
Abstract
Background:
Prosthetic socket fit is an important element associated with successful ambulation and use of a prosthesis. Prosthetists and rehabilitation clinicians would benefit from an assessment tool that discriminates between and quantifies the multiple determinants that influence the lower limb amputee’s performance and satisfaction of a prosthetic socket.
Objectives:
To determine the internal consistency of the comprehensive lower limb amputee socket survey, a new self-report measure of prosthetic socket satisfaction that quantifies suspension, stability, comfort, and appearance.
Study design:
Cross-sectional sample of active amputees.
Methods:
Interviews were conducted with prosthetists, physical therapists, and lower limb amputees to identify clinical concerns and common activities influencing socket fit. An expert panel of five clinicians reviewed the items and constructed the original version of the comprehensive lower limb amputee socket survey which was then administered to a convenience sample of 47 active lower limb amputees. Item analysis and Cronbach’s alpha were used to determine the final version of the comprehensive lower limb amputee socket survey.
Results:
Following item raw score-to-total score correlation with Cronbach’s alpha for comprehensive lower limb amputee socket survey determinants, internal consistency improved when nine questions were eliminated.
Conclusion:
The comprehensive lower limb amputee socket survey is a self-report measure of prosthetic socket satisfaction with very good internal consistency.
Clinical relevance
When socket problems occur, the ability to determine the specific cause can reduce modification time, enhance socket fit, and promote patient satisfaction. A standardized multi-dimensional assessment measure of socket satisfaction enables prosthetists to quantify the multiple determinants of socket satisfaction, improve patient communication, and demonstrate the value of socket interventions.
Keywords
Background
The literature often addresses the importance of securing a good prosthetic socket fit to achieve successful ambulation and satisfaction with prosthetic usage.1–3 Both a comfortable prosthetic socket fit and successful usage of a prosthetic limb are associated with the ability of the lower limb amputee (LLA) to perform activities of daily living and return to work.4,5 Conversely, socket discomfort is associated with numerous visits to the prosthetic clinic to adjust a prosthetic limb with the goal of reducing pain and gait deviations. 5 The process of fabricating an optimal prosthetic socket fit for a LLA requires the technical and clinical skills of a prosthetist; in conjunction with accurate, detailed, and repeated feedback from the patient. The ability to determine the specific socket problem is necessary when developing an appropriate treatment plan, documenting the exact treatment intervention, and ensuring a successful prosthetic socket fit.
Comfort of the prosthetic socket as well as socket appearance contentment has long been recognized as important characteristics influencing prosthetic socket satisfaction.3,6 Currently, only one outcome measure has been specifically designed to evaluate prosthetic comfort, the socket comfort score (SCS) which is a single question with a 0–10-point analog scale that quantifies comfort of the prosthetic socket. 6 No psychometrics with regard to reliability were described in the original publication.
Hafner et al. published the first test–retest reliability of the SCS, reporting interclass correlation (ICC) values of 0.77–0.79, where differences were dependent on mode of administration, paper versus electronic. The SCS had the lowest ICC values of the self-report instruments administered and the authors concluded that a higher test–retest ICC values should be required to reliably assess intra-individual comparisons of socket comfort. 7 The SCS quantifies “socket comfort;” however, the interpretation of comfort remains ambiguous; moreover, the posture of amputee or the position of the socket in relation to the residual limb when discomfort occurs is not addressed.
Two prosthesis-related self-report measures that evaluate several domains that include questions specifically related to prosthetic fit are the Prosthetic Evaluation Questionnaire (PEQ) 8 and the Trinity Amputation and Prosthetic Experience Scales (TAPES). 9 The PEQ uses a linear analog scale response format. The PEQ asks one question about prosthetic comfort in standing and sitting, as well as the look of the prosthesis and choice of clothing because of the prosthesis. The TAPES use a 3-point Likert-type scale to determine satisfaction with prosthetic shape, appearance, fit, and comfort. None of the questions in the PEQ and TAPES refer specifically to the socket rather asking about the prosthesis as a whole. In addition, there are no questions relating to socket suspension and socket stability, structural and functional features that impact prosthetic comfort and performance.10,11
Suspension refers to the retention of the prosthesis to the body, specifically the residual limb. 12 Suspension can be affected by residual limb volume which can fluctuate because of compressive forces, weight-bearing activities, comorbidities, menstrual cycle, body composition, and dietary habits. 13 If the residual limb’s volume changes are greater than the suspension can accommodate, the skin of the residuum may experience an imbalance in compression and shear forces that may potentially lead to deep tissue injury. 14 Moreover, suspension is associated with decreased or increased translational, rotational, and vertical movement between the residuum and socket.10,15–17 Decreased prosthetic socket movement during swing is associated with improved stability; 10 while increased movement may reduce socket stability. 18
Many socket suspension designs are distinctive to each other with regard to materials, mechanism of suspension, skin interface characteristics, and donning/doffing requirements; yet there is no evidence to define which suspension system is best for a particular patient regardless of level of amputation.19,20 Each socket suspension design has advantages that work well for a selected LLA; however, all socket suspension prescriptions must consider the following: residuum shape, muscle strength, soft tissue, scarring, bone, changes in limb volume, the potential for skin issues, and activity level.10,15–17 Each of these issues can cause problems related to discomfort, altered suspension, and decreased stability. For example, silicone liners may vary with materials, thickness, and design. Thicker liners that were reported to be more comfortable were also associated with greater instability during walking. 21 Liners with a distal pin and a lock mechanism at the bottom of the socket can create excessive tension at the distal end of the residuum coupled with proximal compression influencing the sense of comfort to the skin and soft tissue.22,23
Stability is the dynamic postural response to applied or volitional perturbations. 24 Stability has been described with prosthetic alignment, 25 fitting, 26 feet, 27 and socket designs. 28 Stability is associated with postural control, or the ability to maintain balance and reduce abnormal sway that requires additional muscular effort. 29 The ability to maintain postural stability is important during sitting, standing, walking, and stair use to reduce muscular effort and maintain balance. Fatone et al. 30 reported that discrete changes to transfemoral socket stability did alter tissue loading and had meaningful affects with comfort as socket stability in the coronal plane explains 94% of the change in the SCS.
What is not known is which activities impact prosthetic stability and suspension. Common activities such as sitting, standing, walking, and negotiating stairs, in isolation or combination, could potentially alter the fit of the socket and impact stability, suspension, comfort, or the appearance. Currently, the process of evaluating a LLA’s prosthetic fit includes inquiry by the prosthetist regarding socket comfort during standing and walking. Modification of the socket often addresses only comfort during these two situations. By engaging the patient with an objective and repeatable measure of their perception of socket suspension and stability during specific activities such as sitting, ascending, and descending stairs, the communication of factors related to prosthetic utilization may be enhanced.
Sitting can alter socket comfort where the proximal brim can press into the skin anteriorly at the hip with the transfemoral amputee (TFA)31,32 and the posterior brim at the popliteal region where liner bunching can occur with transtibial amputees (TTA). 33 Physical activity in the general population declines throughout adulthood with more people choosing a sedentary lifestyle. 34 Sedentary lifestyle has been found to correlate with long durations of sitting watching television, playing games, and using computers. 35 Failure to address this aspect of the prosthetic socket may lead to dissatisfaction with the entire prosthesis.
Daily activities often include stair negotiation at home or in the community. This task is more demanding than walking on level ground and involves greater muscle forces, and greater movements at the hip and knee joints.36,37 Increased joint movement and muscle forces can increase pressure within the socket potentially affecting comfort and altering stability and suspension of the socket.20,30
Achieving a satisfactory prosthetic socket fit is a complicated process that can be frustrating for the patient and prosthetist. To promote a more effective experience and overcome this problem, it is essential to have an instrument that assesses socket satisfaction but also provides effective communication between the patient and prosthetist. 38 Such an instrument should facilitate repeated objective and measurable feedback by the prosthetic user during the fitting process enabling the prosthetist to precisely determine the exact cause and to quantify the degree of the problem related to the socket. Establishing the duration and frequency a fit problem can also be clinically helpful when assessing socket. Finally, a comprehensive outcome measure that quantifies change over time will enable prosthetists to demonstrate the value of their intervention to patients, referring physicians, and reimbursement agents.
The aim of the study was to determine the internal consistency of a newly developed measure of prosthetic socket satisfaction for people with lower limb loss called the comprehensive lower-limb amputee socket survey (CLASS).
Methods
CLASS development
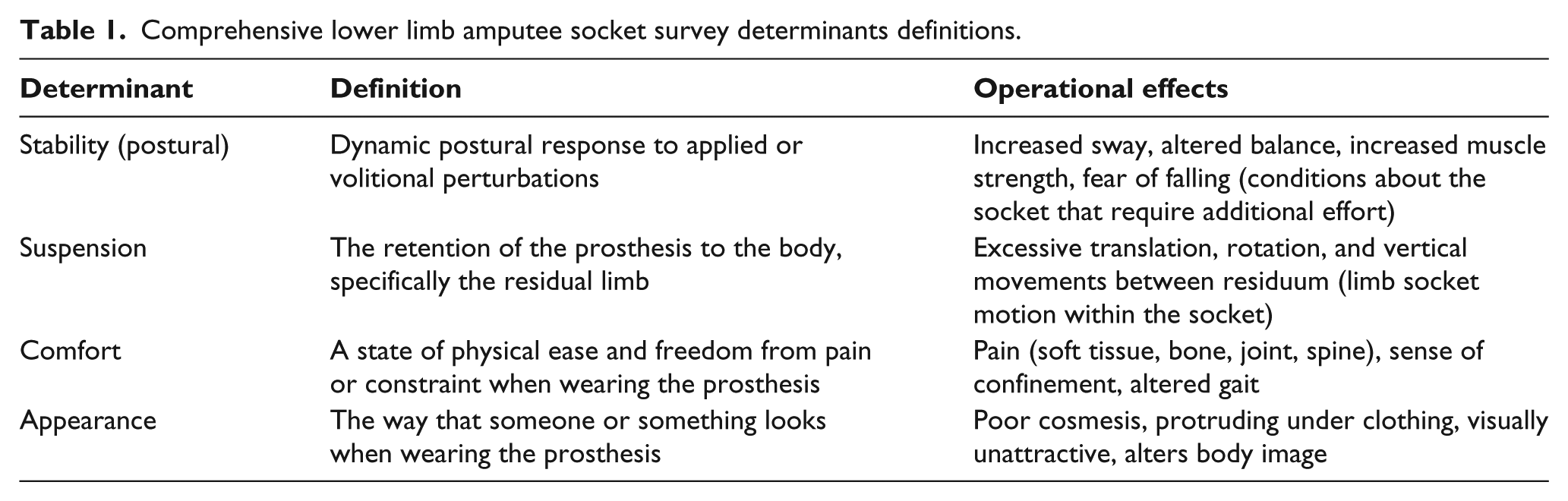
The CLASS was designed to be easy and quick to administer with a scoring system that would give clinicians insights for treatment and monitoring. A focus group of prosthetists, physical therapists, and people with limb loss were interviewed about clinical concerns with socket fit and common activities that typically occur. Following the focus group, an expert panel of five clinicians reviewed the items prior to and after testing. The 24-item survey, using positive language, includes four main prosthetic socket satisfaction determinants: (1) stability, (2) suspension, (3) comfort, and (4) appearance and application. Table 1 defines the four determinants of the CLASS. Each determinant is composed of six specific context items considered to be common functional activities: (1) sitting, (2) standing, (3) walking, (4) stairs, (5) running, jogging, and exercising, and (6) overall satisfaction of each determinant. Socket appearance and application differed slightly: (1) sitting, (2) standing, (4) wearing tight pants, (5) donning and doffing, and (6) overall satisfaction. The first five context items were scored using a 4-point Likert-type scale with response options and corresponding point value of strongly disagree (1), disagree (2), agree (3), and strongly agree (4). The last item of every determinant addressed the overall satisfaction and was scored using a numerical rating scale with values ranging between 0 and 5 points. The maximum possible score for each of the four determinants was 25 points.
Comprehensive lower limb amputee socket survey determinants definitions.
Once consensus of test items was determined, the CLASS was administered to unilateral LLA and feedback recorded as it related to the four determinants. Finally, a team of clinical experts reviewed the internal consistency results and participants’ comments to determine the most meaningful survey items for inclusion in the final CLASS. All revisions of the CLASS after data collection are discussed in the “Results” section.
Study protocol
A cross-sectional convenience sample of active unilateral LLAs was recruited at the Amputee Coalition National Conference in Greensboro, North Carolina, USA. Inclusion criteria for subjects include (1) independent ambulators, (2) aged 18 years or older, (3) current prosthetic socket users, (4) at least 3 months in their current prosthesis, and (5) able to read the English language. Subjects were excluded if he or she was not using a prosthetic socket to ambulate. All participants received an explanation of the study and signed an informed consent approved by the Miami Veteran’s Affairs Institutional Review Board (identifiable information). Following instructions how to answer the CLASS, each participant went on to complete the survey on their own.
Data analysis
Descriptive statistics were computed using mean and standard deviation for continuous data, and frequencies for categorical variable items. Item analysis was performed using Cronbach’s alpha to determine the internal consistency of each of the determinants: (1) stability, (2) suspension, (3) comfort, and (4) appearance and application. Data analysis was performed with SPSS Statistics 22.
Results
Fourty-seven LLAs met inclusion criteria and were enrolled in the study and completed the survey with their characteristics summarized in Table 2. The study population had a majority of women (55%). Trauma was the main cause for amputation (70%, n = 33), followed by dysvascular disease (13%, n = 6), tumor (11%, n = 5), and congenital (6%, n = 3). Most of the participants were active prosthetic users (Medicare Functional Classification Level (MFCL): K4 = 4%, K3 = 77%, K2 = 19%). Type of suspension varied where pin and lock were used by 45% of TTA and suction suspension was used by 41% of TTAs and 67% of TFAs. Other suspension mechanisms used included seal-in liners (3% of TTA and 11% of TFA), vacuum (10% of TTA and 11% of TFA), and lanyard (5.5% of TFA).
Subject demographic for gender, age, and time since amputation.
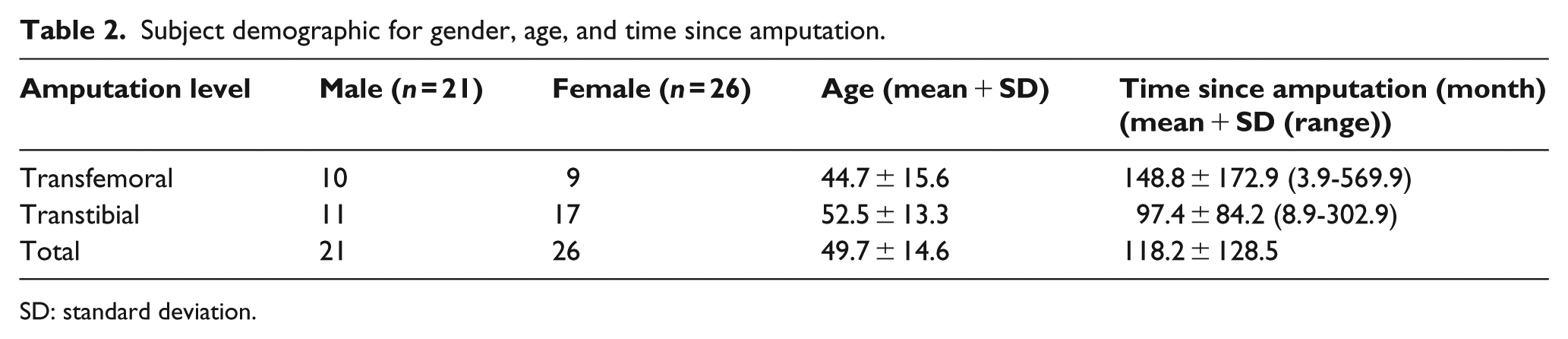
SD: standard deviation.
The four determinants of the 24-item CLASS demonstrated good internal consistency with Cronbach’s alpha ranging between 0.79 and 0.91. Following item analysis, the 24-item survey was modified to 15-item survey. In the (1) stability, (2) suspension, and (3) comfort determinants, removal of the running, jogging, and exercise item and overall experience item improved internal consistency of all three determinants (Table 3). Item total score correlations can be interpreted two ways: as an item discrimination or as an item validity coefficient. As an item discrimination, this coefficient indicates how strongly the item discriminates examinees with high and low total scores. Interpreted as an item validity, this coefficient depicts the predictive utility of the item’s ability to predict the subtest total (adjusted). In Table 3, for the stability determinant the standing item correlated .78 with the adjusted total, indicating that over 60% of the item variance overlaps with the adjusted total. Predictive utility estimates such as theses should range between .35 and .85 generally.
Item raw score-to-total score correlation with Cronbach’s alpha for CLASS determinants.
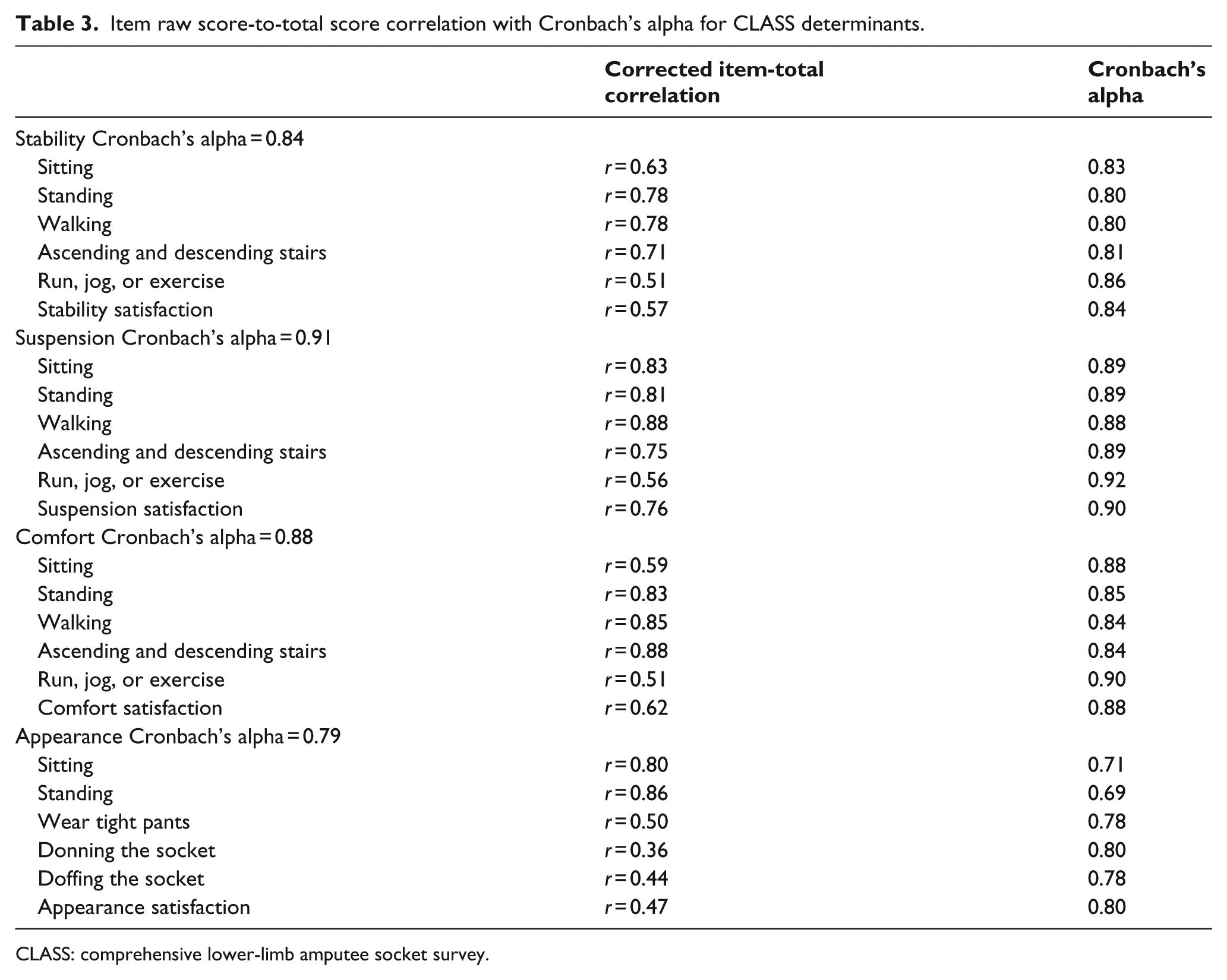
CLASS: comprehensive lower-limb amputee socket survey.
For the appearance and application determinant the total Cronbach’s alpha values improved when donning and doffing the prosthetic socket items were removed from the survey, eliminating the “application” items of the survey and now referred to as the “appearance” determinant. Table 4 presents Cronbach’s alpha of each construct before and after item-analysis.
Cronbach’s α values of CLASS determinants before and after item-analysis.
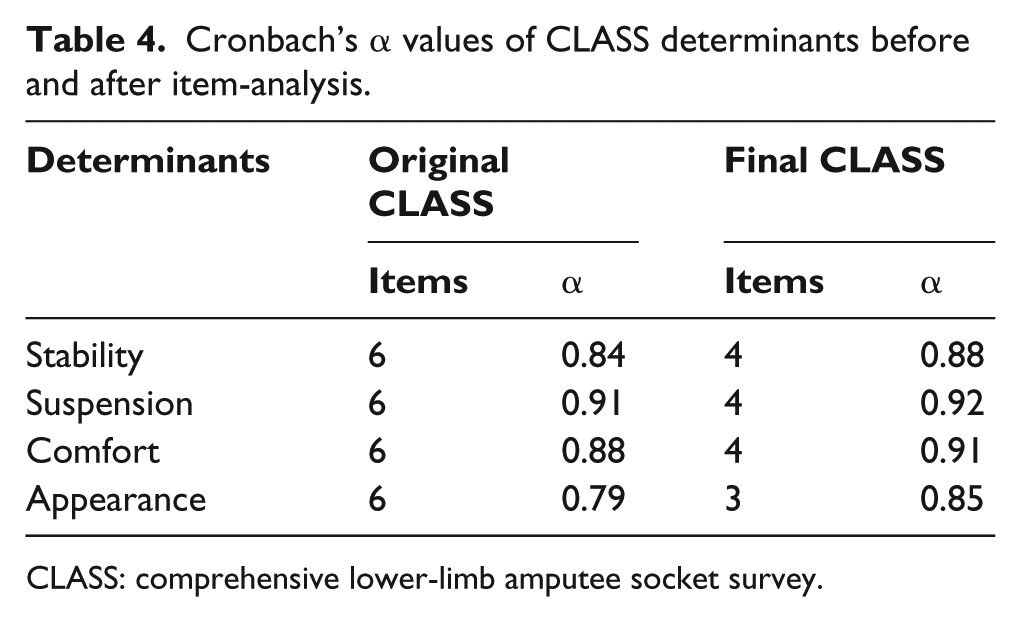
CLASS: comprehensive lower-limb amputee socket survey.
The final CLASS instrument is composed of 15 items across four determinants: (1) stability, (2) suspension, and (3) comfort with a maximum score of 16 points for each determinant plus (4) appearance with a maximum score of 12. Appendix 1 is the CLASS scoring form.
None of the subjects reported difficulty understanding the response options. One concern raised was related to the “wear tight pants” item where some people may not choose to wear tight pants and therefore, the “not applicable” response option would be appropriate. Furthermore, not all prosthetic users will negotiate stairs and some may use a prosthesis for sitting only. Consequently, the “not applicable” option was added to the CLASS.
Discussion
Item analysis of the CLASS determinants revealed that socket satisfaction should not include questions regarding running, jogging, or exercising. It is possible that some of the participants in this study did not engage regularly in running or jogging as these activities are not considered the preferred sports by LLAs. 32 Therefore, the expert panel decided that this item was not appropriate for this survey, as a result, the item was removed and the Cronbach’s alpha score improved for each determinant. As previous described, the internal consistency for the appearance determinant improved when the donning and doffing item was removed suggesting that this item is not related to the other items within the determinant (i.e. sitting, standing, and wearing tight pants).
Current literature on prosthetic satisfaction has primarily focused on measuring socket comfort, appearance, and prosthesis-related quality of life issues.3,6,8,9 While these outcome measures successfully evaluate the level of socket comfort and quality of life of LLAs, they do not provide direct interpretation for clinicians to determine when socket issues occur and which determinants are affected. This type of information is beneficial for the prosthetists to make necessary modifications. The availability of an instrument that can differentiate between the activities and severity of socket issues can assist prosthetists with the treatment to resolve the problem.
The CLASS was designed to provide an effective means of communication for the patient to describe with clarity, the quality of their socket fit during common activities. Typically, the patient does their best to describe a socket issue and the prosthetist makes every effort to modify the socket based on their understanding of the patient’s explanation. However, confusion may arise if patients and practitioners do not have a standardized language. For instance, one practitioner may assess suspension by asking the patient about the number of sock ply, another may ask about difficulty with donning the socket, a third might ask, “does the socket feels sloppy” and the patient could reply with a totally different descriptor such as “the socket is too loose or too tight.” The variation in terms may diminish understanding or the interpretation of meaning between practitioners and patient or between colleagues treating the same patient. By consistently using similar terminology within the clinic, all involved will be able to consistently discuss issues pertinent to suspension, stability, comfort, and appearance and when the problem occurs, during sitting, standing, walking, or stairs, therefore, the clinician can focus on the precise modification that is required.
A convenience sample of active LLAs was recruited to determine the internal consistency of survey items of the CLASS. Because of the small sample of this study, especially the small sub-group of those with limb loss for dysvascular reasons it is not possible to determine the generalizability to all populations for socket fit satisfaction. 39 Likewise, with the absence of LLA’s assigned to the MFCL K1 category and a small percentage of K4, it is unclear what differences, if any, would apply to amputees with lower or higher functional capabilities. The test–retest reliability and validity of the CLASS as an outcome measure of prosthetic satisfaction for all functional levels of LLAs should be established. It should be noted that formal cognitive interviews were not performed.
Conclusion
In today’s healthcare environment, the benefit of every clinical intervention must be demonstrated to the consumer, clinician, and payer. Moreover, people with limb loss should be able to objectively report their level of satisfaction with their prosthetic socket. The CLASS is a reliable, quick, and easy patient report measure that evaluates static and dynamic features of socket stability, suspension, comfort, and appearance.
Footnotes
Appendix 1
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.