
Abstract
Background:
Surfing with transfemoral knee prosthesis requires flexion of the hip, knee, and ankle and balance between flexibility and stiffness of the prosthetic limb. We report on Mr D, a transfemoral amputee, who wanted to surf again.
Case Description and Methods:
Technical specifications were based on Mr D’s complaint. The prosthesis is salt water resistant and combines a shock absorber associated with elastic tendons to permit the knee to bend easily and to facilitate eccentric braking. Surfing was observed using videos of movements and subjective analysis of compensations.
Findings and Outcomes:
Mr D uses this prosthesis for surfing with good results and got back to his former level using compensations. During the takeoff, he cannot shorten his left leg. He makes a circumduction movement to put his leg in front of the board.
Conclusion:
This prosthesis is adapted for surfing and allows precise adjustments to surfing conditions.
Clinical relevance
Appropriate prosthesis design can enable return to surfing for a transfemoral amputee.
Background
During surfing, the lower body is active during three phases: arm paddling, takeoff, and riding the waves. When a wave is caught, the surfer must quickly stand up and perform maneuvers. 1 These actions require ankle dorsiflexion and flexion of knee and hip joints, and balance between flexibility and stiffness of the lower body muscles. To perform these actions, neuromuscular skills such as agility, balance, muscular power, and flexibility are important.1,2
These motions are difficult for people with a lower limb amputation. A few varieties of transfemoral prostheses are designed for board and extreme sports: the Procarve II© of Chabloz Orthopedie (Fr) for skiing, 3 the Moto Knee© of Biodapt (USA) 4 for motorcycling, and the XT9© of SymBiotechs (USA) for most sports. 5 These prostheses allow knee pre-flexion to make movements easier and improve stability while allowing knee flexion movement.
However, in surfing, environmental conditions are unpredictable, the surfer has to evaluate the wave and execute the maneuvers considering each wave as unique and requiring constant adaptation to varying situations.6–8 Unfortunately, the current prostheses cannot be precisely adjusted to environmental conditions directly on the beach. Moreover, they are often too heavy and not salt water resistant.
In this article, we introduce a prosthesis that is adapted to surfing. To our knowledge, no surfing prosthesis has been proposed for individuals with a transfemoral amputation.
Case description and methods
Subject
Mr D, a 35-year-old active man, is a non-professional surfer of good level. He had no previous medical history. In 2011, he was the victim of a shark attack in Reunion Island while surfing and he had a supracondylar amputation. The man underwent numerous months of physical therapy and could walk with a prosthesis composed of a C-Leg knee© and a Vari-Flex© foot.
His main presentation was an inability to surf after his initial rehabilitation and prosthetic management. Concerning the impairment, clinical examination of the left lower limb showed an amputation of the last third of the thigh. The stump was long and fine with a distal edema. His hip flexor was amyotrophic: his left thigh perimeter was 5 cm shorter than the other side. Strength was reduced for the hip flexor, hamstring, and gluteus medius muscles. Sensory abilities were normal. Hip extension was 0°. Different types of pain were observed. The most problematic were neuropathic pains: phantom pains and stump electric discharges at 8/10 (Numeric Rating Scale (NRS)), lumbar pain at 6/10 (NRS), and intense mechanical and friction pain between the stump and the socket at 8/10 (NRS).
Standing balance on the prosthetic limb was less than 10 s. Standing on both lower limbs and gait parameters were typical of other people with similar amputations. Outdoor walking analysis showed severe neuropathic pain after 1000 m.
Mr D’s impairment led to several difficulties with surfing. First, it was usually far from his car to the sea and walking was more difficult because of the irregular ground and sand surface. He had difficulty with all the phases of surfing: arm paddling, taking off, and riding waves.
Technical specifications were established on Mr D’s complaints. Mr D provided consent to participation and to publication of the results of this case study.
Prosthesis
The aim of the prosthesis design was to facilitate surfing. The prosthesis consisted of a socket connected to the 1P600 Bartlett Tendon Knee (BTK©) from Fabtech Systems, a short leg segment, and a foot (Figure 1).

Prosthetic leg. From top to bottom: the socket, the prosthetic knee, the leg segment, and the prosthesis foot.
The socket
The ischial containment socket weighs 1300 g and is in Streifyflex©, derived from low-density polythene associated with a carbon fiber support. Waterproofing was aided by a depressurization valve at the bottom socket extremity and a silicon sleeve at the top socket extremity. The anterior part of the socket was reduced to decrease the conflict between the socket and the anterior superior iliac spine during the takeoff.
The knee
The prosthetic knee must fulfill two conditions to be adapted to surfing. In swing phase, it must be flexible enough for fast flexion so that a surfer could bend the knee easily. In stance phase, it must be stiff and stable enough to ensure stability so that the surfer could stand on the prosthetic leg and have an eccentric braking action. If the knee is too flexible, it may suddenly collapse and cause a fall. If the knee is too stiff, the surfer will not be able to bend the knee and cannot surf correctly.
The BTK from Fabtech Systems is monocentric. It weighs 900 g and is 25.6 cm long. The materials used are anodized aluminum, stainless steel, and carbon. The maximum weight supported by the prosthesis is 125 kg. It combines an air/oil shock absorber associated with an elastic tendon on each side of the knee. The shock absorber Monarch 4.2© of RockShox was developed for mountain biking. It has oil and air chambers in which the pressure can be set between 14 and 275 lbf/in2 (Figure 2(b)). The hydraulic/pneumatic components slow down the movements of flexion and extension of the knee. It is fixed to the swiveling base of the knee and to the fixed frame. Shock absorber settings are adapted to the weight and to the activity through a pump, a ring, and a thumb wheel. The pump adjusts the pressure level in the shock absorber. The ring adjusts the speed of the flexion and the thumb adjusts the extension return.
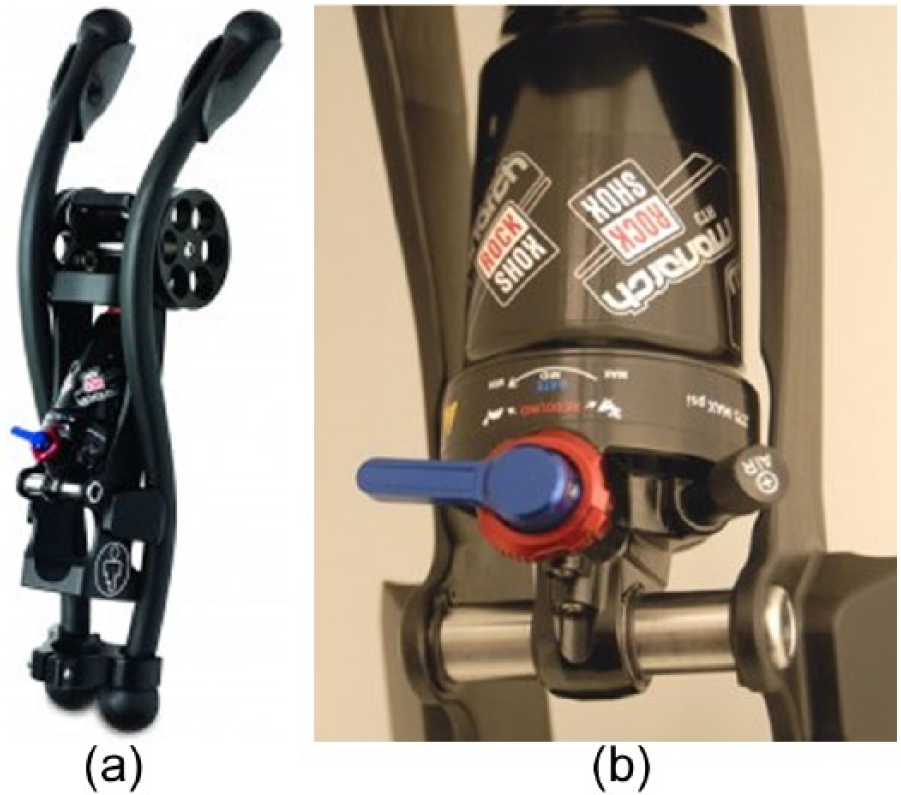
Knee components: (a) BTK© prosthetic knee (Fabtech system) and (b) Monarch 4.2© shock absorber (RockShox).
During knee flexion, elastic tendons help the shock absorber in eccentric braking. They take part in the restoring force of the knee during extension. They are fixed to the front of the socket. The trajectory is parallel on both sides of the knee. In the lower extremity, they are hung on a part fixed to the leg segment, at the back of the knee axis. This part slides along the leg segment and adjusts elastic tendon tension.
Elastic tendons are made up of polyurethane. There are two types: stiff and soft. The choice depends on the activity and on the flexibility desired. Usually, Mr D uses a flexible elastic tendon and a stiff elastic tendon at the same time to achieve a progressive flexion resistance. From 0 to 20 degrees, the soft tendon moment is higher than the knee flexion moment. He cannot bend the knee so a pre-flexion is required. Beyond 20 degrees, the soft tendon stretches and then the stiff one begins stretching beyond 30 degrees until a stable position at 35–40°degrees is reached, when the moment of knee flexion is equal to the sum of the moments of the elastic tendons. Intensity of force can modify the knee flexion angle.
Two extension stops allow knee pre-flexion to facilitate the beginning of the movement. Also, they prevent knee overextension. Elastic tendons articulate on fixed pulleys, in front of the axis of the knee.
The ankle and foot
The ankle–foot pair has to allow movements of flexion–extension and inversion–eversion. The FLEX Walk© foot from Össur is made up of composite glass fiber and carbon (Figure 3). It weighs 550 g. It has a pyramidal connection with a 6-mm-thick split-toe. It mimics the midfoot joint in the front and the rearfoot joint in the back.

The prosthetic foot on a non-slip toe, which is enlarged on the medial part.
The non-slip sole is made up of airlite and is 10 mm thick. The upper face is smooth and stuck to the carbon blade, and the non-slip underside of the sole is in contact with the board. The medial part of the sole is enlarged to always be in contact with the board during the inversion movement of the foot.
Findings and outcomes
In surfing, there are three phases with different biomechanical requirements: arm paddling, takeoff, and riding the waves. Arm paddling consists in rowing toward waves with the arms on both sides of the board and lying down on the trunk, legs slightly elevated. Knee pre-flexion prevents dragging the leg at the back of the board, which could decrease the paddling speed.
During takeoff, Mr D quickly switches from an extended position to a stand-up position. This phase requires a flexion of the hip and knee and dorsiflexion of the ankle. Mr D begins face downward, arms on both sides of the board. When the wave rises up, he straightens his trunk and puts his hands flat on the board. He leans on his superior limbs to be on all fours.
During the takeoff, he cannot shorten his left leg. He makes a circumduction movement to put his leg in front of the board. The previous shortening of the leg segment makes this step easier by reducing the cantilever of the prosthetic limb. The left hand moves to the right to let the prosthetic leg go in front of the board. This stable position is called drop knee: left leg in the front, right leg folded in the back, and upper limbs in support of the right side. When the surfer is steady, he gets up. He then leans on both his arms to switch his back leg from a knee position to a standing position. Then, he fully raises his belly and arms.
To ride waves, the prosthetic leg is at the front with the knee slightly bent. The shock absorber permits eccentric braking to bend progressively and tendons to provide eccentric braking and permit extension (Figure 4). Dorsiflexion and inversion provide permanent contact of the foot with the board.

Mr D achieves a stable flexed knee posture during surfing.
After assessing surfing conditions, Mr D adjusts prosthesis settings on the beach. He chooses tendons and adapts pressure in the shock absorber to surfing conditions and waves.
Mr D manages to surf 2.50-m-high waves, as high as waves he surfed before the accident, but with more difficulties. He uses a longer board that is larger at the back to facilitate stability and management with the foot at the back. He uses the prosthetic leg with other specific settings for other sports: paddling, mountain biking, snowboarding, windsurfing, and skateboarding. He adjusts tendon types (stiff and soft), pressure in the shock absorber by a pump, speed of flexion with the ring, and extension return with the thumb.
Discussion
Mr D can surf again thanks to an adapted prosthesis and a set of movement compensations. Since the prosthesis is not made for walking, he still has difficulties, especially when he goes to the surf spot. He limits walking as much as possible because of intense mechanical pains, by choosing a closer beach or by swimming to the surf spot.
Concerning quality of life, Mr D suffers from neuropathic pains and phantom pains that resist treatments. He also suffers from post-traumatic stress disorder (PTSD). He says that surfing is the only moment when he has no pain and this reduces his anxiety. These observations support reports of surfing facilitating PTSD recovery. 9 People with functional difficulties who are involved in sport have a better quality of life than people who do not engage in sport. 10 Participation in sports helps amputees improve their physical condition and overall well-being.11–13
Few people use adapted sport prostheses. They are used mostly by competitive athletes. 11 The lack of scientific data on sport prostheses and prosthetic adaptations for sports other than running may be explained by the small number of amputees engaged in sports or physical activities.11,14 Scientific data are scarce concerning the efficiency, reliability, and functionality for most sport prostheses and prosthetic adaptations. 12
There is a constant evolution of this prosthesis according to Mr D’s progress and feelings. Further studies should investigate whether a flexible socket made totally of silicon could permit expansion of thigh muscle and prevent quadriceps atrophy. Flexibility of the knee must be developed. The curve of elastomer traction is logarithmic for slight stretching, which makes flexion harder, and a flexion point causes unlocking of the knee. The prosthetic knee could be used for other sports, like mountain biking, using a shock absorber that is adjustable during the activity, with two modes and a wheel: a free mode for free cycling and a hard mode comparable to the BTK knee. This would provide resistance and eccentric braking, for example, to climb a hill standing up on the pedals. Another shock absorber like the Procarve II prosthesis may be designed on the leg segment to facilitate shortening of the leg and eccentric braking. Finally, means must be found to reduce the price of this equipment and allow access to board sports for non-professional sportsmen.
Conclusion
This case report shows that a transfemoral amputee is capable of surfing again, with ability close to that before the amputation thanks to an adapted prosthesis. The BTK knee combines elastic tendons of different hardness with a shock absorber to mimic movements of flexion–extension of the thigh muscles. Mr D easily adjusts the prosthesis to surfing condition at the beginning of the session.
Footnotes
Acknowledgements
We thank BTC orthopedie Marseille for their participation in this study.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.