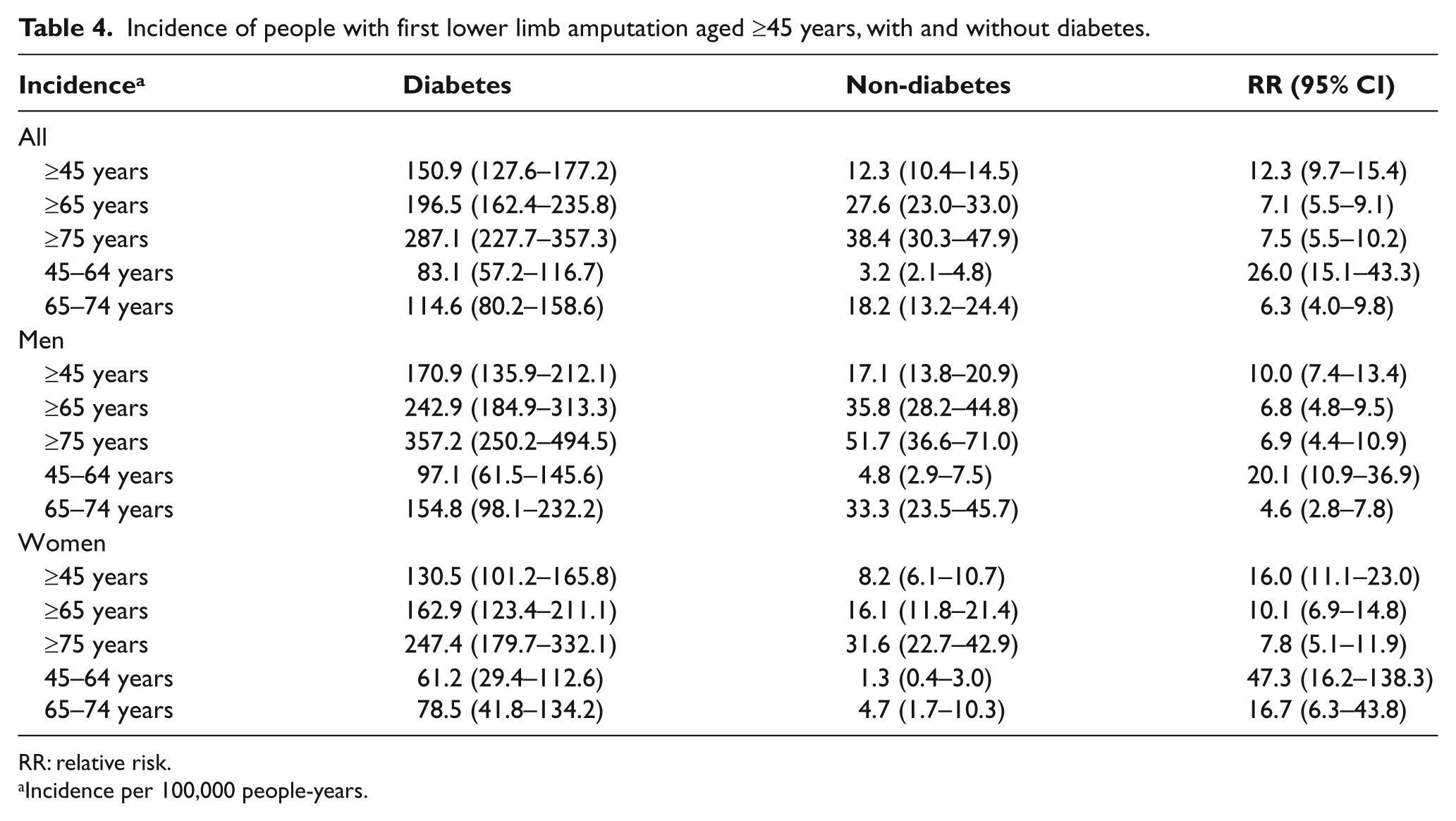
RR: relative risk.
Incidence per 100,000 people-years.
Discussion
Taken as a single time point, the amputation incidence of 23.6 per 100,000 person-years aged ≥45 years can be considered as moderate, falling in the middle of other population studies that have been presented in two systematic reviews.1,13 Although the rate has declined slightly over time, the lack of any statistically significant reduction in the incidence of amputations in our population is of concern and supports a need to investigate the adequacy of multidisciplinary prevention programs and interventions to save limbs. While there are others who report no change in amputation rates,14,15 most research supports an overall trend toward a significantly declining incidence.3 –9
Reasons for unchanged amputation incidence rates must be carefully considered in order to build effective care strategies. It was expected that there would be a shift toward an older age for people undergoing their first amputation as more interventions aim to prevent or delay the procedure. Although this has been reported in other populations, 14 there was no change to the mean age at the time of first amputation in our region. The oldest group of patients appeared to have a reduced incidence, yet the overall rate remained unchanged. A possible explanation is that the surgeon and patient chose not to pursue amputation as a treatment in the older population, or people may have already undergone amputation at a younger age. A decision on when to amputate is made through the combined efforts of medical staff and the patient’s own situation and wishes. Exploration of the individual motivations behind these decisions could offer insight into some of the differences in incidence rates over time, and across different regions.
In Europe, throughout the 1990s, the frequency and quality of multidisciplinary foot care continued to increase, 16 and there was a concerted effort made to reduce diabetes-related amputations through the St Vincent’s Declaration. A study conducted in a separate region of the Netherlands showed that referral of patients at risk to multidisciplinary foot clinics, at least up until the year 2000, was very low. 17 These results, together with our findings of no change to incidence in the time period, support a need to investigate the provision of vascular services and foot clinics in more depth.
Diabetes was diagnosed in 50% of the 2003–2004 cohort. The RR of amputation was 12 times greater in people with a diagnosis of diabetes than the risk of amputation in people without diabetes. This risk is higher than reports from other Western economies, including Germany, Finland, and Sweden, where RR is reported as approximately 7–10 times greater for people with diabetes.6,18,19 Those studies had similar populations to ours based on the inclusion criteria. Therefore, it appears that for people with diabetes in the Northern Netherlands, the RR of amputation proximal to the ankle might be slightly higher than in comparable Western regions. Regrettably, there were no data concerning diabetes available from the 1991–1992 study, and so the impact of this important diagnosis on our unchanged incidence rate cannot be determined. A nationwide study in the Netherlands demonstrated a decreased rate for diabetes-related amputation from 1991–2000. 10 If this reduction is consistent for our region specifically, then we need to look at why the changes are not being reflected in the overall incidence rate, specifically for amputations due to peripheral arterial disease.
The current study was limited to the Northern provinces of the Netherlands, enabling direct comparison to the earlier cohort. However, there are known to be considerable regional variations in incidence rates of lower limb amputation (LLA).1,20,21 In addition, in order to match the methodology of the previous study, data presented are now somewhat outdated from 2003 to 2004, before a major change to the recording of these data was implemented. Both of these points, the region and timing of data collection should be taken into account in generalizing the results. Retrospective identification of LLA poses the inevitable chance of having missed cases. The incidence rates should therefore be considered as potentially underestimated, although any additional cases would not have an effect on our main outcome of no change over time. Our findings in relation to diabetes should also be considered as an underestimation as data were recorded from medical files, some of which had limited or missing information, particularly to distinguish between diabetes type 1 and diabetes type 2. All physicians are encouraged to carefully document this diagnosis to enable differentiation between the two in future work.
Our results were suggestive that a small decrease in incidence had occurred but without statistical confirmation, which is possibly due to the small amputation population size. A repeat study with a recent cohort should be performed, with recognition that the data collection procedures in the Netherlands have changed. This study should aim to evaluate whether the lack of change in incidence was due to chance or a slower implementation of changes in care and prevention, or if indeed we need to seriously consider the services being provided to people with vascular disease and diabetic foot problems.
Conclusions
Our findings of an unchanged incidence need to be investigated further with respect to the provision of services from a range of disciplines, including vascular surgery, diabetes care and multidisciplinary foot clinics. The risk of amputation in people with diabetes in 2003–2004 was high but should be confirmed through a follow-up study. Finding effective methods for reducing the rate of amputation is imperative with diabetes and general population aging presenting an increased number of people at risk.
Footnotes
Acknowledgements
For their active involvement in the studies, we thank the surgeons and colleagues from all hospitals in Drenthe, Friesland and Groningen. We also thank Ms Anoek Teunissen and Mr Koen Esselink, student assistants, for their help with data collection.
Conflict of interest
None declared.
Funding
This work was supported by grants received from the Foundation Beatrixoord North Netherlands and Foundation OIM, Assen (no grant numbers).