
Abstract
The objective of the trial was to evaluate the effectiveness of a short and intensive physiotherapy programme versus usual care, mainly consisting of walking. Fifty-eight male unilateral lower limb amputees were randomised over intensive care (N = 29) and usual care (N = 29); this study was carried out in a clinical environment, within the premises of the International Committee of the Red Cross, in Southern Myanmar. The amputees in the experimental group received a three-day programme built around 7 specific exercises, lasting approximately one hour altogether. Effects were assessed on: 2-minute walk test, physiological cost index (PCI), amount of weight bearing on both legs, 5 questions of the Functional Measure for Amputees questionnaire and the timed up and go test. Trans-tibial amputees were tested the first day they were fitted and then 2 days later; trans-femoral amputees were tested when walking out of the parallel bars and 4 days later. The experimental group showed significant improvement in the 2-minute walk test (p = 0.02), in the PCI (p = 0.02) and in the maximal weight bearing test on the amputated leg (p = 0.04). Despite limited means, research remains feasible in a developing country; this study has demonstrated that physiotherapy is effective in improving functional performance of lower limb amputees and therefore has its place in every rehabilitation centre.
Introduction
Background
Rehabilitation of traumatic amputees is unfortunately a current issue, as consequences of landmines are still a universal and growing problem. It is assumed that there are between 300,000 to 400,000 mine survivors in the world today, with 10 – 15,000 new casualties every year. Myanmar (former Burma) is one of the countries currently producing and using landmines (International Campaign to Ban Landmines 2004). The situation in Myanmar confirms the statement that “landmines injure both combatants and non combatants and that the likelihood of targeting civilians is increased because mines remain after the conflict” (Coupland and Korver 1991).
Especially when one is disabled, mobility is a basic physical, vital and social need and its optimal restoration represents an important goal of rehabilitation programmes (Franghignoni et al. 2004). The International Committee of the Red Cross (ICRC) recognises fully this need, and since 1979 rehabilitation is part of ICRC's activities. Within this context, the organisation is concerned with measuring the efficacy of physiotherapy and optimising costs as well as collecting data about amputee rehabilitation. Up to now, the information available was limited to prosthetics, monetary, qualitative values or descriptive statistics (e.g. number of amputees fitted). However, the ICRC feels that “the ultimate goal of rehabilitation is the reintegration of these persons into their environment to pursue daily activities promoting bipedal functional displacement”. No doubt that “quality of life includes walking again, successful prescription of prosthetic limb to allow maximal performance of the prosthesis, and participation in social activities” (Miller et al. 2001).
This programme was launched in summer 2002 within the setting of the rehabilitation centre in Hpa An, Southern Myanmar. The centre is directly managed by the ICRC with the oversight of the Myanmar Red Cross Society and the Myanmar Ministries of Health and Home Affairs. Directed by two expatriate prosthetists, the national staff employed by the centre is composed of 10 prosthetist trainees, 2 physiotherapy assistant trainees and 10 administrative personnel. Last year, this ICRC centre produced 701 lower limb prostheses and 623 pairs of crutches. The overall working conditions and standards are said to be satisfactory enough to justify promoting this centre as a model for the other 5 fitting places in Myanmar (International Committee of the Red Cross 2004). With the implementation of this rehabilitation centre, Myanmar recognised that the effects of landmines continue long after the conflict. “Loss of land, debt of families, payment of medical treatment, destabilisation of fragile economies and increased demands on the weak health system are some of the consequences of landmines, therefore adequate rehabilitation of amputees is important” (Giannou 1997).
Project goal and research question
This study aims at demonstrating the importance of adequate rehabilitation and is in line with the present trend in physiotherapy to assess its efficacy. It shall also demonstrate the feasibility of research projects taking place in developing countries. Its main goal is to evaluate the efficacy of a short and intensive physiotherapy programme versus usual care that essentially consists of supervised walking. Therefore, the research question studied is whether unilateral trans-tibial and trans-femoral lower limb amputees undergoing a short-term intensive physiotherapy programme perform better than the amputees under usual care.
Method and material
Setting
Planning of the study was conducted via ICRC headquarters, in coordination with Hpa An rehabilitation centre. National consent was not requested because treatments did not differ much from ICRC standards. Local authorities were informed in due time and no objections were raised. Study agreement and medical ethical approval was given by the ICRC Headquarters.
Population
Lower limb amputees eligible to participate in the study came from the local district and surrounding areas, taking advantage of the lack of professional activities during the rainy season. All stayed in the dormitory and received food for free. It should be noted that most of the amputees were not very eager to leave home, for reasons such as protection of their families, and therefore wanted to be fitted as quickly as possible. The majority had never received any kind of rehabilitation.
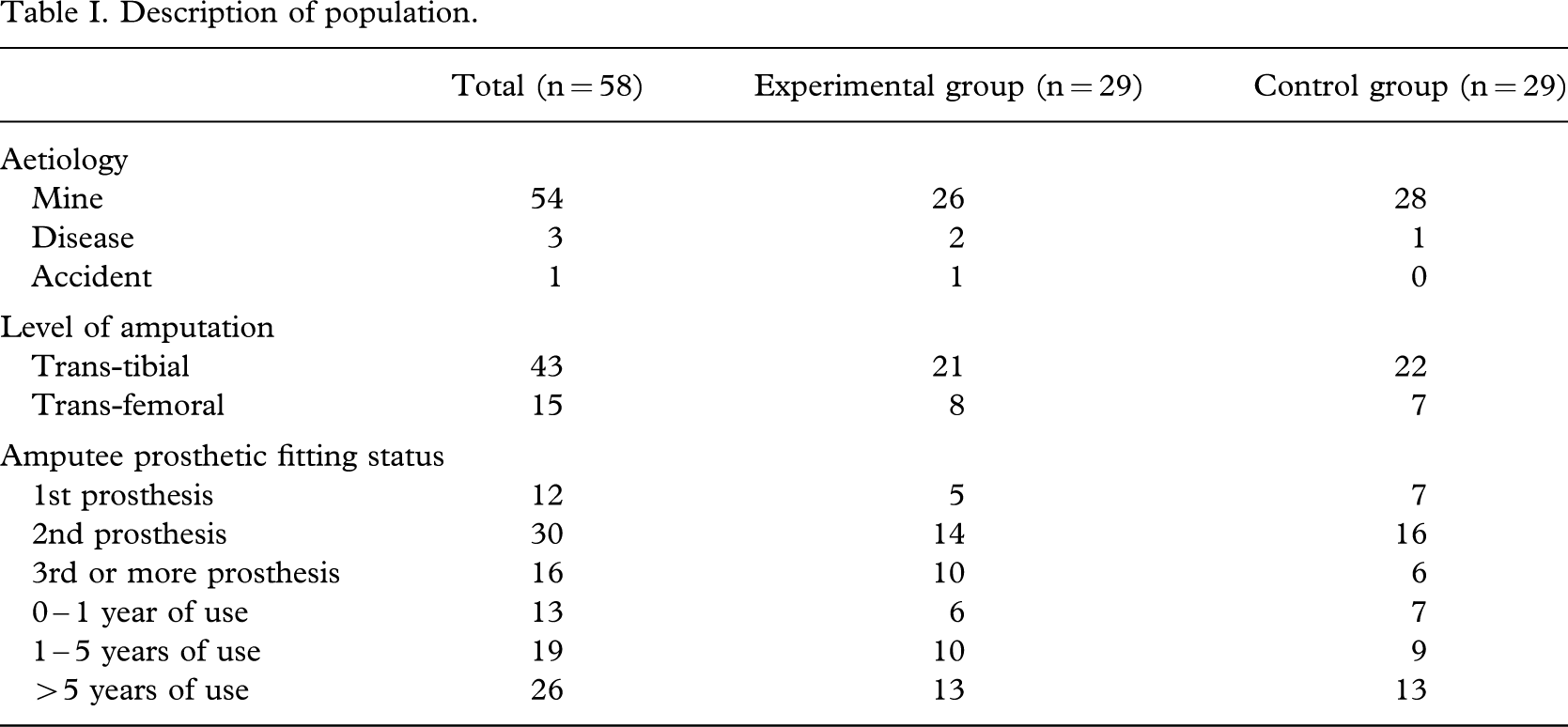
Patients were included when they were above 15 years of age, suffered from a traumatic or tumour related cause of amputation, had unilateral trans-femoral, knee-disarticulation, trans-tibial, ankle disarticulation or partial foot amputations, had never been fitted or had already one or more prosthetic device and were in good general condition. Amputees were divided into 2 categories of amputation levels: trans-tibial, people conserving their knee joint and trans-femoral amputees, those having lost their knee joint (Table I). The pattern for traumatic lower limb amputation was mostly walking on a mine and the level of amputation was mainly determined by the severity of injury, the delay of hospital arrival and the surgeon's capability (Coupland and Korver 1991). Patients with bilateral and hip disarticulation amputation, congenital deformation, impossibility to stay for 5 days post-fitting training, bad stump condition (e.g. sores or important contractures not allowing fitting), cognitive limitations, major cardiopulmonary affections and disagreement to give oral informed consent were excluded.
Description of population
Study design
In this randomised controlled trial (RCT), a randomisation list was generated by computer, with block size of four and provided by the department of epidemiology, Maastricht University. Allocation was concealed. Because of existing constraints (e.g. limited human resources or lack of experienced national staff), blinding of the assessors was not feasible. To assure maximal objectivity, the testers themselves did not record the results. Blinding of the patients was for obvious reasons impossible. It was intended to recruit 30 amputees per group for reasonable robust statistical calculations, given the limited research time of a three month period. Consecutive inclusion of the patients was made after initial assessment. Candidates were informed about the goal and protocol of the study and oral informed consent was requested. It was clearly explained that refusal to participate would not change their treatment and that results would be kept anonymous. Training of the national staff was done before the start of the study and the 10 first patients (not part of the RCT) were used for pilot testing.
Intervention
The experimental group underwent standardised individual intensive training, comprising seven exercises and lasting approximately one hour (maximum time possible considering daily normal workload and teaching). This specific training included lower limb strengthening exercises (e.g. using boxes and ladder), weight bearing (e.g. in position of rice planting), coordination tasks, corrected walking, obstacle management (e.g. walking on uneven ground) and functional training (e.g. carrying water). This setting was in line with Stolov mentioning that walking training should incorporate progressive weight bearing exercises (Stolov 1971).
Amputees in the control group received usual care which consisted mainly of walking under supervision. The training area of both groups was the same, apart from some strengthening and weight bearing exercises done indoors. Because of the centre's production schedule and personal constraints of amputees in Myanmar, maximal post-fitting training period was of 3 days for trans-tibial amputees and 5 to 7 days for trans-femoral amputees. Very few of the participants would agree to stay longer for training or for the study, but the majority of the patients used maximum time from 9 a.m. to 4 p.m. to walk on their own or play ball games.
Testing
During the 3 months, two Myanmar physiotherapy assistant trainees carried out the tests under the expatriate physiotherapist's supervision. One expatriate prosthetist was responsible for the overall fabrication and fitting of the prostheses. The equipment required for the tests included: 2 bathroom scales ( +/− 0.500 gr resolution, locally purchased), 1 centimetre measuring tape, 1 stopwatch (1/100 sec accuracy, bought in Switzerland), 1 locally produced wooden chair (adapted to fit the standards), plastic tape and 1 handmade sandbag. The centre's architecture offered a perfect space for testing, with a long corridor and sufficient space for the training. No co-interventions were allowed and all subjects were admitted in the dormitories under the same conditions.
In the field of amputee rehabilitation, Rommer et al.'s (2001) review showed that mobility scales include mainly performance in locomotion, walking distance and walking speed. In the present study, the main outcome chosen was the 2-minute walk test as it appeared to be most relevant and feasible in the study's context and because walking speed is a basic parameter that, when measured objectively, can be useful in characterising an individual walking ability (Boonstra et al. 1993). Secondary outcomes used were the MacGregor Physiological Cost Index (PCI) (Nene 1993; MacGregor 1981), the scale test (Stolov 1971), the Timed Up and Go (TUG) test (Podsiadlo and Richardson 1991), as well as 5 questions taken from the Functional Measure for Amputees Questionnaire (FMA) (Callaghan et al. 2002).
Overall duration of the tests was 30 minutes per person. The expatriate prosthetist verified before each test that alignment, fit and function of the newly provided prosthesis was optimal, as recommended by Isakov et al. (1992). Indeed, “successful rehabilitation of amputees requires that the prosthesis fulfils the needs of amputees (comfort, function and cosmetic), that the various prosthetic components are correctly chosen, assembled and aligned to provide maximum restoration of function and minimum gait deviation” (Yang 1991). For trans-tibial amputees, tests were carried out the day of first fitting in the morning and 2 days later in the afternoon. For trans-femoral amputees, the first test was performed on the day the person felt comfortable to walk unassisted outside of the parallel bars and 4 days later. The expatriate physiotherapist was in charge for the overall coordination of the testing procedure and the written transcription of the results. The tests were performed for all amputees in this sequence: scale test, 2-minute walk test and PCI, questionnaire and TUG. Each of the 2 physiotherapy assistants was responsible for 2 of the 4 tests (Tester 1: scale and 2-minute walk; Tester 2: questionnaire and TUG) to guarantee an optimal level of reproducibility and reliability.
2-minute walk test
The 2-minute walk test took place on a roof-covered walkway (approximately 100 m long and 5 m wide) surrounding the central area of the centre's building and marked every 5 m. Clear instructions (“walk as fast as possible”) were given, encouragement banned and patients were allowed to rest as described originally (Brooks et al. 2001). After the 2 minutes, the physiotherapy assistant dropped a sandbag at the level of the amputee's foot and stopped the timing. The distance (with an accuracy of +/−1 cm) was measured by the physiotherapy assistant with the help of the expatriate physiotherapist.
Physiological cost index (PCI)
For the PCI test, the patient stood for 2 minutes quietly at the departure line, after which the heart rate was measured by the tester and the expatriate physiotherapist took the radial pulse for 30 seconds. This measurement was repeated if the values of both testers differed for more than 5 beats. A few seconds after the end of the 2 minutes walk, pulse was taken again. PCI was calculated in the following manner: PCI (beats/m) = [heart rate at the end (beats/min) – heart rate at rest (beats/min)]/speed (m/min), (MacGregor 1981). The distance for this test not being standardised, we chose the distance walked in 2 minutes (Nene 1983; MacGregor 1981; Graham et al. 2005).
Scale test
The placement of the bathroom scales was standardised (close to each other next to the wall, on a levelled surface). Patients were first weighed on the right scale. They were then asked to stand at ease with one foot on each scale. The weight on both scales was recorded when they stopped holding on and looked straightforward. Finally, the subjects were asked to put the maximal weight on the prosthetic foot, without support of their hands, and had to keep this position for at least 2 seconds. Static weight bearing was defined as [weight bearing on the prosthetic foot (on 1 scale)/total body weight]×100 (Jones 1997).
Questionnaire
5 questions from the Functional Measure for Amputee questionnaire (Callaghan et al. 2002) were selected: ability to don and doff the prosthesis, score of the Locomotor Capability Index (LCI), maximal walking distance, number of falls, walking aid used in and outdoor. Translation into Myanmar dialect was done using the back and forth method (Guillermain et al. 1994). Interviews took place in the physiotherapy room. Finally, it was decided to use only the LCI scores because the other questions were not appropriate for the study's population. This index evaluates the ambulatory skills with prosthesis by assessing 14 different locomotor activities (7 basic items and 7 advanced items) and scores with a 4 level ordinal scale.
Timed up and go test (TUG)
TUG was the last test performed in front of the physiotherapy room. The chair of the orthopaedic centre was adjusted to fit the requirements and its placement marked 10 cm from the departure line; 3 m further a second line indicated the return point. As described originally (Podsiadlo and Richardson 1991), the patient stood up, walked in a safe and comfortable speed to the line and returned to sit down; the test was repeated twice. Time was recorded from the moment when the patient's back left the backrest to the moment it touched it again. During the test, the investigator stood at the level of the chair and did not give any encouragement.
Analysis
Data were entered and checked for completeness and normality. Means and standard deviation for the main outcome measures were calculated at baseline and at follow up. With ANOVA the change of performance after the intervention in both groups of amputees was analysed for the following variables: 2-minute walk test and speed, weight bearing when on 2 feet or when placing maximal weight bearing on the prosthetic leg, LCI, PCI and TUG tests. A regression analysis was performed to identify the predictors of the main outcome measure being the 2-minute walk test. For every statistical analysis, the level of significance was set at p = 0.05. Data analysis was performed with SPSS 12.0 (SPSS 2001).
Results
Population
The population (Tables I and II) consisted of 58 male amputees, 29 belonging to the experimental group and 29 to the control group. Both groups were similar at baseline. The mean age was 36.9 years (SD 11 years) in the experimental group and 35.2 years (SD 8 years) in the control group. Time since amputation (11.3 years; SD 8 and 9.6 years; SD 5) and number of prosthesis worn so far (mean = 1.4; SD 1 in the experimental group and mean = 1; SD 0.7 in the control group) were comparable.
Population and outcomes at baseline (n = 58)
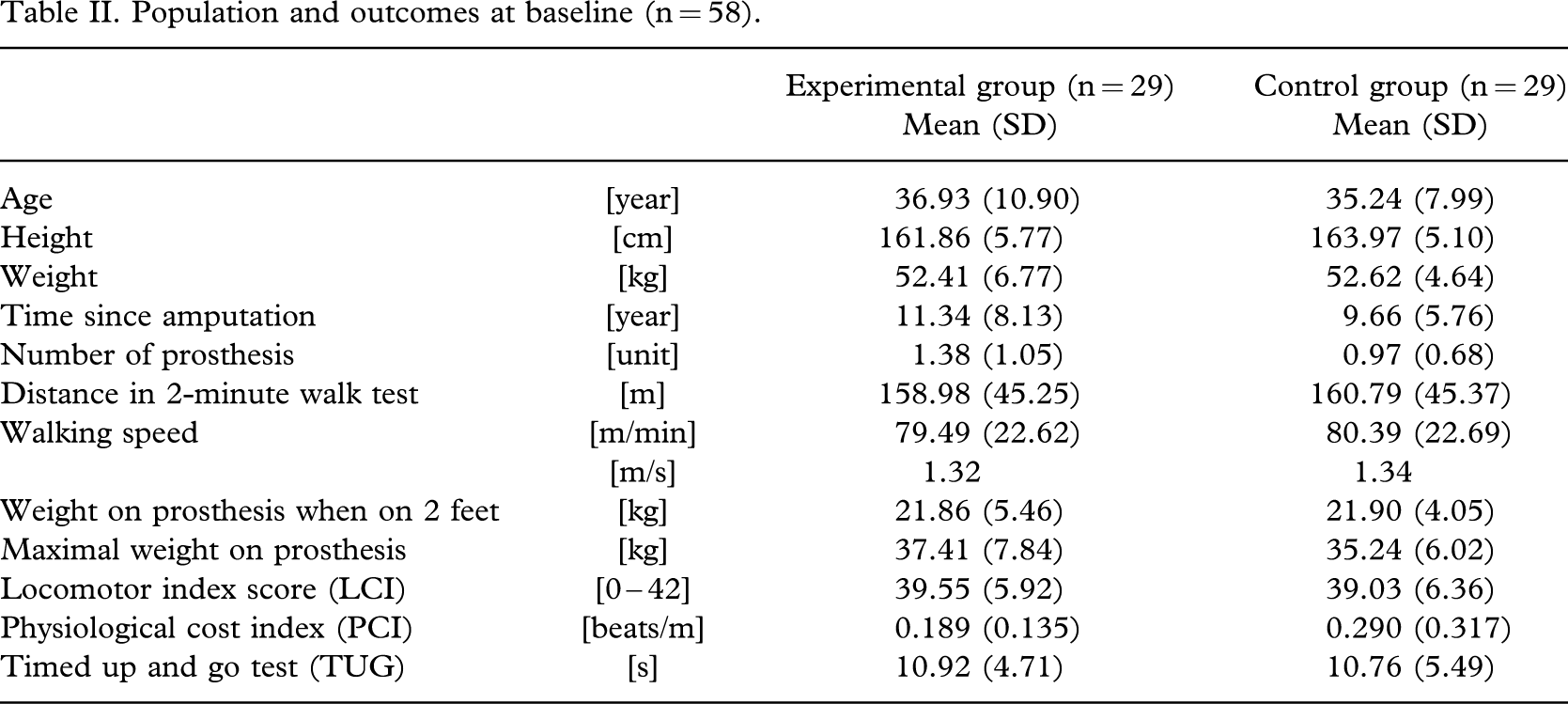
Considering the main outcome, the mean distance walked on the initial 2-minute test was 158.98 m (SD 45.25) in the experimental group and 160.79 m (SD 45.37) in the control group, while walking speed was comparable, with a mean speed of 79.49 m/min (SD 22.62) in the experimental subjects and 80.39 m/min (SD 22.69) for the control ones. The weight placed on the prosthetic foot, when standing on both feet, was 21.86 kg (SD 5.46) in the experimental group and 21.90 kg (SD 4.05) in the controls. (This represents a mean for both groups of 37.52% of body weight). The PCI values were 0.189 beats/m (SD 0.135) in the experimental group and 0.290 beats/m (SD 0.317) in the control group. Finally, the time in seconds to realise the TUG test was of 10.92 s (SD 4.71) in the experimental group and 10.76 s (SD 5.49) in the control group.
Main outcome
The experimental group outperformed the control group significantly in the 2-minute walk test, PCI and scale test (only when weight bearing on the prosthetic foot), 3 of the 5 tests performed (Table III). Considering the main outcome, the 2-minute walk test, the results between pre- and post-intervention showed a significant difference in favour of the experimental group (p = 0.024) with mean improvement in distances of 20.15 m (SD 17.12) for the experimental subjects and 8.93 m (SD 19.52) for the control subjects. The wide standard deviations could be explained by the variability of the amputees, ranging from already fitted trans-tibial amputees to first fitted trans-femoral amputees. Walking speed improved significantly after the intervention in the control subjects (p = 0.016). The PCI demonstrated also a significant difference (p = 0.02), with a mean improvement of 0.77 beats/m for the experimental group versus 0.39 beats/m for the control subjects.
Differences in main outcomes after intervention
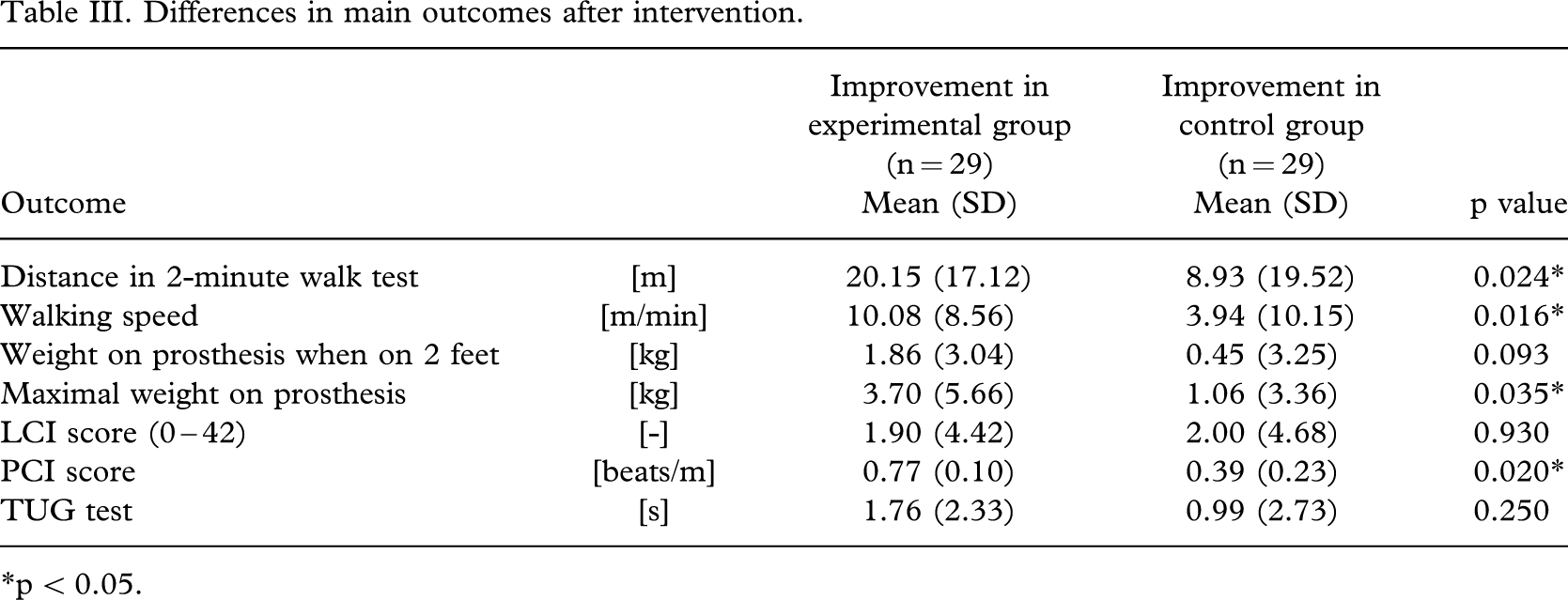
∗p < 0.05.
The improvement in amount of weight bearing, when standing on 2 feet, did not show a significant difference between both groups (p = 0.093). On the contrary, change of amount of weight bearing when asked to place maximal weight on the prosthetic foot showed significant differences (p = 0.021), with a mean difference of 3.7 kg (SD 5.66) for the experimental group and 1.06 kg (SD 3.36) in the control group. Results of the LCI questionnaire did not show a significant difference between both groups (p = 0.93). Finally, means of the TUG tests were not significantly different between both groups (p = 0.25).
Predictor on the main outcome
The variables that predict improvement in the main outcome (walking distance) by a linear regression model (R = 0.505) are the type of therapy (OR = 5.478 with 95% CI = −7.726 to −0.682), weight of the patient (OR = −0.396 with 95% CI = −0.802 to 0.010) and stump length (OR = −4.204 with 95% CI = 0.875 to 10.082) (Table IV).
Predictors for improvement on the 2-minute walk test
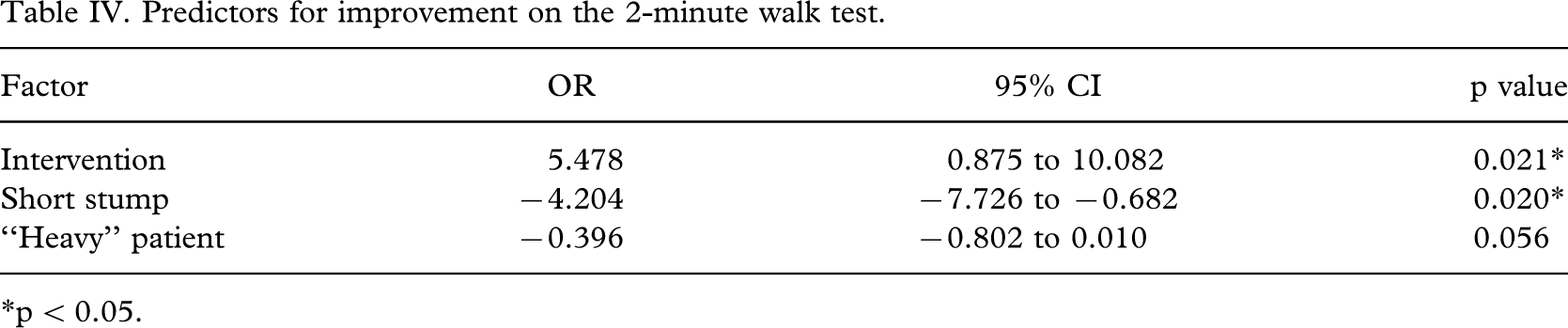
∗p < 0.05.
Discussion
The population was composed of young and fit amputees, while most of the literature describes elderly vascular amputees. Gavrankapetanovic et al. (2001) was one of the few to study age comparable subjects (younger than 30 years), but the issue of performance after injuries of the hindfoot is not comparable to that of Myanmar trans-tibial and trans-femoral amputees.
2-minute walk test
The clinical relevance of the results gives a clear indication that even short but specific physiotherapy programmes have significant results on lower limb amputee walking performance. Intensity of training and optimising of potential is probably more important than physiotherapy duration (3 sessions of one hour each approximately). The motivation given to practice at an adequate level of effort instead of just free ambulation could be another explanation of better improvement in the experimental group. Other factors could be the variation of practice, better gait pattern or confidence while practising walking on different grounds, etc. The walking test was probably the closest to the reality, the most sensitive to change in such a short training period and surely the most attractive for both patients and physiotherapy assistants.
This test was chosen because it is simple and easy to administer; furthermore because some newly fitted amputees cannot walk for 6 minutes. It was also confirmed that the 2-minute test is a good tool to measure functional exercising capacity in persons with lower limb amputation. Brooks et al. (2001) demonstrated that this test is responsive to change in rehabilitation of amputees, and has a good correlation with measures of functioning and prosthetic use. Butland et al. (1982) showed that the 2-minute test correlates highly with the 12-minute test (r = 0.86) and the 6-minute test (r = 0.89). Finally, there is a good reliability for speed recording for both comfortable and fast speed (test-retest correlation coefficient of 0.83 – 0.98) (Boonstra et al. 1993).
The mean speed of our population is 1.33 m/s. This is comparable to the preferred walking speed of 1 – 1.67 m/s, reported by Waters and Mulroy (1999) or 1.39 m/s cited by Jones et al. (2001) or 1.37 m/s of Gonzales et al. (1994). Boonstra et al. (1993) examined 16 trans-femoral amputees (mean age of 40 years) with a mean fast gait speed of 1.26 m/s. Isakov et al. (2000) examined traumatic amputees (aged from 32 to 57 years, heavier and taller than the present study's population) and reported a mean comfortable speed of 1.24 m/s.
PCI
The PCI measures the heart rate in a reliable but not valid way for healthy subjects (Graham et al. 2005); it can nevertheless be considered as a good method to monitor changes in the energy expenditure for walking in such an environment and in people with disabilities. It is relatively easy to measure and does not require elaborate instrumentation. The observed small differences in walking speed are not sufficient to change cardiac rate, nevertheless, the intensity of the 3-day training might have been the cause of the significant difference in favour of the experimental group. Hypotheses are that experimental subjects managed their efforts better during this specific training or were stimulated to walk more during the rest of the day. Considering the results, Nene (1993) showed that PCI values among adults are 0.2 – 0.55 beats/m and in adolescents 0.15 – 1.65 beats/m, and that there is no significant difference between different age groups. MacGregor (1981) gives values for normal subjects of 0.51 – 0.11 beats/m and Graham et al. (2005) shows values of 0.30 – 0.34 beats/m, unfortunately, the authors cannot be sure that the mean PCI value of the present population (0.23 beats/m) can be considered as normal because the amputees were measured while standing and not sitting for 10 minutes.
Scale test
One could argue that 3 days of intensive rehabilitation are not sufficient for assimilating the newly learned skills or acquiring new habits, and therefore could not have an effect on the results of the test when standing spontaneously on 2 feet. But on specific verbal stimulation of the therapist (“put the maximum weight on your prosthetic foot”), the amputees of the experimental group, having done more specific weight bearing exercises, might recall the performance trained specifically, and therefore perform better. Confidence, strategy and balance on the prosthetic foot were certainly also increased through functional tasks such as walking on a bridge carrying water canisters. ICRC physiotherapy staff used bathroom scales in exercising for a long time, having noticed that simple measurements of weight distribution can assist in retraining amputees to stand, balance and walk; it also gives objective confirmation of clinical improvement by providing a numerical feedback.
The authors modified the protocol proposed by Jones et al. (1997) to the need of the present population and this might explain the difference in the results: Jones gives higher values than this study for static weight bearing; for trans-tibial amputees, 94.93% (range from 77 – 100%), and 88.36% for trans-femoral amputees (range from 43 – 100%) in a population of 73 amputees (48 trans-tibial and 25 trans-femoral amputees, mean age of 60). When asked to put maximal weight on prosthesis, the authors' population reached 36.33% (SD = 7.01) of their body weight before training and 38.72% (SD = 8.31) after 3 days of training; when on their 2 feet, the results were 41.47% (SD = 0.06) before training and 43.64% (SD = 0.07) after physiotherapy.
TUG test
The TUG test is simple, pragmatic, quick and easy to perform, does not require special equipment nor professional expertise or training. In addition, it can be used as a descriptive tool, screening test or to monitor change over time. This test correlates with the Berg Balance test (r = −0.81) and with the Barthel Index (r = −0.78) (Podsiadlo and Richardson 1991). Schoppen et al. (1999) report for the TUG an intra-rater validity of r = 0.93 and inter-rater validity of r = 0.96, showing some relationship with the Sickness Impact Profile and other measure instruments: it therefore appears to predict the patient's ability to go outdoors safely, measuring the physical mobility of elderly with lower limb amputations.
Mean TUG improvement of the 2 groups did not change significantly. The test is probably not sensitive enough for fit amputees, and the walking distance too short. The time of this study's population (mean = 10.8 s, SD 5.15) is slightly slower but comparable to those of Podsiadlo and Richardson (1991) with elderly healthy volunteers doing this test in 10 seconds or less (mean = 8.5 s, SD 7 – 10 s). This duration is much smaller that the one of elderly patients (10 to 240 s) (Podsiadlo and Richardson 1991). The mean time of a population of 21 – 94 years old amputees (73% male) was of 24.5 s and therefore much slower than the authors' young traumatic amputees (Schoppen et al. 1999). Clinically, a result of 20 seconds or less in the TUG assures independence in basic transfers and less than 10 seconds signifies being freely independent; therefore, it illustrates well the excellent level of independence of Myanmar amputees.
Questionnaire
The use of the FMA questionnaire conceived for a Scottish population of mostly diabetic amputees highlighted some interesting cultural differences, as well as characteristics related to the population type. It is used to assess the level of mobility, independence, extent of prosthetic use and to identify factors that might influence these outcomes (Callaghan et al. 2003). First of all, the authors had to select the most relevant questions and could only use those categorized as enabling factors, according to Gauthier's PRECEDE model (Grisé et al. 1993); this model identifies 3 domains: predisposing factors (motivation given for a behaviour), enabling factors (factors related to the realisation of locomotor abilities) and reinforcing factors (factors evaluating satisfaction and benefits of the behaviour) (Gauthier-Gagnon and Grise 1994). Questioning for predisposing factors had no sense in the present population. Reinforcing factors concerned by quality of the prosthesis and owner satisfaction were not relevant either.
Question 2 of the FMA, in fact the LCI, was therefore the most interesting, relevant and best understood. The question about the walking distance was probably misinterpreted; indeed most of the patients answered that they could walk as far as possible, but said also that they could walk at most for 1 hour. Myanmar people often assess distances or times in a different way compared to us (e.g. distance between places used as reference instead of meters, the position of the sun instead of the display of a watch, which only a few possess). Worth mentioning is that the LCI is disease specific and includes the perception of capability. It shows a high internal consistency with a Cronbach alpha of 0.95, an intra-class correlation of 0.98 and correlated with all criterion measure (r = 0.61 – 0.76), proving that it captures the global locomotor ability of people with lower limb amputation (Franchignoni et al. 2004).
Predicting factors
The main factor predicting the results of the 2-minute walk test is the type of intervention indicating that our intervention was properly designed, according to the needs of the amputees; it was aimed at improving functional skills of subjects and did address the main goal: optimal ambulation. The fact that stump length predicts walking speed may agree with conventional thinking: the longer the stump, the best the control over the prosthesis, for trans-tibial amputees, longer stumps offer most favourable control over their knee and for trans-femoral amputees, longer stumps prevent for example muscle contractures limiting walking speed. Another predicting factor was the weight of the patient, which might indicate that the lightest patients perform better than the heaviest ones. With a mean weight of 52.5 kg in the present population, the authors have difficulties interpreting this result.
Time since amputation, level of amputation, stump characteristics such as pain, skin problems were not predictors for results of the 2-minute walk test. Time since amputation may not be a predictor because of the amputees showing overall excellent test results. Newly fitted patients in Myanmar are highly motivated, the majority not suffering from bad habits and receiving minimal training during the first days of prosthetic use. Similarly amputees fitted for a long time perform well as they use their prosthesis daily. On the other hand, it is understandable that stump pain and stump problems do not influence the outcome. The present study's subjects do not pay much attention to physical problems, often just used to facing difficult health conditions (e.g. stump problems).
Study limits and strengths
Amputees of the control group quickly realised that they missed interesting and new exercises and were prone to try them on their own. Moreover, the experimental group might have shared their experience with the subjects of the control group. Concerning possible bias in the 2-minute walk test and PCI, the order to walk as fast as possible might have been incorrectly followed by some amputees. Nene's protocol, asking the subjects to be seated for 10 minutes prior the test, could not be respected because of time constraints.
Using analogue scales presented disadvantages such as poor reliability (even after daily calibration), possible reading errors and variation in time measurement. In the TUG test, the authors cannot be sure that the order to walk at a comfortable speed was given adequately and followed by all amputees. The starting position might have been less comfortable for this population which was shorter than the European one (e.g. feet not resting properly on the floor because of the seat height). For all tests, the skills of the testers might have improved during the 3 months. Concerning the questionnaire, many of the patients did not understand the national language and the tester had to translate the questions into the patient's dialect.
Implementing a study in a clinical environment is not easy and even more challenging if the staff is not used to testing procedures. But the novelty of this experience and motivation of staff and amputees assisted in the implementation of this research. In a developing country, using equipment such as a stopwatch or validated testing procedures can appear highly technical for the staff and the patients: this presented some opportunities for improving education and informing about current practice abroad. Explaining concepts as basic as weight and height, notion of time or results of a test was not obvious; it proved to be an occasion for some of the subjects to learn more about their body or other value systems. There is no doubt that using more sophisticated equipment such as force platforms instead of bathroom scales might have provided more precise measurement of weight bearing. Energy expenditure test on a treadmill with oxygen consumption methods in place of heart rate measurement could have given more detailed results, too; with evidence, this equipment is not adequate in such an environment. Low cost equipment can be useful for research if used in a proper way. Finally both the staff and the amputees were in a position to understand the proposed method; in this sense, the learning process was clearly positive.
Conclusion
This study has shown that a short and intensive physiotherapy programme yields positive results in terms of improving the walking speed, the intervention being the best predictor of the main outcome. This form of training is more useful in the rehabilitation of traumatic amputees than usual care consisting mainly of walking. Given the social, economic and political consequences of landmines, the authors recommend adequate curative, rehabilitative and preventive measures, including specific physiotherapy training when treating traumatic lower limb amputees. Recent experience in Aceh province (Indonesia) following the consequences of the Tsunami disaster unfortunately shows that rehabilitation measures are not yet implemented on a regular basis: new amputees appear not to have systematic access to prosthetic care (Perlez 2005). Research in the field of traumatic amputees is all the more justified, since the number of potential disabling weapons keeps increasing; the probability of being injured by mines or fragments remains high for the foreseeable future.
Footnotes
Acknowledgements
The authors acknowledge the contribution of Hpa An rehabilitation centre team and the excellent collaboration of the amputees. This study would not have been possible without the assistance of Khin Moe Kyi and Nan Kaw Kei, physiotherapy assistants, and of Frédérique Bonvin, physiotherapist. The authors also wish to thank Ms Condie (University of Strathclyde) for allowing them to use the FMA questionnaire and the University of Zürich who put at their disposal the SPSS statistical software package. Last but not least, the authors are very grateful to Dr Blanc (University Hospital Geneva) for his assistance throughout the project.